Clubfoot | CAVE Deformity | Ponseti Method | Relapse Prevention
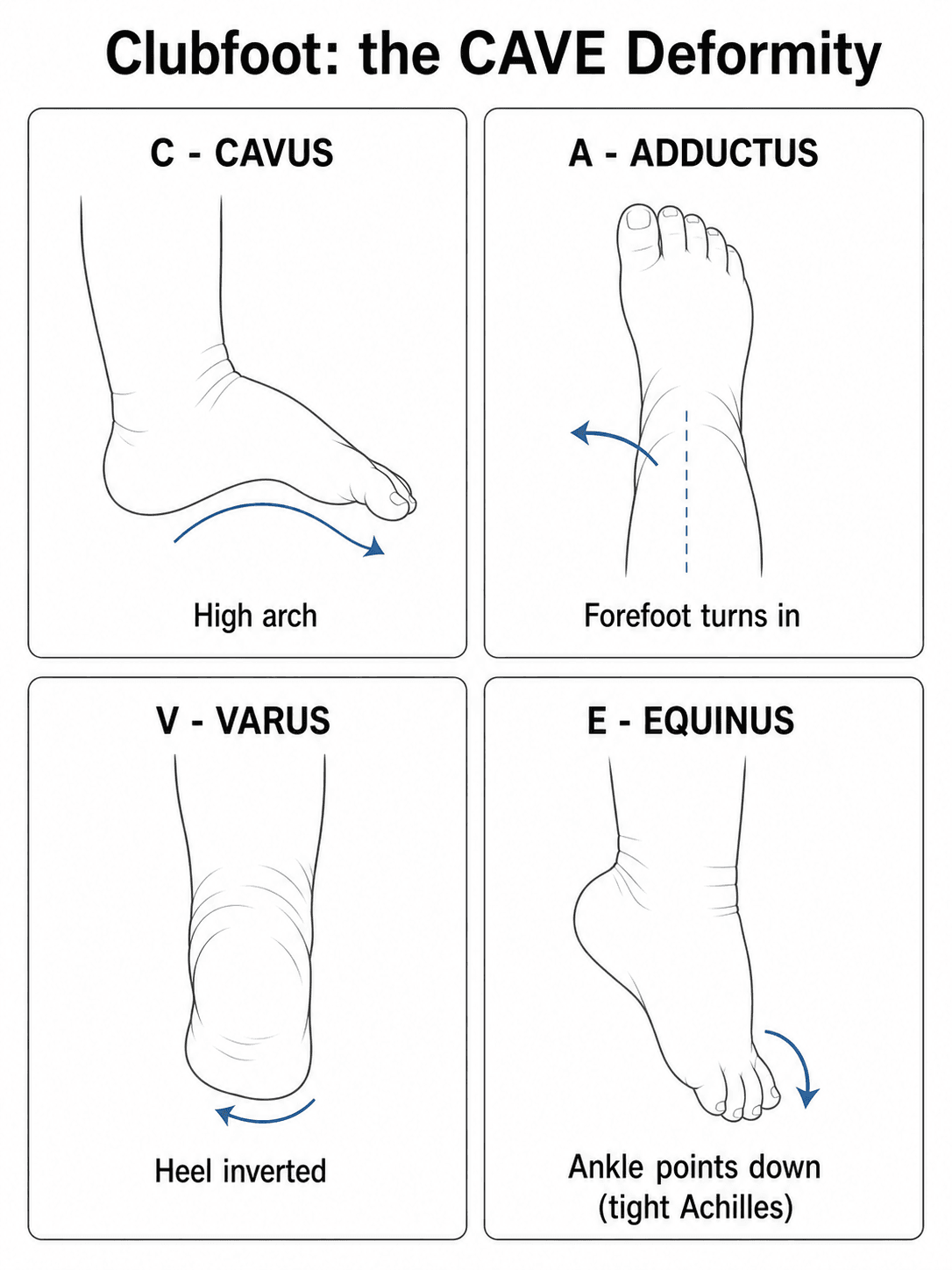
- Clubfoot is a congenital rigid deformity with four components: cavus, adductus, varus, equinus (CAVE)
- Pirani score 0-6 guides treatment; higher scores predict more casts and possible tenotomy
- Ponseti method: weekly serial casts with specific manipulation sequence then percutaneous Achilles tenotomy
- Foot abduction brace (FAB) worn 23 hours/day for 3 months then nights until age 4-5 to prevent relapse
- Relapse managed by repeat casting and possible repeat tenotomy; surgery only for resistant cases
- “Always assess for associated conditions: spina bifida, arthrogryposis, neuromuscular disorders
- “Pirani score greater than 4 predicts need for tenotomy in over 80 percent of cases
- “Never force dorsiflexion before correcting adductus and varus - risks rocker-bottom deformity
- “Foot abduction brace compliance is the single most important factor preventing relapse
Correct in order: Cavus first (supinate forefoot), then adductus and varus together (abduction), equinus last (after tenotomy). Reversing order produces rocker-bottom flatfoot.
Six signs scored 0-1 each: posterior crease, empty heel, rigid equinus, medial crease, lateral head of talus, medial crease. Total 0-6. Score greater than 4 almost always needs tenotomy.
Weekly casts: Manipulate to correct cavus then abduct forefoot while counter-pressure on talus head. Never dorsiflex until last cast. Above-knee casts with knee at 90 degrees.
FAB 23/7 for 3 months then nights until age 4-5. Denis Browne bar with feet externally rotated 60-70 degrees on affected side. Non-compliance causes 30-50 percent relapse rate.
- Assessment
- Pirani score, rule out neuromuscular cause
- Treatment
- Ponseti serial casting weekly
- Key Pearl
- Start within first week of life for best results
- Assessment
- Confirm after 4-6 casts
- Treatment
- Percutaneous Achilles tenotomy
- Key Pearl
- Tenotomy performed in clinic under local
- Assessment
- Recurrent adductus or equinus
- Treatment
- Repeat casting plus possible repeat tenotomy
- Key Pearl
- Bracing compliance review critical
CAVECAVE Deformity Sequence
Hook:Correct CAVE in sequence - cavus, adductus, varus, then equinus after tenotomy!
PELHMMPirani Score Components
Hook:PELHMM scores the six signs - total greater than 4 predicts tenotomy!
ABDUCTPonseti Casting Principles
Hook:ABDUCT the foot correctly - above knee, before dorsiflex, under talus, cavus first, tenotomy last!
Overview and Epidemiology
Clubfoot is the most common congenital musculoskeletal deformity. Untreated it produces a painful, stiff, non-plantigrade foot that severely limits walking and causes lifelong disability. The Ponseti method has transformed outcomes worldwide with greater than 90 percent success when performed correctly, avoiding the need for extensive surgery in most children.
- Incidence: 1 in 1000 live births worldwide
- Bilateral: 50 percent of cases
- Male predominance: 2:1 male to female ratio
- Familial: 30 percent have family history
- Associated conditions: Spina bifida, arthrogryposis, neuromuscular disorders in 10-20 percent
- Untreated: Painful gait, callosities, inability to wear shoes
- Early treatment: Plantigrade flexible foot in over 90 percent
- Relapse risk: 30-50 percent without compliant bracing
- Long-term: Good function into adulthood with proper care
- Global burden: Major cause of disability in low-resource settings
Pathophysiology

The deformity arises from abnormal development of the talus and its articulations. The talus is smaller with medial deviation of the neck. The calcaneus is inverted and medially displaced under the talus. The navicular is displaced medially on the talar head. Contracted soft tissues include the tibialis posterior, Achilles, and plantar fascia. The deformity is rigid and resists passive correction. The CAVE components reflect these fixed bony and soft-tissue relationships.
- Anatomic Cause
- Plantarflexed first ray and contracted plantar fascia
- Clinical Sign
- High medial arch, forefoot supination
- Correction Method
- Supinate forefoot in first cast
- Anatomic Cause
- Medial navicular displacement on talus, tight tibialis posterior
- Clinical Sign
- Medial deviation of forefoot, prominent talar head laterally
- Correction Method
- Abduct forefoot with talar head pressure
- Anatomic Cause
- Inverted calcaneus under talus, tight deltoid and spring ligaments
- Clinical Sign
- Hindfoot inversion, narrow heel
- Correction Method
- Continue abduction to evert calcaneus
- Anatomic Cause
- Contracted Achilles and posterior capsule, plantarflexed talus
- Clinical Sign
- Ankle plantarflexion, empty heel sign
- Correction Method
- Percutaneous tenotomy then dorsiflexion
Cavus first: Supinating the forefoot unlocks the midfoot and allows subsequent abduction. Dorsiflexing early creates a rocker-bottom deformity with midfoot break. Adductus and varus together: Abduction around the talar head corrects both by rotating the calcaneus out from under the talus. Equinus last: Only after the foot is abducted greater than 60 degrees can the ankle be safely dorsiflexed.
Growth drives recurrence: The foot grows rapidly in the first 3-5 years. Without the foot abduction brace holding the foot in abduction and dorsiflexion, the tight medial structures re-contract and the deformity recurs. 23 hours per day initially: Ensures constant stretch during maximal growth velocity. Night bracing until age 4-5: Covers the period of rapid longitudinal growth.
Classification and Types
Pirani and Dimeglio Scoring
- Components
- Six clinical signs (posterior crease, empty heel, rigid equinus, medial crease, lateral talus, medial malleolus)
- Score Range
- 0-6 (each sign 0, 0.5 or 1)
- Clinical Use
- Predicts number of casts and tenotomy need; score greater than 4 predicts tenotomy
- Components
- Four components (equinus, varus, adductus, internal rotation) plus additional points for rigidity
- Score Range
- 0-20
- Clinical Use
- More detailed for research; less used in routine Ponseti clinics
Pirani scoring is performed at each visit and guides progression. A score that plateaus above 2 after four casts suggests need for tenotomy or further evaluation.
Clinical Assessment
- Prenatal diagnosis: Increasingly common with ultrasound
- Family history: 30 percent have affected relative
- Birth history: Full term, any NICU stay
- Associated conditions: Developmental hip dysplasia, spina bifida
- Previous treatment: Any manipulation or casting attempted
- Rigidity: Assess passive correctability of each CAVE component
- Skin: Deep creases, callosities if previously treated
- Neurology: Tone, reflexes, spontaneous movement
- Spine: Dimple, hairy patch, scoliosis
- Hips: Ortolani and Barlow testing for DDH
Posterior crease: 0 = none, 0.5 = superficial, 1 = deep extending to heel. Empty heel: 0 = calcaneus easily palpated, 0.5 = partially filled, 1 = no palpable calcaneus. Rigid equinus: 0 = dorsiflexion past neutral, 0.5 = to neutral, 1 = less than neutral. Medial crease: 0 = none, 0.5 = superficial, 1 = deep to lateral border. Lateral head of talus: 0 = covered, 0.5 = partially covered, 1 = fully uncovered. Medial malleolus to navicular distance: 0 = greater than 1 cm, 0.5 = 0.5-1 cm, 1 = less than 0.5 cm.
- Key Distinguishing Feature
- CAVE deformity, no other anomalies
- Neurologic Signs
- Normal
- Management Difference
- Ponseti method standard
- Key Distinguishing Feature
- Multiple joint contractures, stiff throughout
- Neurologic Signs
- Often normal cognition
- Management Difference
- May require early soft-tissue releases
- Key Distinguishing Feature
- Clubfoot plus lower limb paralysis or sensory loss
- Neurologic Signs
- Absent reflexes, anal wink absent
- Management Difference
- Bracing may need modification for insensate foot
- Key Distinguishing Feature
- Rigid convex plantar surface, rocker-bottom
- Neurologic Signs
- May have neuromuscular association
- Management Difference
- Requires different casting or surgery
Spina bifida: Always examine the spine for dimples or hairy patches. A missed myelomeningocele changes bracing strategy and prognosis dramatically. The foot may be insensate, risking pressure sores with aggressive casting or bracing.
Congenital Vertical Talus: the Critical Mimic
The one diagnosis you must not treat as a clubfoot is congenital vertical talus (CVT) - it looks like a "reverse clubfoot", and casting it in the clubfoot direction makes it worse.
- Clubfoot (CTEV)
- Concave (high medial arch, cavus)
- Congenital vertical talus
- Convex - rigid rocker-bottom
- Clubfoot (CTEV)
- Adducted and supinated
- Congenital vertical talus
- Abducted and dorsiflexed
- Clubfoot (CTEV)
- Equinus plus varus
- Congenital vertical talus
- Equinus plus valgus
- Clubfoot (CTEV)
- Displaced medially on the talus
- Congenital vertical talus
- Dorsally dislocated onto the talar neck (irreducible)
- Clubfoot (CTEV)
- Around 10-20 percent neuromuscular/syndromic
- Congenital vertical talus
- Strongly associated with neuromuscular disease and chromosomal/CNS anomalies
- Clubfoot (CTEV)
- Not routine (clinical diagnosis)
- Congenital vertical talus
- Forced-PLANTARFLEXION lateral - the talus stays vertical and the navicular does not reduce
CVT is managed by the "reverse Ponseti" (Dobbs) method - serial casts that plantarflex and invert the foot (the opposite direction to clubfoot) to reduce the talonavicular joint, followed by percutaneous pinning of the reduced talonavicular joint and an Achilles tenotomy. Recognising it prevents the disaster of casting a vertical talus as though it were a clubfoot.
Investigations
Diagnostic Workup
Pirani score: Document at every visit to track progress. Dimeglio score: Optional for research or complex cases. Photographs: Baseline and serial to monitor correction.
Ultrasound hips: Rule out developmental dysplasia of the hip (increased association). Spine ultrasound or MRI: If any spinal dimple or neurologic sign. Genetic review: For syndromic features or family history.
X-ray: Not routine for idiopathic clubfoot. Useful in older children for assessing tarsal relationships or planning osteotomies. CT or MRI: Reserved for relapsed or revision cases to assess bone and soft-tissue anatomy.
Routine radiographs are not required for diagnosis or monitoring of idiopathic clubfoot treated with Ponseti. The diagnosis is clinical. X-rays are reserved for atypical presentations, suspected vertical talus, or planning secondary surgery in older children. Over-reliance on imaging delays treatment and adds unnecessary cost.
Management Algorithm

Standard Ponseti Method for Idiopathic Clubfoot
Goal: Achieve a plantigrade, flexible, pain-free foot with minimal surgery.
Casting Sequence
Correct cavus: Supinate forefoot to align metatarsal heads. Apply above-knee cast: Knee at 90 degrees, cast to groin. Duration: 7 days.
Abduct forefoot: Counter-pressure on talar head, abduct to 60-70 degrees. Correct varus: Calcaneus everts as abduction progresses. Weekly change: Remove, re-score Pirani, re-manipulate.
Assess for tenotomy: If dorsiflexion blocked at greater than 10 degrees equinus after abduction achieved. Percutaneous Achilles tenotomy: In clinic under local anaesthetic. Final cast: 3 weeks in dorsiflexion and abduction.
The knee must be flexed to 90 degrees in the cast. This prevents the cast from slipping off and maintains the correction achieved by manipulation. Straight-leg casts allow the foot to slip into equinus inside the cast, undoing the week's work.
Anterior Tibialis Tendon Transfer for Dynamic Supination
Between repeat casting and the (rare) posteromedial release sits a key, high-yield relapse operation the algorithm must not skip:
Indication: dynamic supination of a structurally corrected foot - the child (usually about 2.5 to 4 years old) intoes and supinates in the swing phase of gait because of an over-pulling, medially-inserting tibialis anterior, despite a flexible, plantigrade foot at rest. It corrects the muscle imbalance that drives recurrence; it does NOT correct a fixed deformity. Prerequisites: the foot must first be made supple (re-cast any residual fixed deformity first), and the lateral cuneiform must be ossified (hence the age threshold) to receive the transfer. Procedure: the whole tibialis anterior tendon is transferred laterally to the third (lateral) cuneiform, converting it from a supinator/invertor into a more central dorsiflexor and re-balancing the foot; a concurrent repeat tenotomy is added if equinus has recurred. Why it fits Ponseti: it treats the muscle imbalance of relapse with a tendon rebalancing rather than a joint-sacrificing release, keeping the foot mobile. The originator series (Laaveg-Ponseti; Morcuende) reported it as the operation that prevents further relapse.
Complications
Complications arise from the untreated deformity, from faulty casting technique, and from over-aggressive surgery.
- Painful non-plantigrade foot: weight-borne on the dorsolateral border, with callosities and bursae
- Difficulty with footwear and reduced walking tolerance / lifelong disability (a major burden in low-resource settings)
- Fixed bony deformity with secondary degenerative change if relapse is left late
- Relapse (30-50% with non-compliant bracing) - recurrent adductus/equinus
- Rocker-bottom (midfoot break) deformity from dorsiflexing before the cavus/adductus is corrected - the classic technical error
- Cast complications: pressure sores, slippage with loss of correction (below-knee or under-flexed casts), thermal/plaster injury, neurovascular compromise if too tight
- Tenotomy complications: bleeding (posterior tibial/peroneal vessels), incomplete division, rarely neurovascular injury
- Over-correction / pes planovalgus and weakness from extensive posteromedial release; stiffness, scarring and growth disturbance after open surgery
- Brace problems: skin irritation, non-compliance, pressure sores on an insensate (e.g. spina bifida) foot
A ROCKER-BOTTOM deformity is produced by dorsiflexing the foot before the cavus, adductus and varus have been corrected (or before tenotomy relieves the equinus). The midfoot breaks while the hindfoot stays in equinus. Respect the CAVE sequence and never force dorsiflexion early.
Guidelines, Registries & Global Practice
- Incidence is consistent worldwide at approximately 1 in 1000 live births
- Untreated clubfoot remains a major cause of disability in low-resource countries
- Ponseti method has been adopted globally through training programmes in Africa, Asia and Latin America
- Late presentation is common in resource-poor settings and still responds to Ponseti principles
- High-resource: Dedicated clubfoot clinics, trained physiotherapists, custom braces, weekly cast clinics
- Low-resource: Task-shifting to non-physician providers, low-cost braces, community follow-up
- Universal principle: Outcome depends on correct manipulation sequence and brace compliance, not on expensive equipment
- Global initiatives: MiracleFeet, Ponseti International Association, and national programmes have treated hundreds of thousands of children
- Initial Treatment
- Weekly serial casts starting in first week of life
- Tenotomy Indications
- When dorsiflexion blocked after midfoot correction (Pirani greater than 4)
- Bracing Protocol
- 23 hours per day for 3 months, then nights to age 4-5
- Initial Treatment
- Ponseti delivered by specialist physiotherapists in dedicated clinics
- Tenotomy Indications
- Same criteria; performed in outpatient setting
- Bracing Protocol
- Denis Browne bar or equivalent dynamic brace
- Initial Treatment
- Task-shifted to trained clinical officers or nurses
- Tenotomy Indications
- Tenotomy by trained non-surgeons in many settings
- Bracing Protocol
- Locally fabricated braces with community support
There is no international implant registry for clubfoot because the Ponseti method is predominantly non-operative. Long-term outcome data come from single-centre series and national clubfoot programme audits. The consistent message across all registries and guidelines is that early diagnosis, correct casting technique, and brace compliance determine success.
Record in every clubfoot case:
- Pirani score at presentation and each visit
- Number of casts and whether tenotomy performed
- Brace prescription and compliance discussion
- Family education on relapse risk if brace not worn
- Associated conditions screened (spine, hips, neurology)
A child who relapses because of inadequate bracing documentation or education represents a preventable failure of the healthcare system.
Controversies & Areas of Uncertainty
The classic Denis Browne bar is effective but compliance can be poor. Dynamic braces and shorter night-only protocols from age 2 are being studied. No high-level evidence yet defines the minimum effective bracing duration.
Some centres use ultrasound or radiographs to confirm correction, but most high-volume Ponseti practitioners rely on clinical scores alone. The added value of routine imaging has not been demonstrated in randomised trials.
Syndromic, neuromuscular, and arthrogrypotic clubfeet have lower success rates with standard Ponseti. Whether early limited surgery or modified casting protocols improve outcomes remains unclear.
While most children walk normally, subtle stiffness, calf weakness, and higher rates of arthritis in adulthood are reported. The contribution of the original deformity versus treatment remains debated.
MCQ Practice Points
Q: What is the first component of the CAVE deformity to be corrected in the Ponseti method? A: Cavus. The forefoot is supinated to align the metatarsal heads and unlock the midfoot before any abduction or dorsiflexion is attempted. Correcting cavus first prevents a rocker-bottom deformity.
Q: A newborn has a Pirani score of 5. What does this predict? A: High likelihood of needing percutaneous Achilles tenotomy. Scores greater than 4 predict that greater than 80 percent of feet will require tenotomy. The score also correlates with the number of casts required.
Q: Why must casts be applied above the knee with the knee flexed to 90 degrees? A: To prevent cast slippage and maintain correction. Below-knee casts allow the foot to slip back into equinus inside the cast. Knee flexion locks the cast on the limb and maintains the abduction achieved by manipulation.
Q: What is the single most important factor preventing relapse after Ponseti correction? A: Compliance with the foot abduction brace. Non-compliance leads to 30-50 percent relapse rate. The brace must be worn 23 hours per day for 3 months then at night until age 4-5 years.
Q: When is posteromedial release indicated in clubfoot management? A: Only after failed Ponseti treatment despite compliant bracing, or in syndromic/resistant cases. Greater than 95 percent of idiopathic clubfeet are successfully managed without extensive surgery. Posteromedial release is now a last resort.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 2-week-old infant presents with bilateral rigid clubfeet. Pirani score is 5.5 on the right and 4.5 on the left. No other anomalies are found on examination. The parents are anxious about surgery. Outline your management plan.”
“A 3-year-old child who had successful Ponseti treatment as an infant now presents with recurrent adductus and mild equinus. The parents admit the brace was discontinued at age 2 because the child refused to wear it. Pirani score is now 3.0. How do you manage this?”
Key Anatomy and Deformity
- CAVE: cavus (high arch), adductus (forefoot medial deviation), varus (hindfoot inversion), equinus (ankle plantarflexion)
- Talus smaller with medially deviated neck; calcaneus inverted and displaced medially; navicular displaced medially
- Contracted structures: Achilles, tibialis posterior, plantar fascia, posterior and medial capsules
- Rigid deformity resists passive correction; must correct in CAVE sequence
Scoring Systems
- Pirani 0-6: six signs each scored 0, 0.5 or 1 (posterior crease, empty heel, rigid equinus, medial crease, lateral talus, medial malleolus)
- Score greater than 4 predicts tenotomy in over 80 percent of cases
- Dimeglio 0-20: more granular but less used clinically
- Score at every visit to track progress and predict tenotomy
Ponseti Casting Principles
- Above-knee casts with knee at 90 degrees to prevent slippage
- Correct cavus first by supinating forefoot, then abduct around talar head
- Never dorsiflex until adductus and varus corrected (risk of rocker-bottom)
- Weekly casts until midfoot corrected and Pirani plateaus
Tenotomy and Bracing
- Percutaneous Achilles tenotomy when dorsiflexion blocked after midfoot correction
- Final cast 3 weeks in dorsiflexion and abduction after tenotomy
- Foot abduction brace 23 hours per day for 3 months then nights to age 4-5
- Brace compliance is the single most important factor preventing relapse
Relapse and Surgery
- Relapse almost always due to bracing non-compliance; treat with repeat Ponseti casting
- Repeat tenotomy safe if equinus recurs
- Posteromedial release reserved for resistant or syndromic cases after failed Ponseti (less than 5 percent)
- Always exhaust non-operative options before extensive surgery
Evidence Base
Congenital Club Foot: The Results of Treatment (the Classic)
- Seminal description of the manipulation-and-serial-casting technique that became the Ponseti method, followed by retentive bracing
- Reported the results of treatment and established the principle of correcting the deformity in a specific sequence
- Foundational paper now reprinted as a JBJS/CORR 'Classic'
Long-term results of treatment of congenital clubfoot
- 70 patients (104 club feet) followed 10 to 27 years after Ponseti treatment
- Functional results were satisfactory in 88.5% of feet and 90% of patients were satisfied with appearance and function
- Foot/ankle motion was often limited and the talocalcaneal angle frequently not fully corrected; anterior tibial tendon transfer appeared to prevent relapse
Ponseti method for idiopathic clubfoot
- Consecutive series of 157 patients (256 clubfeet); correction achieved in 98% (all but 3 patients), with 90% needing 5 or fewer casts
- Only 2.5% required extensive corrective surgery - a radical reduction versus historical surgical rates
- 11% relapsed, and relapse was related to foot-abduction-brace non-compliance rather than age, prior treatment or initial severity
Relapse after Ponseti treatment
- 51 infants (86 idiopathic clubfeet) treated by the Ponseti method, analysed for recurrence risk factors
- Brace NON-COMPLIANCE was overwhelmingly the strongest predictor of recurrence (odds ratio 183, p<0.00001)
- Lower parental education (high-school or less) was also significant (OR 10.7); deformity severity, age at start and prior treatment were NOT predictive