Anterolateral Bowing | NF1 Association | Recalcitrant Nonunion
- NF1 mutation drives impaired osteoblast function and poor bone healing
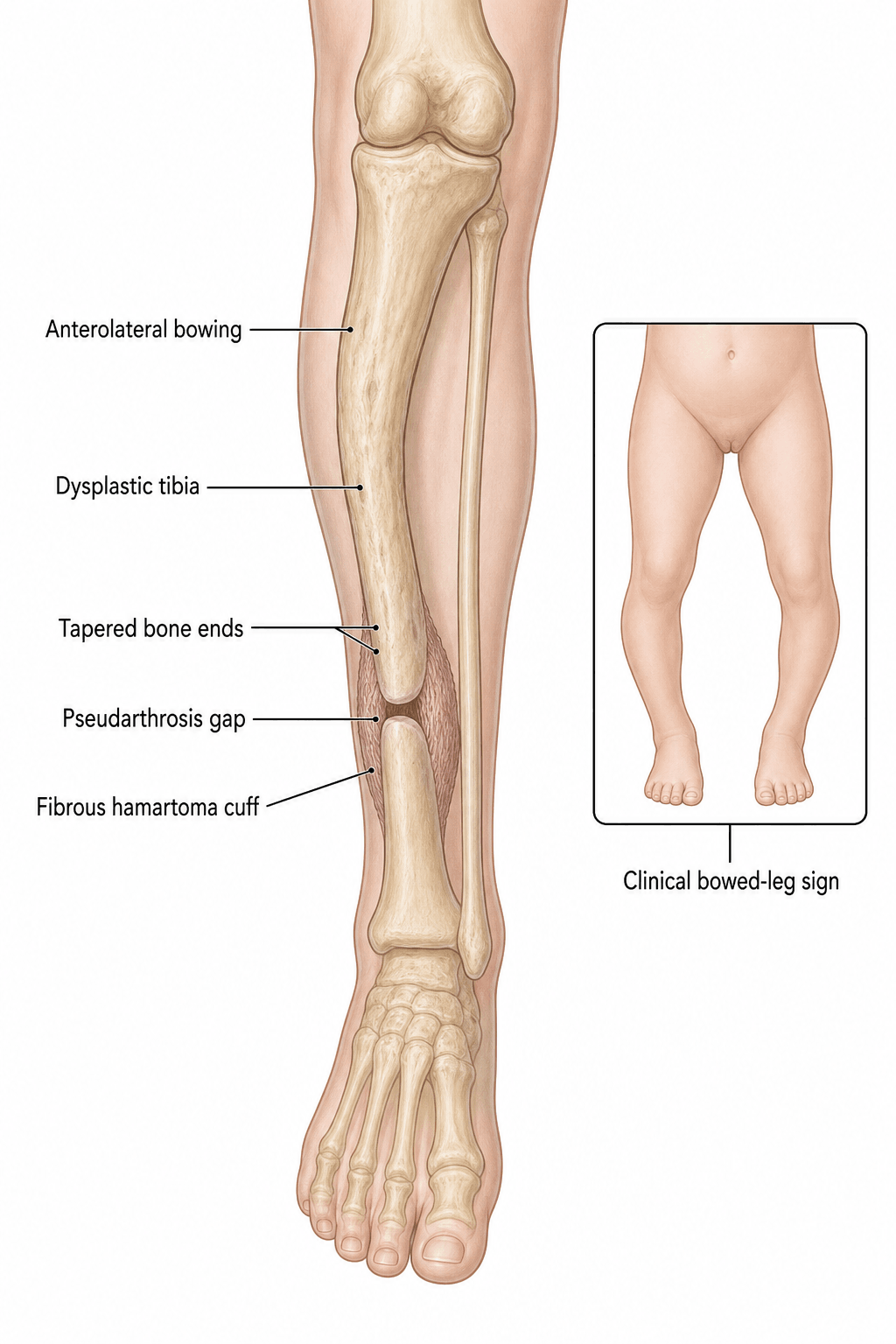
- Anterolateral bowing begins in infancy and fractures early leading to pseudarthrosis
- Crawford classification guides prognosis and timing of intervention
- Union rates remain low despite modern techniques; refracture is common
- Cross-union technique and vascularised fibula offer highest long-term success
- “Always screen for NF1 stigmata in any anterolateral bow
- “Type IV pseudarthrosis has the worst healing potential
- “Ilizarov with compression-distraction remains gold standard in many centres
- “Amputation rate still 10-30 percent in refractory cases worldwide
50-80 percent of CPT cases have NF1. Look for cafe-au-lait macules, axillary freckling, Lisch nodules, and family history. NF1 drives the poor bone biology and higher refracture risk.
The hallmark deformity. Begins in infancy, apex at junction of middle and distal thirds. Progresses to fracture by age 2-3 years in most untreated cases. Differentiate from posteromedial bowing which has excellent prognosis.
Guides prognosis and treatment timing. Type I has best prognosis; Type IV established pseudarthrosis has poorest healing potential. Serial radiographs track progression from bowing to cystic change to frank nonunion.
Union is difficult to achieve and maintain. Even after apparent radiographic union, refracture rates exceed 50 percent. Multiple surgeries common; amputation remains a realistic endpoint in 10-30 percent of severe cases.
- Diagnosis
- Crawford I-II on X-ray, NF1 screen positive
- Treatment
- Prophylactic bracing, serial observation
- Key Pearl
- Prevent fracture before pseudarthrosis develops
- Diagnosis
- Crawford III, narrow canal with sclerosis
- Treatment
- Consider early surgery or protected weight-bearing
- Key Pearl
- Pre-pseudarthrosis window for intervention
- Diagnosis
- Crawford IV, atrophic bone ends
- Treatment
- Surgical reconstruction (Ilizarov, vascular fibula, cross-union)
- Key Pearl
- High refracture risk; counsel family early
CALMSNF1 Features in CPT
Hook:CALMS reminds you to screen every CPT patient for NF1 stigmata!
RIBVCSurgical Options for Established CPT
Hook:RIBVC - five letters, five strategies for the toughest nonunion in orthopaedics!
Overview and Epidemiology
Congenital pseudarthrosis of the tibia is one of the most challenging conditions in paediatric orthopaedics. Despite advances in fixation, biology, and microsurgery, union rates remain 50-80 percent at best and refracture occurs in over half of united cases. Early recognition of anterolateral bowing before fracture, NF1 screening, and realistic family counselling are essential. The condition accounts for a disproportionate share of paediatric amputation and multiple surgical interventions worldwide.
- Incidence: 1 in 140,000 to 1 in 250,000 live births
- NF1 association: 50-80 percent of all CPT cases
- Sex ratio: Slight male predominance (1.2:1)
- Laterality: Unilateral in greater than 95 percent; right equals left
- Age at fracture: Mean 2.5 years, range birth to 12 years
- Recalcitrant nonunion: Highest failure rate of any long-bone nonunion
- Refracture: greater than 50 percent after apparent union
- Limb-length discrepancy: 2-5 cm common at skeletal maturity
- Amputation rate: 10-30 percent in refractory cases
- Multiple surgeries: Average 3-6 procedures per patient
Pathophysiology
NF1 is caused by loss-of-function mutations in the neurofibromin gene on chromosome 17. Neurofibromin normally inhibits RAS signalling; its absence leads to uncontrolled RAS activity, impaired osteoblast differentiation, increased osteoclast activity, and a fibrous hamartoma replacing normal bone at the pseudarthrosis site. The hamartoma produces excessive TGF-beta and has poor vascularity, explaining the atrophic nonunion and high refracture rate even after stable fixation. Fibular pseudarthrosis coexists in 50-75 percent of cases and must be addressed to prevent valgus collapse.
- Pathology
- Periosteal dysplasia, NF1 hamartoma
- Radiograph
- Anterolateral bow, normal canal (Crawford I)
- Risk if Untreated
- Fracture by age 3 years in 70 percent
- Pathology
- Medullary narrowing, sclerosis
- Radiograph
- Type II-III changes, impending fracture
- Risk if Untreated
- Pathologic fracture within months
- Pathology
- Atrophic bone ends, fibrous hamartoma
- Radiograph
- Type IV mobile nonunion +/- fibula
- Risk if Untreated
- Refracture, shortening, deformity
Poor biology: Deficient osteoprogenitor cells, excessive fibrous tissue, low BMP responsiveness. Mechanical factors: Narrow distal fragment, poor purchase for fixation, high shear at apex. Vascular compromise: Hamartoma is hypovascular; periosteal stripping during surgery worsens it. Fibular involvement: Untreated fibular pseudarthrosis leads to valgus and refracture.
Growth disturbance: Asymmetric physeal growth from NF1 dysplasia. Periosteal tethering: Fibrous hamartoma tethers lateral cortex. Muscle imbalance: Weak anterior compartment contributes to apex anterior deformity. Mechanical axis: Lateral bow places distal tibia in varus, increasing fracture risk.
Classification and Types
Crawford Classification (1986) - Gold Standard
- Radiographic Features
- Anterolateral bow, normal medullary canal
- Prognosis
- Best; may never fracture
- Treatment Approach
- Observation, prophylactic bracing
- Radiographic Features
- Narrowed canal, cortical sclerosis
- Prognosis
- Good if protected
- Treatment Approach
- Bracing, early surgery if cystic change
- Radiographic Features
- Cystic lesion at apex
- Prognosis
- Moderate; high fracture risk
- Treatment Approach
- Consider prophylactic surgery
- Radiographic Features
- Established pseudarthrosis +/- fibula
- Prognosis
- Poorest; high refracture
- Treatment Approach
- Surgical reconstruction mandatory
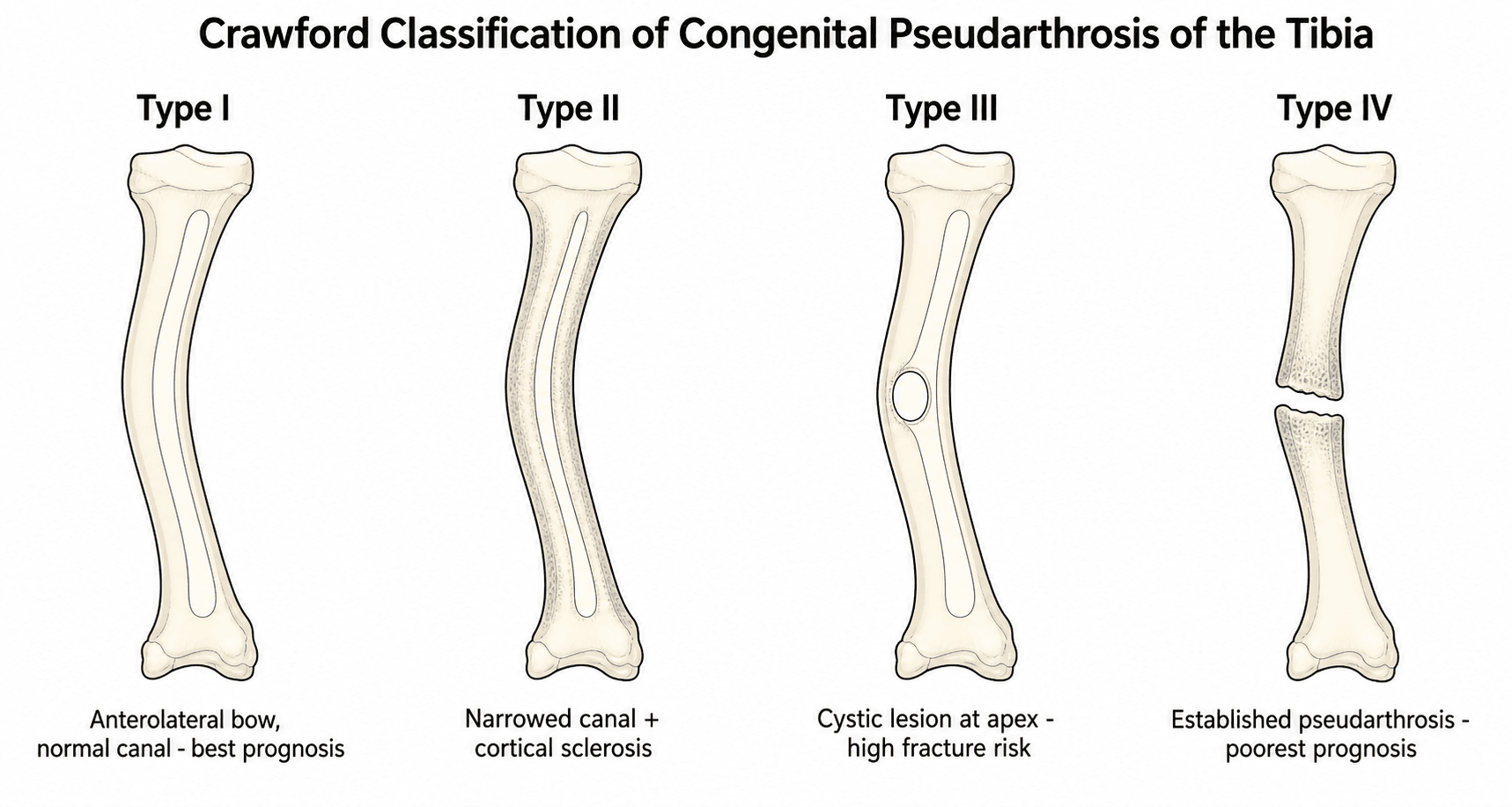
Crawford classification remains the most widely used because it directly correlates with natural history and guides the timing of surgical intervention.
BSCPCrawford Classification Progression
Hook:BSCP takes the tibia from bowing to pseudarthrosis - catch it before P!
Boyd Classification: The Six Types
The Boyd system (1982) predates Crawford and is referenced above as having "six types including atrophic and hyperplastic" — it is worth knowing in full because it is descriptive and aetiologic (it captures the lesion's origin and the fibula) where Crawford is purely radiographic. The trade-off is reproducibility: Boyd is harder to apply consistently, which is why Crawford remains the staging tool of choice. The six Boyd types describe the spectrum from a defect present at birth through to a pseudarthrosis arising within a tumour.
- Defining feature
- Anterior(-lateral) bowing with a tibial DEFECT present at birth; other congenital anomalies may coexist
- Prognosis / note
- Variable; defect present from birth
- Defining feature
- Anterolateral bowing with an HOURGLASS CONSTRICTION; spontaneous or low-energy fracture usually before age 2
- Prognosis / note
- The classic 'high-risk' tibia and the most common type; strongest NF1 link, poorest prognosis
- Defining feature
- Pseudarthrosis arising within a CYST, typically at the middle-distal third junction
- Prognosis / note
- Recurrence after treatment is less common than in types I and II
- Defining feature
- Pseudarthrosis originating in a SCLEROTIC segment WITHOUT canal narrowing; an insufficiency/stress fracture develops and may progress
- Prognosis / note
- Better prognosis, especially if treated before a complete fracture
- Defining feature
- Pseudarthrosis with a DYSPLASTIC FIBULA (fibula and/or tibia involved)
- Prognosis / note
- Good if confined to the fibula; behaves like type II once the tibia is involved
- Defining feature
- Pseudarthrosis from an INTRAOSSEOUS neurofibroma or schwannoma
- Prognosis / note
- Rare; prognosis depends on the tumour and its treatment
Use both, for different reasons. Crawford (I-IV) is radiographic, reproducible, and the standard for STAGING and timing of intervention. Boyd (I-VI) is descriptive and captures the lesion's origin (defect at birth, hourglass constriction, cyst, sclerosis, dysplastic fibula, or intraosseous tumour) — Boyd Type II (hourglass constriction, fracture before age 2) is the classic high-risk NF1 tibia, and Boyd Type VI flags the rare tumour-related pseudarthrosis that needs a different work-up.
Clinical Assessment
- Onset: Noticed bowing in first year of life
- Family history: NF1 in first-degree relatives
- Previous fractures: Number, age, healing attempts
- Functional limitation: Pain, limp, shoe wear problems
- Prior surgery: Number of procedures, complications
- Inspection: Anterolateral bow, skin dimpling, cafe-au-lait spots
- Palpation: Mobile pseudarthrosis, warmth, tenderness
- Gait: Short limb, circumduction, valgus thrust
- Neurovascular: Usually intact; check for NF1 neuropathy
- Associated: Scoliosis screen, limb-length discrepancy
Posteromedial bowing: Benign, resolves spontaneously, excellent prognosis, no NF1 link. Physiologic bowing: Symmetric, physiologic varus, resolves by age 2. Rickets / metabolic: Bilateral, metaphyseal changes, biochemical abnormalities. Osteogenesis imperfecta: Multiple fractures, blue sclerae, family history, collagen mutation. Always obtain full-length standing radiographs and NF1 clinical screen on every anterolateral bow.
- Direction
- Anterolateral
- NF1 Link
- 50-80 percent
- Prognosis
- Poor without surgery
- Key Discriminator
- Crawford changes, mobile nonunion
- Direction
- Posteromedial
- NF1 Link
- None
- Prognosis
- Excellent, resolves
- Key Discriminator
- Spontaneous correction, calcaneovalgus foot
- Direction
- Symmetric varus
- NF1 Link
- None
- Prognosis
- Resolves by age 2
- Key Discriminator
- No apex, normal bone quality
- Direction
- Variable
- NF1 Link
- Rare
- Prognosis
- Variable with bisphosphonates
- Key Discriminator
- Multiple fractures, blue sclerae
NF1 stigmata checklist: greater than 6 cafe-au-lait macules greater than 5 mm (prepubertal), axillary/inguinal freckling, greater than 2 neurofibromas or 1 plexiform, optic glioma, greater than 2 Lisch nodules, sphenoid dysplasia or thinning long bone, first-degree relative with NF1. Two or more criteria confirm NF1. Genetic testing confirms but is not required for diagnosis.
Investigations
Imaging and Laboratory Protocol
Views: AP and lateral tibia/fibula, full-length standing both legs, hand for bone age if discrepancy. Look for: Crawford type, fibular status, shortening, ankle valgus, proximal migration of fibula. Clinical correlation: Serial films every 3-6 months in bowing stage to detect cystic change or fracture.
Indication: Characterise pseudarthrosis morphology, bone stock, and plan fixation or transport. Findings: Atrophic bone ends, medullary canal diameter, hamartoma extent, fibular pseudarthrosis. Pre-op planning: Determine rod diameter, Ilizarov ring size, need for bone transport segment length.
Indication: Pre-operative planning for vascularised fibula or cross-union; assess hamartoma extent. Findings: Fibrous hamartoma replacing bone, periosteal reaction, muscle quality, vascular anatomy. Utility: Helps decide between Ilizarov, vascular fibula, or combined approaches.
NF1 testing: Clinical diagnosis sufficient; genetic confirmation if family planning or atypical features. Bloods: Full blood count, coagulation, type and screen before major reconstruction. Bone biochemistry: Calcium, phosphate, PTH, vitamin D to exclude metabolic contributors.
X-rays are the cornerstone; diagnosis and classification are radiographic. MRI and CT are adjuncts for surgical planning only. Do not delay bracing or referral while awaiting advanced imaging in an infant with anterolateral bowing.
Management Algorithm
Pre-fracture Anterolateral Bowing (Crawford I-III)
Goal: Prevent fracture and pseudarthrosis development through protected weight-bearing and monitoring.
Management Protocol
Bracing: Custom total-contact KAFO or AFO with anterior shell to counteract bow. Weight-bearing: As tolerated; encourage normal development. Surveillance: Clinical and radiographic review every 3 months. Family education: Signs of fracture (pain, swelling, refusal to bear weight).
Decision point: Prophylactic surgery versus continued bracing. Factors favouring surgery: Rapid cystic expansion, narrow canal less than 50 percent normal, family compliance concerns. Surgical options: Intramedullary rod insertion before fracture, or Ilizarov with prophylactic compression. Counsel: Even with surgery, fracture risk remains elevated.
The goal of bracing is to convert a high-risk Crawford II or III tibia into a Type I that never fractures. Success depends on compliance and early application before the first fracture. Once fracture occurs, the biology changes permanently and union becomes far more difficult.
Intramedullary Rod Fixation: Transankle and Telescoping Rods
The management tabs reference a "Williams or telescoping rod" and note that a telescoping rod "allows growth while maintaining stability" — these warrant developing, because the intramedullary rod is the workhorse of fixation in established CPT and the choice of rod is a common viva question. The principle is that a rod which spans the pseudarthrosis AND crosses the ankle (a TRANSANKLE or transcalcaneal rod) gives the best control of the short, dysplastic distal fragment and the most durable protection against recurrent angular deformity and refracture through the remaining years of growth. The rod is generally left across the ankle until skeletal maturity; the temporary loss of ankle motion is accepted because distal control matters more, and the ankle remodels.
- Williams rod
- Smooth solid (originally a two-part male-female obturator) intramedullary rod
- Telescoping (Fassier-Duval) rod
- Self-elongating two-component rod that telescopes as the bone grows
- Williams rod
- Fixed length; the bone grows off the end so the rod is progressively outgrown
- Telescoping (Fassier-Duval) rod
- Lengthens with the limb, maintaining fixation across the growing segment
- Williams rod
- Planned exchange/re-rodding as the child grows or the rod migrates
- Telescoping (Fassier-Duval) rod
- Fewer planned exchanges; revised mainly for failure, migration or non-telescoping
- Williams rod
- Long-established, widely available, low cost; still effective transankle
- Telescoping (Fassier-Duval) rod
- Adopted from osteogenesis imperfecta practice; favoured where revision burden is a concern
A rod is rarely used alone in CPT. Durable union depends on combining stable intramedullary fixation with the biology: radical resection of the fibrous hamartoma, autograft with or without BMP, periosteal grafting, and stabilisation of the fibula (or a tibia-fibula cross-union). The Paley combined ("4-in-1" / cross-union) strategy deliberately pairs a transankle intramedullary rod with cross-union, BMP and a bisphosphonate to attack the mechanics and the poor biology at the same time, which is the rationale for the very low refracture rates reported with that approach.
The distal tibial fragment in CPT is short, dysplastic and gives poor fixation purchase — a rod stopping above the ankle leaves it uncontrolled and prone to recurrent deformity and refracture. A transankle (transcalcaneal) rod captures that fragment and the hindfoot, holding alignment until skeletal maturity. Combine it with hamartoma excision, grafting/BMP and fibular stabilisation; rod fixation alone, without addressing the biology and the fibula, has a high failure rate.
Complications
- Incidence
- greater than 50 percent overall
- Risk Factors
- NF1, narrow canal, early weight-bearing
- Management
- Re-frame or revise fixation; consider cross-union
- Incidence
- 2-5 cm common at maturity
- Risk Factors
- Multiple surgeries, growth disturbance
- Management
- Epiphysiodesis, lengthening, shoe lift
- Incidence
- 30-50 percent with fibular involvement
- Risk Factors
- Untreated fibular pseudarthrosis
- Management
- Fibular stabilisation or supramalleolar osteotomy
- Incidence
- 10-30 percent after surgery
- Risk Factors
- Atrophic biology, inadequate fixation
- Management
- Revision surgery, vascular fibula, cross-union
- Incidence
- 10-30 percent refractory cases
- Risk Factors
- Multiple failed surgeries, infection, family choice
- Management
- Below-knee amputation with modern prosthetics
Achieving radiographic union is only the first battle. The second, and often harder, battle is maintaining union through skeletal maturity. Protect the leg with bracing or frame for 6-12 months after apparent union. Monitor closely for early refracture. Cross-union and vascularised fibula currently offer the lowest refracture rates in published series.
Outcomes and Prognosis
- Union Rate
- 70-85 percent
- Refracture Rate
- 40-60 percent
- Limb Salvage
- 70-85 percent
- Union Rate
- 80-95 percent
- Refracture Rate
- 20-40 percent
- Limb Salvage
- 85-95 percent
- Union Rate
- greater than 90 percent
- Refracture Rate
- less than 20 percent
- Limb Salvage
- greater than 95 percent
- Union Rate
- 50-70 percent
- Refracture Rate
- greater than 60 percent
- Limb Salvage
- 60-75 percent
Best prognosis: Crawford I-II caught before fracture, non-NF1, good family compliance, access to specialist paediatric limb reconstruction centre. Poor prognosis: NF1 positive, Crawford IV at presentation, fibular pseudarthrosis, prior failed surgery, short distal fragment, infection. Key threshold: First fracture before age 3 years predicts worse outcome; multiple surgeries before age 5 years increase amputation risk.
Guidelines, Registries & Global Practice
- Incidence 1 in 140,000-250,000 worldwide; no clear geographic variation
- NF1 association consistent across populations (50-80 percent)
- Amputation rates higher in low-resource settings due to limited access to Ilizarov and microsurgery
- Specialist centres in high-resource countries report better limb salvage (greater than 85 percent)
- High-resource: Ilizarov, vascular fibula, cross-union, BMP, dedicated limb reconstruction teams
- Limited-resource: IM rod plus autograft, prolonged bracing, higher amputation threshold
- Universal principle: Early bracing before fracture and realistic family counselling are low-cost interventions that improve outcome everywhere
- Surgery: Concentrated in 10-15 global centres with sufficient case volume for expertise
- Diagnosis emphasis
- Crawford classification + NF1 screen on every anterolateral bow
- Surgical strategy
- Ilizarov or vascular fibula at specialist centres; cross-union for salvage
- Long-term protection
- 12 months protected weight-bearing after union; monitor to skeletal maturity
- Diagnosis emphasis
- Early referral to limb reconstruction units before first fracture
- Surgical strategy
- Fibular stabilisation mandatory; cross-union gaining favour
- Long-term protection
- Long-term bracing until growth complete
- Diagnosis emphasis
- Genetic counselling offered for NF1-positive families
- Surgical strategy
- Individualised; IM rod, Ilizarov, or vascular fibula per surgeon preference
- Long-term protection
- Refracture risk discussed; amputation offered after multiple failures
There is no international CPT registry. Evidence is derived from single-centre series and expert consensus. The European Paediatric Orthopaedic Society (EPOS) and POSNA have published treatment algorithms emphasising early referral, fibular management, and prolonged protection. Cross-union is the most recent advance with the lowest published refracture rates.
Record in every anterolateral bowing case:
- Crawford type on initial and serial radiographs
- NF1 clinical criteria met or excluded
- Bracing compliance and family education provided
- Referral to specialist centre documented A missed opportunity to brace before fracture is a recurring source of preventable morbidity worldwide. Always document the bowing direction, NF1 screen, and management plan at the first visit.
Controversies & Areas of Uncertainty
Some centres advocate early rod insertion or Ilizarov compression before fracture in cystic lesions; others continue bracing until fracture occurs. No randomised data exist; decision is individualised by family compliance, canal diameter, and centre expertise.
Off-label BMP-2 or 7 is used by some surgeons to augment biology at the pseudarthrosis site. Small series suggest modest improvement in union rates, but concerns remain about cost, heterotopic ossification, and lack of high-level evidence.
Ilizarov, vascularised fibula, and cross-union all have advocates. No head-to-head trials. Ilizarov is most accessible globally; vascular fibula requires microsurgery; cross-union is emerging as preferred salvage with lowest refracture in recent reports.
After 3-4 failed reconstructions, severe shortening, or infection, many families choose amputation for quality-of-life reasons. Modern below-knee prostheses allow excellent function and sports participation; decision timing and counselling are critical.
MCQ Practice Points
Q: Which Crawford type has the worst prognosis for union? A: Type IV (established pseudarthrosis). Type I has normal canal and best prognosis; Type IV has atrophic bone ends, fibrous hamartoma, and the highest refracture rate despite surgery.
Q: What percentage of congenital pseudarthrosis of the tibia cases are associated with NF1? A: 50-80 percent. Every child with CPT requires full NF1 clinical screening (cafe-au-lait count, axillary freckling, Lisch nodules, family history). NF1-positive cases have worse biology and higher refracture risk.
Q: What is the typical age of first fracture in untreated anterolateral bowing? A: Mean 2.5 years (range birth to 12 years). Most untreated Crawford II-III cases fracture by age 3 years. Once fracture occurs, the pseudarthrosis biology is established and healing potential drops dramatically.
Q: Which surgical technique currently reports the lowest refracture rate in refractory CPT? A: Cross-union (tibia-fibula synostosis). Recent series show union greater than 90 percent and refracture less than 20 percent by creating a single-bone leg with larger cross-sectional area and better mechanics.
Q: What is the overall amputation rate in congenital pseudarthrosis of the tibia? A: 10-30 percent in refractory cases. Despite modern techniques, a subset of patients with multiple failures, infection, or severe shortening ultimately undergo below-knee amputation with excellent prosthetic function.
Clinical Imaging
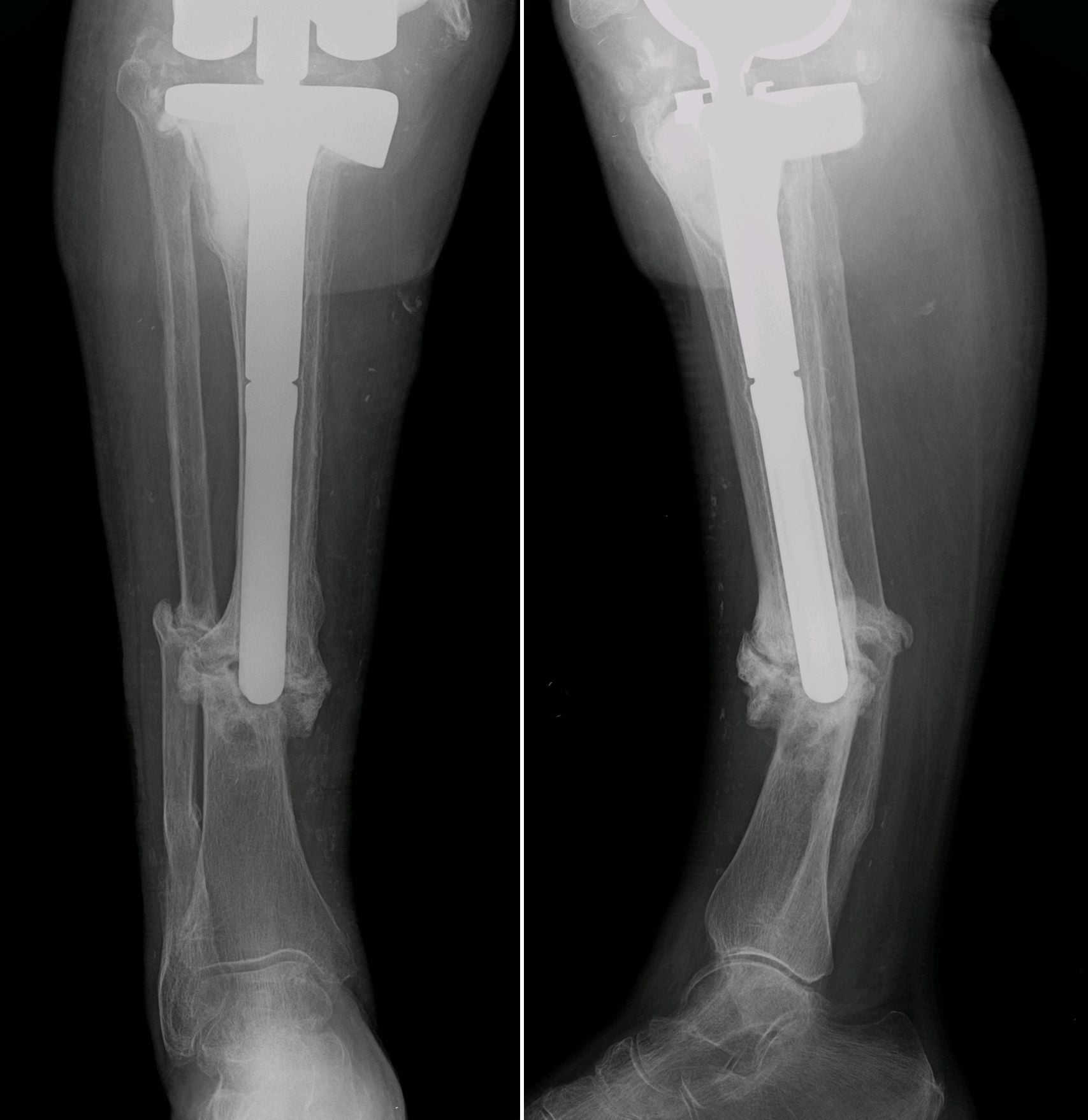
Radiographic Progression of Anterolateral Bowing to Pseudarthrosis
Congenital pseudarthrosis of the tibia (CPT) is defined by a dysplastic nonunion that develops after pathologic fracture through an area of anterolateral bowing. The natural history begins with a sclerotic or cystic lesion in the distal third of the tibia that progresses to fracture and established pseudarthrosis. Early radiographs show anterolateral bowing without fracture; later films demonstrate atrophic bone ends, sclerosis, and eventual pseudarthrosis with fibular involvement in over 50 percent of cases.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 14-month-old presents with progressive anterolateral bowing of the right tibia noticed since age 6 months. The child has six cafe-au-lait macules greater than 5 mm and axillary freckling. X-rays show Crawford Type II changes with cortical sclerosis and narrowed medullary canal. No fracture has occurred. What is your diagnosis, work-up, and management plan?”
“A 7-year-old with known NF1 and Crawford Type IV congenital pseudarthrosis has undergone three failed attempts at union (two IM rod plus graft, one Ilizarov). The leg is 4 cm short, the pseudarthrosis is mobile with atrophic bone ends, and the fibula is also pseudarthrotic with ankle valgus. The family is desperate to avoid amputation. What surgical strategy would you recommend?”
Key Biology and NF1
- NF1 mutation in 50-80 percent; drives poor osteoblast function and fibrous hamartoma
- Hamartoma produces TGF-beta, is hypovascular, and replaces normal bone at pseudarthrosis site
Crawford Classification
- Type I: anterolateral bow, normal canal - best prognosis, brace
- Type II: narrowed canal, sclerosis - protect, consider early surgery
- Type III: cystic lesion - high fracture risk, surgical threshold
- Type IV: established pseudarthrosis - worst outcome, surgery mandatory
Natural History
- Anterolateral bowing begins in infancy; mean fracture age 2.5 years if untreated
- Once fractured, biology changes permanently; refracture greater than 50 percent after union
Surgical Principles
- Debride hamartoma, stabilise (Ilizarov, rod, plate), address fibula
- Cross-union or vascular fibula for lowest refracture; protect 6-12 months post-union
Complications and Endpoints
- Refracture greater than 50 percent, LLD 2-5 cm, ankle valgus, amputation 10-30 percent
- Amputation is realistic endpoint after multiple failures; modern prosthetics give excellent function
Evidence Base and Key Trials
Osseous manifestations of neurofibromatosis in childhood
- Review of the osseous manifestations of neurofibromatosis in childhood, including tibial dysplasia and pseudarthrosis
- Describes the Crawford classification of anterolateral tibial bowing/dysplasia (types I-IV), with established pseudarthrosis the most severe pattern
- Emphasises the strong association of congenital tibial pseudarthrosis with NF1 and its recalcitrant, refracture-prone nature
- Also catalogues spinal (scoliosis/kyphosis, dural ectasia) and other skeletal manifestations of NF in children
Descriptive analysis of tibial pseudarthrosis in patients with neurofibromatosis 1
- Descriptive case-control analysis of 85 NF1 patients with long-bone pseudarthrosis from an international NF database
- ~5% of NF1 individuals have congenital long-bone pseudarthrosis, and 50-80% of congenital pseudarthrosis cases have NF1
- Significant MALE predominance with no parent-of-origin effect, suggesting male gender as a susceptibility factor
- Half of affected children sustained their fracture before age 2, and approximately 16% underwent amputation
Treatment of congenital pseudoarthrosis of the tibia using the Ilizarov technique
- 15 patients (16 CPT) treated with the Ilizarov method using compression, distraction, resection/shortening, bone transport or invagination
- Union achieved in 94% after one treatment and 100% after a second treatment; all angular deformity corrected
- Lengthening performed in 12 of 16; mean follow-up 4 years (range 2-7)
- Five refractures occurred (three early, two late); prior pin sites and residual deformity were predisposing factors
Congenital pseudarthrosis of the tibia: long-term followup of 29 cases treated by microvascular bone transfer
- Long-term follow-up of 29 patients with congenital pseudarthrosis of the tibia treated by vascularised (microvascular) fibular bone transfer
- Rate and speed of healing were superior to those of any other published method, with a generally acceptable final outcome at maturity
- The technique also permits secondary lengthening procedures
- Age at first fracture, age at operation, gender and type of fixation did not significantly influence the outcome