From functional assessment to multilevel reconstruction
- Start with function and goals: walking distance, aids, falls, pain, fatigue, stairs, transfers, school participation and family priorities.
- Classify the child after assessment: distribution of involvement, movement disorder, GMFCS level, gait pattern and lever-arm status.
- Separate dynamic spasticity from fixed contracture, weakness, poor selective control, torsion and compensation before selecting treatment.
- The key sagittal patterns in spastic diplegia are true equinus, jump gait, apparent equinus and crouch gait.
- SEMLS is not multiple releases on one day; it is gait-analysis-informed correction of the whole kinetic chain with a long rehabilitation plan.
- “GMFCS is assigned from observed and reported functional mobility; it is not a single history question.
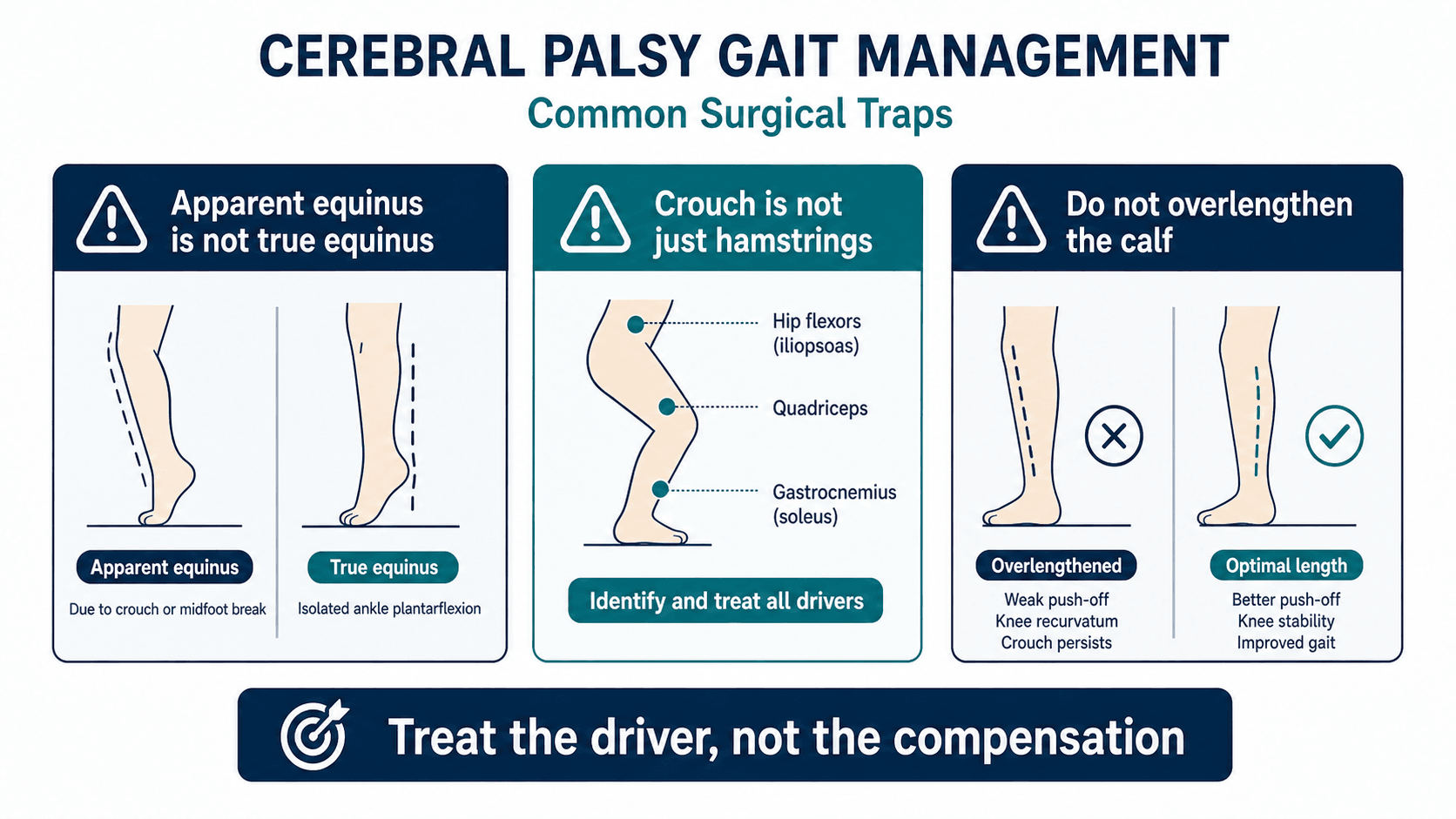
- “Toe walking may be true equinus, jump gait, apparent equinus, dystonia, short-limb compensation or balance strategy.
- “Crouch gait is multifactorial: weak plantarflexors, patella alta, knee flexion contracture, planovalgus, torsion and previous overlengthening may matter more than hamstrings.
- “A gait lab report supports clinical reasoning. It is not an operation list.
The common error in cerebral palsy gait is to operate on the most obvious deformity instead of the primary driver. Achilles lengthening for apparent equinus and isolated hamstring lengthening for multifactorial crouch are classic examples.
Images and Diagrams



Gait Decision Framework
The modern literature is consistent on the core message: cerebral palsy gait should be understood as a whole-limb mechanical problem, not as a list of tight muscles. SEMLS studies, gait-analysis reviews and crouch-gait papers repeatedly support the same practical sequence: define the functional goal, classify the gait pattern, identify fixed deformity and lever-arm dysfunction, choose procedures that match the drivers, and plan rehabilitation as part of the treatment.
- What the literature supports
- GMFCS is a reliable gross motor function classification, but it does not define the gait deformity
- Practical use
- Use it to frame goals and prognosis, then assess gait separately
- What the literature supports
- Sagittal pattern systems help separate true equinus, jump gait, apparent equinus and crouch
- Practical use
- Name the pattern before choosing calf, hamstring or bony surgery
- What the literature supports
- Gait analysis improves understanding of kinematics, kinetics, EMG timing and compensations
- Practical use
- Use it to reconcile clinical examination with surgical planning
- What the literature supports
- Crouch is multifactorial; hamstrings are not always the main problem
- Practical use
- Look for patella alta, weak plantarflexors, planovalgus, torsion and fixed knee flexion
- What the literature supports
- Systematic reviews show improvements in gait parameters, but outcomes vary with selection, procedure choice and rehabilitation
- Practical use
- Counsel families about goals, recovery and possible revision rather than promising normal gait
SEMLS evidence at a glance
- Pooled analysis showed multilevel surgery improved gait (Gait Profile Score; SMD -0.80, 95% CI -0.95 to -0.65) but did not change gross motor function (SMD 0.38, 95% CI -0.25 to 1.01) or gait speed (SMD 0.12, 95% CI -0.01 to 0.25).
- Only one of 74 included studies was a randomised controlled trial; the remainder were cohort studies.
- Participation, quality of life and adverse events were inadequately reported in most studies.
- Practical answer
- Better endurance, fewer falls, less pain, brace tolerance, easier care or improved participation
- Why it matters
- Treatment should be judged against function, not cosmetic appearance
- Practical answer
- Distribution, movement disorder, GMFCS, gait pattern and lever-arm status
- Why it matters
- This turns observation into a management framework
- Practical answer
- Spasticity, contracture, weakness, poor selective control, torsion and compensation
- Why it matters
- Each has different treatment logic
- Practical answer
- Complex ambulant CP, especially before SEMLS
- Why it matters
- It reveals hidden drivers and reduces guesswork
- Practical answer
- A single coordinated multilevel correction plus rehabilitation pathway
- Why it matters
- It avoids repeated isolated operations and repeated recovery cycles
GOALSStart With Function
Hook:GOALS prevents the assessment becoming a list of operations.
T-C-W-LDrivers of Abnormal Gait
Hook:T-C-W-L asks why the gait pattern exists before deciding what to treat.
SEMLSSingle-Event Multilevel Surgery
Hook:SEMLS is a planning philosophy, not a theatre list.
Overview/Epidemiology
Cerebral palsy gait is a dynamic, multiplanar orthopaedic problem. The brain lesion is non-progressive, but the musculoskeletal consequences progress because the child grows through abnormal tone, muscle imbalance, weakness, impaired motor control and altered loading. A toddler with dynamic equinus may become a school-aged child with fixed calf contracture, tibial torsion, planovalgus, knee flexion contracture, patella alta and increasing energy cost.
The central idea is that CP gait is rarely a single tight muscle. A visible abnormality may be the primary pathology, a compensation, or the only mechanism keeping the child upright.
- Possible drivers
- True ankle equinus, apparent equinus from proximal flexion, dystonia, short-limb compensation, poor balance or learned strategy.
- Why it matters
- Achilles lengthening helps only selected true equinus and may worsen crouch if the diagnosis is wrong.
- Possible drivers
- Weak plantarflexors, knee flexion contracture, patella alta, planovalgus, external tibial torsion, hamstring overactivity, previous Achilles overlengthening or poor selective control.
- Why it matters
- Isolated hamstring lengthening may fail if lever-arm dysfunction is the main driver.
- Possible drivers
- Femoral anteversion, internal tibial torsion, foot deformity or compensation.
- Why it matters
- Derotation decisions should match functional gait findings, not a single static measurement.
SEMLS developed to avoid repeated isolated operations. Treating equinus one year, hamstrings another year and femoral anteversion later can create sequential imbalance and repeated rehabilitation cycles. SEMLS aims to correct clinically important fixed deformities and lever-arm dysfunctions together, once the gait pattern is sufficiently understood and the child can participate in rehabilitation.
Cerebral palsy is the most common cause of lifelong physical disability beginning in childhood. Orthopaedic gait surgery mainly concerns ambulant children, particularly those with spastic diplegia or hemiplegia and GMFCS I to III function. In non-ambulant children, orthopaedic priorities often shift toward hip surveillance, sitting, hygiene, pain, skin protection, transfers and care.
The practical learning sequence is:
- Define the functional problem.
- Classify function and gait pattern.
- Identify dynamic tone, fixed contracture, weakness, torsion, foot deformity and compensation.
- Decide whether non-operative care, tone management, orthoses, surgery or surveillance best matches the goal.
- If surgery is required, plan the whole limb and rehabilitation pathway.
Definition of SEMLS
Single-event multilevel surgery is the planned correction of clinically important musculoskeletal deformities at multiple anatomical levels during one operative episode. In ambulant CP, it is usually planned from clinical examination, radiographs, rotational assessment and instrumented gait analysis.
A concise definition:
SEMLS is a gait-analysis-informed single-stage strategy for ambulant children with cerebral palsy, designed to correct fixed soft-tissue contractures and bony lever-arm dysfunctions at the hip, knee, tibia, ankle and foot, with one coordinated rehabilitation pathway.
The phrase "single-event" does not mean every abnormality must be treated. It means the clinically relevant fixed deformities that drive the gait problem are corrected together where this is safer and more logical than serial isolated surgery.
SEMLS is not a random package of releases. It is not a response to a gait-lab printout alone. It is not appropriate for every child with CP. It is a selected reconstruction plan for a selected child with a defined functional goal.
What This Topic Covers
This topic is organised around the decisions that make cerebral palsy gait assessment safe and useful:
- Explain why CP gait deteriorates despite a static neurological lesion.
- Classify common gait patterns in spastic diplegia and hemiplegia.
- Distinguish true equinus, jump gait, apparent equinus and crouch gait.
- Describe how GMFCS is assigned from function.
- Interpret the major outputs of instrumented gait analysis.
- Match SEMLS procedures to deformity, gait pattern and lever-arm dysfunction.
- Avoid the major overcorrection traps: calcaneus after Achilles lengthening and worsening crouch after inappropriate lengthening.
- Explain SEMLS to a family in practical terms.
Essential Gait Biomechanics
Normal gait cycle
Normal gait is usually divided into stance and swing. Stance occupies roughly 60 percent of the gait cycle and includes initial contact, loading response, midstance, terminal stance and pre-swing. Swing occupies roughly 40 percent and includes initial swing, mid-swing and terminal swing.
Efficient gait needs:
- Heel strike or controlled initial contact.
- Controlled tibial progression over a stable foot.
- Adequate stance-phase knee extension without recurvatum or collapse.
- Hip extension in terminal stance.
- Heel rise and plantarflexion power in terminal stance and pre-swing.
- Adequate knee flexion in swing for foot clearance.
- Controlled terminal swing knee extension.
- Balanced pelvic motion with limited compensatory trunk movement.
Why CP disrupts gait
The child with CP loses gait efficiency when tone, weakness, contracture and skeletal alignment disturb the normal sequence.
- Effect on gait
- Poor push-off and reduced stance-phase knee extension moment.
- Treatment implication
- Avoid overlengthening the calf and worsening crouch.
- Effect on gait
- Foot cannot act as a stable lever.
- Treatment implication
- Foot stabilisation or orthotic strategy may be needed before gait improves.
- Effect on gait
- Foot lever points away from the line of progression.
- Treatment implication
- Tibial derotation may be needed when lever-arm failure drives crouch.
- Effect on gait
- Hip internal rotation and altered knee progression.
- Treatment implication
- Consider femoral derotation when gait analysis and examination agree.
- Effect on gait
- Limits knee extension.
- Treatment implication
- Lengthen only when contracture is a true driver, not a compensatory stabiliser.
CP gait is a kinetic-chain problem
A deformity at one level changes the apparent problem elsewhere.
- Visible gait effect
- Absent heel strike
- Clinical trap
- Misdiagnosing apparent equinus as true calf equinus
- Visible gait effect
- Anterior pelvic tilt and lumbar lordosis
- Clinical trap
- Missing the proximal driver while focusing on the ankle
- Visible gait effect
- Poor push-off and crouch tendency
- Clinical trap
- Blaming hamstrings alone
- Visible gait effect
- Weak push-off and midfoot break
- Clinical trap
- Treating calf weakness without restoring the foot lever
- Visible gait effect
- Extensor lag and crouch
- Clinical trap
- Using hamstring lengthening without restoring the extensor mechanism
- Visible gait effect
- Reduced swing-phase knee flexion
- Clinical trap
- Trying to fix stiff knee gait with hamstring surgery
Natural History of Gait Deterioration and Timing of SEMLS
The brain lesion is static, but the topic's recurring theme is that the GAIT deteriorates because the child grows through abnormal tone, weakness and lever-arm dysfunction. Understanding this trajectory is what determines WHEN to intervene.
- What happens
- Dynamic spasticity (for example dynamic equinus); the gait pattern is still evolving
- Implication for timing
- Non-operative tone management (botulinum toxin, serial casting, orthoses); gait analysis is less reliable and soft-tissue lengthenings recur with growth, so avoid early irreversible surgery
- What happens
- The gait pattern matures and becomes reproducible; fixed contracture and lever-arm dysfunction declare themselves
- Implication for timing
- The usual window for gait-analysis-informed SEMLS when deformity is fixed and functionally important
- What happens
- Rising body mass and longer levers outstrip plantarflexor and quadriceps strength - the crouch crisis, when weak muscles can no longer sustain a toe-walking pattern
- Implication for timing
- High-risk window for rapid crouch collapse; act before crouch and bony deformity become fixed and irreversible
- What happens
- High energy cost of crouch; a proportion of GMFCS II-III walkers lose efficient or independent ambulation
- Implication for timing
- Preserving ambulation and energy efficiency is a central goal of well-timed surgery
Cerebral palsy is a non-progressive brain lesion, but the GAIT deteriorates because the child grows through abnormal tone, weakness and lever-arm dysfunction. The dangerous window is the pubertal growth spurt, when rising body mass and longer levers outstrip plantarflexor and quadriceps strength and a toe-walking or jump-gait child can collapse into high-energy crouch - the crouch crisis. This drives SEMLS timing: too early and the gait pattern is unreliable to interpret while soft-tissue lengthenings recur with growth; too late and crouch and bony deformity become fixed and a proportion of children lose efficient community walking. The usual target is once the gait pattern is mature and the deformity is fixed and functionally important - commonly around school age - and before adolescent crouch collapse.
Pathophysiology
CP gait abnormalities arise from neurological and musculoskeletal factors acting together.
Neurological contributors
- Spasticity: velocity-dependent resistance to stretch.
- Dystonia: involuntary fluctuating postures or movements.
- Co-contraction: simultaneous activation of antagonists, reducing smooth motion.
- Poor selective motor control: inability to isolate hip, knee, ankle and foot movement.
- Weakness: particularly hip extensors, hip abductors, quadriceps, dorsiflexors and plantarflexors.
- Impaired balance: abnormal trunk and pelvic strategies.
- Motor learning differences: persistence of inefficient movement patterns after deformity correction.
Musculoskeletal contributors
- Muscle-tendon contracture.
- Joint contracture.
- Femoral anteversion.
- Tibial torsion.
- Patella alta and extensor mechanism insufficiency.
- Planovalgus or equinovarus foot deformity.
- Hip displacement and pelvic obliquity.
- Scoliosis or spinal imbalance.
Lever-arm dysfunction
Muscles need stable skeletal levers. Even strong muscles cannot work efficiently if the lever is malaligned.
- Femoral anteversion changes hip rotation and reduces efficient abductor mechanics.
- External tibial torsion externally rotates the foot lever and weakens the plantarflexion-knee-extension couple.
- Planovalgus shortens and destabilises the foot lever.
- Midfoot break allows collapse rather than push-off.
- Patella alta reduces the effectiveness of the quadriceps mechanism and contributes to extensor lag.
This is why bony correction and foot reconstruction may be more important than additional soft-tissue lengthening in selected children.
Sagittal Gait Patterns in Spastic Diplegia

The Rodda and Graham sagittal classification is useful because it links observed gait to treatment reasoning. It should not replace full assessment.
Definition
True equinus means ankle plantarflexion during stance. The ankle is plantarflexed relative to the tibia, and the forefoot commonly contacts first.
Posture
- Hip relatively extended.
- Knee relatively extended or sometimes recurvatum.
- Ankle plantarflexed.
- Forefoot initial contact.
- Heel may not reach the ground.
Drivers
- Dynamic gastrocnemius or soleus spasticity.
- Fixed gastrocnemius contracture.
- Fixed gastrocsoleus contracture.
- Equinovarus foot.
- Dystonia or poor motor control.
Assessment
Examine passive ankle dorsiflexion with the knee flexed and extended, perform the Silfverskiold test, assess hindfoot position, check for midfoot break, and decide whether equinus is needed for stability.
Treatment logic
Dynamic equinus may respond to therapy, orthoses, botulinum toxin or serial casting. Fixed gastrocnemius contracture may need gastrocnemius recession. Fixed gastrocsoleus contracture may need tendo-Achilles lengthening in selected cases, but overlengthening can cause calcaneus and crouch.
Hemiplegic Gait Patterns
Hemiplegic gait is commonly described using the Winters, Gage and Hicks pattern. The value is not memorising labels; it is linking the involved levels to treatment.
- Main abnormality
- Drop foot in swing
- Typical features
- Ankle is usually acceptable in stance but dorsiflexion is inadequate in swing
- Treatment logic
- AFO, strengthening, functional electrical stimulation in selected cases
- Main abnormality
- Equinus in stance and swing
- Typical features
- Forefoot contact, possible recurvatum in type IIB
- Treatment logic
- Calf procedure only if fixed contracture and clinically indicated
- Main abnormality
- Equinus plus stiff knee
- Typical features
- Reduced swing knee flexion, toe drag, rectus femoris overactivity may contribute
- Treatment logic
- Calf correction plus rectus femoris transfer only when gait analysis supports it
- Main abnormality
- Multilevel involvement
- Typical features
- Hip flexion, adduction/internal rotation, stiff knee and equinus
- Treatment logic
- Often needs multilevel assessment and selected SEMLS
Functional Classification
Distribution and movement disorder
Begin by describing the child, not the operation.
- Spastic hemiplegia: one side predominantly involved, often with equinus or equinovarus, drop foot in swing, stiff knee gait or internal rotation gait.
- Spastic diplegia: both lower limbs involved, usually with relative upper limb sparing, commonly showing equinus, jump gait, apparent equinus, crouch, scissoring, internal rotation and planovalgus.
- Quadriplegia: all four limbs involved; gait surgery is less often the primary goal and orthopaedic care commonly focuses on hips, sitting, spine, hygiene, comfort and transfers.
- Dyskinetic or dystonic CP: variable posture and tone may make SEMLS outcomes less predictable if dystonia is dominant.
GMFCS from real-world function
GMFCS is assigned or confirmed from observed and reported function. It is based on what the child can do in daily life, with emphasis on sitting, transfers and mobility.
Build the level from functional questions:
- Does the child walk indoors, outdoors and at school?
- Are stairs possible, and is a rail required?
- Does the child use AFOs, crutches, a walker or a wheelchair?
- How far can the child walk before fatigue?
- Does the child fall?
- Can the child keep up with peers?
- Are transfers independent?
- Has function declined with growth?
- Is pain limiting walking?
Then classify:
- GMFCS I: walks without major limitations, but speed, balance, running and jumping may be impaired.
- GMFCS II: walks without handheld mobility devices but has limitations with distance, uneven ground, crowds, inclines or speed.
- GMFCS III: walks with a handheld mobility device and often uses wheeled mobility for longer distances.
- GMFCS IV: self-mobility is limited; powered mobility or substantial assistance is often required.
- GMFCS V: transported in a manual wheelchair, with severe limitations in head and trunk control.
The common gait-improvement SEMLS group is ambulant CP, especially GMFCS I to III. GMFCS IV and V children may still need orthopaedic surgery, but the goals are usually comfort, sitting, hygiene, hip containment, standing transfers and care rather than efficient community walking.
Describe the child's actual mobility, aids, endurance, falls, stairs and participation. Then assign GMFCS. Do not treat GMFCS as something the family simply tells you.
Clinical Assessment
History: define the lived problem
The history should explain why the child is presenting now.
- Main concern: tripping, fatigue, pain, loss of walking, brace intolerance, cosmetic concern, hygiene, transfers or school participation.
- Function: indoor walking, outdoor walking, stairs, playground, sport, endurance and community mobility.
- Mobility aids: AFO type, walker, crutches, wheelchair, night splints and tolerance.
- Falls: frequency, direction, triggers and injuries.
- Pain: hip, knee, foot, back, brace pressure or post-activity pain.
- Fatigue: distance before stopping, end-of-day deterioration and recovery time.
- Development: prematurity, neonatal history, milestones and cognitive or communication needs.
- Neurology: seizures, dystonia, medication, selective control concerns and tone management.
- Previous treatment: physiotherapy, strengthening, botulinum toxin, serial casting, orthoses, baclofen, intrathecal baclofen, selective dorsal rhizotomy and prior orthopaedic surgery.
- Growth: recent growth spurt, worsening contracture or new functional decline.
- Goals: what change would make treatment worthwhile?
- Rehabilitation reality: school support, therapy access, transport, home setup and family capacity.
Observation
Observe before touching the limb. Watch transfers, standing balance, shoes, braces and spontaneous walking. Then observe barefoot and braced gait from the side, front and behind.
Record:
- Walking speed and endurance.
- Initial contact: heel, flat foot or toe.
- Knee position in stance.
- Hip flexion and pelvic tilt.
- Foot progression angle.
- Step length and symmetry.
- Base width and scissoring.
- Trunk lean, arm posture and balance.
- Compensations: vaulting, circumduction, hip hiking and excessive pelvic rotation.
Physical examination
The examination should explain the gait, not merely document range.
- What to assess
- Velocity-dependent catch, clonus, dystonia and co-contraction
- Why it matters
- Dynamic tone may respond to non-operative tone management
- What to assess
- Hip flexors, adductors, hamstrings, gastrocnemius and soleus
- Why it matters
- Fixed contracture changes operative planning
- What to assess
- Hip abductors/extensors, quadriceps, dorsiflexors and plantarflexors
- Why it matters
- Weakness limits lengthening and predicts crouch risk
- What to assess
- Ability to isolate hip, knee, ankle and foot movement
- Why it matters
- Poor control limits expected surgical gain
- What to assess
- Hip rotation, thigh-foot axis, transmalleolar axis and foot progression
- Why it matters
- Identifies lever-arm dysfunction
- What to assess
- Planovalgus, equinovarus, midfoot break, callosities and braceability
- Why it matters
- A poor foot lever weakens push-off
Key tests
- Thomas test: hip flexion contracture.
- Hip abduction in flexion and extension: adductor tightness and hip surveillance relevance.
- Popliteal angle: hamstring length.
- Duncan-Ely or prone rectus test: rectus femoris tightness or overactivity clue.
- Silfverskiold test: gastrocnemius versus soleus contribution to equinus.
- Patellar height and extensor lag: extensor mechanism insufficiency.
- Rotational profile: femoral anteversion and tibial torsion.
- Foot assessment: hindfoot, midfoot, forefoot, subtalar flexibility and braceability.
- Strength and selective motor control: essential before lengthening decisions.
Investigations and Gait Analysis

Plain radiographs
- AP pelvis: migration percentage, acetabular index, femoral head shape, neck-shaft angle, hip subluxation, pelvic obliquity and pain source.
- Standing long-leg radiographs: coronal alignment and mechanical axis when deformity is suspected.
- Foot radiographs: weight-bearing AP and lateral views for planovalgus, cavovarus, midfoot break, talonavicular coverage and calcaneal pitch.
- Spine radiographs: scoliosis or pelvic obliquity when clinically relevant.
- Patellar height imaging: useful when crouch, extensor lag or anterior knee pain is present.
CT and MRI
CT may help quantify femoral anteversion or tibial torsion when clinical and gait findings are unclear. CT should support the decision; it should not replace functional assessment.
MRI brain is not routinely required for established CP gait planning, but may be appropriate if the neurological diagnosis is unclear, progressive or atypical.
Instrumented gait analysis
Instrumented gait analysis is most useful in complex ambulant CP, especially before SEMLS. It combines video, kinematics, kinetics, dynamic EMG, plantar pressure and temporospatial measures.
- What it shows
- Visual pattern, symmetry, orthotic effect and compensations
- Clinical use
- Correlates the data with what the clinician sees
- What it shows
- Speed, cadence, step length, stride length and support time
- Clinical use
- Quantifies function and response to treatment
- What it shows
- Joint angles across the gait cycle
- Clinical use
- Defines hip, knee, ankle, foot and pelvic motion
- What it shows
- Joint moments, power and ground reaction force
- Clinical use
- Shows whether muscles generate useful support and push-off
- What it shows
- Timing of muscle activity
- Clinical use
- Helps identify inappropriate rectus femoris, hamstring or calf activity
- What it shows
- Loading distribution and foot lever quality
- Clinical use
- Guides orthoses and foot reconstruction
- What it shows
- Oxygen cost or physiological cost index
- Clinical use
- Frames endurance and efficiency
What gait lab does not replace
Gait analysis cannot decide whether the family can manage rehabilitation, whether pain is the main complaint, whether school planning is realistic, or whether surgery matches the child's priorities. The report must be reconciled with examination, radiographs and shared decision-making.
Quantifying Gait: Summary Indices
The SEMLS evidence reports outcomes as the Gait Profile Score, but the topic never explains the summary indices that turn a gait-laboratory dataset into a single comparable number. These are how gait quality and treatment response are reported and compared.
- What it measures
- Root-mean-square deviation of nine key kinematic variables (the Gait Variable Scores) from typical data, in degrees
- Direction and use
- Lower is better (less deviation); fell after SEMLS in the meta-analysis; the Movement Analysis Profile displays the component scores
- What it measures
- Scaled multivariate index of kinematic normality
- Direction and use
- 100 represents unimpaired gait and each 10 points below 100 is about one standard deviation from typical; higher is better
- What it measures
- Structured observational (video) scoring of gait events at foot, knee, hip, pelvis and trunk
- Direction and use
- Usable without a full gait laboratory - valuable where instrumented analysis is unavailable
- What it measures
- Validated measure of gross motor capacity, distinct from the GMFCS classification
- Direction and use
- Tracks function over time; note SEMLS improves gait indices but not the GMFM or walking speed
Gait quality is reported as summary indices: the Gait Profile Score (root-mean-square deviation of nine key kinematic variables from normal, in degrees, displayed as the Movement Analysis Profile) and the Gait Deviation Index (scaled so 100 is unimpaired and each 10 points is about one standard deviation). Where a full gait laboratory is unavailable, the Edinburgh Visual Gait Score gives a structured observational alternative. These indices standardise outcome reporting and improve after SEMLS, but they summarise rather than localise - the individual kinematic curves and Movement Analysis Profile still tell you WHICH level to treat. Remember the key dissociation in the evidence: SEMLS improves the gait indices but not the Gross Motor Function Measure or walking speed.
Differential Diagnosis
A non-progressive brain lesion is the defining feature of cerebral palsy. Before committing a child to a gait-correction pathway, exclude conditions that mimic spastic diplegia but progress, are inherited, or are treatable in a completely different way. A worsening, regressing or strongly familial picture, or an unusually pure dystonia, should prompt neurology review rather than orthopaedic surgery.
- Discriminating features
- Non-progressive lesion, often with prematurity or perinatal insult; static motor disorder that worsens mechanically only through growth
- Why it changes management
- Standard gait-pattern and SEMLS framework applies
- Discriminating features
- Slowly progressive, symmetrical lower-limb spasticity, frequent positive family history, often normal birth history
- Why it changes management
- Progression and inheritance change prognosis and counselling; surgery gives only temporary benefit
- Discriminating features
- Diurnal fluctuation worse in evening, dystonic posturing, dramatic response to a levodopa trial
- Why it changes management
- A levodopa trial can avoid unnecessary surgery; missing it is a classic trap
- Discriminating features
- Bilateral toe-walking, normal tone and neurology, normal development, able to stand flat-footed on request
- Why it changes management
- Often non-operative; not part of the CP spectrum
- Discriminating features
- Boys, calf pseudohypertrophy, Gowers sign, proximal weakness, very high creatine kinase, progressive
- Why it changes management
- Lengthening surgery is contraindicated reasoning; weakness, not spasticity, drives gait
- Discriminating features
- Mixed upper and lower motor neuron signs, bladder symptoms, back or foot changes, progression
- Why it changes management
- Requires neurosurgical assessment before any limb surgery
- Discriminating features
- Cavovarus feet, distal wasting, areflexia, sensory signs, family history
- Why it changes management
- Foot deformity is neuropathic and progressive; plan differs from spastic foot
Loss of previously acquired skills, marked diurnal variation, a strong family history, pure dystonia without spasticity, sensory level or bladder involvement should all trigger neurological reassessment before gait surgery is planned.
Management Principles
Management is matched to function, age, gait pattern, impairments, goals and rehabilitation capacity.
Physiotherapy and strengthening
Therapy targets strength, balance, endurance, motor control and gait retraining. Strengthening of hip extensors, hip abductors, quadriceps and plantarflexors is particularly important in crouch and after SEMLS.
Orthoses
Orthoses should match the gait pattern. A hinged AFO, solid AFO, ground-reaction AFO or supramalleolar orthosis can help or harm depending on the deformity, strength and foot lever. A ground-reaction AFO may help selected crouch by influencing the ground reaction force, but it requires adequate passive correction, a braceable foot and enough tolerance to wear it.
Tone management
Botulinum toxin and serial casting may help younger children with dynamic focal spasticity, especially dynamic equinus. They do not correct fixed bony torsion, established lever-arm dysfunction or severe contracture.
Surveillance
Growth changes everything. Reassess hip displacement, pain, contracture progression, brace tolerance, function and walking endurance over time.
- Reasonable direction
- Physiotherapy, AFO optimisation, botulinum toxin and/or serial casting
- Avoid
- Early irreversible calf surgery without proving fixed contracture
- Reasonable direction
- Gastrocnemius recession when equinus is functionally important
- Avoid
- Overlengthening the whole gastrocsoleus unit
- Reasonable direction
- Careful tendo-Achilles lengthening in selected cases, especially unilateral fixed equinus
- Avoid
- Achilles lengthening for apparent equinus or crouch-prone diplegia
- Reasonable direction
- Strengthening, ground-reaction bracing if braceable, foot lever correction when indicated
- Avoid
- Isolated hamstring lengthening as the only solution
- Reasonable direction
- Consider distal femoral extension osteotomy with patellar tendon advancement or shortening when indicated
- Avoid
- Correcting the femur but ignoring extensor mechanism insufficiency
- Reasonable direction
- Femoral derotation osteotomy if clinical gait and rotational profile agree
- Avoid
- Operating from CT version alone
- Reasonable direction
- Tibial derotation osteotomy when functionally significant
- Avoid
- Treating knee flexion without correcting the foot progression driver
SEMLS Surgical Menu

The exact SEMLS package is individualised. The procedures below are common options; they are not a mandatory list.
Hip-level procedures
Adductor lengthening
Indications include adductor contracture, scissoring, reduced abduction, selected hip-at-risk patterns and hygiene/care needs in non-ambulant children. Commonly addressed muscles include adductor longus, gracilis and adductor brevis. Avoid destabilising the hip by treating adductors without considering hip containment.
Iliopsoas lengthening
Indications include hip flexion contracture, excessive anterior pelvic tilt, jump gait and persistent hip flexion in stance. Overlengthening can weaken hip flexion and impair swing advancement.
Femoral derotation osteotomy
Indications include excessive femoral anteversion with internal rotation gait, patellar maltracking or lever-arm dysfunction. Correction should be based on clinical rotational profile and gait, not CT numbers alone. Avoid overcorrection into external rotation.
Knee-level procedures
Medial hamstring lengthening
Indications include true hamstring contracture, increased popliteal angle, knee flexion contracture and excessive knee flexion in stance where hamstrings are a major driver. It is not the default treatment for all crouch gait.
Rectus femoris transfer
Indicated for selected stiff-knee gait with reduced or delayed swing-phase knee flexion and inappropriate rectus femoris activity. Dynamic EMG and kinematics are important. Poor selective control, weak push-off or lever-arm dysfunction may also cause poor knee flexion and should not be mistaken for isolated rectus overactivity.
Distal femoral extension osteotomy
Considered for severe crouch with fixed knee flexion deformity, especially in older children and adolescents. It corrects sagittal knee alignment and is often combined with patellar tendon advancement or shortening when extensor mechanism insufficiency is present.
Patellar tendon advancement or shortening
Indicated when patella alta and extensor lag contribute to crouch. If knee flexion deformity is corrected but patella alta is ignored, crouch may persist.
Tibial-level procedures
Tibial derotation osteotomy
Indications include clinically significant internal or external tibial torsion with abnormal foot progression and lever-arm dysfunction. External tibial torsion is especially important in crouch because it weakens the effective foot-ankle lever.
Calf and ankle procedures
Gastrocnemius recession
Considered when equinus is gastrocnemius-driven with a positive Silfverskiold pattern. In diplegia, gastrocnemius recession may preserve soleus better than tendo-Achilles lengthening.
Tendo-Achilles lengthening
Considered for fixed gastrocsoleus equinus in selected children, more commonly in hemiplegic fixed equinus than diplegic crouch-prone patterns. Risks include overlengthening, calcaneus, weak push-off and worsening crouch.
Foot procedures
Planovalgus correction
Indications include pain, brace intolerance, midfoot break, progressive deformity and lever-arm failure. Options include calcaneal lengthening osteotomy, medial column procedures, subtalar fusion or triple fusion in older severe rigid deformity.
Equinovarus correction
Indications include lateral border weight-bearing, recurrent sprains, brace difficulty and pressure callosity. Options include split tibialis anterior transfer, split tibialis posterior transfer, tendon lengthening, osteotomy or fusion in severe rigid deformity.
Pattern-Based Treatment Reasoning
True equinus
Decide whether the equinus is dynamic or fixed, gastrocnemius-only or gastrocsoleus, unilateral or bilateral, and whether it provides stance stability.
- Dynamic equinus: therapy, orthoses, botulinum toxin or serial casting.
- Fixed gastrocnemius contracture: gastrocnemius recession may be considered.
- Fixed gastrocsoleus contracture: Achilles lengthening may be considered with caution.
- Apparent equinus: do not lengthen the Achilles.
Jump gait
Jump gait is a multilevel flexed pattern with equinus. Treatment may require hip flexor, hamstring, calf, rotational or foot-level correction depending on findings. Isolated calf surgery is often incomplete.
Apparent equinus
The ankle is not the primary problem. Treat proximal flexion drivers, lever arms, weakness and gait pattern. Achilles lengthening here can create avoidable crouch.
Crouch gait
Crouch is a high-energy flexed gait pattern. Treatment depends on the drivers:
- Flexible mild crouch: strengthening, endurance work and selected orthoses.
- Hamstring-driven crouch: selected hamstring lengthening.
- Lever-arm crouch: correct femoral anteversion, tibial torsion, planovalgus or foot collapse.
- Extensor mechanism crouch: consider distal femoral extension osteotomy and patellar tendon advancement/shortening when indicated.
- Calcaneus or weak plantarflexor crouch: avoid further calf lengthening and focus on support, strengthening and lever arms.
Stiff-knee gait
The problem is reduced or delayed swing knee flexion. Rectus femoris transfer is considered only when the gait-lab and clinical pattern support inappropriate rectus activity. Circumduction, hip hiking and vaulting may be compensations for poor clearance.
Scissoring
Assess adductor tone, hip abduction range, hip displacement risk, balance and selective control. Do not treat scissoring in isolation without understanding the hip and functional goal.
Complications and Pitfalls
General complications
- Pain and delayed recovery.
- Blood loss.
- Wound problems or infection.
- Cast pressure sores.
- Neurovascular injury.
- Delayed union or nonunion after osteotomy.
- Hardware irritation.
- Rehabilitation failure.
- Loss of confidence or temporary loss of walking independence.
- Residual deformity, recurrence or need for revision surgery.
Procedure-specific complications
- Important complications
- Overlengthening, calcaneus, weak push-off, worsening crouch
- Avoidance principle
- Confirm true equinus and preserve strength
- Important complications
- Anterior pelvic tilt, weakness, recurvatum, persistent crouch
- Avoidance principle
- Use only when hamstrings are a true driver
- Important complications
- Persistent stiff knee, adhesions, limited benefit
- Avoidance principle
- Confirm swing-phase rectus overactivity
- Important complications
- Overcorrection, undercorrection, nonunion, hardware symptoms
- Avoidance principle
- Plan from functional rotation, not CT alone
- Important complications
- Compartment syndrome, peroneal nerve injury, malrotation
- Avoidance principle
- Careful correction, fixation and monitoring
- Important complications
- Undercorrection, overcorrection, nonunion, lateral column pain
- Avoidance principle
- Restore a braceable plantigrade lever
High-risk clinical reasoning errors
- Treating every toe-walker as true equinus.
- Lengthening Achilles for apparent equinus.
- Treating every crouch gait with hamstring lengthening.
- Ignoring weak plantarflexors.
- Ignoring patella alta and extensor lag.
- Ignoring planovalgus as a lever-arm problem.
- Planning from CT torsion numbers alone.
- Planning SEMLS without rehabilitation.
Rehabilitation After SEMLS
Rehabilitation is part of the indication. A child who cannot complete the rehabilitation pathway may not benefit from the operation.
Preoperative phase
- Define functional goals.
- Explain the timeline to the family and school.
- Optimise strength, nutrition, skin and equipment.
- Plan wheelchair, walking aids, orthoses and home transfers.
- Prepare for pain, casts, braces and reduced independence.
Early postoperative phase
- Pain and spasm control.
- Neurovascular and wound monitoring.
- Cast and pressure-area care.
- Transfers and safe positioning.
- Protection of osteotomies and tendon procedures.
- Family training.
Recovery phase
- Restore safe range without overstretching repairs.
- Begin muscle activation.
- Progress weight bearing according to procedures and fixation.
- Optimise orthoses.
- Strengthen hip extensors, abductors, quadriceps and plantarflexors.
Gait retraining phase
- Relearn walking with corrected alignment.
- Progress aids and endurance.
- Reintroduce stairs and school participation.
- Monitor recurrence, weakness, pain and brace fit.
Maximum functional benefit may take 12 to 24 months.
Clinical Reasoning Examples
Initial approach to a child with CP gait concern
"I would assess this child in a multidisciplinary cerebral palsy gait clinic. I would define the functional concern, family goals, distribution of involvement, movement disorder, GMFCS level, dynamic versus fixed deformity, strength, selective motor control and lever-arm dysfunction. I would not plan surgery from visual gait alone. For complex ambulant CP, especially before SEMLS, I would combine clinical examination, radiographs, rotational assessment and instrumented gait analysis."
If shown a toe-walking video
"I would first distinguish true equinus from apparent equinus. True equinus is ankle plantarflexion relative to the tibia. Apparent equinus may be caused by hip and knee flexion with a relatively plantigrade ankle. The distinction is critical because Achilles lengthening in apparent equinus can weaken the plantarflexors and worsen crouch."
Explaining what SEMLS means
"SEMLS is single-event multilevel surgery. It is the planned correction of clinically significant fixed soft-tissue contractures and bony lever-arm abnormalities affecting gait in one operative episode, usually informed by instrumented gait analysis, with one coordinated rehabilitation pathway."
Choosing investigations
"I would obtain radiographs relevant to the clinical problem: pelvis for hip surveillance, feet for planovalgus or cavovarus, long-leg alignment if coronal deformity is suspected, and rotational imaging only where it changes planning. For complex ambulant gait, I would use instrumented gait analysis including video, kinematics, kinetics, dynamic EMG, plantar pressure and temporospatial data."
Main danger in CP gait surgery
"The biggest danger is treating the visible compensation rather than the primary driver. Examples include Achilles lengthening for apparent equinus and isolated hamstring lengthening for crouch without addressing plantarflexor weakness, patella alta, external tibial torsion or planovalgus."
Common Reasoning Pitfalls
Pitfall 1: Toe walking means Achilles lengthening
Incorrect. Toe walking may be true equinus, jump gait, apparent equinus, dystonia or compensation.
Pitfall 2: Crouch means tight hamstrings
Incorrect. Crouch may be driven by weak plantarflexors, patella alta, planovalgus, external tibial torsion, prior Achilles overlengthening, weak quadriceps, hamstring contracture or fixed knee flexion deformity.
Pitfall 3: CT version decides femoral osteotomy
Incorrect. CT can quantify version, but clinical gait and instrumented gait analysis determine whether rotation is functionally important.
Pitfall 4: Rectus transfer for any stiff knee
Incorrect. Confirm inappropriate rectus femoris activity and the correct kinematic pattern. Poor push-off, weakness and poor selective control can also reduce swing knee flexion.
Pitfall 5: SEMLS is just multiple releases
Incorrect. Modern SEMLS may include soft-tissue balancing, tendon transfers, osteotomies, patellar tendon procedures and foot reconstruction, all linked to one rehabilitation plan.
Summary Tables
- Hip
- Neutral or extended
- Knee
- Neutral or recurvatum
- Ankle/foot
- Plantarflexed
- Common driver
- Gastrocsoleus spasticity or contracture
- Treatment principle
- Treat calf only when true equinus is confirmed
- Hip
- Flexed
- Knee
- Flexed
- Ankle/foot
- Equinus
- Common driver
- Hip flexor, hamstring and calf involvement
- Treatment principle
- Multilevel assessment and selected correction
- Hip
- Flexed
- Knee
- Flexed
- Ankle/foot
- Neutral or dorsiflexed
- Common driver
- Proximal flexion pattern
- Treatment principle
- Do not lengthen Achilles unless true equinus coexists
- Hip
- Flexed
- Knee
- Flexed
- Ankle/foot
- Dorsiflexed or calcaneus
- Common driver
- Weakness, lever-arm failure, patella alta or contracture
- Treatment principle
- Correct all drivers; avoid reflex hamstring or calf lengthening
- Hip
- Variable
- Knee
- Reduced swing flexion
- Ankle/foot
- Toe drag or compensation
- Common driver
- Rectus femoris overactivity or poor clearance mechanics
- Treatment principle
- Rectus transfer only if confirmed
- Hip
- Variable
- Knee
- Crouch tendency
- Ankle/foot
- Valgus and midfoot break
- Common driver
- Ineffective foot lever
- Treatment principle
- Restore a stable plantigrade foot
- Favourable
- Ambulant or meaningful supported walking goal
- Concerning
- Non-ambulant child if the goal is efficient gait
- Favourable
- Fixed multilevel deformity or lever-arm dysfunction
- Concerning
- Purely dynamic tone problem
- Favourable
- Clinical assessment, imaging and gait analysis agree
- Concerning
- Unclear driver or compensation misunderstood
- Favourable
- Spasticity with predictable pattern
- Concerning
- Uncontrolled dystonia or mixed movement disorder
- Favourable
- Family, school and therapy pathway realistic
- Concerning
- Unable to complete postoperative rehabilitation
- Favourable
- Functional, measurable goals
- Concerning
- Expectation of normal gait or quick recovery
Guidelines, Registries & Global Practice
Cerebral palsy is the most common cause of physical disability beginning in childhood worldwide, but its prevalence, surveillance infrastructure and treatment access differ sharply between high-income and low- and middle-income settings. Gait-correction surgery sits within a wider, internationally consistent care model built on multidisciplinary assessment, structured hip surveillance and instrumented gait analysis where available.
Global epidemiology
- Birth prevalence
- 1.6 per 1000 live births
- Source
- McIntyre et al. 2022, systematic analysis (PMID 35952356)
- Birth prevalence
- 1.5 per 1000 live births; declining across Europe and Australia
- Source
- McIntyre et al. 2022 (PMID 35952356)
- Birth prevalence
- Up to 3.4 per 1000 live births; trends not yet measurable
- Source
- McIntyre et al. 2022 (PMID 35952356)
- Birth prevalence
- 2.95 per 1000 children surveyed
- Source
- Chauhan et al. 2019, systematic review and meta-analysis (PMID 31300955)
Spastic subtypes predominate, and gait-correction surgery mainly concerns ambulant children at GMFCS levels I to III, especially spastic diplegia and hemiplegia. The higher burden in low- and middle-income countries is accompanied by less access to gait laboratories, orthotics and structured rehabilitation, which shifts real-world practice toward clinical decision-making without instrumented analysis.
Major guidance, side by side
- Relevant position
- Multidisciplinary management; orthopaedic surgery for established contracture or deformity affecting function or care; structured hip surveillance
- Practical implication
- Surgery follows defined function or care goals, not appearance
- Relevant position
- Evidence-based hip-surveillance and tone-management pathways; SEMLS for selected ambulant children after gait analysis
- Practical implication
- Frames SEMLS as selected reconstruction, not routine treatment
- Relevant position
- Tone management and selected orthopaedic correction within a multidisciplinary team
- Practical implication
- Aligns with global emphasis on team-based selection
- Relevant position
- Standardised radiographic hip surveillance by GMFCS level to detect displacement before dislocation
- Practical implication
- Surveillance, not gait surgery, dominates GMFCS IV-V care
Across guidelines the recommendations converge: multidisciplinary assessment, separation of dynamic tone from fixed deformity, gait analysis before complex multilevel surgery, and tone-management options (botulinum toxin, baclofen, selective dorsal rhizotomy) considered alongside orthopaedic correction. Differences are largely in service organisation rather than principle.
Evidence on tone management as part of the pathway
Selective dorsal rhizotomy (landmark RCT meta-analysis)
- Pooled data from three RCTs showed selective dorsal rhizotomy plus physiotherapy reduced spasticity versus physiotherapy alone (Ashworth mean change difference -1.2, p less than 0.001).
- SDR plus physiotherapy produced a small but significant gain in gross motor function (GMFM change-score difference +4.0, p=0.008).
- Functional improvement related directly to the percentage of dorsal root tissue transected.
Global prevalence of cerebral palsy
- Overall CP birth prevalence in high-income countries has declined to 1.6 per 1000 live births.
- Pre-/perinatal CP birth prevalence declined significantly across most European and Australian regions, with no change in postneonatal CP.
- Limited data from low- and middle-income countries show markedly higher prevalence, up to 3.4 per 1000 live births for pre-/perinatal CP.
Practice variation
- Gait analysis access: routine in many high-income tertiary centres before SEMLS, but scarce in low-resource settings, where clinical pattern recognition and observational gait analysis carry more weight.
- Tone management: availability of intrathecal baclofen and selective dorsal rhizotomy varies by centre and country, altering the balance between neurosurgical and orthopaedic management.
- Hip surveillance: standardised population programmes are established in some regions (for example Australia, Scandinavia and parts of the UK) but absent elsewhere, changing how late displacement presents.
- Rehabilitation: outcomes after SEMLS depend heavily on access to prolonged structured rehabilitation, which is unevenly available worldwide.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 10-year-old ambulant child with spastic diplegic CP presents with worsening crouch gait and fatigue. How do you assess and manage?”
“A child appears to toe walk, but gait analysis shows ankle dorsiflexion is near neutral while the hip and knee remain flexed. What is the diagnosis and why does it matter?”
“A family asks why their child needs several procedures at the same operation. How do you explain SEMLS?”
Classify
- CP distribution
- Movement disorder
- GMFCS from function
- Sagittal gait pattern
- Lever-arm status
Assess
- Goals, pain, fatigue and falls
- Barefoot and braced gait
- Tone and fixed contracture
- Strength and selective control
- Rotational profile and foot shape
Recognise
- True equinus
- Jump gait
- Apparent equinus
- Crouch gait
- Stiff-knee gait
Pitfalls
- Treating GMFCS as a standalone history item
- Achilles lengthening for apparent equinus
- Hamstring lengthening for every crouch
- Ignoring weakness and lever arms
- Planning SEMLS without rehabilitation
“Think function, classify, identify the driver, then plan the whole limb.”
Evidence Base
GMFCS
- GMFCS classifies gross motor function in cerebral palsy using self-initiated movement, especially sitting, transfers and mobility.
- Interrater reliability (kappa) was 0.55 for children under 2 years and 0.75 for children 2 to 12 years.
- It frames prognosis and goals but does not define the gait pattern or operation.
Sagittal gait patterns in spastic diplegia
- Spastic diplegic gait can be classified into sagittal patterns including true equinus, jump gait, apparent equinus and crouch, based on pattern recognition combined with kinematic data.
- The longitudinal arm of 34 children demonstrated the reliability of the classification over time.
- Pattern recognition links gait to muscle targets, orthoses and surgical planning but remains a guide, not a substitute for full assessment.
Selected References
-
Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol. 1997;39:214-223. PMID: 9183258
-
Rodda J, Graham HK. Classification of gait patterns in spastic hemiplegia and spastic diplegia: a basis for a management algorithm. Eur J Neurol. 2001;8 Suppl 5:98-108. PMID: 11851738
-
Rodda JM, Graham HK, Carson L, Galea MP, Wolfe R. Sagittal gait patterns in spastic diplegia. J Bone Joint Surg Br. 2004;86:251-258. PMID: 15046442
-
McGinley JL, Baker R, Wolfe R, Morris ME. The reliability of three-dimensional kinematic gait measurements: a systematic review. Gait Posture. 2009;29:360-369. PMID: 19013070
-
McGinley JL, Dobson F, Ganeshalingam R, Shore BJ, Rutz E, Graham HK. Single-event multilevel surgery for children with cerebral palsy: a systematic review. Dev Med Child Neurol. 2012;54:117-128. PMID: 22111994
-
Lamberts RP, Burger M, du Toit J, Langerak NG. A systematic review of the effects of single-event multilevel surgery on gait parameters in children with spastic cerebral palsy. PLOS One. 2016. PMID: 27755599
-
Amirmudin NA, Lavelle G, Theologis T, Thompson N, Ryan JM. Multilevel surgery for children with cerebral palsy: a meta-analysis. Pediatrics. 2019;143:e20183390. PMID: 30918016
-
Kedem P, Scher DM. Evaluation and management of crouch gait. Curr Opin Pediatr. 2016;28:55-59. PMID: 26709688
-
Galey SA, Lerner ZF, Bulea TC, Zimbler S, Damiano DL. Effectiveness of surgical and non-surgical management of crouch gait in cerebral palsy: a systematic review. Gait Posture. 2017;54:93-105. PMID: 28279852
-
O'Sullivan R, Marron A, Brady K. Crouch gait or flexed-knee gait in cerebral palsy: is there a difference? Gait Posture. 2020;82:153-160. PMID: 32927222
-
Theologis T. Lever arm dysfunction in cerebral palsy gait. J Child Orthop. 2013;7:379-382. PMID: 24432098
-
Carty CP, Walsh HPJ, Gillett JG, et al. The effect of femoral derotation osteotomy on transverse plane hip and pelvic kinematics in children with cerebral palsy: a systematic review and meta-analysis. Gait Posture. 2014;40:333-340. PMID: 24984692
-
Davids JR. The foot and ankle in cerebral palsy. Orthop Clin North Am. 2010;41:579-593. PMID: 20868886
-
Sees JP, Miller F. The foot in cerebral palsy. Foot Ankle Clin. 2021;26:639-653. PMID: 34752232
-
Guinet AL, Khouri N, Desailly E. Rehabilitation after single-event multilevel surgery for children and young adults with cerebral palsy: a systematic review. Am J Phys Med Rehabil. 2022;101:389-399. PMID: 34393188
-
McIntyre S, Goldsmith S, Webb A, et al. Global prevalence of cerebral palsy: a systematic analysis. Dev Med Child Neurol. 2022;64:1494-1506. PMID: 35952356
-
Chauhan A, Singh M, Jaiswal N, Agarwal A, Sahu JK, Singh M. Prevalence of cerebral palsy in Indian children: a systematic review and meta-analysis. Indian J Pediatr. 2019;86:1124-1130. PMID: 31300955
-
Armstrong RW. The first meta-analysis of randomized controlled surgical trials in cerebral palsy (2002). Dev Med Child Neurol. 2008;50:244. PMID: 18352992