Benign metaphyseal lesion, classic radiograph and mechanical fracture risk
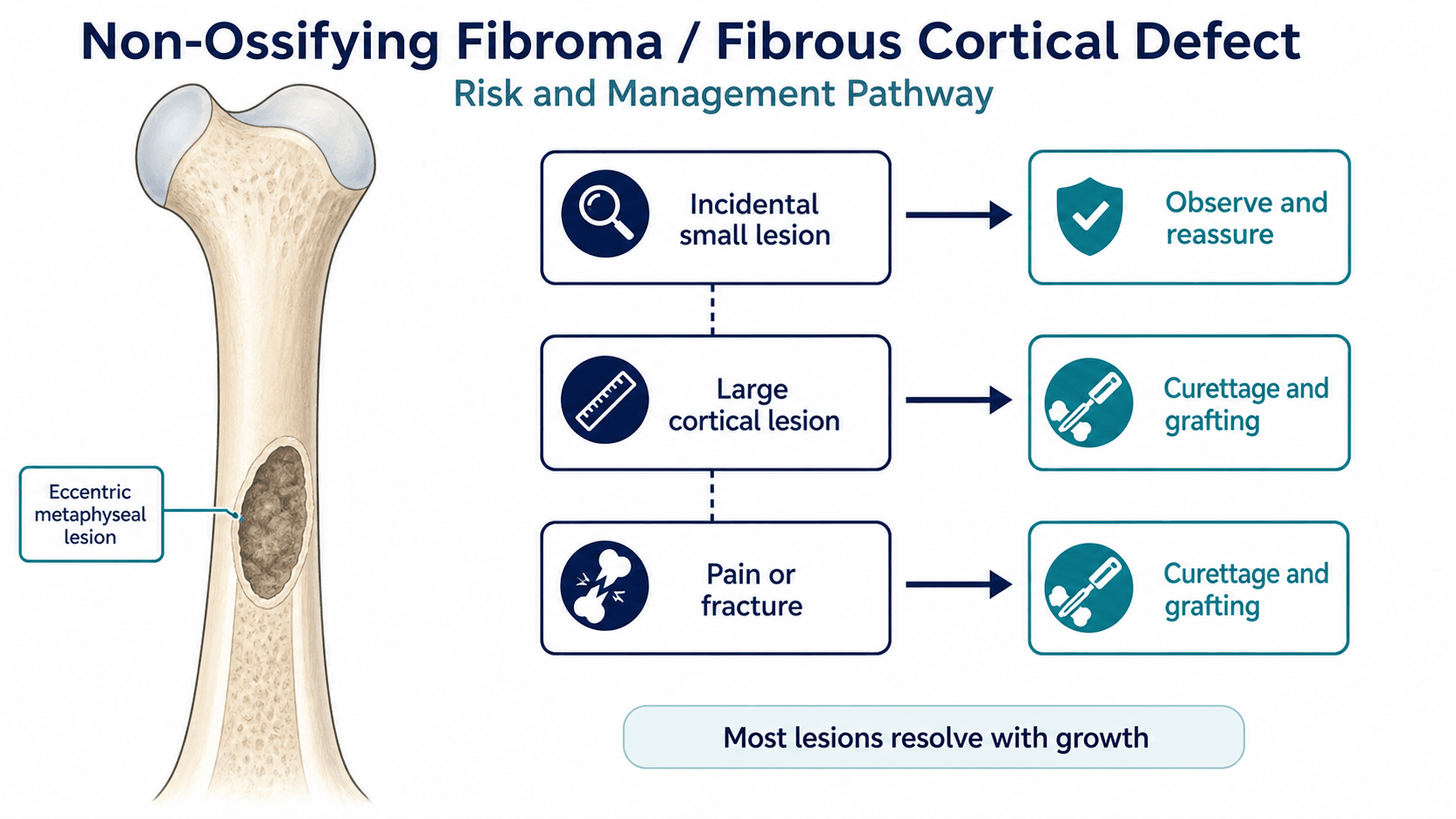
- Fibrous cortical defect and non-ossifying fibroma are a size spectrum of benign eccentric cortically based metaphyseal lesions.
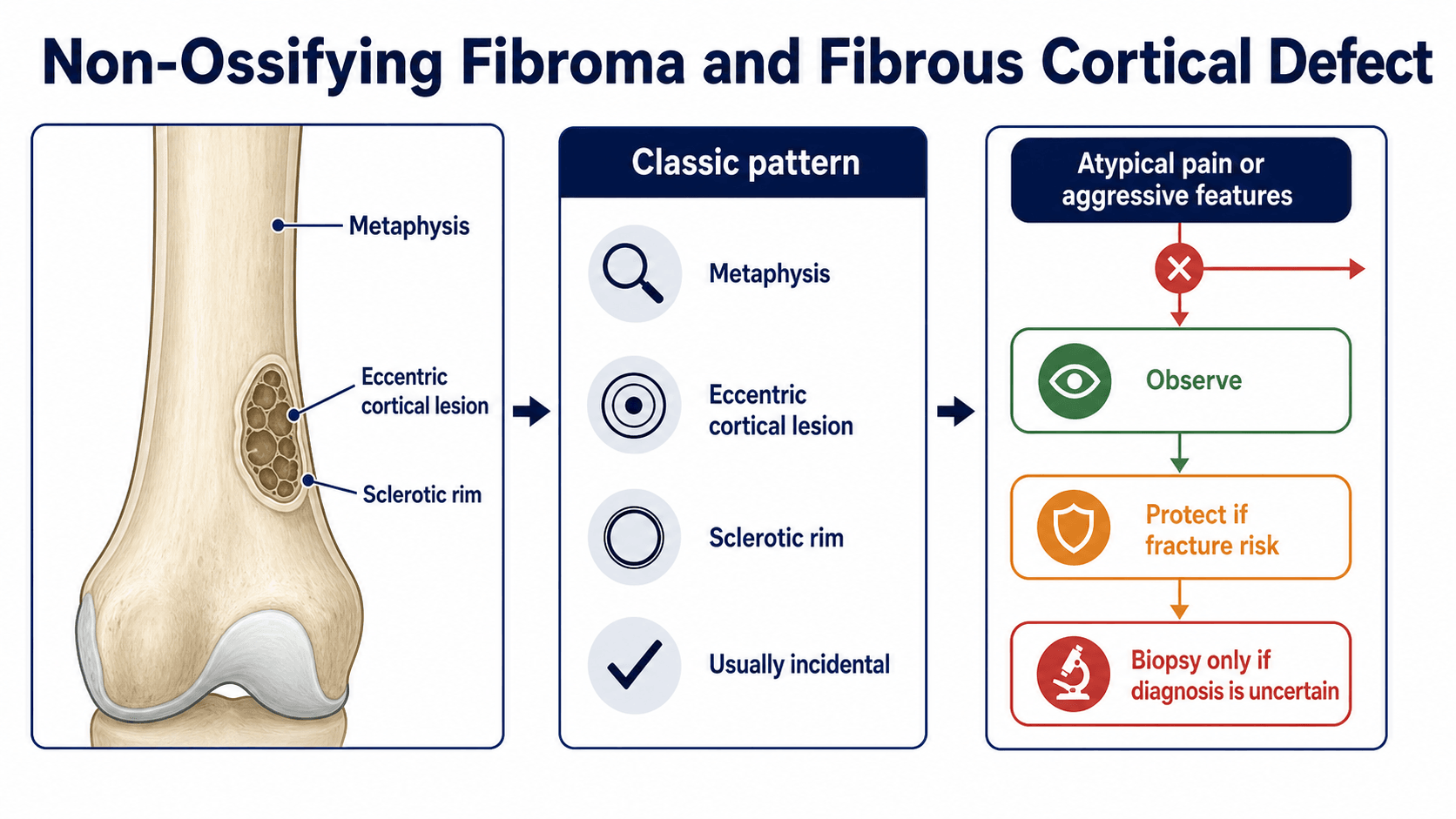
- Classic radiograph shows an eccentric metaphyseal lytic lesion with a sclerotic rim and narrow zone of transition.
- Most lesions are incidental, asymptomatic and involute with skeletal maturity.
- Large lesions with cortical thinning in weight-bearing bones require fracture-risk assessment.
- Pain before trauma, aggressive periosteal reaction, soft-tissue mass or systemic symptoms are not classic and should prompt reconsideration.
- “The commonest presentation is an incidental X-ray finding after minor trauma.
- “A dramatic-looking lesion can still be benign if the pattern is classic.
- “Do not biopsy a classic asymptomatic NOF just because the word lesion sounds alarming.
- “Benign does not always mean mechanically irrelevant; size and cortical thinning matter.
A classic asymptomatic non-ossifying fibroma does not need biopsy. A painful, aggressive or mechanically dangerous lesion does need reassessment.
Images and Diagrams
- Answer
- Eccentric metaphyseal cortically based lytic lesion with sclerotic rim.
- Clinical use
- Supports diagnosis without biopsy.
- Answer
- Usually none unless fracture or incidental trauma pain.
- Clinical use
- Pain should match the clinical story.
- Answer
- Large lesion with cortical thinning in weight-bearing bone.
- Clinical use
- Assess fracture risk and activity advice.
- Answer
- Night pain, soft-tissue mass, aggressive periosteal reaction, systemic symptoms.
- Clinical use
- Escalate diagnosis.
NOFRecognition
Hook:NOF keeps the classic pattern easy to recall.
RIMRadiographic Pattern
Hook:RIM separates classic benign imaging from aggressive lesions.
FRACTUREMechanical Risk
Hook:FRACTURE keeps benign biology and mechanical strength separate.
Overview/Epidemiology
Non-ossifying fibroma and fibrous cortical defect are among the most common benign bone lesions seen in children. They are usually developmental fibrous lesions rather than aggressive tumours. The distal femur, proximal tibia and distal tibia are common sites, and many are discovered incidentally after X-rays for minor trauma.
The clinical value is pattern recognition. When the radiographic appearance is classic and the child is asymptomatic, confident explanation prevents unnecessary biopsy, MRI and anxiety. The separate task is mechanical: a large lesion can thin the cortex and predispose to pathological fracture, especially in a weight-bearing bone.
Pathophysiology
The lesion consists of fibrous tissue within cortex and metaphyseal cancellous bone. It is eccentric and cortically based, usually near the metaphysis. As the child grows, the lesion appears to move away from the physis and often becomes more sclerotic before involuting.
The sclerotic rim and narrow zone of transition reflect slow, non-aggressive behaviour. The lesion becomes clinically important when it occupies enough bone diameter to reduce bending strength. Pain without fracture is not the typical story and should prompt careful clinical correlation.
Histopathology
Although NOF/FCD is fundamentally a radiographic diagnosis, its microscopic appearance is examinable and explains the imaging. Macroscopically the lesion is well-circumscribed, firm and characteristically yellow-brown — the colour gives the older synonym fibroxanthoma.
Histologically it is a benign fibrous (fibrohistiocytic) lesion showing:
- Bland spindle fibroblasts and myofibroblasts arranged in a whorled or storiform ("cartwheel") pattern within a collagenous stroma.
- Scattered benign multinucleated osteoclast-type giant cells.
- Foamy lipid-laden macrophages (xanthoma cells) and haemosiderin-laden macrophages — the latter give the brown colour.
- No cytological atypia and no malignant mitoses, and crucially no osteoid or bone produced by the lesion itself — a key distinction from osteosarcoma, and from fibrous dysplasia, which contains metaplastic woven bone.
The histology is identical across the size spectrum, so a fibrous cortical defect and a non-ossifying fibroma cannot be separated microscopically — they differ only in size and extent. The picture is also indistinguishable from a benign fibrous histiocytoma of bone, which is essentially a NOF arising in an atypical (older, non-metaphyseal, sometimes painful) setting. More recently, activating mutations in the MAP-kinase pathway (for example in KRAS and FGFR1) have been reported in NOF, placing it on a spectrum with other MAPK-driven benign bone lesions.
The histology is benign but non-specific — storiform spindle cells, giant cells and foam cells are shared with several other lesions. This is exactly why the radiograph outperforms biopsy here: the imaging pattern (eccentric, cortically based, sclerotic rim, narrow transition zone) is effectively diagnostic, whereas histology only confirms "a benign fibrous lesion." Biopsy is therefore reserved for radiographically atypical cases.
Classification
- Fibrous cortical defect: small, cortically based lesion.
- Non-ossifying fibroma: larger lesion extending into metaphyseal cancellous bone.
- Healing lesion: increasing sclerosis and reduced lucency.
- Fractured lesion: pathological fracture through weakened cortex.
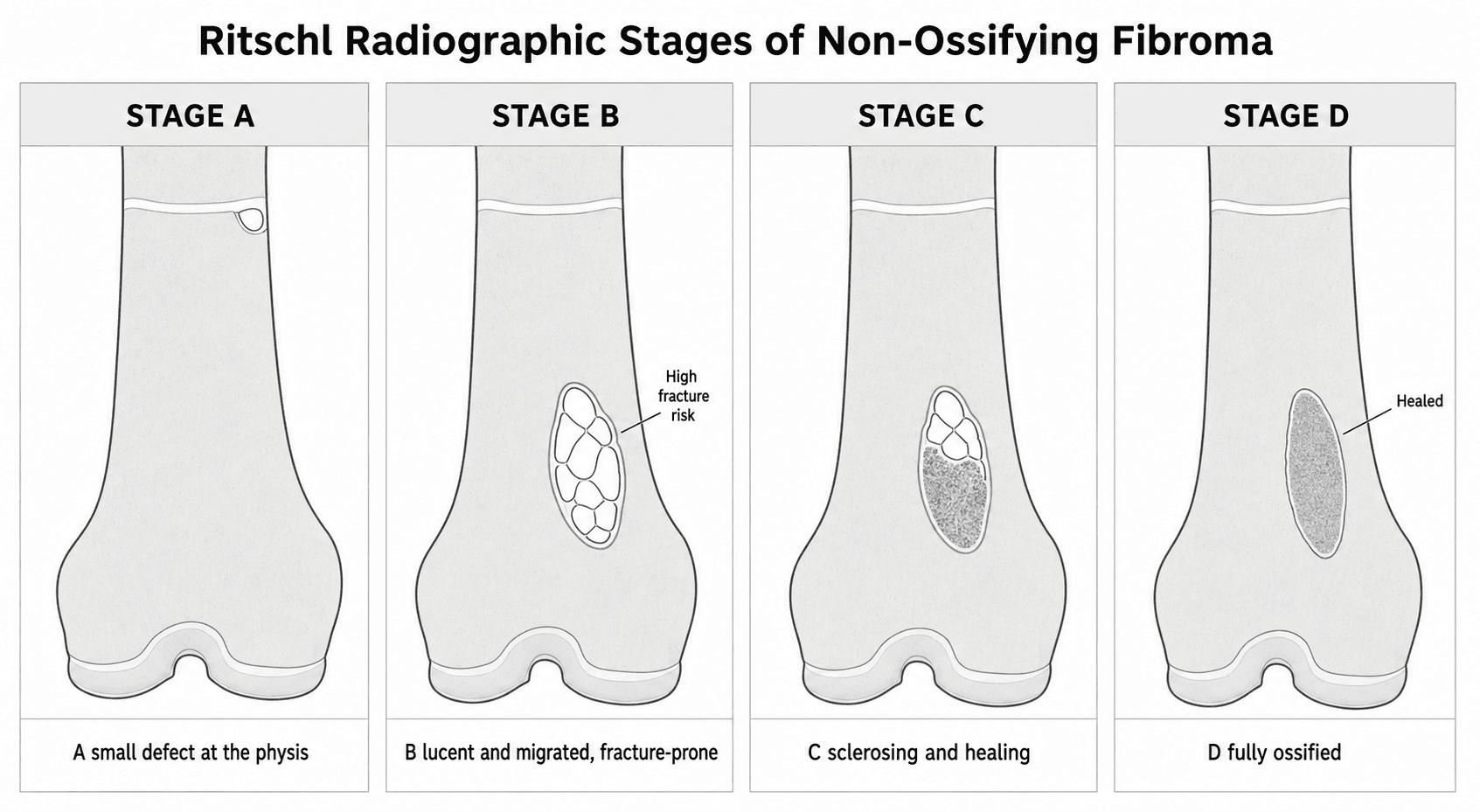
Ritschl Radiographic Staging
Beyond the practical spectrum above, the lesion evolves through a predictable radiographic life-cycle described by the Ritschl stages. This is the common language the natural-history and fracture-risk literature uses (the surveillance and pain studies in the Evidence Base are all framed around it), so an examiner may ask you to describe it.
- Radiographic appearance
- Small cortical lucency lying close to (juxta-) the physis — the fibrous cortical defect stage.
- Significance
- Early lesion; incidental, low risk.
- Radiographic appearance
- Larger, polycyclic / multiloculated lucency with a sclerotic margin that has 'moved' away from the physis into the metaphysis or diaphysis as the bone grows.
- Significance
- The predominantly LUCENT stage — this is when pathological fracture occurs (all fractures in the natural-history series were stage B).
- Radiographic appearance
- Progressive sclerosis begins (often from the diaphyseal side) and the lucency fills in.
- Significance
- Healing / involuting; fracture risk falling.
- Radiographic appearance
- Complete, homogeneous sclerosis — the lesion is ossified and healed.
- Significance
- Resolved; can be discharged.
The staging earns its keep in two ways. It explains why a NOF appears to "migrate" down the shaft with growth — the lesion stays put while the physis grows away from it. And it focuses fracture-risk counselling and six-to-twelve-month surveillance on the lucent stage B lesion, with discharge once a lesion sclerose into stage C–D.
Clinical Presentation
History
Ask why the X-ray was taken. In many children, the lesion is incidental and the injury pain comes from a sprain or contusion rather than the lesion. Ask whether pain preceded trauma, whether pain is at rest or night, and whether the child has fever, weight loss, systemic symptoms or previous fracture through the same area.
Examination
Most incidental lesions have a normal examination. If there is pain, localise it carefully and correlate it with the X-ray. Look for swelling, deformity, tenderness, loss of function and inability to weight bear. A mass, skin change or pain out of proportion is not a typical NOF finding. If fracture is present, document alignment, adjacent joint motion and neurovascular status.
If the child has severe unexplained pain, do not let the label NOF stop you from checking for fracture or an alternative diagnosis.
Investigations
Plain radiographs in two planes are usually enough when the lesion is classic. The diagnosis should be made from the pattern: eccentric, metaphyseal, cortically based, lytic, sclerotic rim and narrow transition zone. Measure lesion size and cortical thinning when fracture risk is relevant.

MRI is not routine for classic incidental NOF. It is useful when symptoms, location or imaging features are atypical, or when the diagnosis is uncertain. Biopsy is avoided when the radiographic appearance is classic because it adds morbidity without improving care.
- Investigation
- Plain radiographs in two planes
- Decision it informs
- Supports diagnosis without biopsy.
- Investigation
- Measure lesion size and cortex
- Decision it informs
- Guides activity advice and follow-up.
- Investigation
- MRI and specialist tumour review
- Decision it informs
- Reassesses diagnosis before surgery.
- Investigation
- Full fracture radiographs
- Decision it informs
- Plans immobilisation, fixation or lesion treatment.
- Why it matters
- Large transverse involvement reduces bending strength.
- How to use it
- Historically used as a warning threshold, but not an automatic operation.
- Why it matters
- Long lesions have been associated with pathological fracture risk in classic series.
- How to use it
- Use with site, cortex and symptoms rather than as a stand-alone rule.
- Why it matters
- The remaining cortex is the structural support.
- How to use it
- Consider activity advice, follow-up or prophylactic treatment in high-load bones.
- Why it matters
- Distal tibial lesions have been studied as a higher-risk subgroup.
- How to use it
- Be more cautious with large lucent distal tibial lesions.
- Why it matters
- Classic incidental NOF is usually painless.
- How to use it
- Exclude fracture, stress reaction or a different diagnosis before attributing pain to NOF.
- Why it matters
- Some studies use CT features such as coronal and sagittal width, cortical breach and lack of neocortex.
- How to use it
- Reserve CT for cases where the structural-risk answer will change management.
Differential Diagnosis
The eccentric metaphyseal lucency of a NOF overlaps with several lesions. The discriminators are location within the bone (cortical/eccentric versus central), zone of transition, periosteal reaction and the clinical story.
- Distinguishing features
- Eccentric, cortically based, metaphyseal, sclerotic rim, narrow zone of transition, often multilobulated.
- Clue that it is NOT a NOF
- Reference pattern - asymptomatic, involutes with maturity.
- Distinguishing features
- Central, symmetric, metaphyseal lucency; fallen-fragment sign after fracture; commonly proximal humerus or femur.
- Clue that it is NOT a NOF
- Centrally located and symmetric rather than eccentric and cortically based.
- Distinguishing features
- Expansile, eccentric, may show fluid-fluid levels on MRI; can grow rapidly and thin the cortex.
- Clue that it is NOT a NOF
- Rapid expansion, fluid-fluid levels and ballooned cortex.
- Distinguishing features
- Central, ground-glass matrix, may bow long bones (shepherd's crook at hip); polyostotic in McCune-Albright.
- Clue that it is NOT a NOF
- Ground-glass matrix and central location rather than a lucent rimmed defect.
- Distinguishing features
- Anterior tibial diaphyseal cortex of young children, anterior bowing, multiloculated lucency.
- Clue that it is NOT a NOF
- Diaphyseal anterior tibia with bowing; mimics adamantinoma, may need biopsy.
- Distinguishing features
- Lucency with thick sclerotic rim, penumbra sign, may cross physis; pain and warmth.
- Clue that it is NOT a NOF
- Pain, systemic signs, penumbra sign and possible physeal involvement.
- Distinguishing features
- Variable - can be permeative or well-defined; bevelled edges in skull; may be painful.
- Clue that it is NOT a NOF
- More aggressive or permeative pattern and clinical symptoms.
- Distinguishing features
- Small nidus with reactive sclerosis; classic night pain relieved by NSAIDs.
- Clue that it is NOT a NOF
- Night pain relieved by NSAIDs and a sclerotic nidus, not a benign lucency.
- Distinguishing features
- Permeative or moth-eaten lysis, wide zone of transition, periosteal reaction, soft-tissue mass.
- Clue that it is NOT a NOF
- Cortical destruction, soft-tissue mass and aggressive periosteal reaction - never a NOF.
Management
Explain that this is a benign developmental lesion. If the imaging is classic and the child is asymptomatic from the lesion, biopsy is not needed. Follow-up may not be required for small low-risk lesions, but larger lesions can be reviewed until sclerosis or stability is seen.
Complications
Clinical complications
- Pathological fracture in a large lesion.
- Recurrent fracture if a large lesion persists.
- Pain from an unrelated diagnosis attributed to NOF.
- Missed aggressive lesion when red flags are ignored.
Management complications
- Unnecessary biopsy, MRI or surgery.
- Excessive activity restriction and family anxiety.
- Curettage, graft or fixation complications.
- Delayed return to sport after fracture.
A classic NOF is benign, but size and cortex decide whether it is also mechanically safe.
Decision-Making in Practice
Non-ossifying fibroma and fibrous cortical defect management is usually about recognising a benign lesion and deciding whether fracture risk changes treatment. Most are incidental and need reassurance, but large, expansile, weight-bearing lesions or lesions associated with pain or fracture need a more formal plan.
- Assess
- Eccentric metaphyseal lucency, sclerotic rim, cortically based and age-appropriate
- Management consequence
- Typical asymptomatic lesions can usually be observed
- Assess
- Pain, lesion size, cortical thinning, distal tibia location, expansion and activity level
- Management consequence
- High-risk lesions need activity advice, surveillance or prophylactic treatment
- Assess
- Aggressive features, soft-tissue mass, periosteal reaction, atypical age or night pain
- Management consequence
- Escalate imaging and tumour referral rather than curetting blindly
- Assess
- Displacement, stability, lesion size and location
- Management consequence
- Treat fracture stability first; curettage and grafting are selective
- Assess
- Sclerosis, ossification, symptoms and growth
- Management consequence
- Discharge when benign behaviour is clear and fracture risk is low
Do not biopsy a classic asymptomatic NOF simply because it is large on a report. Conversely, do not dismiss pain, rapid growth, aggressive radiographic features or a lesion in an atypical patient. The important clinical distinction is typical benign behaviour versus diagnostic uncertainty.
Surgery is considered for symptomatic lesions, impending fracture risk, recurrent fracture, large structural lesions in high-load regions or when fixation is required for a pathological fracture. Curettage, grafting and internal fixation decisions should be based on mechanical risk and diagnosis confidence.
Clinical Reasoning Notes
How to describe the X-ray
Use the exact language: eccentric metaphyseal cortically based lytic lesion with a sclerotic rim and narrow zone of transition. Then add site, size, cortical thinning and whether there is fracture.
Common pitfalls
- Calling it cancer.
- Biopsying a classic asymptomatic lesion.
- Ignoring aggressive features.
- Ignoring fracture risk in a large lesion.
- Attributing unrelated pain to the lesion.
- Forgetting to explain the benign natural history to the family.
Counselling language
Families often hear "bone lesion" and think cancer. A clear explanation helps: this is a common benign childhood lesion that often heals with growth. If it is large, the concern is bone strength rather than cancer behaviour.
Guidelines, Registries & Global Practice
Global epidemiology
- NOF/FCD are the most common benign skeletal lesions of childhood and adolescence; classic radiographic estimates suggest fibrous cortical defects are present in a substantial minority of children (figures of around 30 percent of children in some radiographic series), with most regressing spontaneously by skeletal maturity.
- Peak presentation is in the first two decades, with a slight male predominance; the distal femur, proximal tibia and distal tibia dominate, reflecting the rapidly growing metaphyses of the lower limb.
- Multifocal disease raises the possibility of Jaffe-Campanacci syndrome or neurofibromatosis type 1, which carry materially higher fracture risk.
Side-by-side guidance
- Position on diagnosis
- Classic lesion diagnosed on radiographs; biopsy usually unnecessary
- Position on intervention
- Observation for most; treatment for large, painful or fractured lesions
- Position on diagnosis
- Pattern recognition on plain films; MRI only for atypical features
- Position on intervention
- Conservative care default; surgery for impending or actual pathological fracture
- Position on diagnosis
- Recognise NOF as a benign lesion underlying many paediatric pathological fractures
- Position on intervention
- Treat the fracture on its mechanical merits; lesion-directed surgery is selective
- Position on diagnosis
- Refer atypical or aggressive-appearing lesions to a sarcoma unit before any biopsy
- Position on intervention
- Biopsy and definitive surgery planned by the tumour service, never ad hoc
The practical message is consistent worldwide: a classic asymptomatic lesion is diagnosed radiographically and observed; anything atypical is referred before biopsy. Differences are of emphasis (thresholds for follow-up imaging and prophylactic surgery), not of principle.
Registry and database notes
There is no dedicated implant registry for NOF because it is rarely implant-treated. Relevant data instead come from orthopaedic-oncology referral databases and paediatric fracture series, which consistently show that pathological fractures cluster in large lucent lower-limb lesions and that misreferral of benign lesions (and of stress fractures complicating them) as suspected sarcoma is common.
High- versus limited-resource practice
- Well-resourced settings: ready access to MRI and specialist sarcoma services allows confident non-operative management with selective imaging; the main risk is over-investigation and over-treatment of a benign lesion.
- Limited-resource settings: plain radiography remains the cornerstone, which is appropriate because classic NOF is a radiographic diagnosis; the priorities are recognising red flags that warrant referral and avoiding both unnecessary biopsy and missed aggressive lesions when advanced imaging is scarce.
Controversies and Areas of Uncertainty
Most of the debate around NOF/FCD is about how aggressively to risk-stratify and intervene, not about the benign diagnosis itself.
- Fracture-risk thresholds are imperfect. The classic Arata "greater than 50 percent transverse diameter plus over 33 mm length" rule comes from a retrospective fracture cohort with no asymptomatic comparison group, so it identifies lesions that have already fractured rather than reliably predicting who will. Many large lesions never fracture, so thresholds inform conversation rather than mandate surgery.
- Whether to follow up at all. Small classic asymptomatic lesions may be discharged without imaging, while larger lesions are often reviewed until sclerosis or ossification appears. There is no high-level evidence defining the optimal interval; six to twelve month intervals through the lucent (Ritschl B) stage are pragmatic rather than proven.
- Prophylactic curettage versus watchful waiting. Curettage and grafting reliably promotes healing but carries its own morbidity (growth-plate injury, recurrence, donor-site issues). For a lesion that may involute spontaneously, the threshold for prophylactic surgery is genuinely contested and should be individualised.
- Pain attribution. Recent cross-sectional data show spontaneous pain is reported in roughly half of children with FCD/NOF, challenging the dogma that these lesions are always painless and reminding clinicians to exclude stress reaction, stress fracture and alternative pathology before attributing pain to the lesion.
- Role of CT/MRI. Advanced imaging is reserved for atypical features or structural questions plain films cannot answer; routine cross-sectional imaging of a classic lesion adds radiation, cost and anxiety without changing management.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A child has an incidental distal femur NOF after a knee injury. How do you manage it?”
“A child fractures through a large tibial NOF. What is your approach?”
“A 13-year-old has a metaphyseal lucency around the knee. The referring report mentions a possible aggressive lesion. How do you decide whether this is a benign NOF or something sinister, and what do you do?”
Classic X-ray
- Eccentric
- Metaphyseal
- Cortical based
- Lytic
- Sclerotic rim
Clinical
- Usually incidental
- Pain if fracture
- No systemic symptoms
- Normal clinical assessment
Treat
- Reassure
- Observe
- Assess fracture risk
- Curettage selected
- Fix fracture if needed
Red Flags
- Night pain
- Soft-tissue mass
- Aggressive periosteal reaction
- Systemic symptoms
- Atypical site
Evidence Base
Landmark fracture-risk thresholds (Mayo Clinic series)
- 23 pathological fractures through histologically confirmed NOF over 49 years; mean age 12 years.
- All but one fracture occurred in the lower limb, most commonly the distal tibia (10 cases).
- In every patient the fibroma occupied greater than 50 percent of the transverse bone diameter on both AP and lateral films.
- In all non-fibular lesions the vertical length exceeded 33 mm.
Natural history and Ritschl staging
- 87 patients with 103 NOFs followed through the Ritschl stages.
- All six pathological fractures occurred in stage B (lucent) lesions, with mean length 44 mm and roughly 75 percent transverse and 87 percent sagittal bone involvement.
- No fractures occurred in stages A, C or D; four of the six fractures were in the tibia.