Age-based differential, septic arthritis safety and hip referred pain
- Assess weight-bearing status and illness severity before narrowing the differential.
- Always examine hip rotation in a child with thigh or knee pain.
- Septic arthritis is time-critical because cartilage damage can occur quickly.
- Kocher and modified Kocher criteria are risk tools for the painful hip, not rules that overrule clinical concern.
- Normal early radiographs do not exclude infection, toddler fracture, early Perthes disease or malignancy.
- Non-accidental injury must be considered when the history and developmental stage do not fit.
- “A child who will not walk is different from a child who limps but runs into the room.
- “Loss of internal rotation is an important hip warning sign.
- “Night pain, systemic symptoms and bone tenderness deserve respect.
- “Observation needs explicit review triggers, not vague reassurance.
Do not label a child as transient synovitis if they are febrile, toxic, refusing to weight bear, waking with night pain, systemically unwell or have restricted hip motion out of proportion to the story.
Images and Diagrams

- Answer
- Sick versus well and painful versus painless
- Clinical use
- Decides urgent sepsis pathway versus structured outpatient workup
- Answer
- Hip, because hip disease can present as knee pain
- Clinical use
- Do not miss SUFE, septic hip or Perthes disease
- Answer
- MRI when infection, tumour or occult fracture remains possible
- Clinical use
- Avoids false reassurance from normal early X-rays
- Answer
- Only if red flags absent and review triggers are clear
- Clinical use
- Observation is active management
LIMPFirst Pass Assessment
Hook:LIMP keeps the first minute safe.
HIPHip Safety
Hook:HIP prevents missed referred pain.
SEPTICInfection Screen
Hook:SEPTIC keeps infection at the front of the assessment.
Overview/Epidemiology
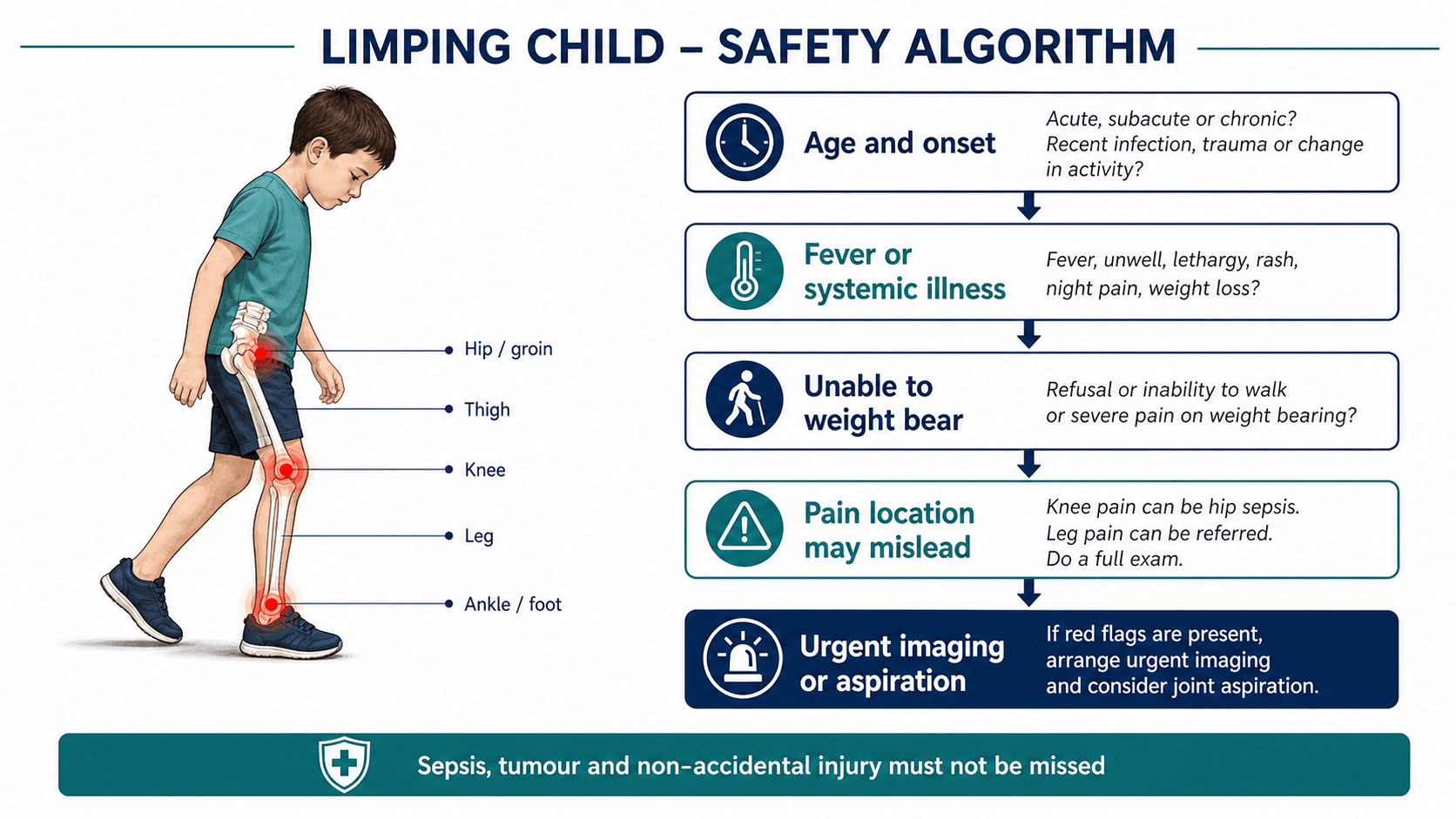
A limp is a presentation, not a diagnosis. It may come from pain, weakness, deformity, limb-length difference, neuromuscular control, inflammatory disease, infection, tumour, trauma or compensation. The safe clinician does not begin by reciting a long differential list. The safe clinician first asks: is this child sick, can they weight bear, is the limp painful, and what dangerous diagnosis must not be missed today?
Age is the strongest first organiser. Toddlers commonly present with occult trauma, infection, developmental hip issues, neuromuscular patterns or safeguarding concerns. School-age children raise the probability of transient synovitis, Perthes disease, infection, inflammatory disease and malignancy. Adolescents require a specific hip screen for slipped upper femoral epiphysis, even when the child points to the knee.
The hip deserves special attention because children localise pain poorly. Hip pathology may be felt in the thigh or knee. A teenager with knee pain and a normal knee examination may have SUFE. A younger child with a subtle limp and reduced hip abduction or internal rotation may have Perthes disease. A febrile non-weight-bearing child may have septic arthritis or osteomyelitis even if early radiographs are normal.
Observation is not a passive decision. Safe observation requires a well child, reassuring examination, improving symptoms, no red flags, a clear working diagnosis and explicit return triggers.
Pathophysiology
The gait pattern gives the first physiological clue. An antalgic gait shortens stance phase on the painful limb. Trendelenburg gait reflects hip abductor weakness, hip pain or altered femoral head mechanics. A short-leg gait suggests limb-length difference or pelvic obliquity. Circumduction, toe walking, spasticity, ataxia or foot drop move the differential toward neuromuscular disease.
The mechanism behind the limp differs by pathology.
- Why the child limps
- Raised intra-articular pressure plus cartilage injury from inflammation and bacterial toxins.
- Clinical clue
- Fever, refusal to weight bear and severe pain with passive movement.
- Why the child limps
- Sterile painful hip effusion, usually self-limiting and improving.
- Clinical clue
- Well child, often post-viral, with less severe systemic features.
- Why the child limps
- Metaphyseal infection may spread to soft tissue, abscess or adjacent joint.
- Clinical clue
- Focal bony tenderness, fever or pain out of proportion; early X-rays may be normal.
- Why the child limps
- Femoral head osteonecrosis followed by fragmentation and remodelling.
- Clinical clue
- School-age child with limp, hip stiffness and reduced abduction/internal rotation.
- Why the child limps
- Failure through the proximal femoral physis; the epiphysis stays in the acetabulum while the metaphysis displaces.
- Clinical clue
- Adolescent with groin, thigh or knee pain and loss of internal rotation.
- Why the child limps
- Subtle spiral tibial fracture produces pain with weight bearing.
- Clinical clue
- Young child with tibial tenderness and normal or subtle initial radiographs.
- Why the child limps
- Marrow pain, systemic illness or cortical involvement can precede obvious radiographic change.
- Clinical clue
- Night pain, pallor, bruising, weight loss or persistent bone pain.
- Why the child limps
- Fracture or soft-tissue injury with a history that does not fit age or development.
- Clinical clue
- Inconsistent mechanism, delay, multiple injuries or injury in a non-mobile child.
Classification
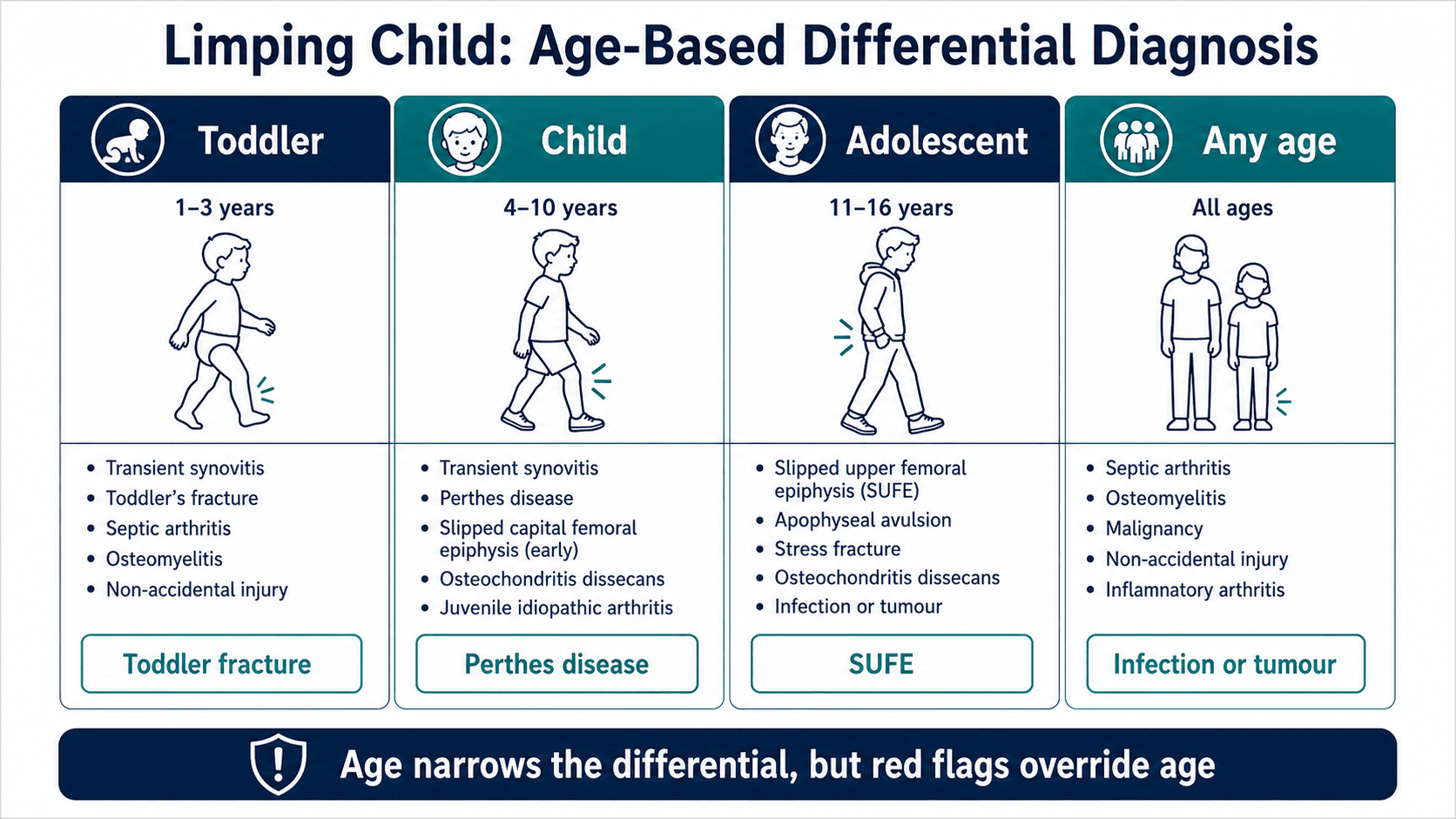
- Toddler: toddler fracture, infection, DDH, non-accidental injury, neuromuscular disorder.
- Child: transient synovitis, Perthes disease, osteomyelitis, septic arthritis, inflammatory disease, malignancy.
- Adolescent: SUFE, sports injury, stress fracture, apophyseal avulsion, infection, inflammatory disease.
Clinical Presentation
History
The history should identify acuity, severity, red flags and the most likely anatomical source.
- Ask specifically
- Sudden trauma, gradual limp, morning stiffness, intermittent limp, night pain, acute refusal to walk, improving or worsening course.
- Why it matters
- Separates trauma, infection, inflammatory disease, tumour and benign recovery patterns.
- Ask specifically
- Walking normally, limping, crawling, standing only with support, or refusing to weight bear after analgesia.
- Why it matters
- Non-weight bearing is a major escalation sign, especially with fever or hip pain.
- Ask specifically
- Fever, malaise, weight loss, pallor, bruising, recurrent infections, recent viral illness, recent antibiotics.
- Why it matters
- Infection, malignancy and inflammatory disease can look orthopaedic at first.
- Ask specifically
- Hip, groin, thigh, knee, tibia, ankle, foot, back or abdomen.
- Why it matters
- Hip disease can present as thigh or knee pain; do not clear the hip from a normal knee X-ray.
- Ask specifically
- Mechanism, timing, witness account and whether the story fits developmental ability.
- Why it matters
- A toddler fracture is common; non-accidental injury is the dangerous miss.
- Ask specifically
- Previous hip disease, sickle cell disease, immunosuppression, inflammatory disease, malignancy, neuromuscular disease or safeguarding concerns.
- Why it matters
- Changes the threshold for imaging, blood tests and senior review.
Examination
Observe before touching the child. A child who runs around the room is different from a child who lies still and refuses to move the hip. Note whether the gait is antalgic, Trendelenburg, short-leg, circumduction, toe-walking, spastic, ataxic or foot-drop pattern.
Examine from spine to foot.
- What to assess
- Temperature, hydration, pallor, bruising, toxicity and systemic illness.
- Diagnosis not to miss
- Sepsis, malignancy or safeguarding concern.
- What to assess
- Back tenderness, abdominal signs, lymphadenopathy and systemic clues.
- Diagnosis not to miss
- Discitis, psoas pathology, inflammatory disease or malignancy.
- What to assess
- Internal rotation, abduction, flexion posture and pain with passive motion.
- Diagnosis not to miss
- Septic hip, Perthes disease and SUFE.
- What to assess
- Effusion, tenderness, range and stability, while still screening the hip.
- Diagnosis not to miss
- Referred hip disease or true knee sepsis/injury.
- What to assess
- Focal tenderness, swelling, callus, foot posture and refusal to load.
- Diagnosis not to miss
- Toddler fracture, stress injury, osteomyelitis or foot pathology.
- What to assess
- Tone, reflexes, power, coordination and foot posture.
- Diagnosis not to miss
- Cerebral palsy, neuromuscular disorder, spinal lesion or painless gait disorder.
- What to assess
- Bruising, swelling, scars, burns and multiple injury sites.
- Diagnosis not to miss
- Non-accidental injury or infection source.
Pain with passive hip motion, especially in a febrile or non-weight-bearing child, is a high-risk finding. Loss of internal rotation in an adolescent suggests SUFE until excluded. Reduced abduction and internal rotation in a school-age child raises concern for Perthes disease.
If a child has knee pain with a normal knee examination, examine and image the hip before discharge.
Investigations
- Investigation
- AP and lateral tibia radiographs, repeat if initially negative
- Decision it informs
- Detect toddler fracture or healing periosteal reaction
- Investigation
- AP pelvis and lateral hip radiographs
- Decision it informs
- Assess Perthes disease, SUFE, DDH sequelae or fracture
- Investigation
- FBC, ESR, CRP, blood cultures and hip ultrasound when indicated
- Decision it informs
- Stratify septic arthritis and osteomyelitis risk
- Investigation
- MRI of the relevant region
- Decision it informs
- Detect osteomyelitis, abscess, tumour, stress fracture or early Perthes disease
Investigations should answer the dangerous question still open after history and examination. Do not order the same panel for every child without deciding what you are trying to exclude.
Radiographs
- AP pelvis and lateral hip views for hip, thigh or knee pain when Perthes disease or SUFE is possible.
- Tibia radiographs for toddler fracture; repeat imaging may show periosteal reaction if early films are normal.
- Local radiographs for focal bony tenderness or trauma.
- Skeletal survey through the appropriate safeguarding pathway when non-accidental injury is suspected.
Blood tests
FBC, ESR, CRP and blood cultures support infection risk assessment. They are particularly useful in febrile, non-weight-bearing or systemically unwell children. Normal early markers do not overrule a concerning examination.
Septic hip risk stratification
Kocher-style criteria help separate septic arthritis from transient synovitis in a child with an acutely irritable hip, but they are not a substitute for clinical judgement, aspiration when indicated, or senior review.
- Threshold commonly used
- Temperature at least 38.5 degrees Celsius.
- How to use it
- Raises probability of septic arthritis, especially with non-weight bearing.
- Threshold commonly used
- Refuses to walk or cannot weight bear after analgesia.
- How to use it
- A major escalation sign; do not label as benign synovitis.
- Threshold commonly used
- At least 40 mm/hour.
- How to use it
- Supports inflammatory or infective pathology but is not specific.
- Threshold commonly used
- Greater than 12 x 10^9/L.
- How to use it
- Useful risk marker but may be normal in some infections.
- Threshold commonly used
- Greater than 20 mg/L in modified criteria.
- How to use it
- Strong additional risk marker; trend and clinical picture matter.
Prediction rules perform differently across populations, organisms and joints. The CRP-containing (Caird) version discriminates better than the original Kocher rule and, in validation work, performs reasonably for large joints beyond the hip. Kingella infection and early disease may be less dramatic, with normal markers in a meaningful minority. If the child looks septic, has severe passive-motion pain, or deteriorates, escalate even if the criteria are incomplete.
Ultrasound
Hip ultrasound detects effusion but does not prove pus. It is most useful when interpreted with fever, weight-bearing status, pain with passive motion, inflammatory markers and clinical trajectory.
MRI
MRI is the escalation test when occult infection, abscess, tumour, stress fracture, discitis, early Perthes disease or unexplained persistent pain remains possible after initial assessment. MRI is also useful when symptoms are severe and the source is unclear.
If SUFE is possible, make the child non-weight bearing and obtain AP pelvis and appropriate lateral hip imaging. Do not force a painful frog lateral in a possible unstable slip.
Microbiology and empirical antibiotic cover
When septic arthritis or osteomyelitis is likely, empirical antibiotics should reflect the most probable organism for the child's age and host factors - a point examiners frequently push to after the Kocher/Caird discussion. Staphylococcus aureus is the commonest pathogen across all ages, but the differential cover changes with age, vaccination status and comorbidity.
- Key organisms
- Staphylococcus aureus, Group B Streptococcus, Gram-negative bacilli (e.g. E. coli).
- Implication for empirical cover
- Broader cover including Gram-negatives; higher risk of multifocal disease and adjacent septic arthritis.
- Key organisms
- Staphylococcus aureus and Kingella kingae (culture-elusive; PCR/blood-culture-bottle inoculation improves yield).
- Implication for empirical cover
- Cover Kingella - it may have mild markers and negative routine cultures and can mimic transient synovitis.
- Key organisms
- Staphylococcus aureus predominant; consider MRSA where prevalent.
- Implication for empirical cover
- Add MRSA cover (e.g. clindamycin/vancomycin) in high-prevalence areas or severe disease.
- Key organisms
- Staphylococcus aureus and Salmonella species.
- Implication for empirical cover
- Salmonella is classically over-represented in sickle-cell osteomyelitis; cover it specifically.
- Key organisms
- Haemophilus influenzae type b (now rare where Hib vaccine is routine).
- Implication for empirical cover
- Consider Hib in the unvaccinated; its decline is a vaccination success story.
- Key organisms
- Neisseria gonorrhoeae (may be polyarticular / migratory with tenosynovitis and rash).
- Implication for empirical cover
- Take a sexual history; gonococcal arthritis needs specific cover and contact tracing.
- Key organisms
- Pseudomonas aeruginosa.
- Implication for empirical cover
- Add anti-pseudomonal cover for plantar puncture osteomyelitis/septic arthritis.
Empirical regimens must follow local paediatric infection guidelines and resistance patterns. Take cultures before antibiotics where the child is stable enough, but never delay antibiotics in a septic child to obtain them.
Differential Diagnosis
- Typical pattern
- Well child, recent viral illness, mild to moderate hip irritation and improving course.
- Immediate decision
- Observe only with clear safety-netting and no septic features.
- Typical pattern
- Fever, toxic appearance, refusal to weight bear and painful passive motion.
- Immediate decision
- Urgent senior review, cultures, imaging, aspiration or washout pathway.
- Typical pattern
- Focal metaphyseal tenderness, fever or pain out of proportion; early radiographs may be normal.
- Immediate decision
- MRI and infection pathway when source remains concerning.
- Typical pattern
- School-age child with limp, hip stiffness and reduced abduction/internal rotation.
- Immediate decision
- AP pelvis and lateral imaging; paediatric orthopaedic referral.
- Typical pattern
- Adolescent with hip, thigh or knee pain, obligatory external rotation and loss of internal rotation.
- Immediate decision
- Make non-weight bearing and image both hips urgently.
- Typical pattern
- Young child with tibial tenderness and reluctance to walk.
- Immediate decision
- Tibia radiographs; repeat imaging or immobilise if clinical suspicion remains.
- Typical pattern
- Night pain, systemic symptoms, bruising, pallor or persistent bone pain.
- Immediate decision
- Urgent paediatric assessment and appropriate imaging/labs.
- Typical pattern
- Mechanism inconsistent with developmental ability or injury pattern.
- Immediate decision
- Document carefully and activate safeguarding pathway.
Management
- Escalate early to senior orthopaedic and paediatric teams.
- Keep nil by mouth if septic arthritis or urgent surgery is possible.
- Obtain cultures and inflammatory markers without delaying treatment in a septic child.
- Aspirate and drain the joint when septic arthritis is likely.
- Start empiric antibiotics according to local paediatric infection guidelines after cultures when safe.
Suspect an underlying endocrine or metabolic disorder when a slip occurs outside the usual window or body habitus: a child younger than about 10 or older than 16 years, or one below the 50th centile for weight (i.e. not the typical overweight adolescent). In these atypical slips, ask about and screen for hypothyroidism, growth-hormone deficiency / panhypopituitarism (especially if on growth-hormone therapy), renal osteodystrophy (chronic kidney disease), and prior pelvic radiotherapy or chemotherapy. Atypical and bilateral slips warrant endocrine referral, and bilaterality (present in a substantial minority, often metachronous) is why both hips are imaged and monitored.
Complications
Early
- Delayed septic arthritis diagnosis with cartilage injury.
- Missed SUFE with progression to unstable slip.
- Missed osteomyelitis with abscess formation.
- Inappropriate reassurance despite malignancy red flags.
- Unrecognised safeguarding concern.
Late
- Avascular necrosis or deformity from missed hip disease.
- Chronic osteomyelitis after delayed infection treatment.
- Growth disturbance from infection or physeal injury.
- Persistent gait abnormality due to missed neuromuscular or structural cause.
- Family loss of trust after vague safety-netting.
Observation is only safe when the child is well, the examination is reassuring, red flags are absent and the family knows exactly when to return.
Decision-Making in Practice
A limping child is a safety diagnosis until the dangerous causes are excluded. The first decision is not the final diagnosis; it is whether the child is systemically unwell, unable to weight bear, has severe pain, has a septic joint risk or has a non-orthopaedic emergency.
- Key findings
- Fever, tachycardia, severe pain, refusal to move joint, high CRP or rigors
- Action
- Urgent senior review, cultures, imaging, aspiration or washout pathway
- Key findings
- Refuses to walk after analgesia or has night/rest pain
- Action
- Image and investigate; do not label as benign transient synovitis
- Key findings
- Toddler fracture, Perthes, slipped epiphysis, infection, malignancy or inflammatory disease by age
- Action
- Choose imaging by age, site and red flags
- Key findings
- Knee pain, limited hip rotation or obligate external rotation
- Action
- Image the hip when knee symptoms do not explain the presentation
- Key findings
- Comfortable, afebrile, walking, normal or improving markers
- Action
- Safety-net with clear return triggers
The assessment should use age bands. Toddlers commonly have occult trauma, toddler fracture or infection. Children aged four to eight need careful assessment for Perthes, transient synovitis and infection. Adolescents need slipped upper femoral epiphysis considered even when pain is felt in the knee. Any age can present with malignancy, inflammatory disease, discitis or non-accidental injury.
Transient synovitis is a diagnosis of recovery, not a label for every painful hip. A child who remains febrile, cannot weight bear, has rising inflammatory markers, severe passive-motion pain or persistent symptoms needs reassessment for septic arthritis, osteomyelitis, abscess or another diagnosis.
Clinical Reasoning Notes
Do not start with a long list of diagnoses. Start with the child status: sick or well, weight bearing or not, painful or painless, and age band. This immediately separates septic arthritis and major red flags from the more common benign causes.
Transient synovitis is common, but the diagnosis should include why septic arthritis is unlikely. A well child who can weight bear, has mild symptoms after a viral illness, has improving pain and has reassuring inflammatory markers is very different from a febrile child who refuses to move the hip.
A normal X-ray is not the same as a normal child. Early osteomyelitis, tumour, toddler fracture, stress fracture and early Perthes disease can have subtle or normal radiographs. If the story remains concerning, escalate to MRI, repeat imaging or senior review rather than discharging on the basis of one normal film.
Non-accidental injury is not an accusation; it is a safety diagnosis that must be considered when the history, developmental stage and injury pattern do not match. The orthopaedic role is to recognise the mismatch, document carefully and activate the correct safeguarding pathway.
The discharge plan should sound precise: "This is the most likely diagnosis, these are the dangerous diagnoses we do not currently think are present, this is the follow-up plan, and these symptoms should bring you back urgently."
Common pitfalls
- Calling it transient synovitis before assessing septic arthritis risk.
- Forgetting that hip disease can present as knee pain.
- Relying on ultrasound effusion alone to diagnose septic arthritis.
- Missing SUFE because the child points to the knee.
- Ignoring night pain or systemic symptoms.
- Not considering safeguarding in a non-walking child with fracture.
Guidelines, Registries & Global Practice
The limping child is a worldwide presentation, but the diagnostic emphasis and available tools vary by setting. The core safety logic, separating sepsis and red flags from benign causes, is universal.
Global epidemiology
- Limp is a common paediatric emergency presentation; transient synovitis is the single most frequent cause of acute non-traumatic hip pain in children, typically aged 3 to 8 years.
- Septic arthritis of the hip is uncommon but time-critical, with the highest incidence in infants and young children.
- Kingella kingae is now recognised as the leading cause of osteoarticular infection in children under 4 years where molecular diagnostics are used; in settings reliant on conventional culture, a high proportion of these infections are reported as culture-negative.
- Perthes disease peaks at roughly 4 to 8 years with a male predominance; reported incidence varies several-fold between populations and is higher in some northern European cohorts.
- SUFE incidence tracks childhood obesity and is rising in many regions; bilaterality is common, which is why both hips are imaged and monitored.
Side-by-side guidance
- Emphasis
- Scenario-driven imaging by age, localisation, fever and weight-bearing status.
- Practical point
- No single test fits all; radiograph, ultrasound and MRI each have defined roles.
- Emphasis
- Early senior involvement, structured assessment and timely access to MRI and theatre for the septic joint.
- Practical point
- A non-weight-bearing febrile child should not wait for routine pathways.
- Emphasis
- GRADE-based diagnosis and treatment of bone and joint infection, including MRI for extent and source control.
- Practical point
- Culture and marker trends guide antibiotic duration and the IV-to-oral switch.
- Emphasis
- Physeal injury principles for SUFE and containment principles for Perthes.
- Practical point
- Stable versus unstable SUFE and lateral pillar grade in Perthes drive management.
Registry and surveillance notes
- Unlike arthroplasty, the limping child has no single implant registry; evidence comes from prospective cohorts (Kocher, Caird), classification studies (Loder, Herring) and national infection surveillance.
- SUFE and Perthes outcomes are tracked through paediatric orthopaedic networks and multicentre studies rather than device registries, which is why classification-based prognosis (lateral pillar, stable/unstable) remains central.
High- versus limited-resource practice
- Where MRI and molecular testing are readily available, occult infection, early Perthes disease and Kingella can be confirmed earlier and aspiration targeted more precisely.
- In limited-resource settings, serial clinical examination, repeat plain radiographs, ultrasound and empirical pathways carry more weight, and a lower threshold for senior review and joint aspiration compensates for diagnostic uncertainty.
- The universal safety rule holds everywhere: a febrile child who will not weight bear is treated as a possible septic joint until excluded, regardless of the imaging available.
Controversies and Areas of Uncertainty
- Prediction rules versus clinical judgement. Kocher and Caird criteria stratify risk but were derived in specific hip cohorts and perform variably elsewhere. They support, never replace, aspiration and senior review when a child looks septic.
- The Kingella era. The rise of Kingella kingae, which often produces mild markers and negative cultures, blurs the line between transient synovitis and true infection in toddlers and challenges scores built before molecular testing.
- Imaging escalation thresholds. When to move from radiograph and ultrasound to MRI, and how quickly, is debated and resource-dependent; MRI is the most sensitive escalation test but access and the need for sedation in young children constrain its use.
- Perthes containment. The benefit of operative containment is concentrated in older children with more severe lateral pillar grades; for younger or milder hips, observation may match surgery, so management remains individualised.
- Antibiotics before aspiration. Balancing prompt empirical antibiotics in a septic-looking child against obtaining diagnostic cultures first is a recurring judgement call, guided by how unwell the child is.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A six-year-old has fever, hip pain and refuses to weight bear. What is your approach?”
“An overweight adolescent presents with vague knee pain and a limp. The knee X-ray is normal. What must you do?”
“A 14-month-old who was crawling and cruising is brought in refusing to bear weight on the right leg. There is no clear history of trauma and the child is afebrile. How do you proceed?”
First Look
- Sick or well
- Weight bearing or not
- Painful or painless
- Age band
- Hip screen
Red Flags
- Fever
- Refusal to walk
- Night pain
- Systemic symptoms
- Severe hip stiffness
- Safeguarding concern
Do Not Miss
- Septic arthritis
- Osteomyelitis
- SUFE
- Perthes disease
- Malignancy
- Non-accidental injury
Safe Plan
- Analgesia
- Targeted imaging
- Escalate high risk
- Defined review
- Clear return triggers
Evidence Signals
Acutely limping child imaging is scenario-based
- Imaging choice should be driven by age, localisation, fever, weight-bearing status and suspected diagnosis.
- Radiography, ultrasound, MRI, nuclear medicine and CT each have specific roles.
- No single imaging test replaces the clinical scenario.
Kocher criteria identify high-risk irritable hips
- The original predictors were fever, non-weight bearing, ESR at least 40 mm/hour and WBC greater than 12 x 10^9/L.
- Risk increased as more predictors were present.
- The rule was developed for differentiating septic arthritis from transient synovitis of the hip.
CRP improves septic hip risk assessment
- CRP greater than 2.0 mg/dL, or greater than 20 mg/L, was a strong independent risk factor.
- The modified criteria add CRP to the original Kocher variables.
- Clinical judgement and joint aspiration remain essential when septic arthritis is likely.
PIDS/IDSA 2021 guideline on acute haematogenous osteomyelitis
- GRADE-based multidisciplinary guideline for diagnosis and management of acute haematogenous osteomyelitis in children.
- MRI is recommended when abscess, the extent of infection or source control is uncertain.
- Cultures, inflammatory marker trends and response to therapy guide antimicrobial duration and the oral switch.
Caird modified algorithm outperforms Kocher and extends beyond the hip
- Secondary analysis of a prospective paediatric emergency cohort presenting with monoarticular joint pain.
- The Caird (CRP-containing) algorithm discriminated septic arthritis better than Kocher (AUC 0.84 versus 0.75 for hip).
- The Caird algorithm also performed well for non-hip joints (knee, ankle, elbow), AUC approximately 0.80.
Kingella kingae is the leading cause of infection in under-fours and is culture-elusive
- In 123 children aged 6 to 48 months with atraumatic osteoarticular complaints, Kingella accounted for 30 of 40 osteoarticular infections.
- Oropharyngeal swab PCR for Kingella had 100 percent sensitivity and 90.5 percent specificity for Kingella osteoarticular infection.
- Kingella infection is often low-grade, with normal CRP and white-cell count in a substantial minority, so it can mimic transient synovitis.
Evidence Base
SUFE physeal stability predicts avascular necrosis
- Reclassified slipped capital femoral epiphysis as stable or unstable based on ability to weight bear rather than acute or chronic.
- Avascular necrosis developed in 14 of 30 (47 percent) unstable slips and in none of the 25 stable slips.
- A satisfactory result occurred in 96 percent of stable but only 47 percent of unstable hips.
Perthes outcome driven by lateral pillar and age, not bracing
- Prospective multicentre study of 345 hips followed to skeletal maturity across five treatment groups.
- Lateral pillar classification and age at onset were the strongest predictors of outcome; bracing was no better than observation.
- Children over 8 years with lateral pillar B or B/C-border hips did significantly better with surgical containment.
Leukaemia can masquerade as juvenile arthritis
- Among 762 children with acute lymphoblastic leukaemia, 49 (6.4 percent) initially presented mimicking juvenile arthritis.
- Common features were fever, pallor, night pain and bone pain, often with asymmetric oligoarthritis.
- These children tended to have lower total leukocyte counts and a longer symptom-to-diagnosis interval.
Age-based diagnostic reasoning
- The common causes of limp change with developmental stage.
- Toddler, child and adolescent groups need different first-line thinking.
- Age-based pathways reduce missed hip disease and infection.