NF1 Association | Crawford Classification | Vascularized Fibula Gold Standard | High Failure Rate
- 50-90% associated with NF1 - always assess for café-au-lait spots, neurofibromas, family history
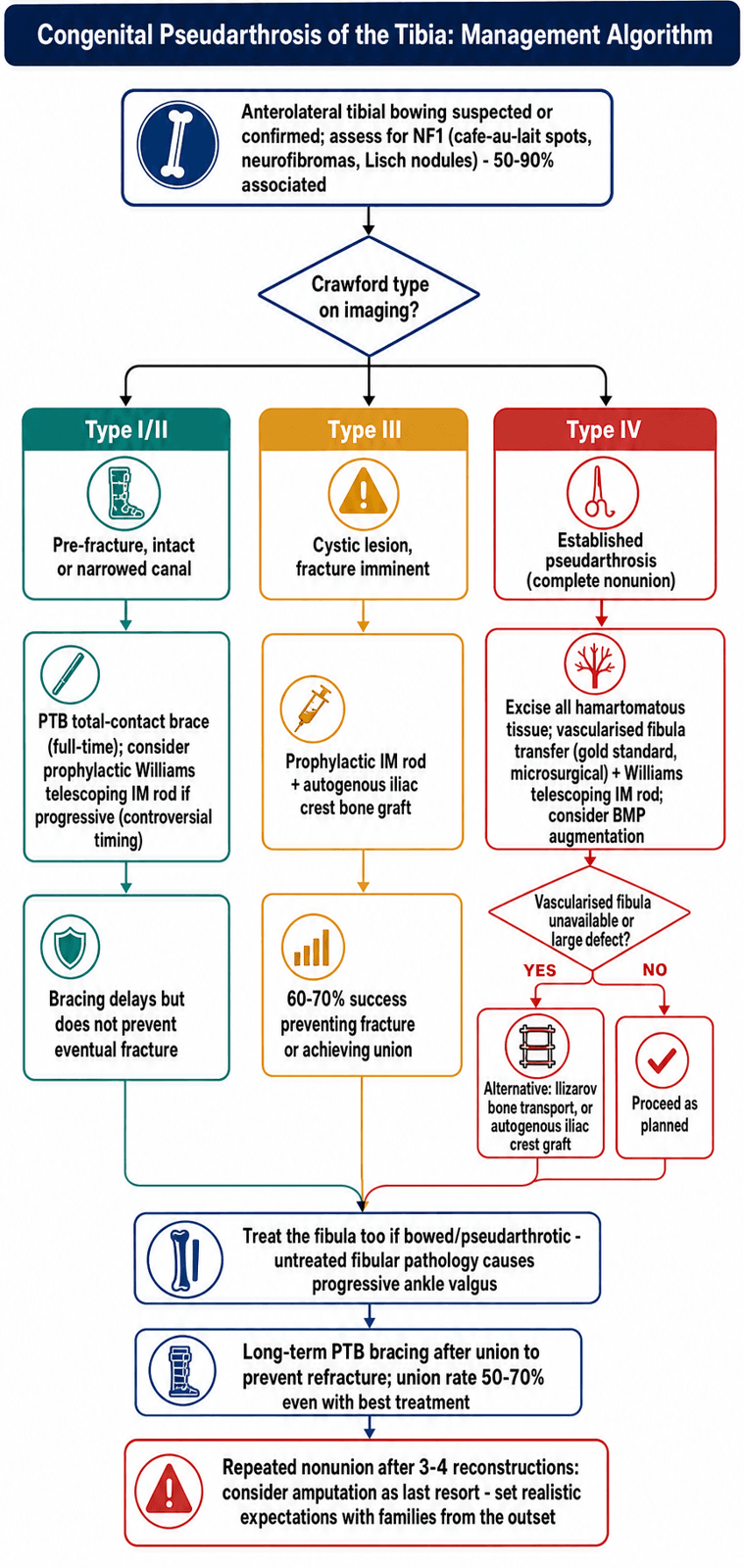
- Crawford classification guides treatment: Type I/II = bracing/prophylaxis, Type III/IV = surgical reconstruction
- Vascularized fibula transfer is gold standard for established pseudarthrosis (Type IV)
- Pre-fracture bracing (PTB orthosis) may delay fracture but does not prevent it
- High failure rate - multiple surgeries often needed, amputation may be required after multiple failures
- “Crawford classification is high-yield - know all 4 types and treatment implications
- “Vascularized fibula transfer is gold standard - preserves blood supply, better union rates
- “Williams telescoping rod allows growth while maintaining stability
- “Always assess for NF1 - café-au-lait spots, Lisch nodules, family history
50-90% of CPT associated with NF1 - always assess for café-au-lait spots (over 6 spots over 1.5cm), neurofibromas, Lisch nodules, family history. NF1 diagnosis affects prognosis and treatment approach.
Type I/II (pre-fracture): Bracing, prophylactic rod. Type III (cystic): Prophylactic rod + bone graft. Type IV (established): Vascularized fibula transfer (gold standard), IM rod, Ilizarov. Classification determines urgency and approach.
Vascularized fibula transfer preserves blood supply, achieves 50-70% union rate (best of all options). Requires microsurgery expertise. Combined with IM rod for stability. BMP may augment healing.
Multiple surgeries often needed - union rate 50-70% even with best treatment. Amputation may be required after 3-4 failed reconstructions. Realistic expectations essential for families.
- Description
- Anterior bowing, intact canal
- Treatment
- PTB brace, prophylactic rod
- Union Rate
- Prevention
- Description
- Anterior bowing, narrowed canal
- Treatment
- PTB brace, prophylactic rod
- Union Rate
- Prevention
- Description
- Cystic lesion, fracture imminent
- Treatment
- Prophylactic rod + bone graft
- Union Rate
- 60-70%
- Description
- Established pseudarthrosis
- Treatment
- Vascularized fibula + IM rod
- Union Rate
- 50-70%
Overview and Epidemiology
Congenital pseudarthrosis of the tibia (CPT) is a rare condition characterized by failure of the tibia to heal after fracture, resulting in a persistent nonunion. It is strongly associated with neurofibromatosis type 1 (NF1) and represents one of the most challenging conditions in pediatric orthopedics.
- Incidence: 1 in 140,000 to 250,000 live births
- Male to female ratio: 1.5:1
- Bilateral involvement: 10-15% of cases
- Left side slightly more common
- Strong association with NF1 (50-90% of cases)
CPT results from abnormal bone formation and healing. The exact mechanism is unknown but involves:
- Hamartomatous tissue at pseudarthrosis site (fibrous, non-ossifying)
- Abnormal periosteum (thickened, constrictive)
- Poor vascularity at pseudarthrosis site
- Abnormal bone biology (osteoclasts, osteoblasts dysfunction)
- NF1 gene mutation (when associated)
The condition represents a spectrum from anterior bowing (pre-fracture) to established nonunion (pseudarthrosis).
Pathophysiology and Mechanisms
The tibia is the primary weight-bearing bone of the lower leg. It has a triangular cross-section with anterior, medial, and lateral surfaces. The medullary canal contains bone marrow and provides a pathway for intramedullary fixation.
In CPT, there is:
- Anterior bowing: Characteristic deformity (anterolateral)
- Hamartomatous tissue: Fibrous, non-ossifying tissue at pseudarthrosis site
- Abnormal periosteum: Thickened, constrictive, prevents healing
- Narrowed medullary canal: In Type II, canal becomes sclerotic and narrowed
- Cystic lesions: In Type III, cystic changes precede fracture
- Established nonunion: In Type IV, complete pseudarthrosis with no healing potential
The hamartomatous tissue at the pseudarthrosis site prevents normal bone healing. The tissue is:
- Fibrous and avascular
- Contains abnormal cells (not true bone-forming cells)
- Creates a barrier to healing
- May be related to NF1 gene mutation (when associated)
When CPT is associated with NF1:
- NF1 gene mutation affects bone biology
- Abnormal periosteal function
- Poor vascularity
- Worse prognosis than isolated CPT
Understanding the pathology helps guide treatment - excision of hamartomatous tissue is essential.
Classification Systems
Crawford Classification (1986)
The most widely used classification, based on radiographic appearance:
- Radiographic Appearance
- Anterior bowing
- Medullary Canal
- Intact
- Treatment
- PTB brace, prophylactic rod
- Radiographic Appearance
- Anterior bowing
- Medullary Canal
- Narrowed/sclerotic
- Treatment
- PTB brace, prophylactic rod
- Radiographic Appearance
- Cystic lesion
- Medullary Canal
- Cystic changes
- Treatment
- Prophylactic rod + bone graft
- Radiographic Appearance
- Established pseudarthrosis
- Medullary Canal
- Nonunion
- Treatment
- Vascularized fibula + IM rod
Type I: Anterior bowing present, medullary canal intact. No fracture yet. Treatment: Total contact PTB brace, consider prophylactic IM rod if progressive deformity.
Type II: Anterior bowing with narrowed or sclerotic medullary canal. Fracture risk higher. Treatment: PTB brace, prophylactic IM rod often indicated.
Type III: Cystic lesion in tibia, fracture imminent. Medullary canal shows cystic changes. Treatment: Prophylactic IM rod with bone grafting to prevent fracture.
Type IV: Established pseudarthrosis - complete nonunion. No healing potential without surgery. Treatment: Vascularized fibula transfer (gold standard) combined with IM rod.
The classification guides treatment urgency and approach.
Clinical Assessment
- Anterior bowing noted at birth or early infancy
- May have history of minor trauma leading to fracture
- Family history of NF1 (if associated)
- Difficulty with weight-bearing or walking
- Previous treatment attempts (if established pseudarthrosis)
Physical Examination
- Anterior (anterolateral) bowing of tibia
- May have visible pseudarthrosis site (if Type IV)
- Limb length discrepancy (if established)
- Ankle deformity (valgus, equinus)
- Assess for NF1 features:
- Café-au-lait spots (over 6 spots over 1.5cm)
- Axillary/inguinal freckling (Crowe's sign)
- Neurofibromas
- Lisch nodules (iris examination)
- Pseudarthrosis site may be palpable (Type IV)
- Anterior bowing may be felt
- Assess for mobility at pseudarthrosis (if present)
- Ankle: May have limited dorsiflexion (equinus)
- Knee: Usually normal
- Assess for contractures
- Usually normal
- Assess for NF1-related neuropathies (rare)
- Fibular involvement (common - may also have pseudarthrosis)
- Ankle deformity (valgus, equinus)
- Limb length discrepancy
Differential Diagnosis of Anterolateral Tibial Bowing
Anterolateral bowing is the key discriminator - posteromedial bowing is a benign, self-correcting entity and must NOT be confused with CPT.
- Bowing Direction
- Anterolateral
- Key Features
- NF1 in most; dysplastic/cystic bone; progresses to fracture and nonunion
- Prognosis
- Guarded - high reconstruction failure
- Bowing Direction
- Posteromedial
- Key Features
- Calcaneovalgus foot; normal bone architecture; no fracture
- Prognosis
- Benign - corrects spontaneously, residual LLD
- Bowing Direction
- Anterolateral
- Key Features
- Absent/hypoplastic fibula, ball-and-socket ankle, lateral ray deficiency
- Prognosis
- Variable - depends on limb deficiency
- Bowing Direction
- Usually varus, symmetric
- Key Features
- Bilateral, metaphyseal changes, biochemical abnormality
- Prognosis
- Resolves with treatment of cause
- Bowing Direction
- Tibia vara (medial)
- Key Features
- Sharp focal medial cortex defect, often resolves
- Prognosis
- Generally self-limiting

Investigations
- Assess anterior bowing (characteristic)
- Evaluate medullary canal (intact, narrowed, cystic, or nonunion)
- Measure bowing angle
- Assess for pseudarthrosis (Type IV)
- Evaluate fibula (may also be affected)
- Measure limb length discrepancy
- Assess alignment
- Evaluate ankle deformity
- May help assess medullary canal status
- Evaluate cystic lesions (Type III)
- Plan surgical approach
- Assess soft tissue (hamartomatous tissue)
- Evaluate vascularity
- Plan vascularized fibula transfer
- Genetic testing (NF1 gene mutation)
- Ophthalmology examination (Lisch nodules)
- Family history assessment
- Dermatology assessment (café-au-lait spots, neurofibromas)
- May assess vascularity at pseudarthrosis site
- Less commonly used now
CALMNF1 Diagnostic Criteria
Hook:CALM diagnosis: Café-au-lait spots, Axillary freckling, Lisch nodules, and Multiple neurofibromas confirm NF1!
Treatment Approach
Treatment Philosophy
Treatment goals:
- Prevent fracture (Type I/II)
- Achieve union (Type III/IV)
- Maintain limb length
- Preserve function
- Pre-fracture (Type I/II): PTB brace, prophylactic IM rod
- Pre-fracture (Type III): Prophylactic rod + bone graft
- Established (Type IV): Vascularized fibula transfer (gold standard), IM rod, Ilizarov
- Early intervention (before fracture if possible)
- Excision of hamartomatous tissue
- Stable fixation (IM rod)
- Vascularized bone graft (best healing)
- Long-term bracing post-union
Success rate: 50-70% even with best treatment.
VIBECPT Treatment Options
Hook:VIBE with treatment: Vascularized fibula (gold standard), IM rod (stability), Bracing (prevention), and Excision (remove pathology)!
REBUILDCPT Surgical Principles
Hook:REBUILD the tibia: Remove pathology, Establish stability, Bone graft, Union goal, Ilizarov option, Long-term bracing, and Don't give up!
Surgical Techniques
Vascularized Fibula Transfer (Gold Standard)
Type IV established pseudarthrosis.
- Excision:
- Remove all hamartomatous tissue
- Debride pseudarthrosis site
- Remove abnormal periosteum
- Fibula harvest:
- Contralateral fibula (usually)
- Preserve peroneal vessels
- Length: match defect size
- Microsurgical transfer:
- Anastomose peroneal vessels to recipient vessels
- Position fibula in tibial defect
- Fixation with IM rod
- Stabilization:
- Williams telescoping rod
- Allows growth
- Maintains stability
Cast 3-6 months, then protected weight-bearing. Long-term PTB brace.
Preserves blood supply, best union rates (50-70%).


Cross-Union (4-in-1 Osteosynthesis): What the Emerging Technique Actually Is
The evidence base and the controversies section repeatedly invoke cross-union as the technique giving the highest union and lowest refracture rates (Rastogi pooled review: 100% union, 22.5% refracture, union at 4.5 months), yet the operation is easy to name and hard to picture. Cross-union deliberately abandons the goal of reconstituting a normal, separate tibia and fibula. Instead it fuses the tibia and fibula into a single broad synostosis across the pseudarthrosis level.
After radical excision of the pseudarthrosis and the surrounding dysplastic hamartomatous periosteum, the freshened tibial ends are apposed and the adjacent fibula is united to the tibia both proximal and distal to the defect. Choi and colleagues termed this "4-in-1 osteosynthesis" because the four bone ends - proximal and distal tibia, proximal and distal fibula - are grafted into one continuous mass. The result is a wide, large-cross-sectional-area load-sharing block rather than a narrow single-bone union that is prone to refracture.
- Radical resection of pseudarthrosis, sclerotic bone and the constrictive periosteal sleeve back to healthy bleeding bone.
- Autograft (iliac crest) packed into the tibiofibular interval, frequently augmented with rhBMP-2.
- Intramedullary fixation (Williams or Fassier-Duval telescoping rod) to hold alignment and share load.
- Circular/Ilizarov external fixation for compression and simultaneous correction of length and deformity.
uniting the fibula to the tibia widens the fusion mass, removes the unsupported dysplastic fibula as a source of ongoing deformity and ankle valgus, and mechanically buttresses the reconstruction. The trade-offs are loss of independent tibiofibular motion and reliance on small series with short follow-up - it is the current direction of travel, not a proven, durable gold standard.
Q: What is the "cross-union" or "4-in-1 osteosynthesis" and why is it favoured? A: It is deliberate creation of a broad tibiofibular synostosis across the pseudarthrosis - fusing the four tibial and fibular bone ends into one wide load-sharing mass after radical resection, combined with autograft/BMP, an intramedullary rod and circular fixation. The large cross-sectional union resists refracture (pooled refracture around 22%), which is why practice is converging on it despite short follow-up.
Fibular Involvement and Progressive Ankle Valgus: Why You Must Treat the Fibula
The topic notes that fibular involvement is common and that outcome studies favour procedures that address the fibula, but the mechanism and its management deserve to be spelled out, because ankle valgus is one of the commonest long-term problems in CPT.
The fibula is part of the disease, not a bystander. In many CPT cases the fibula is itself dysplastic or carries its own pseudarthrosis. Singer and Johnston showed that reconstructions fixing both tibia and fibula (their types A and B) were significantly superior to tibia-only surgery (type C), which produced no excellent results - the practical origin of the maxim "treat the fibula, not just the tibia."
- A dysplastic or ununited, shortened fibula fails to buttress the lateral ankle.
- The lateral malleolus migrates proximally, the talus tilts into valgus, and progressive ankle valgus and instability follow (El-Gammal series: mean ankle valgus around 12 degrees despite union).
- Ankle valgus compounds any limb-length discrepancy and accelerates degenerative change at the ankle.
- Achieve fibular union - restoring the lateral column (a major rationale for the cross-union/synostosis strategy) prevents progression.
- Guided growth in the skeletally immature ankle: medial distal tibial hemiepiphysiodesis (for example a medial malleolar screw) gradually corrects the valgus while growth remains.
- Distal tibiofibular synostosis (Langenskiold procedure) can stabilise the mortise and prevent proximal fibular migration.
- Supramalleolar osteotomy for fixed deformity near or after skeletal maturity.
- Long-term surveillance to skeletal maturity, since valgus and instability can recur even after tibial union.
Q: Why does ankle valgus develop in CPT and how is it addressed? A: A dysplastic or ununited, shortened fibula stops buttressing the lateral ankle, the lateral malleolus migrates proximally and the talus tilts into valgus. Address it by uniting the fibula (cross-union restores the lateral column), guided growth with a medial distal tibial hemiepiphysiodesis (medial malleolar screw) in the growing child, a Langenskiold distal tibiofibular synostosis, or a supramalleolar osteotomy for fixed deformity at maturity - which is why treating the fibula, not just the tibia, matters.
Complications
- Infection (5-10%)
- Wound healing problems
- Neurovascular injury (microsurgery)
- Graft failure (vascularized fibula)
- Hardware problems
- Persistent pseudarthrosis (30-50% failure rate)
- May require multiple surgeries
- Amputation after 3-4 failures
- Recurrent anterior bowing
- Ankle deformity (valgus, equinus)
- Limb length discrepancy
- Shortening of affected limb
- May require lengthening procedures
- Stiffness (IM rod through ankle)
- Deformity (valgus, equinus)
- May require ankle fusion
- Fibular nonunion (rare)
- Ankle instability (if too much fibula removed)
- Peroneal nerve injury
- Careful patient selection
- Meticulous surgical technique
- Adequate excision of hamartomatous tissue
- Stable fixation
- Long-term bracing
- Realistic expectations
Postoperative Care
- Pain management
- Neurovascular monitoring (especially microsurgery)
- Wound care
- Immobilization (cast, external fixator)
- Long leg cast 3-6 months
- Non-weight bearing initially
- Serial radiographs to assess healing
- Cast changes if needed
- Protected weight-bearing
- Gradual return to activities
- Long-term PTB brace (full-time initially, then part-time)
- Activity modification (avoid high-impact sports)
- Annual assessment until skeletal maturity
- Monitor for refracture
- Assess limb length discrepancy
- Evaluate ankle function
- Address complications as they arise
- PTB orthosis long-term
- May need until skeletal maturity
- Prevents refracture
- Activity modification
Outcomes and Prognosis
- Vascularized fibula transfer: 50-70%
- Autogenous iliac crest: 30-50%
- Ilizarov: 40-60%
- Overall: 50-70% with best treatment
- Early treatment (before multiple fractures)
- Adequate excision of hamartomatous tissue
- Vascularized bone graft
- Stable fixation
- NF1-negative (better than NF1-positive)
- NF1 association (worse prognosis)
- Multiple previous surgeries
- Large defect
- Poor vascularity
- Inadequate excision
- Most patients function well after union
- May have activity limitations
- Ankle problems common
- Limb length discrepancy may require lengthening
- Psychosocial support important
- Refracture risk: 20-30% even after union
- Long-term bracing often needed
- Ankle problems may require fusion
- Limb length discrepancy may worsen
- Regular follow-up essential
Guidelines, Registries & Global Practice
Global Epidemiology:
- Incidence approximately 1 in 140,000 to 250,000 live births (rare worldwide)
- NF1 prevalence in CPT pooled at 55% across the literature, but up to 84% in cohorts using strict NIH criteria with serial follow-up, because NF1 features often emerge after the CPT diagnosis (Van Royen 2016)
- Anterolateral bowing presents in infancy; bilateral disease in 10-15%
Guidance and Consensus (no formal single-society guideline exists):
- Position / Emphasis
- Resect dysplastic periosteum and hamartoma; stable fixation; treat the fibula; multidisciplinary NF1 care
- Position / Emphasis
- Charnley-Williams permanent IM rod widely used; cross-union and VFG in specialist centres
- Position / Emphasis
- All CPT children require formal NF1 assessment and genetic counselling; serial review if criteria not yet met
- Position / Emphasis
- Circular fixation for union plus simultaneous correction of LLD and deformity
- No dedicated CPT implant registry exists given rarity. Evidence is driven by pooled systematic reviews (e.g. Rastogi 2022, 1227 patients) and multicentre paediatric collaboratives rather than arthroplasty-style national registries.
- NF1 disease registries and rare-disease networks increasingly capture orthopaedic outcomes.
- High-resource settings: microsurgical VFG, BMP adjuncts, modern telescoping rods, cross-union, and combined IMR plus Ilizarov are feasible; early referral to specialist limb-reconstruction centres.
- Limited-resource settings: vascularized transfer and BMP may be unavailable; emphasis falls on non-vascularized autograft with IM rodding or Ilizarov, longer bracing, and earlier consideration of amputation with prosthetic fitting where multiple reconstructions are not feasible.
Paediatric orthopaedic surgeon, microsurgeon/plastic surgeon, clinical geneticist, physiotherapist, orthotist/prosthetist, and psychological support for child and family.
- High failure rate and likelihood of multiple operations
- Realistic union expectations and 30-50% refracture risk even after union
- Amputation framed as a functional treatment option, not a failure
- Long-term follow-up to skeletal maturity for refracture, LLD and ankle deformity
Controversies and Areas of Uncertainty
CPT is a low-volume, heterogeneous condition with no randomised trials - almost all evidence is Level III/IV. The following remain genuinely contested.
1. Is there a single "gold standard" operation? Three strategies dominate: intramedullary rodding (Charnley-Williams), Ilizarov/circular fixation, and vascularized fibular graft (VFG). The Rastogi systematic review favours combined IMR plus Ilizarov and VFG over either alone, but no head-to-head trial exists. The newer cross-union (4-in-1) technique reports the best early union and lowest refracture, yet rests on small series with short follow-up. The honest exam answer is that practice is converging on combined biological and mechanical strategies rather than any one named operation.
2. Role of biological adjuncts (BMP, bisphosphonates). The anabolic (BMP) plus anti-catabolic (bisphosphonate) concept is biologically rational given the NF1 bone phenotype, but evidence is limited to small series. rhBMP use in skeletally immature children is off-label, and a survival benefit over meticulous resection and stable fixation alone is unproven.
3. Prophylactic rodding of pre-fracture bowing (Crawford I/II). Bracing reliably delays but does not prevent fracture. Whether to insert a prophylactic telescoping rod before the first fracture is debated - it may protect the limb, but commits a young child to ankle-spanning hardware and revisions, and some series show fracture still occurs.
4. Timing of amputation. After repeated failed reconstructions with severe LLD and a stiff, deformed ankle, amputation can outperform a non-functional salvaged limb. The number of attempts before recommending amputation is not standardised and is individualised to function, family wishes and psychosocial factors.
5. Refracture and retained hardware. Refracture rates of 30-50% mean "union" is not the endpoint. Whether a load-sharing rod should be retained permanently to skeletal maturity (supported by Johnston's long-term data) versus removed is debated.
MCQ Practice Points
Q: What percentage of congenital pseudarthrosis of tibia cases are associated with neurofibromatosis type 1? A: 50-90% - CPT has a strong association with NF1. Always assess for café-au-lait spots (over 6 spots over 1.5cm), axillary freckling, Lisch nodules, and family history. NF1-positive cases have worse prognosis.
Q: What is the gold standard treatment for Crawford Type IV (established pseudarthrosis) congenital pseudarthrosis of tibia? A: Vascularized fibula transfer combined with Williams telescoping IM rod - this achieves the best union rates (50-70%). The vascularized fibula preserves blood supply, enhancing healing compared to non-vascularized grafts.
Q: What is the union rate for congenital pseudarthrosis of tibia with the gold standard treatment (vascularized fibula transfer)? A: 50-70% - even with the best treatment (vascularized fibula transfer + IM rod), union rate is only 50-70%. This reflects the challenging nature of the condition. Multiple surgeries are often needed, and amputation may be required after 3-4 failures.
Q: What is the treatment for Crawford Type I/II (pre-fracture) congenital pseudarthrosis of tibia? A: Total contact PTB (patellar-tendon-bearing) orthosis with activity modification - bracing delays but does not prevent eventual fracture. Prophylactic IM rod may be considered if deformity progresses. Early intervention is key.
Q: What is the advantage of the Williams telescoping intramedullary rod in congenital pseudarthrosis of tibia? A: Allows growth while maintaining stability - the telescoping design allows the rod to lengthen as the child grows, maintaining mechanical stability throughout growth. It is inserted through the calcaneus and talus into the tibia, though ankle stiffness is a common complication.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 2-year-old child presents with anterior bowing of the left tibia noted since birth. The child has multiple café-au-lait spots and a family history of neurofibromatosis. Radiographs show anterior bowing with intact medullary canal. How would you assess and manage this child?”
“A 5-year-old child with known CPT and NF1 presents with an established pseudarthrosis (Crawford Type IV) after a fracture 6 months ago. Previous treatment with casting failed. The pseudarthrosis site is mobile. What is your treatment approach?”
“A 10-year-old child with CPT and NF1 has undergone 3 previous attempts at reconstruction (2 vascularized fibula transfers, 1 Ilizarov) all of which failed. The pseudarthrosis persists, there is significant limb length discrepancy (8cm), and the ankle is stiff and deformed. The family is asking about further treatment options. How would you counsel them?”
Key Facts
- 50-90% associated with NF1 - always assess
- Crawford classification: Type I-IV guides treatment
- Vascularized fibula transfer is gold standard (50-70% union)
- High failure rate - multiple surgeries often needed
Crawford Classification
- Type I: Anterior bowing, intact canal = PTB brace, prophylactic rod
- Type II: Anterior bowing, narrowed canal = PTB brace, prophylactic rod
- Type III: Cystic lesion = Prophylactic rod + bone graft
- Type IV: Established pseudarthrosis = Vascularized fibula + IM rod
Treatment by Type
- Type I/II: PTB brace (delays but doesn't prevent fracture)
- Type III: Prophylactic rod + bone graft
- Type IV: Vascularized fibula transfer (gold standard) + Williams rod
- Key: Excision of hamartomatous tissue essential
Surgical Pearls
- Vascularized fibula preserves blood supply - best union rates
- Williams telescoping rod allows growth while maintaining stability
- Excision of hamartomatous tissue is critical - will fail without it
- BMP may augment healing as adjunct
Complications
- Nonunion: 30-50% failure rate even with best treatment
- Refracture: 20-30% risk even after union
- Ankle stiffness: Common with IM rod through ankle
- Amputation: 10-20% after multiple failures
Evidence Base
Surgical Options Compared - Systematic Review (Cross-Union vs Others)
- 57 studies, 1227 patients (1235 tibias) pooled
- Final union: IMR 76.5%, Ilizarov 81.5%, combined IMR+Ilizarov 92.4%, VFG 87.1%
- Refracture: IMR 48.1%, Ilizarov 47.7%, combined 33.7%, VFG 34.6%
- Cross-union: 100% union, lowest refracture (22.5%), shortest union time (4.5 months)
Charnley-Williams IM Rod - Outcomes at Skeletal Maturity
- 34 type-IV CPT followed to skeletal maturity (mean 11.9 years)
- 82% achieved a functional (grade 1 or 2) limb; all grade-3 patients requested amputation
- Procedures addressing the fibula (types A/B) were superior to tibia-only (type C)
- Refracture in 13 of 33 united cases, but only 3 failed to reheal; NF1 status did not affect outcome
Vascularized Fibular Graft + Ilizarov - Long-Term (Telescoping VFG)
- 11 Crawford type-IV NF1 patients, mean follow-up 10 years (most after multiple prior failures)
- Primary union in all cases at mean 7.2 months; LLD reduced from 7.9 cm to 2.7 cm
- Recurrent stress fractures in 82%, tibial deformity in 73%, ankle valgus mean 12 degrees
- Simultaneously treats nonunion and shortening without osteotomy of diseased bone
Prevalence of NF1 in CPT
- Pooled literature prevalence of NF1 in CPT 55.4% (95% CI 50.4-60.4%)
- Study cohort prevalence 84% (21 of 25) by NIH criteria
- NF1 features often appear only AFTER the CPT diagnosis in young children
- Recommends repeat examination and genetic counselling for all CPT patients
BMP plus Bisphosphonate as Biological Adjunct
- 8 Crawford type-IV cases (6 NF1) treated with BMP-7 plus pamidronate/zoledronic acid
- Primary healing in 6 of 8 at mean 5.5 months
- Rationale: NF1 bone shows deficient anabolism and excessive catabolism
- Concept of balancing anabolic (BMP) and anti-catabolic (bisphosphonate) effects
Ilizarov Distraction for CPT in Adults
- 14 adults (50% NF1), half with prior surgical failure
- Bone union achieved in all; LLD reduced from 11.3 cm to 1.1 cm
- AOFAS hindfoot score improved 53.5 to 63.9; success rate 92.9%
- Mean external fixation time 19.5 months