Pediatric Spine | Vertebral Anomalies | Early Onset | VACTERL Association
- Definition: Spinal deformity caused by abnormal vertebral development in utero (first 6 weeks)
- Worst Prognosis: Unilateral unsegmented bar with contralateral hemivertebra (5-10 degrees progression per year)
- Associations: High rate of associated anomalies (VACTERL) - Renal (25%), Cardiac (10%), Intraspinal (20-40%)
- MRI Mandatory: Must screen for intraspinal anomalies (tethered cord, syrinx, diastematomyelia) before surgery
- Renal Ultrasound: Mandatory screening for all patients
- “Unilateral Bar + Contralateral Hemivertebra = 'Malignant' curve (rapid progression)
- “Always check kidneys (Renal US) and heart (Echo)
- “Thoracic Insufficiency Syndrome is the main mortality risk in early onset severe curves
- “Growth potential: T1-S1 grows 10cm from age 0-5, and 10cm from 10-maturity. Fusing too early creates short trunk.
25% Association. Renal agenesis, horseshoe kidney. YOU MUST ORDER A RENAL ULTRASOUND on diagnosis. Genitourinary anomalies are the most common extraspinal association.
20-40% Association. Diastematomyelia, tethered cord, syrinx, Chiari. YOU MUST ORDER A TOTAL SPINE MRI before any corrective surgery.
10% Association. VSD, ASD, Tetralogy. Listen for murmurs and refer for Echo if suspected or syndromic.
Vertebral, Anal, Cardiac, Tracheo-Esophageal, Renal, Limb. Look for imperforate anus, thumb hypoplasia (radial deficiency).
- Progression Rate
- Less than 1° / year
- Severity
- Benign
- Management Action
- Observation
- Progression Rate
- 1-2° / year
- Severity
- Mild
- Management Action
- Observation
- Progression Rate
- 2-5° / year
- Severity
- Moderate
- Management Action
- Early surgery often required
- Progression Rate
- 5-6° / year
- Severity
- Severe
- Management Action
- Fusion of bar typically needed
- Progression Rate
- Greater than 10° / year
- Severity
- Malignant
- Management Action
- URGENT Surgery
VACTERLVACTERL Association
Hook:A child with a bad back needs checking from top (TEF) to bottom (Anus) and limbs!
TULIPProgression Risk Factors
Hook:TULIPs grow fast, and so do these curves if you miss the risk factors.
Overview and Epidemiology
Congenital Scoliosis is a lateral curvature of the spine due to vertebral malformations present at birth. Unlike idiopathic scoliosis, the deformity is structural from the outset and often rigid.
- Incidence: 0.5-1 per 1000 live births.
- No strong genetic pattern (mostly sporadic), though some familial clusters exist.
- Maternal Diabetes and valproic acid exposure are risk factors.
- Gender: Girls more common than Boys (slightly).
- Without treatment, 75% progress.
- Progression depends on the balance of growth.
- Thoracic Insufficiency Syndrome (TIS): The inability of the thorax to support normal respiration / lung growth. This is the main life-threatening complication of early onset severe deformities.
Pathophysiology and Mechanisms
Embryology
- Mesenchymal Stage (Weeks 4-6): This is when the axial skeleton forms.
- Somitogenesis: Somites form along the notochord.
- Re-segmentation: The caudal half of one somite fuses with the cranial half of the next to form a vertebra.
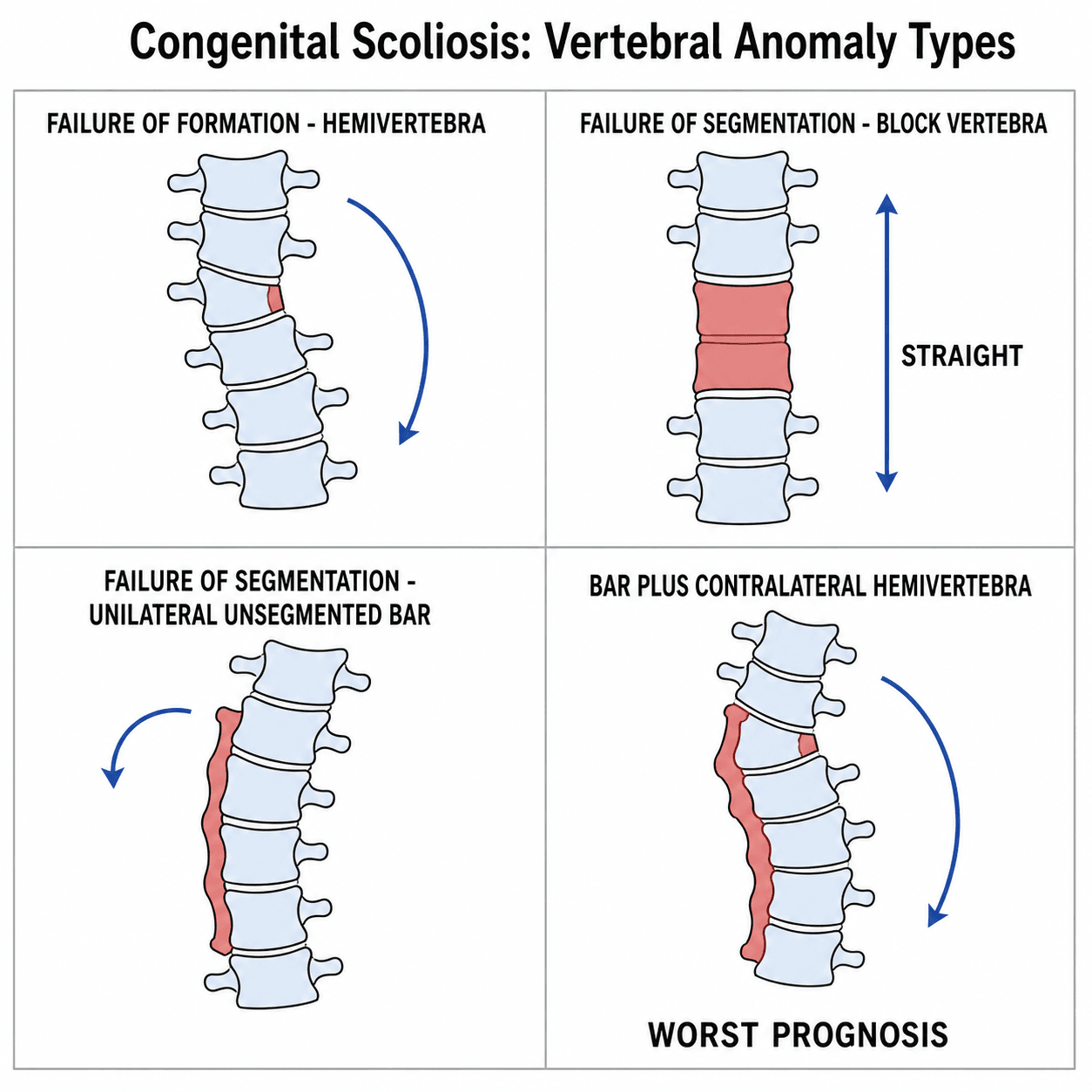
- Defects:
- Failure of Formation: Hemi-vertebra (Wedge).
- Failure of Segmentation: Unsegmented Bar (Block).
Growth Potential
- The spine grows most rapidly in the first 5 years (T1-S1 length increases 10cm) and during adolescent growth spurt (another 10cm).
- Fusion Conundrum: Fusing the thoracic spine early stops vertical growth.
- Loss of correction? No, but loss of lung volume.
- You need approx 18-22cm of T1-T12 height for adequate adult pulmonary function.
- Early fusion of greater than 4 segments in a young child can lead to TIS.
The Genetics: TBX6 Compound Inheritance
Most congenital scoliosis is sporadic, but a recognised genetic mechanism now explains a meaningful minority and is increasingly examined.
- The TBX6 compound-inheritance model: in roughly 10% of patients with isolated congenital scoliosis (vertebral malformation without a syndrome), the cause is a rare loss-of-function TBX6 variant (commonly a 16p11.2 microdeletion) on one allele combined with a common hypomorphic TBX6 risk haplotype on the other - a "compound heterozygosity" that drops TBX6 dosage below the threshold needed for normal somite segmentation. Because neither allele alone causes disease, inheritance looks sporadic.
- Pathway: TBX6 acts in the Notch / segmentation-clock machinery that drives somitogenesis - the same pathway whose disruption (DLL3, MESP2, LFNG, HES7) causes spondylocostal dysostosis.
- Why it matters: identifying a 16p11.2 deletion has counselling implications (it also carries developmental and neuropsychiatric associations) and frames congenital scoliosis as a dosage-sensitive developmental disorder rather than a purely random event.
Q: A child has isolated congenital scoliosis with no family history - what is the best-characterised genetic mechanism? A: TBX6 compound inheritance - a rare null TBX6 allele (commonly a 16p11.2 microdeletion) together with a common hypomorphic TBX6 haplotype on the other chromosome, reducing TBX6 dosage below the segmentation threshold. It accounts for about 10% of isolated cases; because neither allele alone is sufficient, the pattern appears sporadic. TBX6 acts in the Notch/segmentation-clock somitogenesis pathway.
Classification
Winter's Classification (Based on X-ray)
Type I: Failure of Formation
- Incarcerated Hemivertebra: Only pedicles are deformed, body is set into the spine. Slow progression.
- Fully Segmented Hemivertebra: Disc space above and below. Acts as a growing wedge. Rapid progression.
- Semi-segmented: Fused to one adjacent vertebra.
- Wedge Vertebra: Partial formation failure.
Type II: Failure of Segmentation
- Block Vertebra: Bilateral failure. Stable, short segment. No treatment usually.
- Unilateral Unsegmented Bar: Unilateral failure. The fused side doesn't grow, the open side does. Very bad prognosis.
Type III: Mixed
- Combination of both.
- Unilateral Bar + Contralateral Hemi: The "Malignant Curve". The bar tethers one side, the hemivertebra pushes growth on the other. Rapid relentless progression.
Classification dictates urgency.
The Sagittal Counterpart: Congenital Kyphosis
Congenital vertebral anomalies also cause deformity in the sagittal plane - congenital kyphosis - graded by the same formation/segmentation logic but carrying a distinct and dangerous complication: it is the commonest congenital cause of paraplegia.
- Anomaly
- Failure of FORMATION (posterior/posterolateral vertebral-body defect)
- Behaviour / risk
- Most progressive AND highest risk of paraplegia - the apex angulates sharply over the cord
- Anomaly
- Failure of SEGMENTATION (anterior unsegmented bar)
- Behaviour / risk
- Slower, more rounded progression; lower (but not zero) paralysis risk
- Anomaly
- Mixed
- Behaviour / risk
- Variable
- Why Type I is dangerous: the deficient vertebral body lets the kyphosis angulate acutely at the apex, draping the cord over the deformity - progressive Type I kyphosis can produce a gradual spastic paraparesis.
- Treatment: early posterior fusion can arrest a small Type I curve in a very young child; an established or larger deformity needs combined anterior and posterior fusion (with anterior decompression if neurology is present). Bracing does not work.
Q: Which congenital spinal anomaly most often causes paraplegia, and why? A: Type I congenital kyphosis (failure of formation) - the deficient vertebral body lets the spine angulate sharply at the apex, draping the cord over the kyphos and producing progressive cord compression. It warrants early fusion (posterior alone if small and young, combined anterior-posterior if established), unlike the more benign segmentation-failure (Type II) kyphosis.
Clinical Assessment
Assessment Protocol
- Cutaneous markers of dysraphism: Hairy patch, dimple, sinus, hemangioma.
- Shoulder balance, Trunk shift.
- Facial asymmetry (Goldenhar).
- Limb deformities (Radial clubhand - VACTERL).
- Detailed lower limb neuro exam.
- Reflexes (Abdominal reflexes often absent in extensive syrinx).
- Ankle clonus (Tethering).
- Cardiovascular exam (Murmurs).
- History of renal issues or UTIs.
- Anal patency.
Always look at the skin over the spine. A hairy patch (faun's beard) or deep dimple is highly suggestive of underlying spinal dysraphism (spina bifida occulta, diastematomyelia).
Investigations
- Indication
- First line
- What to look for
- Count vertebrae, identify bars/hemis, measure Cobb angle.
- Indication
- Mandatory
- What to look for
- Renal agenesis (25%).
- Indication
- Mandatory pre-op
- What to look for
- Tethered cord, Syrinx, Diastematomyelia, Chiari.
- Indication
- Pre-op planning
- What to look for
- Visualize complex bony anatomy, pedicle morphology for screws.
- Indication
- Mandatory
- What to look for
- Cardiac flow anomalies.
The Spur Must Go First. If a bony spur (diastematomyelia) is present, you cannot distract/straighten the spine until it is excised. Distraction against a spur will split the cord (neurological catastrophe).



Differential Diagnosis
The key task is to distinguish congenital scoliosis (structural vertebral malformation present at birth) from other early-onset curves, because management and prognosis differ sharply. The defining feature is an identifiable vertebral anomaly (hemivertebra, bar, block) on plain films - not simply an early or rigid curve.
- Distinguishing feature
- Discrete vertebral anomaly (hemivertebra/bar/block) on radiograph
- Response to bracing
- Poor (rigid, structural)
- Pitfall
- Missing intraspinal anomaly on MRI before correction
- Distinguishing feature
- Normal vertebral morphology; rib-vertebra angle difference (Mehta) guides risk
- Response to bracing
- Many resolve; serial casting effective if progressive
- Pitfall
- Labelling a progressive curve idiopathic without ruling out a subtle hemivertebra
- Distinguishing feature
- Long C-shaped curve, pelvic obliquity, underlying CP/SMA/DMD
- Response to bracing
- Limited; postural seating support
- Pitfall
- Attributing a syndromic child's curve solely to vertebral anomaly
- Distinguishing feature
- Cafe-au-lait spots, short sharp dystrophic curve, rib penciling
- Response to bracing
- Poor in dystrophic curves
- Pitfall
- Treating an NF-1 dystrophic curve as routine congenital deformity
- Distinguishing feature
- Multiple, generalized segmentation defects with rib fusions (TBX6/DLL3)
- Response to bracing
- Poor; high TIS risk
- Pitfall
- Calling diffuse multi-level segmentation a single congenital curve
Management Algorithm
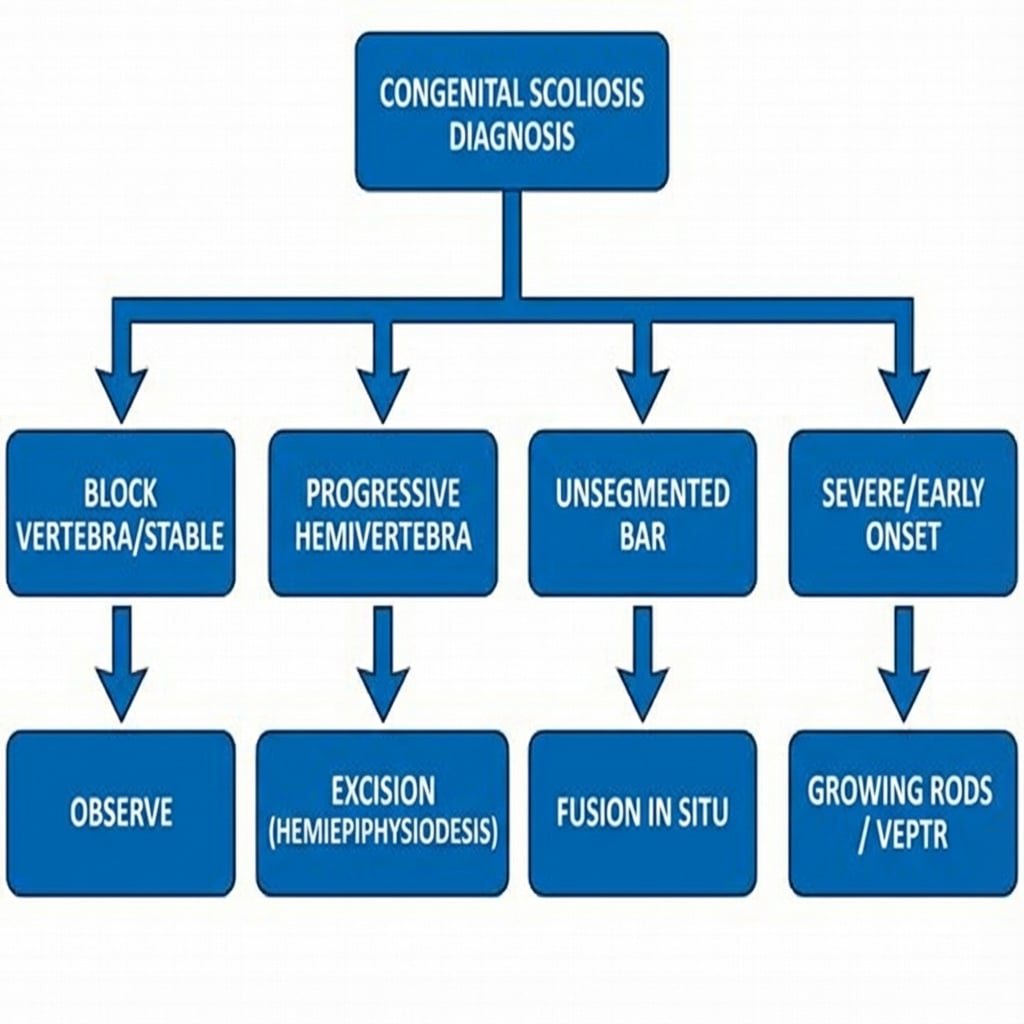
Observation
- Indications: non-progressive curves, block vertebrae, balanced deformities.
- Protocol: X-ray every 6-12 months during growth.
Bracing?
- Role: Limited to NONE.
- Congenital curves are rigid and do not respond to bracing.
- Exception: Occasionally used to control compensatory curves above/below the congenital defect to delay surgery.
Observation requires strict radiographic intervals.
Surgical Technique
Posterior Fusion of Unsegmented Bar
Goal: Stop the "bad" side from not growing? No, stop the good side? Actually, treating a bar involves fusing the bar to stop any growth, and often fusing the convex (growing) side? No.
Correct Logic: An unsegmented bar has NO growth plates. The contralateral side has normal growth plates. This causes the curve. Surgery: Convex Epiphysiodesis. Stop the growth on the convex (healthy) side to match the lack of growth on the concave (bar) side.
- Approach: Posterior or combined A/P.
- Ablate the growth plates/discs on the convex side.
- Apply fusion mass.
- Result: arrest of progression (maybe some auto-correction).
Early intervention prevents severe deformity.
STOPSurgical Goals
Hook:STOP the curve to save the lungs.
Complications
- Risk Factor
- Osteotomy, Diastematomyelia distraction
- Management
- IOM monitoring. Wake up test. Remove spurs first.
- Risk Factor
- Posterior fusion with open anterior growth plates in young child
- Management
- Add anterior fusion or exclude growth plates.
- Risk Factor
- Long revisions, syndromes
- Management
- Washout, antibiotics.
- Risk Factor
- Growing rods, poor bone stock
- Management
- Revision.
- Risk Factor
- Proximal Junctional Kyphosis
- Management
- Extension of fusion.
Postoperative Care and Rehabilitation
Protocol
- ICU observation (neuromonitoring considerations).
- Pain control.
- Mobilize as tolerated (no brace usually needed if rigid fixation).
- Wound checks.
- Return to school.
- No impact sports.
- X-ray to assess arthrodesis.
- Gradually increase activity.
- Monitor for Crankshaft (if young).
- Monitor for PJK.
- Lung function tests.
Outcomes
Prognosis:
- Hemivertebrae: Excision yields excellent correction and balance.
- Unsegmented Bars: Early convex epiphysiodesis can halt progression but rarely corrects deformity substantially.
- Untreated: Can lead to severe deformity (greater than 100 degrees), Cor Pulmonale, and early death from respiratory failure.
Guidelines, Registries & Global Practice
Global epidemiology:
- Incidence approximately 0.5-1 per 1000 live births worldwide; one of the commonest causes of structural scoliosis presenting in infancy.
- Largely sporadic; environmental contributors (maternal pregestational diabetes, valproate, gestational hypoxia/carbon monoxide in experimental models) and genes affecting somitogenesis (e.g. the Notch/segmentation-clock pathway, TBX6 in spondylocostal/multiple-vertebral-segmentation phenotypes) are implicated.
- Slight female predominance; high rate of associated VACTERL, intraspinal, cardiac and renal anomalies across all populations.
Side-by-side guidance (no single national standard exists for this rare condition; principles are shared):
- Screening emphasis
- Whole-spine MRI, echo and renal US routine at diagnosis; PFTs before/after early surgery
- Treatment philosophy
- Growth-sparing constructs favoured under age 8-10; early short-segment resection for progressive hemivertebrae
- Screening emphasis
- MRI plus cardiac and renal imaging; multidisciplinary tertiary pathway
- Treatment philosophy
- Document progression before fusing; MAGEC and casting in early-onset disease
- Screening emphasis
- MRI mandatory before any correction; CT 3D for bony planning
- Treatment philosophy
- Posterior-only hemivertebra resection well established; VCR reserved for rigid late deformity
- Screening emphasis
- Plain radiographs and clinical screening; MRI/echo where available
- Treatment philosophy
- Later, often larger presentations; in-situ fusion and convex epiphysiodesis when implants/MRI scarce
- There is no implant-survival registry specific to congenital scoliosis the way NJR/AJRR/AOANJRR exist for arthroplasty; growth-friendly implant data come from collaborative early-onset-scoliosis databases (e.g. the Pediatric Spine Study Group / Growing Spine Study Group), which track rod fractures, anchor failure, infection and the law of diminishing returns with repeated lengthening.
- These collaboratives, not national joint registries, are the main source of comparative MAGEC vs traditional growing-rod and VEPTR outcome data.
- High-resource: MRI/echo/renal US at diagnosis, intra-operative neuromonitoring, 3D-CT planning, MAGEC rods to reduce repeat anaesthetics.
- Limited-resource: later presentation with larger rigid curves, restricted MRI access (raising the threshold before any distraction because diastematomyelia may be undetected), and greater reliance on in-situ fusion or convex hemiepiphysiodesis. Where MRI is unavailable, intra-operative neuromonitoring and a low threshold for the Stagnara wake-up test become even more important.
every child with confirmed congenital scoliosis should be managed by a paediatric spine service. A generalist may appropriately initiate screening imaging (whole-spine radiographs, renal ultrasound) but should not undertake correction.
Controversies & Areas of Uncertainty
Early excision (age 2-4) gives a short fusion and lets compensatory curves self-correct, but carries the anaesthetic and neurological risk of operating on tiny pedicles. Some advocate watchful waiting until documented progression. The balance shifts toward earlier surgery for fully segmented lumbosacral hemivertebrae causing trunk decompensation.
Magnetically controlled rods avoid repeated open lengthenings and anaesthetics, but face metallosis, titanium wear debris, lock-pin failure and the same law of diminishing returns. Whether they truly reduce total complications versus traditional rods remains debated and is tracked by early-onset-scoliosis collaboratives rather than randomized trials.
The need for routine anterior fusion to prevent crankshaft after posterior fusion in a skeletally immature child is contested; pedicle-screw constructs with robust posterior arthrodesis may reduce, but not abolish, the phenomenon.
Whether an asymptomatic low-lying conus or filum lipoma must be released before deformity correction, or simply monitored, is unsettled. A bony diastematomyelia spur, however, must be excised before any distraction - this is not controversial.
MCQ Practice Points
Q: What is the most common intraspinal anomaly associated with congenital scoliosis? A: Diastematomyelia (Split cord malformation), followed by tethered cord and syrinx.
Q: Rank the following from worst to best prognosis: Block Vertebra, Fully Segmented Hemivertebra, Unilateral Bar + Contralateral Hemi. A: Worst: Bar + Contralateral Hemi. Middle: Fully Segmented Hemi. Best: Block Vertebra.
Q: How many features are needed to diagnose VACTERL association? A: Typically at least 3 of the 6 features (Vertebral, Anal, Cardiac, TE, Renal, Limb).
Q: Why is an MRI mandatory before casting or surgery in congenital scoliosis? A: To rule out intraspinal anomalies (e.g. syrinx, tethering). Correcting the curve stretches the spinal canal; if the cord is tethered, this stretch causes ischemia and paraplegia.
Q: What is the classic triad of Klippel-Feil syndrome? A: 1. Low posterior hairline. 2. Short neck ("Webbed"). 3. Limited cervical range of motion.
Q: A child with scoliosis has ear tags and facial asymmetry. What is the diagnosis? A: Goldenhar Syndrome (Oculo-auriculo-vertebral spectrum).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A newborn baby is noted to have a spinal deformity. X-ray shows a hemivertebra at L1. The parents ask if surgery is needed now.”
“A 6-year-old boy presents with a worsening thoracolumbar curve. X-rays show a unilateral unsegmented bar on the left from T10-L2 with multiple hemivertebrae on the right.”
“You are performing a hemivertebra excision. During the osteotomy, the neuromonitoring signals (MEPs) drop bilaterally.”
VACTERL Checklist
- Vertebral (X-ray)
- Anal (Exam)
- Cardiac (Echo)
- TE (History/Swallow)
- Renal (Ultrasound)
- Limb (Radius exam)
McMaster Prognosis
- Block: Benign
- Wedge: Mild
- Hemi: Moderate
- Bar: Severe
- Bar+Hemi: Malignant
Key Principle
- MRI before Surgery/Bracing
- Renal US for everyone
- Preserve lung volume (TIS risk)
- Don't fuse greater than 4 segments early
- Check for Diastematomyelia spur
Evidence Base
Natural History of Congenital Scoliosis
- Seminal study of 251 patients with congenital scoliosis followed over time
- Defined the hierarchy of progression by anomaly type
- Worst prognosis: unilateral unsegmented bar with a contralateral hemivertebra (the 'malignant' curve)
- Best prognosis: block vertebra (essentially non-progressive)
Posterior Hemivertebra Resection (Innovative Technique)
- 21 consecutive young children: posterior-only hemivertebra resection with transpedicular instrumentation
- Mean main-curve Cobb angle improved from 41 degrees pre-op to 14 degrees post-op (maintained at 15 degrees)
- Mean kyphosis improved from 24 degrees to 11 degrees
- Complications limited to one infection, one pedicle fracture, two early wire-instrument failures; no permanent neurological injury
Thoracic Insufficiency Syndrome (TIS)
- Defined TIS as the inability of the thorax to support normal respiration or lung growth
- Described the three-dimensional 'windswept' thoracic deformity of fused ribs plus congenital scoliosis
- Introduced the thumb-excursion test and 'space available for lung' as clinical/radiographic markers
- Treatment goal: acutely increase thoracic volume and maintain it during growth, ideally without spine fusion (rationale for VEPTR)