Anatomy, predicted growth, foot function and lifetime mobility planning
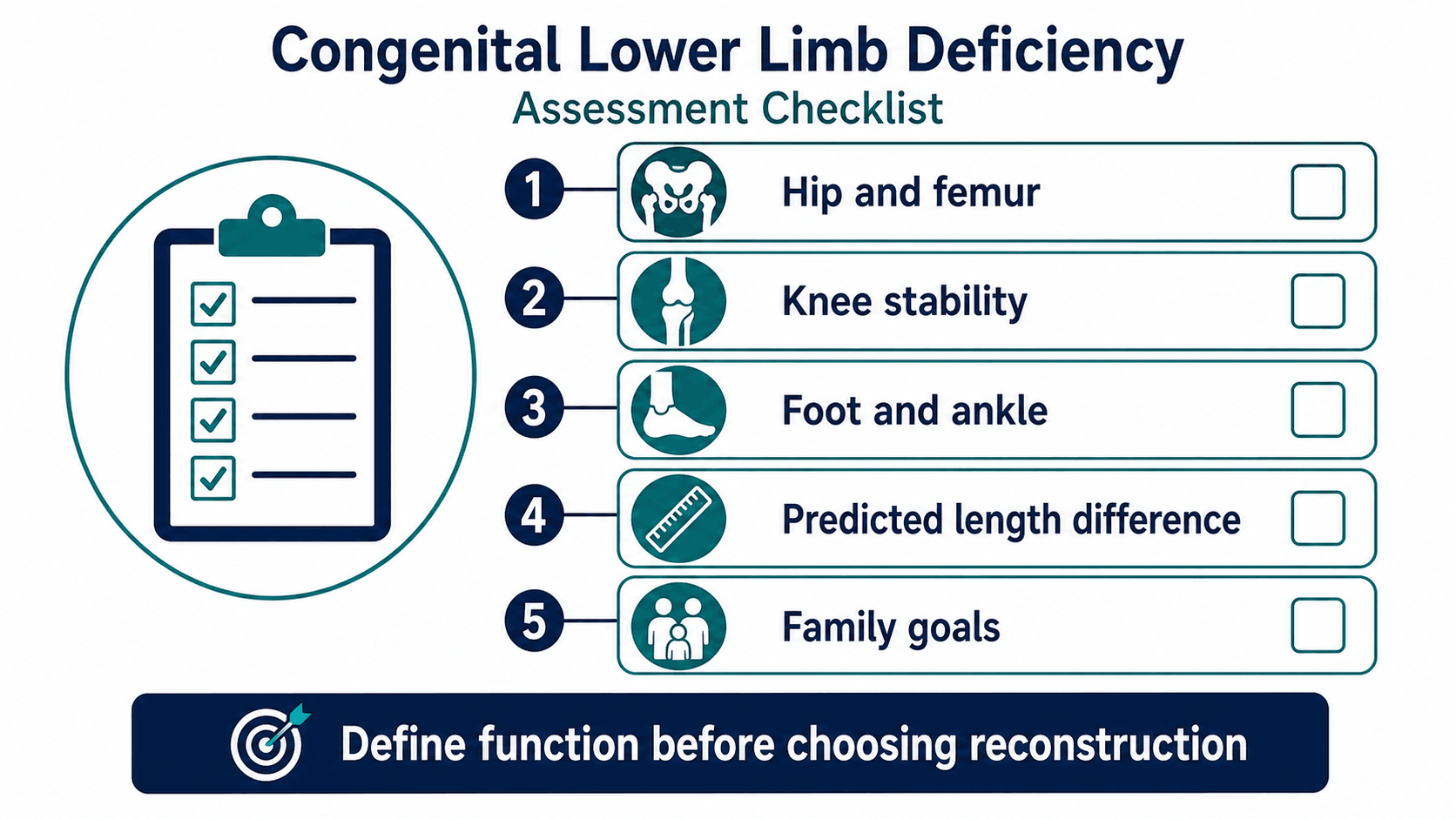
- Do not reduce congenital limb deficiency to centimetres; hip, knee, ankle, foot, soft tissue and prosthetic function change the plan.
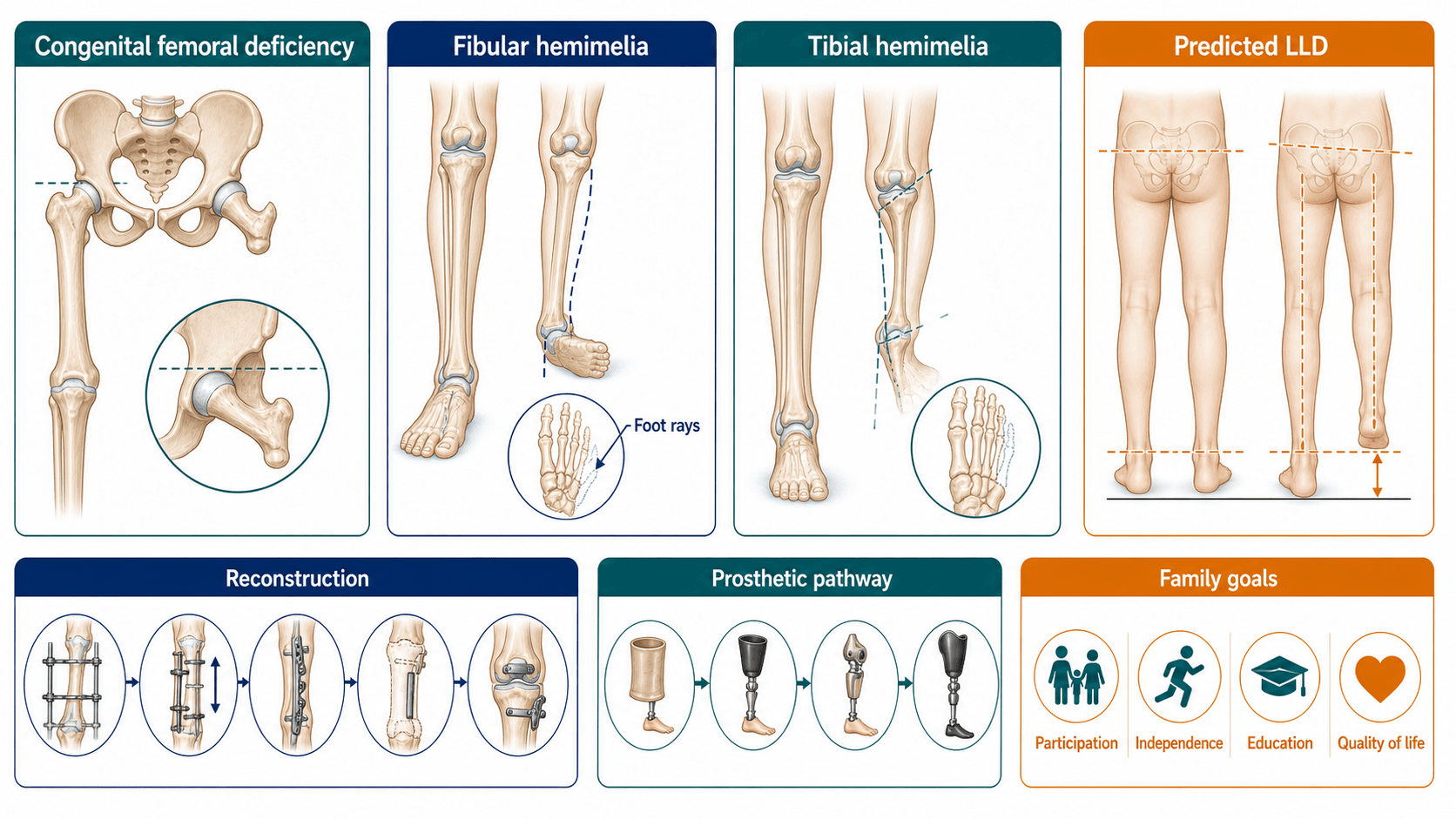
- Congenital femoral deficiency requires assessment of proximal femur, hip stability, knee stability, predicted LLD and possible prosthetic or rotationplasty pathways.
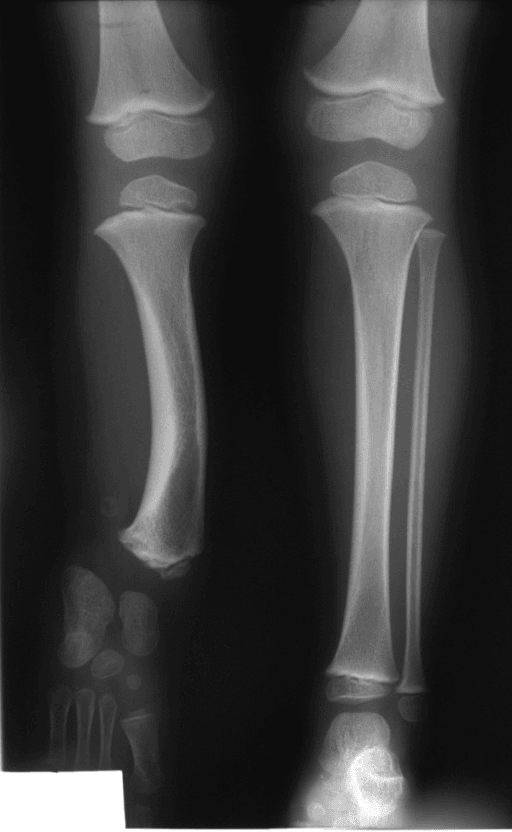
- Fibular hemimelia is a postaxial deficiency; foot rays, ankle valgus, subtalar coalition, knee valgus and knee ligament deficiency are central.
- Tibial hemimelia is rare and often severe; knee extension mechanism, foot support and reconstructability determine whether salvage is realistic.
- Lengthening must be staged around joint stability, nerve stretch, regenerate quality, family burden and rehabilitation capacity.
- Amputation or rotationplasty can be planned functional reconstruction, not failure, when anatomy makes limb preservation a poor mobility strategy.
- “A longer limb with an unstable knee or non-plantigrade foot may function worse than a shorter limb with a good prosthesis.
- “Foot height contributes to total discrepancy and should be included in prediction.
- “A plantigrade, painless, shoeable foot is a prerequisite for many reconstruction pathways.
- “Knee cruciate deficiency may be asymptomatic in a small child but problematic during growth and lengthening.
- “The family needs neutral comparison of burden, risks and expected mobility for each pathway.
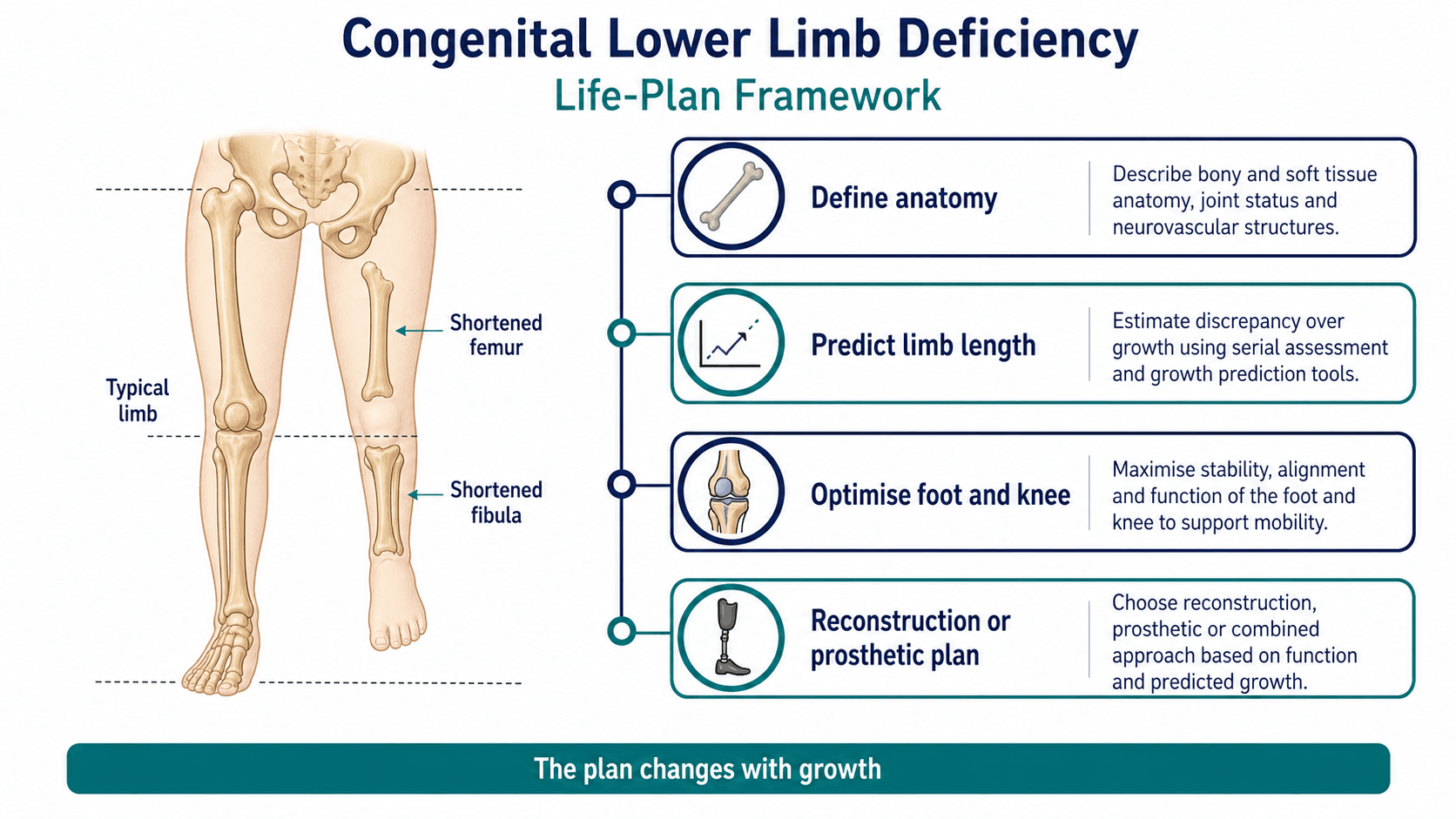
Length prediction is essential, but it is only one part of decision-making. A safe plan also proves that the hip, knee, ankle, foot, soft tissues and family can tolerate the pathway.
Images and Diagrams
- Practical answer
- Define anatomy across pelvis, femur, knee, tibia, fibula, ankle and foot.
- Clinical use
- Prevents length-only decision-making.
- Practical answer
- Limb length discrepancy at maturity, including segment and foot-height contribution.
- Clinical use
- Estimates number and type of equalisation procedures.
- Practical answer
- Hip, knee and ankle stability during growth and lengthening.
- Clinical use
- Avoids subluxation and failed reconstruction.
- Practical answer
- Painless, stable, efficient mobility with a realistic treatment burden.
- Clinical use
- Allows neutral comparison of reconstruction and prosthetic pathways.
LIMBAssessment
Hook:LIMB keeps the assessment broader than centimetres.
FOOTFibular Hemimelia
Hook:FOOT keeps the foot and ankle central in fibular hemimelia.
PLANLife Plan
Hook:PLAN reminds the learner that this is growth-long care.
Overview/Epidemiology
Congenital lower limb deficiency includes a spectrum of femoral, fibular, tibial and foot deficiencies. The child may present at birth with an obvious short limb, missing rays or foot deformity, or later when gait asymmetry, shoe wear, brace difficulty or limb length discrepancy becomes apparent.
The visible discrepancy is only the surface problem. The real decision is whether the limb can become a stable, pain-free, efficient lever for walking.
- What good looks like
- Contained, mobile and able to support the pelvis.
- Why it changes treatment
- Unstable proximal femur or poor abductor function may limit reconstruction.
- What good looks like
- Stable, mobile and controllable in stance.
- Why it changes treatment
- Cruciate deficiency, valgus or extensor deficiency can make lengthening unsafe.
- What good looks like
- Plantigrade, shoeable or prosthesis-friendly.
- Why it changes treatment
- A non-reconstructable foot may make prosthetic care more functional than repeated salvage.
- What good looks like
- Skin, vessels, nerves and muscles can tolerate treatment.
- Why it changes treatment
- Nerve stretch, contracture and regenerate problems increase during lengthening.
- What good looks like
- The child and family can complete staged care and rehabilitation.
- Why it changes treatment
- A technically possible pathway may still be the wrong burden.
Pathophysiology
The deficiency pattern reflects abnormal limb formation rather than a postnatal injury. Each diagnosis is a whole-limb pattern, not a single missing bone.
- Typical anatomy
- Short abnormal femur, proximal femoral abnormality, variable hip and knee involvement.
- Treatment consequence
- Hip containment, abductor function and knee stability decide whether lengthening is realistic.
- Typical anatomy
- Fibular deficiency, lateral ray absence, ankle/subtalar deformity, tibial bowing, knee valgus and cruciate deficiency.
- Treatment consequence
- Foot and ankle reconstructability often drives reconstruction versus prosthetic planning.
- Typical anatomy
- Preaxial deficiency with variable tibia, knee extensor mechanism, ankle support and foot position.
- Treatment consequence
- Severe patterns may be better treated with prosthetic or amputation pathway.
Limb length discrepancy commonly increases proportionally with growth. Segment contribution matters: femoral shortening, tibial shortening and reduced foot height all add to the final difference. The child also adapts: ball-and-socket ankle, pelvic obliquity, compensatory equinus, shoe lifts, brace reliance and altered gait may appear as growth progresses.
The lengthening biology is also abnormal. Short soft tissues, altered nerves and vessels, deficient muscles and unstable joints make repeated lengthening more hazardous than ordinary limb equalisation. This is why reconstruction planning starts with stability and foot function before the amount to lengthen.
Classification
Classifications are useful only if they guide treatment. For congenital femoral deficiency, classifications describe proximal femoral anatomy and reconstructability. For fibular hemimelia, older systems described fibular absence, but modern treatment planning places more weight on foot and ankle deformity, rays, coalition and stability. For tibial hemimelia, classifications describe the amount of tibia present and knee or ankle reconstructability.
- Congenital femoral deficiency: short abnormal femur with variable hip and knee involvement.
- Fibular hemimelia: fibular deficiency with lateral foot ray and ankle/foot deformity.
- Tibial hemimelia: tibial deficiency with severe knee, ankle and foot implications.
- Mixed longitudinal deficiency: combined femoral, fibular, tibial and foot involvement.
The classic classification of congenital femoral deficiency (proximal focal femoral deficiency, PFFD) is the Aitken classification, based on the presence of the femoral head and the femoral segment - and it directly predicts hip stability and reconstructability:
- Aitken A: femoral head present with an adequate acetabulum; short femur with a subtrochanteric defect that ossifies and unites - the most reconstructable, hip stable.
- Aitken B: femoral head present but the acetabulum is more dysplastic; a pseudarthrosis between the head and the short femoral shaft that does NOT unite (a tuft of bone on the proximal shaft).
- Aitken C: femoral head absent or only a small ossific tuft, with a severely dysplastic acetabulum and no connection between head and shaft.
- Aitken D: both the femoral head and the acetabulum are absent - the most severe, with no hip joint.
The modern Paley classification of CFD refines this around what can be reconstructed (Type 1 intact femur with a mobile stable hip and knee; Type 2 mobile pseudarthrosis; Type 3 diaphyseal deficiency), guiding the lengthening-versus-prosthetic decision. The exam point: a present, stable femoral head and acetabulum (Aitken A / Paley 1) is the prerequisite for lengthening reconstruction, whereas an absent head/acetabulum (Aitken C/D) pushes toward a prosthetic or rotationplasty pathway.
Clinical Presentation
History
- Ask specifically
- How it was recognised, prenatal imaging, other limb findings and systemic anomalies.
- Why it matters
- Defines whether this is isolated or part of a broader syndrome.
- Ask specifically
- Crawling, standing, walking distance, stairs, running, sport, falls, pain and fatigue.
- Why it matters
- Determines whether the current limb is useful and what must improve.
- Ask specifically
- Braces, prostheses, sockets, shoe raises, pressure areas and skin breakdown.
- Why it matters
- Shows whether orthotic or prosthetic care is succeeding.
- Ask specifically
- Casts, foot reconstruction, lengthening, epiphysiodesis, amputation, revision surgery and psychological impact.
- Why it matters
- Identifies scars, expectations and remaining options.
- Ask specifically
- Limb preservation, fewer operations, sport, shoe wear, appearance, independence and predictable mobility.
- Why it matters
- Makes counselling honest rather than surgeon-centred.
Examination
Examine from pelvis to toes, then watch gait with and without the orthosis or prosthesis.
- Assess
- Pelvic balance, hip abduction, flexion, containment and Trendelenburg.
- Decision it informs
- Whether the limb can support walking and lengthening.
- Assess
- Femoral length, knee range, valgus, sagittal stability, patellar tracking and extensor mechanism.
- Decision it informs
- Whether the knee is safe for reconstruction or prosthetic control.
- Assess
- Tibial bowing, ankle valgus/equinus, subtalar motion, rays, width, callosities and shoeability.
- Decision it informs
- Whether the foot is reconstructable, braceable or prosthesis-friendly.
- Assess
- Femur, tibia and foot-height contribution.
- Decision it informs
- Prevents treating a total discrepancy without knowing the segment.
- Assess
- Skin, scars, sockets, pressure areas and tolerance.
- Decision it informs
- Predicts complication risk and practical pathway burden.
A plan that looks elegant on a radiograph can fail if the child cannot tolerate the treatment burden or if the final limb is not useful for daily life.
Investigations
Radiographs should answer treatment questions. Full-length calibrated standing films, with an appropriate block under the short limb when possible, help measure segment lengths, mechanical axis and pelvic balance. Dedicated hip, knee, ankle and foot radiographs define reconstructability. In younger children, cartilage and unossified structures may limit plain film interpretation.
MRI is useful in selected cases: hip cartilage, knee cruciate absence, fibular anlage, subtalar coalition, soft tissue and vascular anomalies can all change reconstruction planning. CT may help complex foot and ankle or rotational planning but should be used selectively.
- Investigation
- Calibrated full-length limb radiographs.
- Decision it informs
- Femur, tibia, foot height and mechanical axis.
- Investigation
- Dedicated hip, knee, ankle and foot imaging.
- Decision it informs
- Containment, cruciates, valgus, coalition and plantigrade potential.
- Investigation
- Serial measurements plus bone-age or multiplier-style prediction.
- Decision it informs
- Number of lengthenings, epiphysiodesis or prosthetic strategy.
- Investigation
- MRI or CT selectively.
- Decision it informs
- Cartilage, coalition, anlage, soft tissue or version detail.
- Useful method
- Serial calibrated lengths plus femur, tibia and foot-height measurement.
- How it changes the plan
- Prevents underestimating the real functional discrepancy.
- Useful method
- Multiplier method, Moseley straight-line graph or Green-Anderson growth-remaining method.
- How it changes the plan
- Determines whether shoe lift, epiphysiodesis, lengthening or prosthetic strategy is realistic.
- Useful method
- Projected LLD divided into safe staged gains after joint and foot preparation.
- How it changes the plan
- Large predicted discrepancies may make prosthetic or amputation pathways more predictable.
- Useful method
- Clinical and imaging assessment of hip containment, knee stability, ankle/foot position and soft-tissue envelope.
- How it changes the plan
- Unstable joints or non-plantigrade foot should be corrected or may redirect the pathway.
- Useful method
- Multidisciplinary review with limb reconstruction, prosthetics, therapy and family counselling.
- How it changes the plan
- Compares complete pathways rather than isolated procedures.
Major Conditions
Congenital femoral deficiency
- Key findings
- Femoral shortening, proximal femoral abnormality, hip containment, abductor function and knee stability.
- Treatment logic
- Stable mild patterns may suit staged lengthening; severe unstable patterns may need prosthetic strategy, rotationplasty or other reconstruction.
- Key findings
- LLD, fibular deficiency, lateral ray absence, ankle valgus/equinovalgus, coalition, tibial bowing, knee valgus and cruciate deficiency.
- Treatment logic
- A stable plantigrade foot supports reconstruction; a severely deficient non-shoeable foot may do better with prosthetic pathway.
- Key findings
- Partial or absent tibia, knee flexion contracture, deficient extensor mechanism, ankle instability and foot deformity.
- Treatment logic
- Reconstruction is possible in selected specialist settings, but amputation remains appropriate for many severe patterns.
- Key findings
- Combined femoral, fibular, tibial or foot involvement.
- Treatment logic
- Sequence treatment so hip, knee and foot stability are secured before lengthening exposes another weak level.
Differential Diagnosis
A short or deformed lower limb in a child is not always a longitudinal deficiency. The key task is to separate true congenital segmental deficiency from bowing, dysplasia, constriction and acquired growth arrest, because each has a different natural history and a different treatment pathway.
- Discriminating features
- Short abnormal femur, proximal femoral abnormality, variable hip and knee instability, often with coexisting fibular hemimelia.
- Why it changes the plan
- Hip and knee stability decide whether lengthening, prosthetic fitting or rotationplasty is realistic.
- Discriminating features
- Lateral (postaxial) deficiency, absent lateral rays, ankle valgus or ball-and-socket ankle, tarsal coalition, knee valgus and cruciate deficiency.
- Why it changes the plan
- Foot and ankle reconstructability is usually the pathway-defining issue.
- Discriminating features
- Medial (preaxial) deficiency, knee flexion contracture, deficient extensor mechanism, varus foot; may be familial or syndromic.
- Why it changes the plan
- Knee extensor function and tibial presence determine salvage versus amputation.
- Discriminating features
- Calcaneovalgus foot at birth, apex posteromedial bow that remodels, but predictable residual limb length discrepancy.
- Why it changes the plan
- Bowing largely corrects; the management issue is the discrepancy, not deficiency.
- Discriminating features
- Apex anterolateral bow, narrowed sclerotic canal, association with neurofibromatosis type 1.
- Why it changes the plan
- High fracture and non-union risk; must not be confused with benign posteromedial bowing.
- Discriminating features
- Circumferential skin grooves, distal transverse loss, asymmetric and non-genetic with normal proximal anatomy.
- Why it changes the plan
- Distal transverse pattern rather than longitudinal deficiency; soft-tissue and prosthetic focus.
- Discriminating features
- Disproportionate shortening, other dysmorphic features, family history or genetic diagnosis.
- Why it changes the plan
- Systemic condition needing geneticist input, not isolated limb reconstruction.
- Discriminating features
- Previously normal limb, physeal scar or bar, history of injury, sepsis or surgery.
- Why it changes the plan
- Targeted at the arrested physis (bar resection, epiphysiodesis, lengthening), not congenital reconstruction.
Management Principles
The first management step is not surgery. It is to explain the diagnosis, establish current function, predict future discrepancy and compare realistic pathways.
- Typical components
- Shoe lift, orthosis, prosthetic input, physiotherapy and serial prediction.
- When it makes sense
- Mild discrepancy, stable function, young age or uncertain final pathway.
- Typical components
- Foot/ankle correction, joint stabilisation, staged lengthening, epiphysiodesis and intensive rehabilitation.
- When it makes sense
- Reconstructable joints and foot, acceptable treatment burden and clear functional gain.
- Typical components
- Syme or Boyd amputation, rotationplasty, socket fitting and revisions through growth.
- When it makes sense
- Non-reconstructable foot/joints or when predictable mobility is better than repeated salvage.
- Typical components
- Orthosis or prosthesis plus limited reconstruction, later lengthening or epiphysiodesis.
- When it makes sense
- Child has useful anatomy but still needs long-term device support.
Mild discrepancy or stable function may be managed with monitoring, shoe lift, orthosis, physiotherapy, prosthetic review or delayed equalisation. Prediction should be updated through growth.
This topic repeatedly names three salvage procedures; know what each actually does:
- Syme amputation: an ankle disarticulation through the malleoli that removes the entire foot including the calcaneus, leaving an end-bearing stump capped by the durable heel pad sutured over the distal tibia. Simple and durable, but the heel pad can migrate and the stump is bulbous.
- Boyd amputation: a calcaneotibial fusion - the talus is removed but the calcaneus is preserved and fused to the distal tibia, giving a longer, more robust end-bearing stump and anchoring the heel pad so it cannot migrate (its advantage over Syme). It requires the fusion to heal and leaves a slightly longer limb (relevant in a growing child).
- Van Nes rotationplasty: for severe femoral deficiency, the limb is rotated 180 degrees so the ankle becomes a "knee" - active plantarflexion now extends the prosthetic shank and dorsiflexion flexes it, converting an above-knee amputee into the functional equivalent of a below-knee amputee with far better gait efficiency. The trade-off is the obvious cosmetic/psychosocial impact of a backward-facing foot, which must be discussed and is the main barrier to acceptance.
The unifying principle: amputation or rotationplasty is planned functional reconstruction that creates a stable, end-bearing, prosthesis-ready limb - not a failure of reconstruction.
Lengthening and Reconstruction Risks
Lengthening can be highly effective in selected children, but it is not a passive increase in bone length. It stresses bone, joints, muscle, nerve, vessel, skin and family life. The major preventable errors are lengthening before joint stability is secured, ignoring foot deformity, underestimating soft-tissue tightness, and failing to plan rehabilitation.
- Complications
- Poor regenerate, delayed union, fracture and recurrent deformity.
- Counselling point
- Lengthening requires repeated imaging and may need rate changes or revision.
- Complications
- Hip, knee or ankle subluxation, stiffness, contracture and nerve stretch palsy.
- Counselling point
- Joint protection and therapy are as important as the bone length.
- Complications
- Pin-site infection, hardware irritation, device problems and further surgery.
- Counselling point
- Device care and follow-up are part of the treatment.
- Complications
- Pain, school disruption, psychological fatigue and treatment abandonment.
- Counselling point
- The likely number of procedures and rehabilitation load must be discussed before starting.
Complications
Natural history complications
- Increasing limb length discrepancy.
- Progressive gait asymmetry and pelvic obliquity.
- Foot and ankle deformity limiting shoe wear.
- Knee valgus or instability.
- Pain, fatigue, falls and reduced activity.
Treatment complications
- Pin-site infection or deep infection.
- Poor regenerate, delayed union, fracture or hardware problems.
- Joint subluxation during lengthening.
- Knee, hip or ankle stiffness.
- Nerve stretch symptoms or palsy.
- Socket and skin problems after prosthetic fitting.
- Revision surgery through growth.
- Family and child treatment fatigue.
Lengthening is valuable only if it creates a stable, aligned and useful limb. A longer unstable limb is not a success.
Counselling and Follow-up
Counselling should be neutral and specific. Families should hear that reconstruction and prosthetic care can both be excellent when matched to anatomy. Avoid framing amputation as giving up or reconstruction as automatically superior. Discuss what the child is likely to experience: number of operations, therapy, pain, device time, school disruption, sport participation, prosthetic revisions, cosmesis and psychological support.
Follow-up should update prediction, function and goals. A plan made in infancy may change when foot deformity, knee instability, child preference, family capacity or technology changes. The child should increasingly participate in decisions as they mature.

Decision-Making in Practice
Congenital lower-limb deficiency management is a lifetime mobility plan. The clinical decision is not reconstruction versus amputation in the abstract; it is which pathway gives the child a plantigrade, braceable or prosthesis-friendly limb with the least morbidity and the best function over growth.
- Assess
- Femoral, fibular, tibial, foot-ray, knee and hip anatomy
- Treatment consequence
- Defines whether reconstruction, prosthetics or amputation is realistic
- Assess
- Serial length, multiplier method, congenital pattern and foot height
- Treatment consequence
- Determines epiphysiodesis, lengthening number and timing
- Assess
- Plantigrade foot, ankle stability, rays, coalition, equinovalgus or ball-and-socket ankle
- Treatment consequence
- A non-reconstructable foot may make prosthetic strategy better than repeated salvage
- Assess
- Quadriceps, cruciates, flexion contracture, instability and tibial deficiency
- Treatment consequence
- A stable knee is central to walking and prosthetic control
- Assess
- Treatment burden, travel, complications, school, sport and expectations
- Treatment consequence
- Shared decision-making is essential because both paths are demanding
- Driver
- Predicted discrepancy, foot rays, ankle/subtalar deformity, knee stability and family willingness for staged lengthening.
- Practical implication
- Foot reconstructability is often the pathway-defining issue.
- Driver
- Hip stability, femoral head presence, knee level, projected length, pelvic support and prosthetic implications.
- Practical implication
- A short stable femur is different from an absent proximal femur with unstable hip.
- Driver
- Knee extensor mechanism, tibial support and foot orientation.
- Practical implication
- If the knee-foot unit cannot become useful, prosthetic strategy may be safer.
- Driver
- Preparatory joint/foot surgery, deformity correction, regenerate monitoring and rehabilitation.
- Practical implication
- Lengthening is a programme, not a single operation.
Amputation or rotationplasty is not a failure when it gives earlier, safer, more predictable mobility.
Clinical Reasoning Notes
Structured clinical approach
Start with age, side, ambulatory status and the condition pattern. Describe each anatomical level: pelvis and hip, femur, knee, tibia/fibula, ankle, foot rays and skin. State the current and predicted discrepancy, foot reconstructability, joint stability and the family's goals. Then present a neutral pathway comparison.
Common pitfalls
- Planning from the current centimetre discrepancy alone.
- Forgetting foot-height contribution to total LLD.
- Lengthening above an unstable hip, knee or ankle.
- Ignoring foot reconstructability in fibular hemimelia.
- Presenting prosthetic care as a failure.
- Underestimating rehabilitation and family burden.
- Not updating predictions through growth.
- Forgetting the child's own preference in later childhood.
Integrated clinical approach
"I would not decide from the discrepancy alone. I would define the anatomical deficiency, assess hip and knee stability, decide whether the foot can become plantigrade and shoeable, predict LLD at maturity, and discuss reconstruction, prosthetic or hybrid pathways with the family. The goal is reliable painless mobility with an acceptable lifetime treatment burden."
Guidelines, Registries & Global Practice
Congenital lower-limb deficiency has no single society "guideline" in the way arthroplasty does; practice is shaped by classification-based specialist consensus, prosthetic-rehabilitation standards and resource availability. The picture is genuinely global, and the right pathway shifts with what reconstruction, prosthetics and follow-up a setting can sustain.
Global epidemiology
- Approximate figure
- Most common congenital long-bone deficiency.
- Source context
- Consistently reported across registries and case series.
- Approximate figure
- About 1 per 1,000,000 live births; frequently syndromic or familial.
- Source context
- Fernandez-Palazzi series and rarity reviews.
- Approximate figure
- Femoral anomalies in roughly 59 to 76 percent of fibular deficiency limbs.
- Source context
- Achterman-Kalamchi classification cohort.
- Approximate figure
- Often unilateral; tibial hemimelia may be bilateral and shows familial clustering.
- Source context
- Heterogeneous across small series.
Side-by-side practice frameworks
- Emphasis
- Classification-led decision-making, shared decision-making and outcome measurement (e.g. PODCI).
- Practical message
- Match pathway to Paley/Jones type and document patient-reported function.
- Emphasis
- Centralisation of complex limb deficiency to specialist paediatric limb-reconstruction units with MDT and prosthetic services.
- Practical message
- Refer early; complex reconstruction belongs in high-volume centres.
- Emphasis
- Stability before length: protect joints, achieve a plantigrade foot, then lengthen with monitored regenerate.
- Practical message
- Lengthening is a staged programme, not a single procedure.
- Emphasis
- Multidisciplinary, family-centred counselling comparing reconstruction and prosthetic pathways neutrally.
- Practical message
- Present complete pathways, not isolated operations.
- Emphasis
- Durable end-bearing residual limb and access to growth-adapted prosthetic care.
- Practical message
- Surgical choice must consider lifelong prosthetic and rehabilitation capacity.
Registry and surveillance notes
Unlike arthroplasty, there is no implant registry for these conditions; population data come from congenital-anomaly surveillance networks such as EUROCAT (Europe), the US National Birth Defects Prevention Network and the International Clearinghouse for Birth Defects Surveillance and Research. These define prevalence and associated anomalies but not long-term functional outcomes, which still rely on specialist cohorts.
High- versus limited-resource practice variation
- Typical reality
- Access to staged lengthening, frames, MDT, child psychology and growth-adapted prosthetics.
- Pathway consequence
- Reconstruction and prosthetic pathways can be compared on near-equal footing.
- Typical reality
- Limited frame surgery, fewer revisions feasible, variable prosthetic supply and follow-up.
- Pathway consequence
- A single durable amputation with reliable prosthetic fitting may give better lifetime mobility than incomplete reconstruction.
- Typical reality
- Established deformity, fixed contracture or large discrepancy at first contact.
- Pathway consequence
- Some reconstruction windows are closed; pragmatic prosthetic or salvage planning dominates.
Controversies and Areas of Uncertainty
Several decisions in congenital lower-limb deficiency remain genuinely debated, and a strong exam candidate acknowledges the uncertainty rather than asserting a single right answer.
- The two positions
- Staged reconstruction preserving a plantigrade foot, versus early Syme/Boyd amputation for predictable prosthetic mobility.
- Current balance of evidence
- Meta-analysis favours amputation for satisfaction and fewer complications, but specialist series report excellent reconstruction outcomes in selected feet; choice is individualised.
- The two positions
- Reconstruction (e.g. fibular transfer, knee reconstruction) versus knee disarticulation or below-knee amputation.
- Current balance of evidence
- Amputation remains the stated gold standard; reconstruction is type-dependent and unproven in controlled comparison.
- The two positions
- Rotationplasty converts the ankle into a knee for an active end-bearing limb, versus extension prosthesis or other reconstruction.
- Current balance of evidence
- Rotationplasty gives excellent function but raises cosmetic and psychosocial acceptance issues that vary by family and culture.
- The two positions
- Aggressive early equalisation versus staged lengthening closer to maturity with epiphysiodesis.
- Current balance of evidence
- Larger predicted discrepancies and unstable joints push toward fewer lengthenings or a prosthetic strategy; complication risk rises with magnitude per stage.
- The two positions
- Maximising gain per frame, versus limiting each lengthening to protect joints, nerves and pain scores.
- Current balance of evidence
- Cohort data link larger lengthening (over 6 cm or 25 percent of segment) to worse pain and function, supporting conservative staged gains.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A newborn has unilateral fibular hemimelia. How do you counsel the family?”
“What matters when assessing congenital femoral deficiency?”
“The family wants limb lengthening because they want to avoid amputation. How do you respond?”
“A two-year-old has unilateral tibial hemimelia with a fixed knee flexion contracture and a deficient extensor mechanism. The parents are strongly against amputation. How do you proceed?”
Assess
- Anatomy
- Hip stability
- Knee stability
- Foot rays
- Predicted LLD
Conditions
- CFD
- Fibular hemimelia
- Tibial hemimelia
- Mixed deficiency
Pathways
- Shoe lift or orthosis
- Foot reconstruction
- Lengthening
- Epiphysiodesis
- Prosthesis or amputation
Pitfalls
- Centimetres only
- Unstable joints
- Poor foot
- No prosthetic comparison
- No growth plan
Evidence Signals
Achterman-Kalamchi: the landmark fibular deficiency classification
- Reviewed 97 limbs in 81 patients with congenital fibular deficiency and divided it into Type I (partial hypoplasia) and Type II (complete absence).
- Associated femoral anomalies were present in 76 percent of Type I and 59 percent of Type II limbs, and limb shortening was roughly proportional throughout growth (about 13 percent Type I, 19 percent Type II).
- Type I deficiency was treated by length equalisation, whereas Type II commonly required foot amputation and prosthetic fitting for satisfactory function.
Paley reconstruction classification for fibular hemimelia
- Proposes a classification based on ankle joint morphology rather than the degree of fibular deficiency, because residual or recurrent foot deformity is the main cause of reconstruction failure.
- The SHORDT procedure stabilises a dynamic valgus ankle, while the SUPERankle procedure corrects a fixed equinovalgus foot using bony supramalleolar and subtalar realignment with anlage resection.
- Serial lengthening combined with a plantigrade, painless, functional foot is reported as comparable to or better than Syme amputation with a prosthesis.
SUPERankle plus lengthening: a reconstruction outcomes series
- 29 limbs treated using the Paley classification: 27 reconstructed and 2 treated with primary Syme amputation.
- Excellent or good ASAMI results were achieved in 21 of 27 reconstructed patients (55 percent excellent, 22 percent good).
- Mean limb length discrepancy improved from 3.55 cm at presentation to 1.01 cm after treatment, and operating before age 5 reduced recurrent foot deformity.
Amputation versus reconstruction for fibular hemimelia: meta-analysis
- Pooled 7 retrospective cohorts and 169 fibular hemimelia cases comparing amputation with limb reconstruction.
- Amputation showed higher patient satisfaction (odds ratio 6.8, 95 percent CI 2.4 to 19.2) and far fewer complications (reconstruction odds ratio 28 for complications).
- Reconstruction averaged 4.2 procedures per patient versus 1.5 for amputation, with 1.2 versus 0.2 complications per limb.
Evidence Base
Lengthening is effective for mild and moderate congenital femoral deficiency
- 30 patients with Paley Type 1a, 1b or 2a congenital femoral deficiency and stable hip and knee joints were lengthened with a monolateral external fixator.
- Mean lengthening was 6 cm (correcting about 112 percent of the discrepancy) without significant loss of hip or knee range of motion.
- Complications occurred in 30 of 60 planned procedures (50 percent), and lengthening greater than 6 cm or over 25 percent of femoral length gave worse pain and comfort scores.
Paley reconstruction classification for tibial hemimelia
- Tibial hemimelia is a rare deficiency with a wide spectrum of anomalies, duplications and deficiencies, where amputation with prosthetic fitting has long been the gold standard.
- A new classification is proposed to guide prognosis and reconstructive technique selection based on improved understanding of pathoanatomy.
- Reconstructive options (including fibular transfer and patelloplasty techniques) are matched to specific anatomical types.
Tibial hemimelia: reconstruction versus amputation systematic review
- Pooled 11 studies and 131 patients; Jones Type I was the most common pattern (40.9 percent).
- Reconstruction complications included external fixator tract infection, knee flexion contracture and reduced knee and ankle motion.
- No evidence proved superiority of reconstruction, and amputation remained the stated gold standard.
Tibial deficiency: rarity, the Jones classification and early amputation
- Tibial hemimelia has an incidence of approximately 1 per 1 million live births and is usually associated with other anomalies.
- 22 limbs in 18 patients were classified by Jones, Barnes and Lloyd-Roberts (types Ia, Ib, II, III, IV), and treatment was always surgical.
- Earlier amputation was associated with easier, faster rehabilitation and prosthetic adaptation, accepted by the child as a congenital amputation.