Osteomyelitis, septic arthritis, MRI escalation and surgical drainage
- Acute haematogenous osteomyelitis often begins in the metaphysis.
- Septic arthritis can rapidly damage cartilage.
- Kingella infection in toddlers can be subtle.
- MRI defines marrow, subperiosteal abscess and adjacent joint involvement.
- Antibiotic duration and route depend on organism, response and local protocols.
- “Pseudoparalysis in a baby is infection until proven otherwise.
- “Hip and shoulder infections in infants can cross into the joint through transphyseal vessels.
- “Culture before antibiotics when safe, but do not delay antibiotics in a septic child.
- “Failure of CRP to fall should trigger a search for undrained pus.
A child with fever, severe limb pain and refusal to use the limb has infection until proven otherwise. Do not be reassured by a normal early X-ray.
Images and Diagrams

- Answer
- Septic arthritis with pus under pressure in a joint
- Clinical use
- Needs aspiration or washout plus antibiotics
- Answer
- MRI
- Clinical use
- Shows osteomyelitis, abscess and joint spread
- Answer
- Kingella kingae in young children
- Clinical use
- Can present with less dramatic fever and blood tests
- Answer
- Clinical improvement and falling inflammatory markers
- Clinical use
- Guides IV to oral transition and duration
SICKInfection Red Flags
Hook:SICK keeps the first assessment focused on sepsis, imaging, cultures and source control.
CULTUREMicrobiology Plan
Hook:CULTURE keeps microbiology useful without delaying urgent treatment in an unwell child.
JOINTSeptic Arthritis
Hook:JOINT keeps septic arthritis assessment focused on joint motion, aspiration and timely drainage.
Overview/Epidemiology
Paediatric bone and joint infection is time-sensitive because bacteria, pus and inflammatory pressure can damage cartilage, physis and bone quickly. The two core diagnoses are acute haematogenous osteomyelitis and septic arthritis, but many children sit between these categories: metaphyseal infection may spread to an adjacent joint, a subperiosteal abscess may mimic a joint problem, or pyomyositis may present as a painful limb with fever.
Acute haematogenous osteomyelitis often starts in metaphyseal bone around the knee, hip, ankle and shoulder. Septic arthritis is an orthopaedic emergency because pus within a joint can rapidly damage cartilage and because joint drainage is a source-control decision, not merely an antibiotic decision.
Presentation varies with age. Neonates and infants may present with irritability, poor feeding or pseudoparalysis rather than a classic fever. Toddlers with Kingella kingae infection may have a subtler systemic response than children with Staphylococcus aureus. Children with sickle cell disease, immunosuppression, penetrating wounds or unusual exposures need organism-specific thinking.
The key management question is not "which antibiotic first?" It is "does this child have pus that needs drainage, and have we obtained cultures without delaying treatment?" Antibiotics treat bacteria, but undrained pus can keep the child febrile, painful and systemically unwell.
Pathophysiology

Bacteria seed metaphyseal vessels where sluggish flow and vascular loops favour bacterial deposition. Infection raises intramedullary pressure, compromises perfusion and can break through cortex into a subperiosteal abscess.
- Pathophysiology
- Bacterial seeding starts in metaphyseal marrow and may extend through cortex.
- Clinical consequence
- Early X-rays can be normal; MRI defines marrow and abscess extent.
- Pathophysiology
- Transphyseal vessels can connect metaphysis, epiphysis and joint in infants.
- Clinical consequence
- Hip and shoulder infections can rapidly become combined bone-joint infection.
- Pathophysiology
- Pus and inflammatory mediators damage cartilage by pressure, enzymes and impaired nutrition.
- Clinical consequence
- Painful passive motion is a major warning sign and source control is urgent.
- Pathophysiology
- Common pathogen; MRSA risk depends on local epidemiology.
- Clinical consequence
- Empiric antibiotics must match local resistance patterns.
- Pathophysiology
- Important in toddlers and young children, often with subtler fever and blood-test changes.
- Clinical consequence
- A well-looking toddler can still have true osteoarticular infection.
- Pathophysiology
- Sickle cell disease, puncture wounds, bites, water or farm exposure change organism probability.
- Clinical consequence
- History should change antibiotic and culture strategy.
Delayed or inadequate source control can lead to abscess expansion, pathological fracture, chronic osteomyelitis, sinus formation, growth disturbance, angular deformity, limb-length discrepancy, joint stiffness, chondrolysis, dislocation or avascular necrosis after septic hip.
The Intra-articular Metaphysis and Combined Infection
A key anatomical reason a metaphyseal osteomyelitis becomes a septic joint is the position of the metaphysis relative to the joint capsule. At most joints the metaphysis is extracapsular, so a metaphyseal abscess that breaks through the cortex forms a subperiosteal collection. At a handful of joints the metaphysis lies inside the capsule, and there a metaphyseal abscess can rupture directly into the joint, converting osteomyelitis into a secondary (combined) septic arthritis.
- Intracapsular metaphysis
- Proximal femoral metaphysis is within the capsule
- Consequence
- Proximal femoral osteomyelitis can decompress into the hip - combined infection and risk to the femoral head blood supply
- Intracapsular metaphysis
- Proximal humeral metaphysis is intracapsular
- Consequence
- Proximal humeral osteomyelitis can seed the shoulder joint
- Intracapsular metaphysis
- Proximal radial metaphysis is intracapsular
- Consequence
- Radial neck osteomyelitis can involve the elbow
- Intracapsular metaphysis
- Distal fibular (and part of distal tibial) metaphysis is intracapsular
- Consequence
- Distal fibular osteomyelitis can involve the ankle
This intracapsular-metaphysis route operates at any age. In infants up to around 18 months a second route also exists: transphyseal vessels that cross the physis connect the metaphysis, epiphysis and joint (as noted above), adding to the risk of combined bone-and-joint infection in this age group.
The proximal femur, proximal humerus, proximal radius and distal fibula have intracapsular metaphyses, so a metaphyseal abscess at these sites can rupture straight into the joint. This anatomy is why a "septic hip" may in fact be a proximal femoral osteomyelitis decompressing into the joint, and why the adjacent joint must always be assessed.
Neonatal Bone and Joint Infection
Infection in the neonate behaves as a distinct entity and is easy to miss because the classic signs are usually absent. A septic neonate may simply feed poorly, be irritable or lethargic, or stop moving a limb (pseudoparalysis), often without fever or a raised white-cell count.
- Neonatal specifics
- Often afebrile; poor feeding, irritability, lethargy or pseudoparalysis rather than systemic toxicity
- Action
- Treat pseudoparalysis as infection until proven otherwise; very low threshold to investigate
- Neonatal specifics
- Multiple bones and joints are commonly involved
- Action
- Examine every limb and joint and image widely rather than the symptomatic site alone
- Neonatal specifics
- Group B streptococcus and Staphylococcus aureus predominate, with Gram-negatives such as E. coli
- Action
- Empiric cover must include group B streptococcus, S. aureus and Gram-negative organisms
- Neonatal specifics
- Patent transphyseal vessels readily carry infection from metaphysis to epiphysis and joint
- Action
- Anticipate combined bone-and-joint infection and assess the adjacent joint
- Neonatal specifics
- High rate of physeal and epiphyseal damage, growth arrest, deformity and avascular necrosis (especially the hip)
- Action
- Early aspiration/drainage and long-term growth follow-up
In a neonate, the absence of fever and a normal white-cell count do not exclude bone or joint infection. Pseudoparalysis, poor feeding or irritability should trigger a full septic screen, examination of every limb, and a low threshold for ultrasound, MRI and aspiration - and remember the infection is often multifocal.
Classification
- Osteomyelitis: infection centred in bone marrow and cortex.
- Septic arthritis: infection within a joint space.
- Combined infection: osteomyelitis with adjacent septic arthritis, especially in young children.
- Pyomyositis or abscess: soft-tissue collection that may mimic bone pain.
Clinical Presentation
History
The history should establish severity, likely source, organism clues and whether cultures may already be compromised.
- Ask specifically
- Acute severe pain, progressive limp, refusal to walk, refusal to use limb, pseudoparalysis and response to analgesia.
- Why it matters
- Defines urgency and distinguishes bone tenderness from joint sepsis.
- Ask specifically
- Fever, rigors, malaise, poor feeding, irritability, lethargy or sepsis features.
- Why it matters
- Toxic children need immediate treatment; neonates may be subtle.
- Ask specifically
- Skin infection, varicella, puncture wound, surgery, bite, farm, water or footwear puncture.
- Why it matters
- Changes organism and antibiotic thinking.
- Ask specifically
- Antibiotics already given, prior aspiration, previous admission and immunisation status where relevant.
- Why it matters
- Culture yield and empiric strategy may be affected.
- Ask specifically
- Sickle cell disease, immunosuppression, diabetes, indwelling lines, renal disease, malignancy or neonatal history.
- Why it matters
- Raises risk of unusual organisms or severe spread.
- Ask specifically
- Back pain, abdominal pain, psoas symptoms, refusal to sit, refusal to crawl or multifocal pain.
- Why it matters
- May indicate discitis, pelvic osteomyelitis, psoas abscess or multifocal infection.
Examination
Examine the whole child first. Tachycardia, fever, toxicity, dehydration and reduced interaction change urgency. Then localise the problem.
- Interpretation
- Systemic infection may be progressing.
- Action
- Resuscitate, involve paediatrics/ID/orthopaedics and do not delay antibiotics for perfect cultures.
- Interpretation
- Septic arthritis until proven otherwise.
- Action
- Urgent aspiration or washout pathway.
- Interpretation
- Osteomyelitis is likely, but adjacent joint spread must be excluded.
- Action
- MRI when extent or abscess is uncertain.
- Interpretation
- Bone or joint infection may be present without classic fever.
- Action
- High suspicion, image the region and assess adjacent joints.
- Interpretation
- May identify entry point and organism risk.
- Action
- Culture when possible and broaden exposure history.
- Interpretation
- Abscess, aggressive infection or compartment syndrome concern.
- Action
- Senior review and urgent imaging/source-control decision.
Always assess adjacent joints and the spine when the child will not walk. Document neurovascular status and look for skin portals, puncture wounds, cellulitis, surgical scars, bites and pressure areas.
The child who will not let you move a joint passively is different from the child with focal bone tenderness; both are serious, but septic arthritis changes the clock.
Investigations
- Investigation
- Plain radiographs then MRI when suspicion persists
- Decision it informs
- X-ray excludes other pathology; MRI defines marrow and abscess
- Investigation
- FBC, ESR, CRP and blood cultures
- Decision it informs
- Supports diagnosis and tracks response
- Investigation
- Urgent ultrasound-guided or operative aspiration
- Decision it informs
- Confirms pus and obtains culture
- Investigation
- Repeat MRI or ultrasound
- Decision it informs
- Finds undrained abscess or wrong diagnosis
Blood tests and cultures
FBC, ESR and CRP support diagnosis and trend response. CRP is particularly useful for monitoring because it changes faster than ESR. Obtain blood cultures before antibiotics when safe, but do not leave a septic child untreated for ideal culture timing. Joint aspirate, bone aspirate or operative tissue should be sent for Gram stain, culture and sensitivity when drainage or biopsy occurs.
Imaging
Plain radiographs are useful first-line imaging because they may show alternative diagnoses, advanced bone change, fracture or tumour, but they can be normal early in osteomyelitis. Ultrasound is useful for joint effusion and superficial collection. MRI is the best escalation test for marrow oedema, subperiosteal abscess, intraosseous abscess, pyomyositis, soft-tissue spread, multifocal disease and adjacent joint involvement.
Response monitoring
Clinical response should be visible: falling fever, decreasing pain, improved limb use and falling CRP. Failure to improve should trigger a search for undrained pus, resistant organism, wrong diagnosis, adjacent septic joint, multifocal infection or inadequate drug delivery.
Differential Diagnosis
- Clue
- Well child with hip effusion and improving symptoms.
- Risk if mistaken for simple infection
- Calling true septic arthritis benign.
- Clue
- Focal tenderness, mechanism or healing periosteal reaction.
- Risk if mistaken for simple infection
- Unnecessary antibiotics or missed safeguarding concern.
- Clue
- Night pain, bruising, pallor, weight loss or systemic symptoms.
- Risk if mistaken for simple infection
- Biopsy delay or inappropriate drainage procedure.
- Clue
- Morning stiffness, multiple joints, recurrent swelling or rash.
- Risk if mistaken for simple infection
- Prolonged antibiotics without rheumatology diagnosis.
- Clue
- Recurrent sterile inflammatory bone lesions, often multifocal.
- Risk if mistaken for simple infection
- Repeated antibiotics and surgery without inflammatory diagnosis.
- Clue
- Refusal to sit or walk, back stiffness, abdominal or psoas symptoms.
- Risk if mistaken for simple infection
- Missed spinal or pelvic source.
Management

The treatment plan has three linked goals: stabilise the child, identify and treat the organism, and obtain source control when pus is present. Antibiotics without source control may fail; surgery without microbiology may make definitive treatment harder.
- Treatment direction
- Urgent aspiration or operative washout plus antibiotics.
- Reason
- Cartilage is at risk and pus under pressure needs drainage.
- Treatment direction
- Antibiotics and close clinical/CRP monitoring may be enough.
- Reason
- No drainable source has been identified.
- Treatment direction
- Drain if large, symptomatic, accessible or not responding.
- Reason
- Antibiotics penetrate poorly into undrained pus.
- Treatment direction
- Reassess, repeat imaging and reconsider organism or diagnosis.
- Reason
- Persistent fever, pain or CRP rise often means source control is incomplete.
- Assess sepsis and resuscitate if needed.
- Immobilise for comfort and give analgesia.
- Obtain blood cultures and inflammatory markers.
- Image to localise bone, joint or soft-tissue infection.
- Start empiric antibiotics according to local protocols after cultures when safe.
Complications
Early
- Sepsis and clinical deterioration.
- Abscess formation or spread to adjacent joint.
- Pathological fracture in severe osteomyelitis.
- Joint dislocation or cartilage injury in septic arthritis.
- Need for repeat drainage.
Late
- Growth arrest or angular deformity.
- Avascular necrosis after septic hip.
- Chronic osteomyelitis or sinus formation.
- Joint stiffness, chondrolysis or degenerative change.
- Limb length discrepancy after physeal injury.
The biggest mistake is treating infection as a single dose of antibiotics. Source control, organism control and growth follow-up are all part of the treatment.
Decision-Making in Practice
Paediatric bone and joint infection management is source-control thinking. Antibiotics are essential, but the child improves only when the organism, anatomical source and any pus under pressure are addressed.
- How to decide
- Painful passive motion, effusion, fever, raised CRP or aspirate findings
- Management consequence
- Urgent aspiration or washout plus antibiotics
- How to decide
- MRI for marrow, subperiosteal abscess, pyomyositis and adjacent joint
- Management consequence
- Defines whether antibiotics alone are enough
- How to decide
- Blood cultures, aspirate, bone or abscess culture when safe
- Management consequence
- Narrow therapy and identify Kingella, MRSA or unusual organisms
- How to decide
- Organism, CRP fall, fever resolution, function and source control
- Management consequence
- Switch to oral only when clinical response is secure
- How to decide
- Persistent fever, rising CRP, pain or poor function
- Management consequence
- Search for undrained pus, wrong organism or alternative diagnosis
The most important fork is septic arthritis versus osteomyelitis without joint sepsis. Septic arthritis is a cartilage emergency. Osteomyelitis may be managed medically if the child is stable and there is no collection requiring drainage, but abscess, adjacent joint spread, toxic sepsis or failure of inflammatory markers to fall should trigger repeat imaging and source control.
Kingella kingae has changed the interpretation of the well-looking toddler with osteoarticular infection. Fever and blood tests may be less dramatic, so age, joint symptoms, PCR where available and clinical trajectory matter. Staphylococcus aureus remains central, and local MRSA prevalence should guide empiric therapy.
Clinical Reasoning Notes
- Safe answer
- Name bone, joint, both or soft tissue.
- Common miss
- Treating every painful limb as a single diagnosis.
- Safe answer
- Look for septic joint, subperiosteal abscess, intraosseous abscess or pyomyositis.
- Common miss
- Continuing antibiotics while source control is incomplete.
- Safe answer
- Pain, fever, mobility and CRP should move in the right direction.
- Common miss
- Ignoring a rising CRP or persistent refusal to use the limb.
- Safe answer
- Blood, joint, bone or abscess cultures when safe.
- Common miss
- Missing organism data, especially after prior antibiotics.
- Safe answer
- Growth, joint motion, recurrence and limb-length or angular deformity.
- Common miss
- Stopping care once fever resolves.
Common pitfalls
- Calling it transient synovitis in a febrile non-weight-bearing child.
- Using normal X-ray to exclude early osteomyelitis.
- Forgetting Kingella in toddlers.
- Not imaging the adjacent joint.
- Continuing antibiotics without looking for undrained abscess when CRP rises.
- Stopping follow-up before growth risk is clear.
Guidelines, Registries & Global Practice
Paediatric bone and joint infection is managed worldwide, but organism prevalence, imaging access and antibiotic resistance differ markedly between settings. A globally valid answer states the principle, then flags the local variable that changes it.
Global epidemiology
- Acute haematogenous osteomyelitis has an estimated incidence of roughly 1 to 13 per 100,000 children per year in high-income countries, with higher rates reported in some low- and middle-income and Indigenous populations.
- Septic arthritis incidence is broadly similar in magnitude, peaking in children under 3 years; boys are affected more often than girls.
- Staphylococcus aureus is the dominant pathogen at all ages worldwide. Kingella kingae is the leading cause in the 6 to 24 month group where blood-culture-bottle inoculation and PCR are used. Group B streptococcus and Gram-negative organisms feature in neonates.
- Community-associated MRSA prevalence varies enormously by region and is the single most important driver of empiric antibiotic choice.
Side-by-side guideline comparison
- Imaging stance
- MRI preferred when extent or a collection is uncertain.
- Treatment emphasis
- GRADE-based; early oral switch, shorter courses, surgery for source control.
- Imaging stance
- Radiograph first, MRI with and without contrast as the key advanced study, ultrasound to guide hip aspiration.
- Treatment emphasis
- Imaging should change management, not just confirm inflammation.
- Imaging stance
- Ultrasound and MRI used pragmatically; urgent aspiration of the irritable hip.
- Treatment emphasis
- Prompt source control; supports shorter, oral-switch antibiotic regimens with paediatric ID input.
- Imaging stance
- MRI where available; PCR and blood-culture bottles to capture Kingella.
- Treatment emphasis
- Short-course, early-oral regimens informed by the Finnish RCTs.
Registry and surveillance notes
- Unlike arthroplasty, paediatric infection has no single global implant registry; evidence comes from national surveillance, MRSA resistance monitoring and multicentre cohorts such as the Finnish trials.
- Antimicrobial resistance surveillance networks (for example regional MRSA and Kingella susceptibility data) effectively function as the registries that shape empiric protocols.
High- vs limited-resource practice variation
- Well-resourced setting
- Early MRI and ultrasound on demand.
- Limited-resource setting
- Reliance on radiographs and clinical course; MRI may be delayed or unavailable.
- Well-resourced setting
- PCR, blood-culture bottles, rapid sensitivities.
- Limited-resource setting
- Plate culture only, lower Kingella yield, more empiric treatment.
- Well-resourced setting
- Often earlier, less advanced disease.
- Limited-resource setting
- Later presentation with more chronic osteomyelitis, sequestrum and deformity.
- Well-resourced setting
- Short IV then early oral switch.
- Limited-resource setting
- Longer IV courses and more open surgery where oral bioavailability or follow-up is uncertain.
Controversies and Areas of Uncertainty
Several long-held teachings have softened as randomised and registry data have accumulated. Examiners reward candidates who can state where genuine equipoise exists rather than reciting dogma.
- Traditional view
- Several weeks of IV therapy.
- Current evidence and nuance
- Peltola RCTs support roughly 10 days for septic arthritis and 20 days for osteomyelitis, mostly oral, when CRP normalises quickly in uncomplicated MSSA disease.
- Traditional view
- Prolonged IV via PICC line.
- Current evidence and nuance
- Early oral switch once improving reduces line complications without worsening outcomes; PICC-related harm is now a recognised driver of change.
- Traditional view
- Formal arthrotomy for every septic joint, especially hip and shoulder.
- Current evidence and nuance
- Many joints settle after single aspiration plus antibiotics; the hip remains the joint with the lowest threshold for formal drainage.
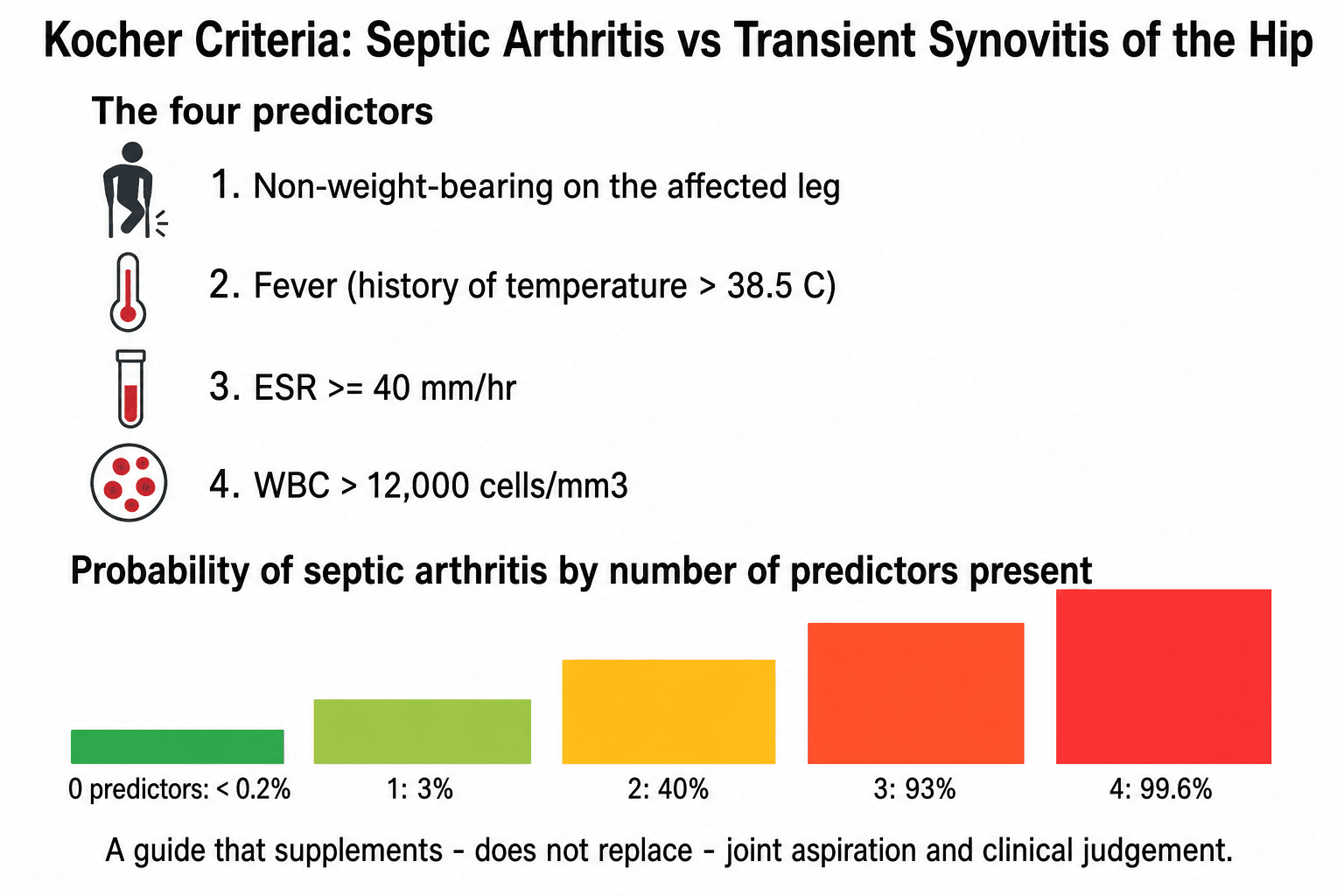
- Traditional view
- Four-variable rule reliably separates septic arthritis from transient synovitis.
- Current evidence and nuance
- External validation is inconsistent; CRP adds value and Kingella is not captured, so the rule guides rather than decides.
- Traditional view
- ESR central to diagnosis.
- Current evidence and nuance
- CRP responds faster and is the preferred monitoring marker; failure of CRP to fall should trigger a search for undrained pus.
- Traditional view
- Reserve MRI for failures.
- Current evidence and nuance
- Earlier MRI changes management by revealing abscess, pyomyositis or adjacent joint disease, but availability and sedation needs limit universal use.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A four-year-old has fever, refuses to weight bear and cries with passive hip rotation. What do you do?”
“A child with distal femur osteomyelitis remains febrile and CRP is rising after antibiotics. What next?”
“An 18-month-old has a 2-day limp and a low-grade temperature. They look well, CRP is only mildly raised and the white cell count is normal. The knee is held flexed and resists passive extension. How do you proceed?”
Recognise
- Fever
- Refusal to walk/use limb
- Pseudoparalysis
- Painful passive joint motion
- Metaphyseal tenderness
Investigate
- FBC ESR CRP
- Blood cultures
- X-ray first
- MRI for marrow/abscess
- Aspiration for septic joint
Treat
- Analgesia
- Cultures when safe
- Empiric antibiotics
- Drain pus
- Monitor CRP and function
Do Not Miss
- Septic hip
- Infant transphyseal spread
- Abscess
- Osteomyelitis
- Growth disturbance
Evidence Signals
These cards are the landmark evidence and current society guidelines that should anchor any viva answer on paediatric bone and joint infection. Two Finnish randomised controlled trials by Peltola and colleagues reshaped global practice by showing that most children can be treated with short antibiotic courses and minimal surgery, while the Kocher prediction rule remains the most cited tool for the irritable hip.
PIDS/IDSA 2021 guideline: diagnosis and management of acute haematogenous osteomyelitis
- First joint PIDS/IDSA clinical practice guideline for acute haematogenous osteomyelitis (AHO), using GRADE methodology.
- MRI is the preferred advanced imaging modality when diagnosis, extent or a drainable collection is uncertain.
- Early transition to oral antibiotics and shorter total courses are recommended once the child is improving and CRP is falling, with surgery reserved for source control.
PIDS/IDSA 2023 guideline: diagnosis and management of acute bacterial arthritis
- Companion guideline to the 2021 AHO document, covering acute bacterial arthritis (ABA) in children using GRADE methodology.
- Synovial fluid and blood cultures should be obtained before or close to antibiotic initiation, and synovial fluid should be inoculated into blood-culture bottles to improve Kingella detection.
- Adjacent osteomyelitis must be considered when symptoms are prolonged or the inflammatory response is marked, and timely drainage is linked to antimicrobial therapy.
Evidence Base
Standardised pathways improve diagnosis and shorten IV treatment
- Retrospective comparison of 117 children (54 pre-guideline, 63 post-guideline) with acute bone and joint infection.
- Implementing an evidence-based pathway significantly reduced IV antibiotic duration and PICC line use (both P less than 0.001).
- Bacterial identification increased (P equals 0.040) without any rise in length of stay or readmission.
Paediatric orthopaedic principle
- Children are not small adults; growth plates, cartilage and remodelling change diagnosis and treatment.
- Serial assessment is often as important as the first radiograph.
- Treatment should protect future reconstructive options.