Measurement, maturity prediction and treatment timing
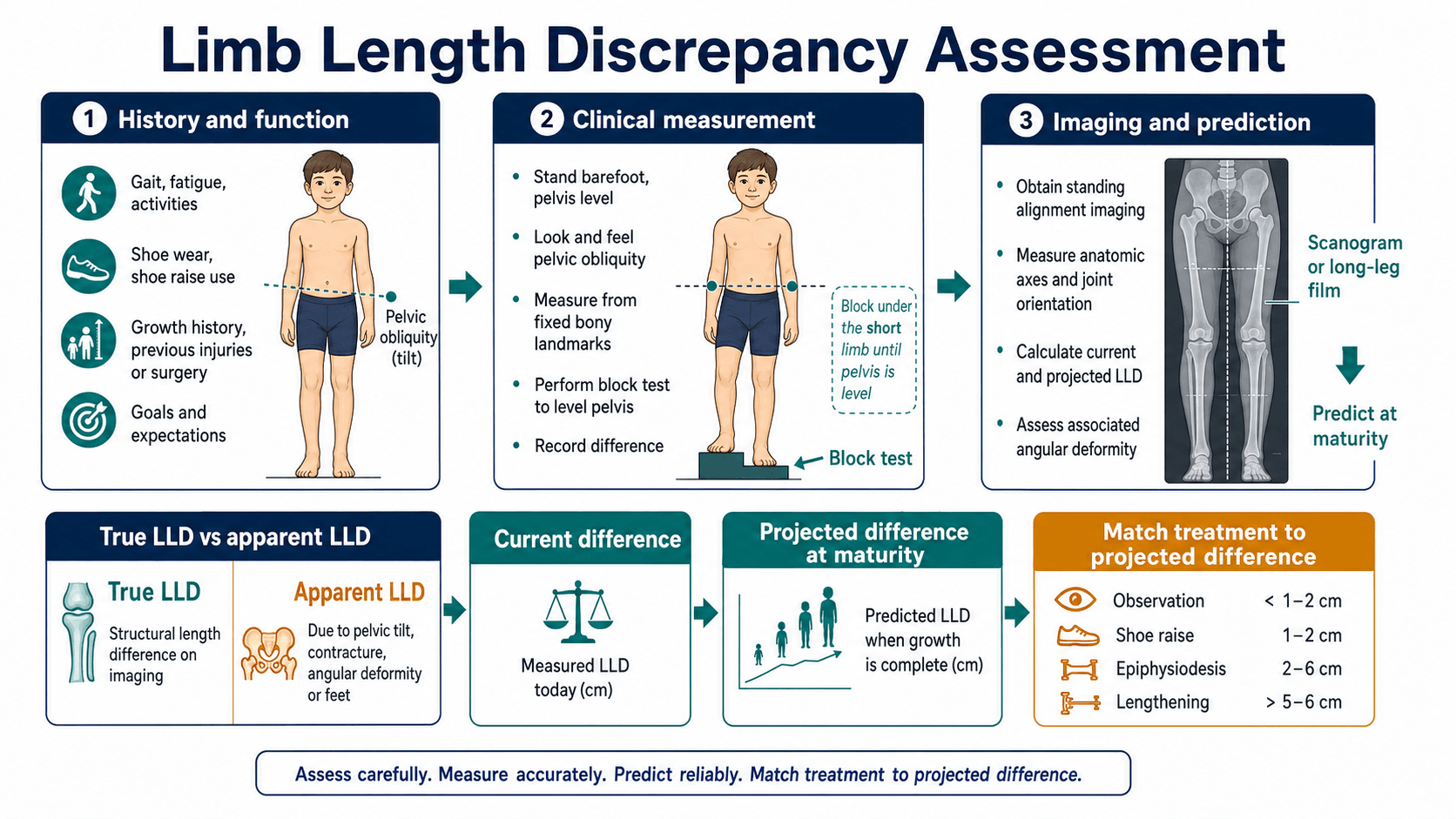
- Separate structural limb length discrepancy from functional discrepancy caused by pelvic obliquity, scoliosis, contracture, pain, equinus or foot height.
- Measure the discrepancy clinically with blocks, then radiographically with calibrated standing imaging that separates femoral and tibial contributions and assesses mechanical axis.
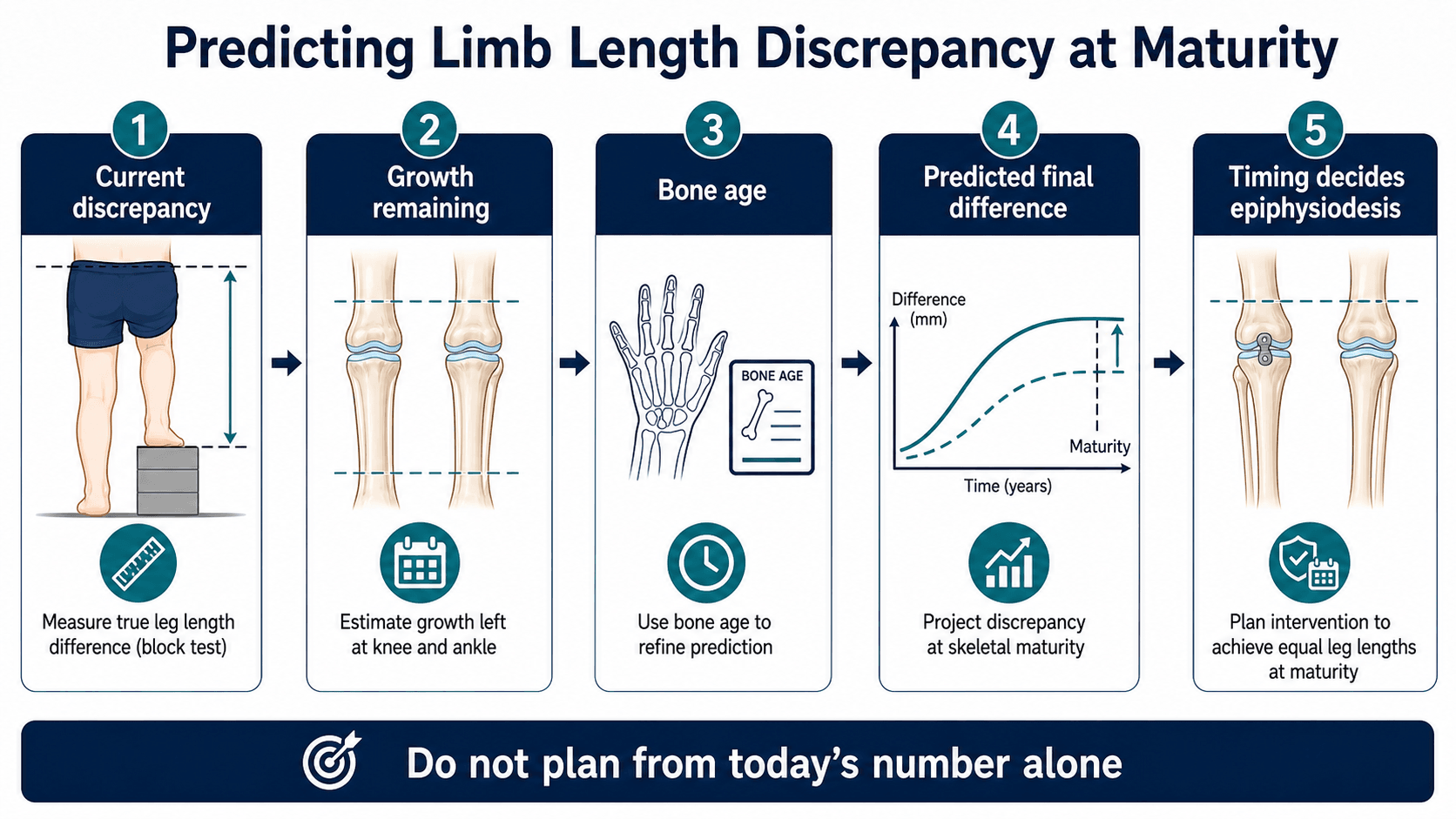
- Base treatment on predicted discrepancy at skeletal maturity, not the current measurement alone.
- Epiphysiodesis slows the longer limb. It is appropriate only when the responsible physis is open, enough growth remains and the predicted discrepancy is within its correction capacity.
- Lengthening is not just bone distraction. It is a prolonged reconstruction affecting regenerate bone, joints, nerves, muscles, school, sport, family capacity and psychological tolerance.
- “A shoe lift is a treatment, not a failure of surgical planning.
- “The block test answers a functional question: how much correction levels the pelvis and improves gait today?
- “Prediction methods are estimates, not guarantees. A mature plan acknowledges error and uses serial review.
- “Do not plan epiphysiodesis without knowing which segment is long and how much growth remains in that segment.
- “A congenital deficiency needs a life-plan, not a single centimetre target.
- “A modern lengthening nail improves patient experience, but it does not make lengthening a low-risk procedure.
A limb length discrepancy value is not a management plan. The plan needs true versus apparent discrepancy, block correction, calibrated segment measurements, bone age, projected discrepancy at maturity, joint and foot assessment, and a realistic discussion of treatment burden.
- Practical interpretation
- The size of the discrepancy is important, but symptoms, gait, maturity, diagnosis and family preference decide treatment.
- Why it changes management
- Prevents automatic surgery for a number alone.
- Practical interpretation
- Growth prediction can be wrong by clinically meaningful margins, especially with abnormal growth or single measurements.
- Why it changes management
- Families must understand residual LLD, undercorrection and overcorrection.
- Practical interpretation
- Standing long-leg radiographs or EOS can assess length, axis and pelvic compensation together.
- Why it changes management
- A scanogram number alone can miss deformity and mechanical axis problems.
- Practical interpretation
- It works best for predicted moderate discrepancy with open physes and enough growth remaining.
- Why it changes management
- The operation is small; the timing decision is the difficult part.
- Practical interpretation
- Motorised nails and modern frames improve control, but stiffness, regenerate problems, nerve symptoms and reoperation still matter.
- Why it changes management
- Technology changes options, not the need for careful selection.
Images and Diagrams

- High-yield answer
- True anatomical versus apparent functional discrepancy.
- Why it matters
- Prevents treating pelvic obliquity or contracture as bony shortening.
- High-yield answer
- Standing block test to level the pelvis.
- Why it matters
- Links the centimetre value to gait and symptoms.
- High-yield answer
- Predicted discrepancy at skeletal maturity.
- Why it matters
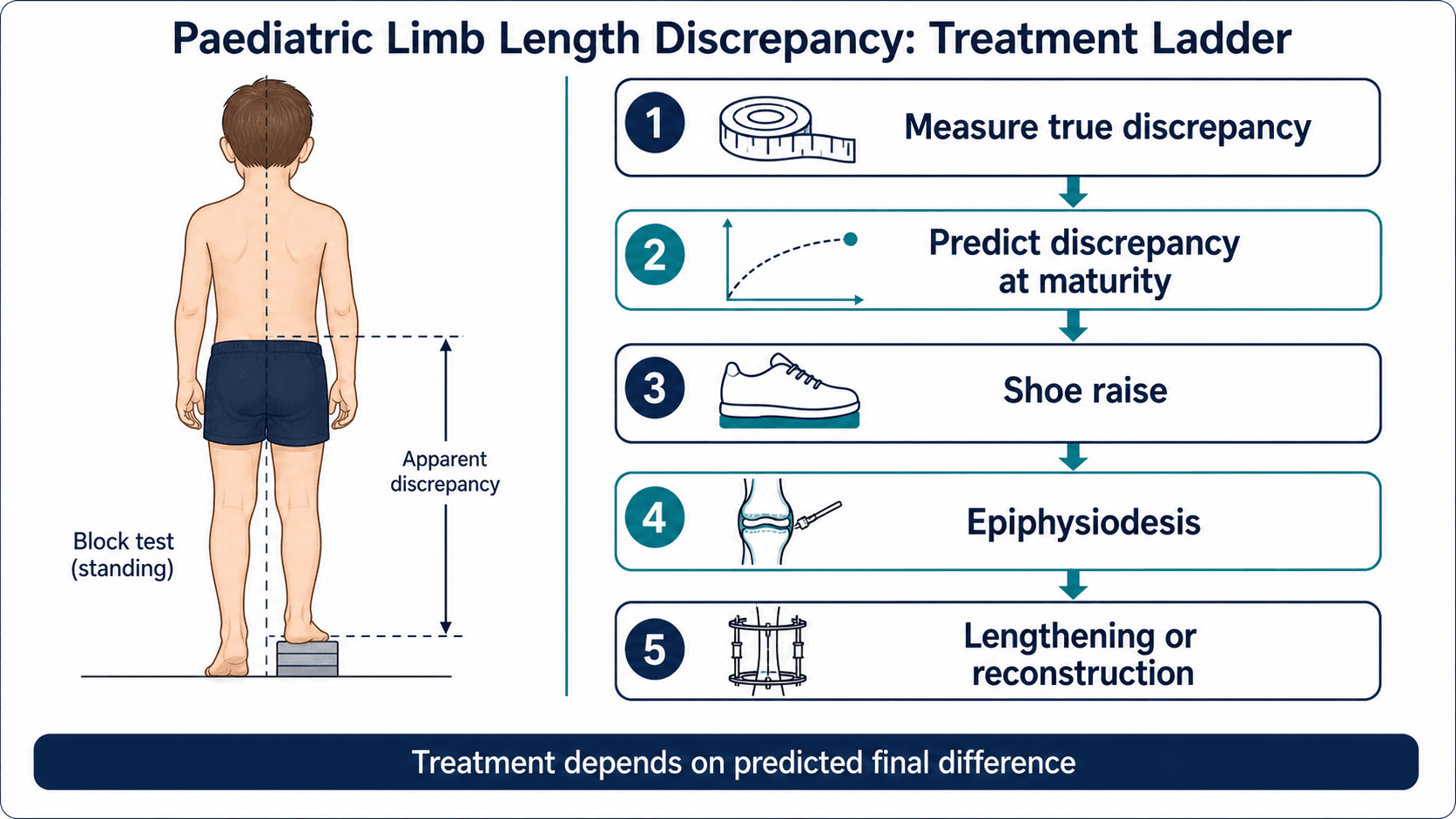
- Less than 2 cm usually lift/observe; 2 to 5 cm often epiphysiodesis if growing; more than 5 cm usually lengthening or reconstruction.
- High-yield answer
- Femur, tibia, foot height, axis and joint stability.
- Why it matters
- Determines which segment is treated and whether lengthening is safe.
- High-yield answer
- Prediction error, residual inequality and treatment burden.
- Why it matters
- LLD surgery is elective and preference-sensitive.
LEVELAssessment Sequence
Hook:LEVEL prevents treatment decisions from being based on a number before the child is properly understood.
PHYSISEpiphysiodesis Checklist
Hook:PHYSIS is the decision gate before arresting growth.
LIFTTreatment Ladder
Hook:LIFT prevents jumping straight from diagnosis to lengthening.
Overview/Epidemiology
Limb length discrepancy is a difference in functional or anatomical length between the lower limbs. Mild asymmetry is common and often asymptomatic. The clinically important problem is not simply whether one leg is shorter, but whether the discrepancy affects gait, pelvis, spine, sport, pain, shoe wear, cosmesis, joints, family burden or long-term function.
The initial clinical distinction is between a true bony discrepancy and an apparent discrepancy caused by pelvic obliquity, spine deformity, contracture, foot height or compensation. Assessment then progresses from block testing and whole-limb examination to calibrated imaging, skeletal maturity assessment and prediction of the discrepancy at maturity.
Published reviews consistently make two important points. First, high-quality evidence for exact treatment thresholds is limited, so many thresholds are consensus-based. Second, treatment is usually elective. A child with a 2 cm discrepancy, a compensating pelvis and no symptoms is not the same clinical problem as a child with a 2 cm discrepancy, pain, a progressive physeal bar or a complex congenital deficiency.
Why it matters clinically
- LLD can increase energy cost and alter gait.
- The short limb may compensate with equinus, toe walking or pelvic drop.
- The long limb may compensate with hip and knee flexion during stance.
- Pelvic obliquity can create a functional scoliosis that improves when the pelvis is levelled.
- A congenital deficiency may involve length, foot rays, ankle stability, knee stability, hip morphology and prosthetic options.
- A post-traumatic physeal arrest may produce both shortening and angular deformity.
Common causes
The diagnosis determines the growth behaviour. A congenital proportional discrepancy behaves differently from a post-traumatic bar, a vascular overgrowth syndrome or a post-infective joint-damaging lesion.
- Congenital or developmental: congenital femoral deficiency, fibular hemimelia, tibial deficiency, hemihyperplasia, skeletal dysplasia, neurofibromatosis, vascular malformation and idiopathic asymmetrical growth.
- Post-traumatic: malunion with shortening, physeal arrest, growth stimulation after femoral shaft fracture, or partial bar formation.
- Infective or inflammatory: neonatal osteomyelitis, septic arthritis, juvenile inflammatory disease or physeal injury.
- Tumour-related: resection, radiation, chemotherapy effects, benign aggressive lesions or limb salvage reconstruction.
- Neuromuscular and functional: pelvic obliquity, scoliosis, hip contracture, knee flexion, equinus, foot deformity or muscle imbalance.
Treatment is elective in most cases. That matters: the indication is not the X-ray measurement alone. The indication is the predicted discrepancy plus symptoms, gait, maturity, treatment risk and the family's priorities.
Decision Framework
Every limb length discrepancy assessment should answer four linked questions.
- What to prove
- Blocks and examination show whether the pelvis levels and whether contracture, scoliosis or foot height is driving the asymmetry.
- Common error
- Treating pelvic obliquity or contracture as bony shortening.
- What to prove
- Femur, tibia, foot height and mechanical axis are measured separately.
- Common error
- Planning distal femoral epiphysiodesis when the tibia or foot is the main contributor.
- What to prove
- Bone age, serial measurements and a recognised prediction method estimate the final discrepancy.
- Common error
- Treating today's measurement in a growing child.
- What to prove
- Lift, epiphysiodesis, shortening, lengthening and prosthetic pathways are matched to function and family goals.
- Common error
- Offering lengthening before proving that simpler options are inadequate.
The goal is functional equalisation, not a mathematical promise of exactly equal limbs. A residual discrepancy of about 1 cm is often acceptable if gait, pelvis and symptoms are satisfactory. Conversely, a smaller discrepancy may still need treatment when it is progressive, symptomatic, associated with deformity or part of a congenital deficiency plan.
Pathophysiology
True anatomical discrepancy
True discrepancy means the bones or foot height are genuinely different. The femur may be short, the tibia may be short, the foot may contribute, or all three may contribute. Segmental localisation is essential because the operation must match the segment.
Examples:
- Congenital femoral deficiency produces a femoral-dominant discrepancy, often with hip and knee instability.
- Fibular hemimelia may combine tibial shortening, foot ray deficiency, ankle deformity and valgus instability.
- Post-infective proximal femoral damage may combine shortening, deformity and joint damage.
- Post-fracture overgrowth may make the injured limb longer, especially after paediatric femoral shaft fracture.
- Physeal arrest can produce both length inequality and angular deformity.
Apparent functional discrepancy
Apparent discrepancy is not a true bony inequality. It is caused by posture, contracture, deformity or pain. This is a common clinical trap.
Common drivers:
- Pelvic obliquity from scoliosis.
- Hip adduction contracture making the limb appear short.
- Hip abduction contracture making the limb appear long.
- Knee flexion contracture functionally shortening the limb.
- Equinus on the short side as compensation.
- Foot height difference from cavus, planovalgus, vertical talus or partial foot deficiency.
- Painful limp being mislabelled as LLD.
Growth behaviour
Congenital discrepancies often behave proportionally: the difference grows as the child grows. This is the basis for multiplier-style prediction. Acquired discrepancies may not behave predictably. A complete physeal arrest, partial bar, fracture overgrowth, vascular malformation, infection or tumour treatment can change the trend, which is why serial measurement is more valuable than a single radiograph.
The knee physes are the usual epiphysiodesis targets because they provide most clinically useful remaining growth: the distal femur contributes approximately 9 mm per year and the proximal tibia approximately 6 mm per year. Together they provide roughly 15 mm per year, although individual growth depends on skeletal maturity, sex, puberty and pathology.
The proximal femur and distal tibia contribute to total limb length, but they are not routine simple LLD arrest targets. They matter in prediction, congenital deficiency planning, ankle-level deformity and complex reconstruction.
Why epiphysiodesis works
Epiphysiodesis slows or stops growth in the longer limb. The shorter limb does not lengthen faster. Equalisation occurs because the long limb stops gaining length while the short limb continues to grow. Therefore epiphysiodesis only works if:
- The child is skeletally immature.
- The physes that are stopped still have enough growth remaining.
- The predicted discrepancy is within the correction capacity of growth arrest.
- The segment treated matches the segment responsible.
- The timing is correct.
The operation is technically simple compared with lengthening, but the planning is not simple.
Why lengthening is different
Lengthening is distraction osteogenesis. A corticotomy or osteotomy creates a biologic regenerate that is gradually distracted. The bone can lengthen, but bone is rarely the only limit.
- Why it matters
- Hip, knee and ankle must tolerate gradual distraction.
- Risk if ignored
- Subluxation, contracture or loss of function.
- Why it matters
- A longer limb still needs a useful end-bearing lever.
- Risk if ignored
- Longer limb with poor shoe wear or poor prosthetic compatibility.
- Why it matters
- Angular and rotational deformity may need simultaneous or staged correction.
- Risk if ignored
- Lengthening magnifies malalignment.
- Why it matters
- Nerves, vessels, muscles and skin often limit safe correction.
- Risk if ignored
- Pain, nerve stretch, stiffness and treatment abandonment.
- Why it matters
- Lengthening requires months of monitoring, therapy and device care.
- Risk if ignored
- Technically successful surgery with poor practical outcome.
Classification
True anatomical LLD
A real difference in bone length or foot height. This requires clinical and radiographic measurement before treatment planning.
Apparent functional LLD
A functional inequality caused by pelvis, spine, joint contracture, ankle position, foot deformity or pain. Treat the driver rather than arresting growth.
Mixed LLD
Common in congenital deficiency and neuromuscular disease. The child may have true shortening plus pelvic obliquity, angular deformity, joint instability and foot-height difference.
Clinical Presentation
Children present in several different ways:
- Parent notices asymmetric gait, hip height or toe walking.
- Screening identifies pelvic tilt or functional scoliosis.
- The child reports fatigue, tripping, sport limitation or shoe-wear difficulty.
- Adolescent reports back pain, hip pain, knee pain or cosmetic concern.
- A known congenital deficiency is followed through growth.
- A post-traumatic or post-infective child develops progressive inequality.
Characteristic compensations
Short side compensation:
- Toe walking or equinus on the short limb.
- Pelvic drop on the short side.
- Increased energy cost.
- Vaulting or circumduction in severe cases.
Long side compensation:
- Knee flexion on the long limb.
- Hip and knee flexion during stance.
- Pelvic hiking.
- Shoe modification or altered foot posture.
History that matters
The history should identify the cause of discrepancy, its progression and whether treatment would improve the child's function:
- Onset: present from birth, noticed with walking, or acquired after fracture, infection or surgery.
- Progression: stable, increasing proportionally, or changing unpredictably.
- Function: walking distance, running, sport, falls, fatigue, pain and school participation.
- Symptoms: back, hip, knee, ankle, foot pain, callosities and shoe intolerance.
- Known diagnosis: congenital femoral deficiency, fibular hemimelia, Perthes disease, SCFE, tumour treatment, infection or skeletal dysplasia.
- Previous treatment: lifts, orthoses, physiotherapy, guided growth, reconstruction, lengthening or prosthetic discussion.
- Family goals: avoid limp, avoid large shoe lift, participate in sport, reduce pain, avoid repeated operations, or plan a congenital deficiency pathway.
Red flags
- Painful limp that does not improve with blocks.
- Night pain, systemic symptoms or tumour/infection features.
- Neurological signs, progressive weakness or abnormal reflexes.
- Rapidly changing discrepancy after physeal injury.
- Pelvic obliquity that does not correct when the limbs are levelled.
- Joint instability in a child being considered for lengthening.
The same measured discrepancy may need observation in one child, a lift in another, epiphysiodesis in a third and staged reconstruction in a congenital deficiency. The decision is measurement plus growth plus function.
Clinical Examination
Inspection standing
Observe the child barefoot from front, side and back:
- Shoulder and pelvic levels.
- Lumbar scoliosis or compensatory curve.
- Iliac crest height.
- Knee flexion on the long side.
- Toe standing on the short side.
- Hindfoot valgus or varus.
- Foot size and foot height.
- Calf and thigh girth.
- Skin scars from trauma, infection or previous reconstruction.
Gait
Look for:
- Antalgic component suggesting pain rather than LLD alone.
- Short-leg gait with pelvic drop.
- Toe walking on the short side.
- Knee flexion on the long side.
- Circumduction or vaulting.
- Trendelenburg pattern suggesting hip abductor weakness or dysplasia.
- Neuromuscular features such as spasticity, foot drop or crouch.
Block test
Place measured blocks under the short limb until the pelvis is level. This is the key clinical test.
The block test tells you:
- The functional correction needed to level the pelvis.
- Whether gait improves with correction.
- Whether spinal or pelvic obliquity is flexible.
- Whether the patient tolerates correction.
- Whether symptoms are likely related to the discrepancy.
Do not assume the block height equals the final surgical target. It is a clinical correction estimate, not a complete maturity prediction.
Length measurement
Clinical tape measurement is useful but not definitive.
- Apparent length: umbilicus to medial malleolus.
- True length: anterior superior iliac spine to medial malleolus.
- Segment lengths: compare femur and tibia clinically, then confirm radiographically.
- Foot contribution: compare plantar foot height, foot length and deformity.
Joint and spine examination
Assess:
- Spine: scoliosis, pelvic obliquity and flexibility.
- Hip: abduction, adduction contracture, flexion contracture, rotation, Trendelenburg and stability.
- Knee: flexion contracture, recurvatum, valgus or varus, instability and patellar height.
- Ankle and foot: equinus, calcaneus, cavus, planovalgus, subtalar stiffness and braceability.
- Neurology: tone, reflexes, power, sensation and selective motor control when indicated.
Hip adduction contracture can make a limb appear short. Hip abduction contracture can make a limb appear long. If this is missed, the calculation and the operation may both be wrong.
Localising the Short Segment Clinically
Before imaging, localise which segment is short - the operation must match the responsible segment. The bedside tools are the Galeazzi (Allis) sign, the true-versus-apparent tape measurement and an assessment of foot height.
- Method
- Supine, both knees flexed to 90 degrees, feet flat and heels level on the couch; compare the knee heights
- What it tells you
- A knee that sits lower viewed from the foot end suggests a shorter TIBIA; a knee set further back viewed from the side suggests a shorter FEMUR
- Method
- True length: ASIS to medial malleolus. Apparent length: umbilicus to medial malleolus
- What it tells you
- A true-length difference is structural; an apparent-only difference points to pelvic obliquity or contracture
- Method
- Compare standing heel/foot height and include the foot in the standing block test
- What it tells you
- Foot-height discrepancy adds to functional length but is NOT corrected by epiphysiodesis - plan a shoe raise or foot surgery
- Method
- Calibrated standing long-leg radiograph or scanogram with segmental measurement
- What it tells you
- Quantifies the femoral, tibial and foot contributions the clinical tests suggested
Before imaging, localise the short segment clinically. The Galeazzi (Allis) sign - both knees flexed to 90 degrees, supine, heels level - compares knee heights: a knee that sits lower viewed from the foot end suggests a short tibia, while a knee set further back viewed from the side suggests a short femur. Confirm with true (ASIS to medial malleolus) versus apparent (umbilicus to medial malleolus) tape lengths, and remember foot height - it adds to the functional length but cannot be corrected by epiphysiodesis. Calibrated standing imaging then quantifies the femoral, tibial and foot contributions, because the operation must match the responsible segment.
Investigations
Use calibrated imaging: standing long-leg radiographs when axis matters, EOS where available for repeated low-dose assessment, scanogram for classic length measurement, and CT scanogram for complex rotation or flexion deformity. The measurement must state total length, femoral length, tibial length, mechanical axis, angular deformity, foot-height contribution when relevant, and whether the pelvis was levelled. Standing imaging is often preferable as a first-line study because it assesses length and mechanical alignment together.
- How it works
- Uses skeletal age and expected remaining growth of the distal femur, proximal tibia and other physes.
- Best use
- Segment-specific planning when deciding distal femur versus proximal tibia epiphysiodesis.
- Limitation
- Needs accurate bone age; chart-based estimates can be wrong in abnormal growth.
- How it works
- Plots serial limb lengths against skeletal maturity to forecast final discrepancy and timing.
- Best use
- Excellent when serial measurements are available and growth appears linear.
- Limitation
- Less useful from a single data point or in unpredictable acquired physeal injury.
- How it works
- Uses age, sex and multipliers to predict mature length and final discrepancy.
- Best use
- Quick, widely used method for both congenital and acquired discrepancy planning.
- Limitation
- Can be inaccurate if physiological age differs from chronological age.
- How it works
- Uses remaining years of growth and approximate annual growth around the knee.
- Best use
- Rapid clinical cross-check.
- Limitation
- Too approximate to be the sole basis for surgery.
Use prediction in practice by measuring current segmental discrepancy, determining skeletal age, estimating final discrepancy formally, repeating the estimate when possible, then choosing the less than 2 cm, 2 to 5 cm, or more than 5 cm pathway. A residual discrepancy of about 1 cm is often acceptable; perfect equality is not guaranteed.
Prediction workflow in clinic
- Measure the current total discrepancy and segmental discrepancy.
- Decide whether the short limb is truly short, the long limb is overgrown, or both are contributing.
- Determine skeletal maturity using bone age or a validated knee maturity method where appropriate.
- Estimate predicted discrepancy at maturity using a recognised method.
- Check the estimate against prior measurements. A single radiograph is weaker than a trend.
- Calculate whether the chosen physis has enough remaining growth to close the gap.
- Counsel the family that prediction error can leave residual discrepancy or overcorrection.
Menelaus-style mental check
This is not a substitute for formal prediction, but it is useful for sense-checking the plan.
- Approximate skeletal maturity: girls around 14 years, boys around 16 years, adjusted for bone age and puberty.
- Approximate growth remaining around the knee: distal femur about 9 mm per year, proximal tibia about 6 mm per year.
- Distal femoral epiphysiodesis alone therefore corrects less than combined distal femoral and proximal tibial epiphysiodesis over the same time.
- If predicted correction required exceeds the remaining growth capacity, epiphysiodesis alone cannot solve the problem.
- Best tool
- Standing block test
- Management implication
- Functional correction and gait response.
- Best tool
- Clinical examination plus block response
- Management implication
- Avoids treating scoliosis, contracture or foot height as bone length.
- Best tool
- Calibrated femur and tibia measurement
- Management implication
- Guides distal femoral, proximal tibial or combined epiphysiodesis.
- Best tool
- Bone age plus multiplier, Moseley or growth remaining method
- Management implication
- Determines timing and treatment ladder.
- Best tool
- MRI or CT physeal mapping
- Management implication
- Determines whether bar resection, guided growth, osteotomy or epiphysiodesis is appropriate.
- Best tool
- Joint-specific imaging and clinical stability assessment
- Management implication
- Identifies hip, knee, ankle or foot problems that must be corrected or protected.
Using the Paley Multiplier
The multiplier method is named as a core prediction tool, but it is worth knowing the actual arithmetic. The multiplier (M) is the ratio of a bone's length at maturity to its length now (M = mature length divided by current length), read from published age- and sex-specific tables. How you apply it depends on whether the discrepancy is proportional.
- How to use the multiplier
- Predicted discrepancy at maturity = current discrepancy multiplied by M (both limbs scale by the same multiplier, so their difference scales too)
- Caveat
- Assumes the discrepancy stays proportional - typical of congenital cases
- How to use the multiplier
- Predict each limb (or segment) separately as current length multiplied by M, then take the difference; do NOT simply multiply the current discrepancy
- Caveat
- Acquired/arrest discrepancies are not proportional, so the simple shortcut over- or under-estimates
- How to use the multiplier
- Growth remaining in a physis is about the predicted mature length minus the current length; use it to check whether arrest can close the predicted gap and to time surgery
- Caveat
- Based on chronological age - correct with bone age if skeletal and chronological age diverge
- How to use the multiplier
- Fast - needs only age, sex and a single current measurement
- Caveat
- Still cross-check against the serial clinical trend; abnormal growth breaks the proportionality assumption
The Paley multiplier (M) is the ratio of a bone's length at maturity to its length now (M = mature length divided by current length), read from age- and sex-specific tables. For a CONGENITAL (proportional) discrepancy you simply multiply: predicted discrepancy at maturity = current discrepancy multiplied by M. For a DEVELOPMENTAL or ACQUIRED discrepancy the difference is not proportional, so you must predict each limb separately (current length multiplied by M) and take the difference rather than multiplying the current gap. Its great strength is speed - a single visit with age, sex and one measurement - but it assumes chronological age tracks skeletal maturity, so correct with bone age when they diverge and always cross-check against the serial trend.
Differential Diagnosis
The differential is about avoiding a false diagnosis of bony LLD. The key discriminators are the response to the standing block test, whether the inequality is in the bone or the soft tissue/posture, and whether one limb is genuinely short or the other is overgrown.
- Distinguishing feature
- Real difference in femur, tibia or foot height.
- Best discriminating test
- Calibrated standing radiograph or scanogram with segmental measurement.
- Why it changes management
- Eligible for lift, epiphysiodesis, shortening or lengthening.
- Distinguishing feature
- Pelvic obliquity and curve correct when blocks level the limbs.
- Best discriminating test
- Block test plus standing spine radiograph levelled and unlevelled.
- Why it changes management
- Treat the length, not the spine; curve resolves with equalisation.
- Distinguishing feature
- Curve and rotation persist despite block correction.
- Best discriminating test
- Standing radiograph with Adams forward bend and Cobb angle.
- Why it changes management
- Spinal deformity needs its own pathway; do not arrest growth for the curve.
- Distinguishing feature
- Limb appears short (adduction) or long (abduction) with pelvis tilted.
- Best discriminating test
- Examination of hip range with Thomas and abduction in extension.
- Why it changes management
- Releasing contracture can change the apparent measurement and the operation.
- Distinguishing feature
- Functional shortening with fixed flexion on the affected side.
- Best discriminating test
- Prone or supine knee extension assessment.
- Why it changes management
- Correcting contracture may remove most of the apparent inequality.
- Distinguishing feature
- Cavus, planovalgus, vertical talus or partial foot deficiency alters functional height.
- Best discriminating test
- Standing foot examination and weight-bearing foot/ankle radiographs.
- Why it changes management
- Foot height is not corrected by epiphysiodesis; needs shoe or foot surgery.
- Distinguishing feature
- Limp does not improve when the pelvis is levelled with blocks.
- Best discriminating test
- Targeted hip/knee imaging for Perthes, SCFE, infection or tumour.
- Why it changes management
- A painful pathology, not LLD, is driving gait; treat the cause.
- Distinguishing feature
- Tone, weakness and pelvic obliquity dominate gait more than length.
- Best discriminating test
- Neurological examination, tone and selective motor control assessment.
- Why it changes management
- Function and contracture, not the centimetre value, often lead management.
- Distinguishing feature
- One limb is long rather than the other being short; may have skin or girth asymmetry.
- Best discriminating test
- Whole-limb examination, segment measurement and overgrowth screen.
- Why it changes management
- Overgrowth syndromes need surveillance and may need tumour screening pathways.
Management
Management principles
The management decision is made in this order:
- Confirm true versus apparent discrepancy.
- Measure current discrepancy clinically and radiographically.
- Localise femur, tibia, foot and axis contributions.
- Estimate maturity discrepancy.
- Place the child into a treatment threshold.
- Check whether contracture, angular deformity, joint instability or foot deficiency changes the plan.
- Choose the least burdensome treatment that achieves a functional goal.
- Explain prediction error, residual inequality and treatment burden.
- Usual strategy
- Observe, insole, internal heel raise, external shoe raise if symptomatic.
- Key decision factors
- Symptoms, gait response to blocks, sport, back pain, cosmesis and family preference.
- Usual strategy
- Timed epiphysiodesis if growth remains; shortening or lift if near maturity.
- Key decision factors
- Bone age, growth remaining, femur versus tibia contribution, acceptable residual LLD.
- Usual strategy
- Lengthening, staged reconstruction, combined procedures or prosthetic pathway.
- Key decision factors
- Joint stability, soft tissues, diagnosis, family capacity, number of stages required.
- Usual strategy
- Bar resection, guided growth, osteotomy, epiphysiodesis or lengthening depending bar size and growth remaining.
- Key decision factors
- Bar location, deformity, remaining growth, joint line, mechanical axis and family expectations.
- Usual strategy
- Treat deformity and function, not the centimetre number alone.
- Key decision factors
- Contracture, malalignment, foot height, hip/knee/ankle stability and neuromuscular control.
The classic threshold ladder is useful: observe or lift for mild discrepancy, epiphysiodesis for predicted 2 to 5 cm with growth remaining, and lengthening or reconstruction for larger discrepancy. But the final decision changes with symptoms, diagnosis, maturity, deformity, foot and joint quality, and family capacity.
When to use
Observation and lifts are usually first-line for predicted discrepancy less than 2 cm, uncertain early measurements, minimal symptoms or families who prefer non-operative care.
What to offer
- Insole or heel raise for small discrepancies.
- Internal shoe lift when shoe volume allows.
- External shoe raise for larger correction.
- Physiotherapy only if compensatory tightness, weakness or gait adaptation exists.
- Surveillance imaging in a growing child because the predicted discrepancy may change.
Practical points
Do not prescribe a lift blindly. Test with blocks, observe gait, and ask whether pain or fatigue improves. Long-standing discrepancies may need gradual lift introduction. A lift corrects function; it does not treat progression.
Lift details
- A small correction can usually be placed inside the shoe.
- Larger correction often needs an external shoe raise.
- Full correction is not always tolerated immediately, especially after long-standing compensation.
- A lift may be definitive, temporary while awaiting maturity, or a bridge to surgery.
- In growing children, repeat prediction because today's mild discrepancy may not remain mild.
Clinical Pitfalls and Management Scripts
Common pitfalls
- Starting with "I would get a scanogram" before saying true versus apparent discrepancy.
- Forgetting the block test.
- Treating the current discrepancy instead of predicted maturity discrepancy.
- Using chronological age alone.
- Forgetting femur versus tibia contribution.
- Ignoring foot height.
- Ignoring angular deformity.
- Offering lengthening without joint stability assessment.
- Calling epiphysiodesis "simple" without discussing timing error.
- Assuming equal legs is always the goal.
Structured case presentation
Use this structure:
- "This child has a suspected limb length discrepancy. I would first distinguish true from apparent discrepancy."
- "I would observe gait and level the pelvis with blocks."
- "I would examine spine, hips, knees, ankles, feet and neurology."
- "I would measure femur, tibia and total limb length using calibrated imaging."
- "I would assess bone age and predict discrepancy at maturity."
- "I would decide whether observation, lift, epiphysiodesis, shortening, lengthening or reconstruction best matches the child."
- "I would discuss prediction error and follow until maturity."
Concise epiphysiodesis summary
"Epiphysiodesis is timed growth arrest of the longer limb. I would only offer it after confirming true anatomical LLD, identifying the responsible segment, estimating bone age and predicted maturity discrepancy, and confirming enough growth remains. I would counsel about undercorrection, overcorrection, angular deformity, residual inequality and the need for follow-up to maturity."
Concise lengthening summary
"Lengthening is considered for larger discrepancies or congenital deficiency pathways, but it requires stable joints, correctable alignment, good range of motion, family commitment and prolonged rehabilitation. The risks include regenerate problems, stiffness, subluxation, nerve stretch, infection, pain and residual discrepancy."
Operative Technique
Timed epiphysiodesis: what the surgeon must know
Epiphysiodesis is not one operation; it is a family of techniques that slow or stop growth in the longer limb. The operative method matters, but timing matters more.
Preoperative checklist
- Confirm current LLD, predicted maturity LLD and acceptable residual inequality.
- Confirm bone age and growth remaining.
- Confirm long limb, long segment and exact physis.
- Review femoral and tibial lengths, mechanical axis and joint status.
- Decide whether distal femur, proximal tibia, both, fibula, or an associated angular correction is needed.
- Mark the operative side carefully because wrong-side surgery is a catastrophic error.
- Explain that equalisation occurs gradually during remaining growth, not immediately.
Which physis to stop
The physis chosen should match the measured segmental discrepancy and the predicted correction required.
- Likely target
- Distal femoral epiphysiodesis
- Important caveat
- Largest single contributor around the knee; check coronal and sagittal alignment.
- Likely target
- Proximal tibial epiphysiodesis
- Important caveat
- Consider the proximal fibula selectively to avoid relative fibular overgrowth or ankle/knee imbalance.
- Likely target
- Combined distal femur and proximal tibia
- Important caveat
- Useful for larger moderate discrepancies if enough growth remains.
- Likely target
- Epiphysiodesis will not correct it
- Important caveat
- Plan shoe modification, foot reconstruction or prosthetic strategy when relevant.
- Likely target
- Bar resection, completion arrest, guided growth or osteotomy
- Important caveat
- Map the bar before choosing a length operation.
Permanent percutaneous epiphysiodesis
The aim is controlled physeal ablation.
Technique principles:
- General anaesthesia or appropriate paediatric anaesthesia.
- Supine positioning with fluoroscopy.
- AP and lateral image confirmation of the physis.
- Small medial and lateral incisions or percutaneous access depending technique.
- Drill, burr or curette the physis sufficiently to create a physeal bridge.
- Confirm physeal ablation radiographically.
- Avoid asymmetric ablation that may cause varus, valgus, procurvatum or recurvatum.
- Close wounds and allow protected or early mobilisation according to local protocol.
Pitfalls:
- Wrong side.
- Wrong physis.
- Insufficient ablation causing continued growth.
- Asymmetric ablation causing angular deformity.
- Injury to joint, neurovascular structures or proximal tibial tubercle region.
Practical details:
- Ablate both medial and lateral sides symmetrically when the aim is pure length arrest.
- Maintain awareness of the joint line and avoid intra-articular penetration.
- In the proximal tibia, respect the tibial tubercle apophysis and the lateral neurovascular anatomy.
- Document fluoroscopic confirmation of level, side and implant or ablation position.
- Continue radiographic surveillance because growth arrest is a biologic response, not just a completed operation.
Percutaneous transphyseal screws
PETS uses screws crossing the physis to slow growth. It is minimally invasive and commonly permits rapid mobilisation. It is attractive around the distal femur and proximal tibia, but it still needs accurate timing, careful screw placement and follow-up.
Advantages:
- Small incisions.
- Short operative time.
- Early mobilisation.
- Hardware can sometimes be removed if clinically required.
Problems:
- Hardware irritation.
- Incomplete arrest.
- Rebound or continued growth after removal.
- Angular deformity if screw placement or physeal response is asymmetric.
- Proximal tibial screw trajectory requires attention to deep peroneal nerve proximity.
Temporary tension-band plates or staples
Temporary implants may slow growth and later be removed. They are more commonly used for guided growth angular correction, but can be considered in selected length problems.
Advantages:
- Potentially reversible.
- Useful if angular correction is also required.
- Avoids complete physeal destruction.
Problems:
- Slower and less predictable for pure length correction.
- Requires removal.
- Rebound growth may occur.
- Hardware irritation or migration can occur.
For pure LLD, temporary tethering should not be presented as automatically equivalent to definitive epiphysiodesis. It can work, but some series report lower efficiency and revision burden, especially when used where a predictable definitive arrest is needed.
Lengthening operations
Lengthening requires the surgeon to manage bone, soft tissue and joints together.
- Key action
- Decide femur, tibia or both; correct angular or rotational deformity simultaneously or in a planned stage.
- Failure to avoid
- Lengthening the wrong segment or magnifying malalignment.
- Key action
- Perform low-energy osteotomy or corticotomy and stabilise with frame, nail or combined construct.
- Failure to avoid
- Poor regenerate biology or unstable fixation.
- Key action
- Wait through latency, then distract gradually while monitoring regenerate and joints.
- Failure to avoid
- Fast distraction, nerve symptoms, joint subluxation or poor regenerate.
- Key action
- Protect until regenerate is strong enough for progression.
- Failure to avoid
- Fracture or deformity through immature regenerate.
- Key action
- Remove frame or implant when safe and continue rehabilitation until gait, strength and range recover.
- Failure to avoid
- Stopping follow-up when the bone unites but function remains poor.
External fixation options:
- Monolateral fixator for simple lengthening.
- Circular frame for lengthening with stability needs, small bone segments or deformity.
- Hexapod frame for multiplanar deformity correction and lengthening.
Internal lengthening options:
- Motorised intramedullary nail in appropriate older children and adolescents.
- Requires adequate bone size, open growth-plate considerations, joint protection and implant availability.
- Avoid when canal size, age, deformity, infection risk or joint instability makes the nail unsafe.
Lengthening-specific technical priorities:
- Prevent hip, knee and ankle contracture.
- Use physiotherapy from the start.
- Monitor regenerate density and shape.
- Slow or pause distraction if regenerate is poor or nerves/joints become symptomatic.
- Consider prophylactic joint spanning or soft-tissue release in high-risk congenital deficiency.
Physeal bar resection principles
Bar resection is a reconstruction of growth, not a standard length-equalisation operation.
- Why it matters
- Complete arrest or inaccessible bars are poor candidates.
- Common failure
- Attempting restoration where meaningful growth cannot return.
- Why it matters
- The child must have enough growth left for resection to matter.
- Common failure
- Technically successful surgery with no clinical benefit.
- Why it matters
- MRI or CT defines bar size, location and approach.
- Common failure
- Incomplete resection or damage to normal physis.
- Why it matters
- Remove the bar while protecting remaining physis.
- Common failure
- Recurrent arrest or iatrogenic growth damage.
- Why it matters
- Guided growth, osteotomy or epiphysiodesis may still be needed.
- Common failure
- Treating growth restoration but leaving angulation or predicted LLD.
The operation is particularly unforgiving because incomplete bar removal may fail, and excessive resection can damage remaining growth potential.
Segment selection
Segment selection should match the measured discrepancy:
- Long femur: distal femoral epiphysiodesis.
- Long tibia: proximal tibial epiphysiodesis.
- Both femur and tibia: combined around-knee epiphysiodesis.
- Foot height difference: epiphysiodesis will not correct the foot component.
- Angular deformity: may need guided growth or osteotomy in addition to length management.
- Proximal femur and distal tibia: include them in prediction, but do not choose them automatically for routine LLD arrest.
Complications and Follow-up
Prediction complications
- Residual discrepancy at maturity.
- Undercorrection if surgery is too late.
- Overcorrection if surgery is too early.
- Wrong segment treated.
- Failure to account for bone age or pubertal timing.
- Failure to update prediction with serial data.
Epiphysiodesis complications
- Continued growth from incomplete arrest.
- Angular deformity from asymmetric arrest.
- Hardware irritation or screw prominence.
- Knee pain or stiffness.
- Infection or wound problem.
- Reduced final height.
- Need for contralateral or revision procedure if prediction proves wrong.
Shortening complications
- Nonunion or delayed union.
- Hardware irritation.
- Malrotation.
- Weakness from excessive shortening.
- Loss of height.
Lengthening complications
- Pin-site infection or implant-related pain.
- Poor regenerate or delayed consolidation.
- Regenerate fracture.
- Joint stiffness.
- Hip, knee or ankle subluxation.
- Nerve stretch symptoms.
- Muscle contracture.
- Psychological fatigue and family burnout.
- Residual discrepancy or recurrent deformity.
Follow-up
Follow-up must continue beyond the operation:
- Recheck clinical block height.
- Repeat calibrated imaging.
- Monitor axis as well as length.
- Confirm the physis has responded.
- Adjust shoe lift during growth.
- Watch for overcorrection.
- Follow to skeletal maturity.
A successful wound review does not mean successful epiphysiodesis. The endpoint is acceptable limb length and alignment at skeletal maturity.
Guidelines, Registries & Global Practice
There is no single high-level international guideline that dictates limb length discrepancy (LLD) thresholds. Practice is built on consensus, narrative reviews and registry-style cohorts rather than randomised trials, and the major bodies (AAOS, the British Society for Children's Orthopaedic Surgery, EFORT/EPOS in Europe, and the deformity-correction community around the AO and Paley schools) converge on a similar treatment ladder while differing in emphasis and the strength of the evidence they cite.
Global epidemiology
Mild anatomical inequality is near universal; it is the magnitude and the symptoms, not the mere presence of inequality, that define a clinical problem.
Anatomical leg-length inequality is near universal but usually small
- Using accurate radiographic methods, anatomical leg-length inequality was present in about 90 percent of people.
- The mean magnitude was only 5.2 mm (SD 4.1 mm), so most inequality is small.
- Inequality did not appear clinically significant for most people until it reached approximately 20 mm.
Shoe lifts: low-quality evidence for symptom relief, guidelines inconsistent
- Across non-randomised studies, about 88 percent of treated adults reported partial or complete pain relief with a shoe lift.
- Overall study quality was low or poor, and only one randomised controlled trial was identified.
- Of nine guidelines reviewed, only two recommended shoe lift use, and those were based on consensus.
How guidance differs across regions
- Position on LLD management
- Treatment-ladder consensus: observe or lift for predicted discrepancy under 2 cm, epiphysiodesis for predicted 2 to 5 cm with growth remaining, lengthening or reconstruction for over 5 cm.
- Evidence strength
- Consensus and review level; no Grade A trial evidence for thresholds.
- Position on LLD management
- Same broad ladder with strong emphasis on multidisciplinary deformity units, calibrated EOS or long-leg imaging and family-centred counselling about treatment burden.
- Evidence strength
- Consensus; centralisation of complex lengthening to specialist centres is custom rather than published mandate.
- Position on LLD management
- Endorses prediction-based timing (Green-Anderson, Moseley, multiplier) and individualised, elective decision-making; the cited German consensus states the decision to treat is always elective.
- Evidence strength
- Narrative review and consensus (Vogt et al, Dtsch Arztebl Int 2020).
- Position on LLD management
- Multiplier method for prediction; structured selection for distraction osteogenesis with frames or motorised nails; stable joints and plantigrade foot are prerequisites.
- Evidence strength
- Validation and Level IV cohort evidence; technique superiority unproven.
- Position on LLD management
- External fixators remain the dominant lengthening tool where motorised nails are unavailable; shoe raises and timed epiphysiodesis are the most accessible interventions.
- Evidence strength
- Practice variation driven by access and cost, not by differing evidence.
Registry and practice-variation evidence
There is no dedicated international LLD registry equivalent to arthroplasty registries. The best registry-style evidence comes from large single-centre and institutional cohorts that prospectively track lengthening and epiphysiodesis to maturity, and these show that method selection - motorised intramedullary nails, epiphysiodesis around the knee, or external fixation - varies widely even within a single expert centre. Practice variation between centres and countries reflects implant availability, cost, family capacity for prolonged rehabilitation and surgeon training far more than disagreement about the underlying treatment ladder.
The treatment ladder (observe/lift under 2 cm, epiphysiodesis 2 to 5 cm, lengthening or reconstruction over 5 cm) is internationally consistent, but it rests on consensus, not randomised trials. A strong exam answer states the ladder and then acknowledges that thresholds are consensus-based and decisions are elective and individualised.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 10-year-old child is referred with a limp and suspected limb length discrepancy. How do you assess them?”
“A growing child has a predicted 3 cm discrepancy at maturity. When would you consider epiphysiodesis?”
“A child with fibular hemimelia has a large predicted discrepancy. How does your approach differ?”
“A teenager has residual discrepancy after epiphysiodesis. What went wrong and what do you do?”
Opening Line
- True versus apparent first
- Block test levels pelvis
- Measure femur and tibia
- Predict maturity discrepancy
- Apply less than 2, 2 to 5, more than 5 cm thresholds
Investigations
- Standing blocks
- EOS or scanogram
- Long-leg alignment
- Bone age
- Green-Anderson, Moseley, multiplier, serial measurements
Treatment Ladder
- Less than 2 cm: observe/lift
- 2 to 5 cm: epiphysiodesis if growing
- Near maturity: lift or shortening
- More than 5 cm: lengthening/reconstruction
- Complex deficiency: whole-limb life-plan
Do Not Miss
- Pelvic obliquity
- Hip contracture
- Foot height
- Angular deformity
- Joint instability
Complications
- Residual LLD
- Overcorrection
- Undercorrection
- Angular deformity
- Lengthening stiffness and regenerate problems
Evidence Base
Treatment indications are elective and individualised
- The evidence base for exact LLD treatment indications is limited.
- Prediction algorithms estimate final discrepancy but have clinically relevant error.
- Treatment should be individualised; the discrepancy size is not the sole determinant.
Multiplier method validation
- The multiplier method was clinically validated for predicting LLD and epiphysiodesis outcome.
- Prediction error still exists and must be included in counselling.
- The method was compared with Moseley prediction.
Prediction variability
- Green-Anderson, Moseley and Paley methods can produce different final predictions.
- PETS improved discrepancy but timing and variability remained important.
- Hardware symptoms can occur even when major complications are avoided.