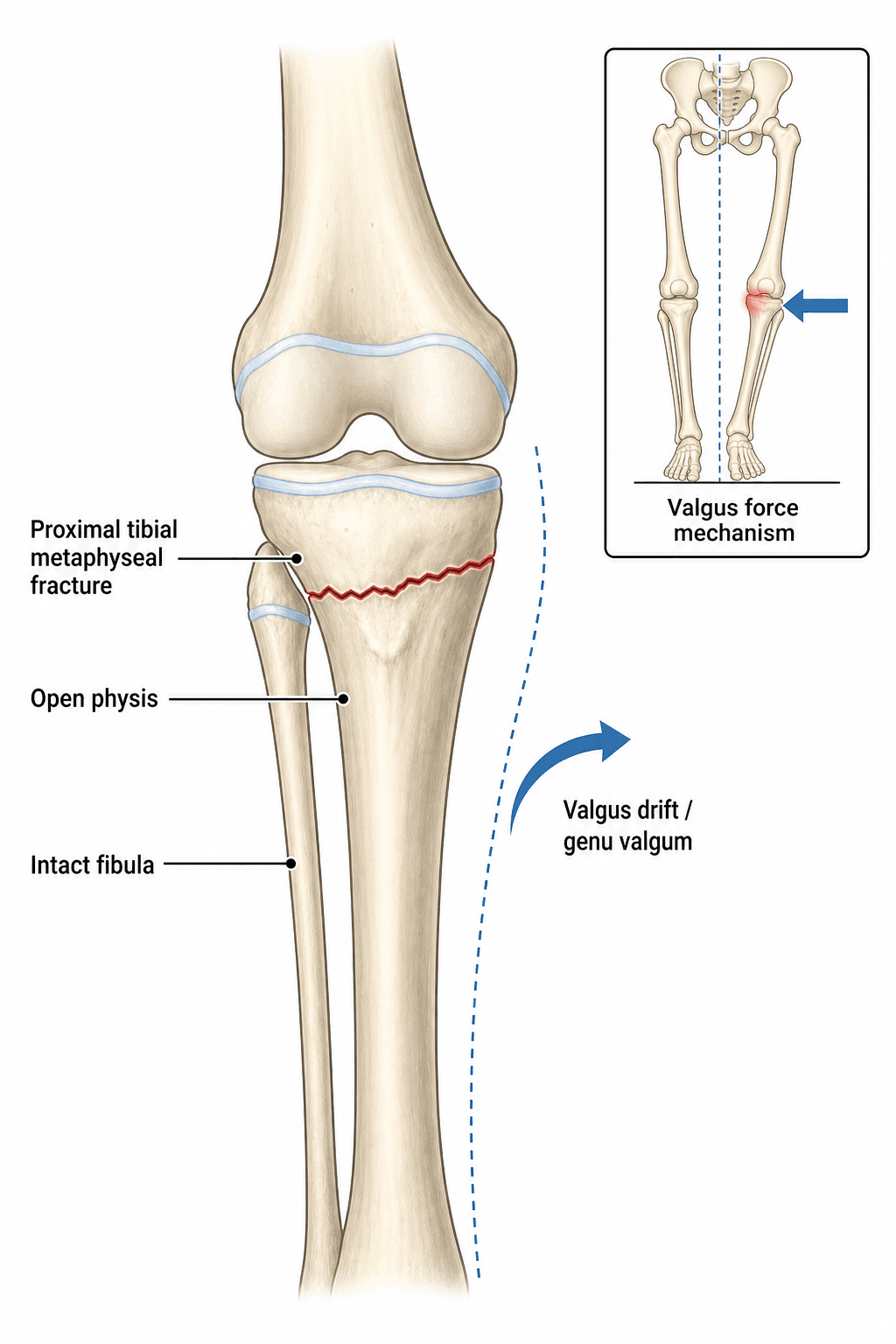
Proximal Tibial Metaphyseal Fracture | Post-Traumatic Valgus Deformity | Paediatric
- Proximal tibial metaphyseal fracture in children 3-8 years carries a high risk of post-traumatic valgus deformity (originally Cozen 1953)
- Valgus typically appears 6-12 months after the fracture has united - parents and surgeons must be warned
- The valgus deformity is usually self-correcting with continued growth over 1-3 years
- Premature corrective osteotomy carries a high rate of recurrence due to ongoing asymmetric growth - DO NOT operate early
- Indications for surgery are persistent deformity beyond skeletal maturity or functional impairment
- “Cozen fracture = proximal tibial metaphyseal fracture + later valgus
- “Counsel parents at the time of the initial injury that a valgus deformity may appear even after a perfectly healed fracture
- “Most cases spontaneously remodel - observation and serial radiographs are the mainstay of treatment
- “If surgery is needed, hemi-epiphysiodesis (guided growth) is preferred before skeletal maturity; corrective osteotomy is reserved for mature patients
Cozen phenomenon = post-traumatic tibia valga after proximal tibial metaphyseal fracture in children, classically described by L. Cozen in 1953. The fracture itself is usually unremarkable, but a progressive valgus deformity appears months later.
Typically children aged 3-8 years (some series up to age 10), with a slight male predominance. The proximal tibial physis is highly active in this age group, contributing to asymmetric growth.
AVOID early corrective osteotomy. The valgus deformity is usually transient and corrects with growth. Premature surgery has a high recurrence rate (up to 50 percent) because the underlying growth asymmetry persists.
Warn parents from day 1 that the leg may develop a knock-knee appearance even after perfect healing. This pre-empts complaints and is medicolegally essential. Document the discussion.
- Typical Management
- Above-knee cast 4-6 weeks, then observe
- Key Pearl
- Warn parents about late valgus
- Pitfall
- Discharging without counselling
- Typical Management
- Closed reduction in slight varus, cast
- Key Pearl
- Slight over-correction may reduce late valgus
- Pitfall
- Leaving in valgus and accepting the result
- Typical Management
- Observe with serial clinical and radiographic review
- Key Pearl
- Most remodel within 2-3 years
- Pitfall
- Listing for corrective osteotomy too early
- Typical Management
- Hemi-epiphysiodesis if growth remaining, or corrective tibial osteotomy
- Key Pearl
- Address only when growth complete
- Pitfall
- Recurrence risk high if osteotomy done early
WAITAvoiding Premature Surgery
Hook:WAIT - the Cozen principle is patience. Premature osteotomy invites recurrence.
Overview and Epidemiology
The Cozen phenomenon is one of the most important and frequently missed concepts in paediatric trauma. A seemingly trivial metaphyseal fracture of the proximal tibia can, months later, produce a striking valgus deformity that alarms both parents and the treating surgeon. Understanding that this deformity is usually self-correcting is the difference between appropriate reassurance and inappropriate early surgery. Recurrence after early osteotomy is one of the most-cited pitfalls in paediatric orthopaedic textbooks.
- Valgus force on an extended knee: Classic mechanism described by Cozen
- Fall from a height: Landing on a planted foot with knee extended
- Bicycle / scooter injury: Twisting or abduction force
- Sports injury: Valgus blow during football, skiing, or playground falls
- MVC (passenger): Dashboard-type injury in older children
- Common injury: Proximal tibial metaphyseal fractures are among the most common paediatric lower-limb fractures
- Age range: Peak incidence 3-8 years, reported up to age 10
- Sex distribution: Slight male predominance reflects exposure to play and sport
- Resource setting: Reported worldwide; mechanism varies by environment (traffic in LMICs, sport in HICs)
- Typical Finding
- 3-8 years (peak)
- Range / Notes
- Most series: 2-10 years
- Typical Finding
- Male slight predominance (1.2-1.5:1)
- Range / Notes
- Reflects activity exposure
- Typical Finding
- Either side, no strong predominance
- Range / Notes
- Bilateral cases exceedingly rare
- Typical Finding
- Up to 50-90 percent in some series
- Range / Notes
- Lower in displaced fractures reduced anatomically
- Typical Finding
- Approximately 85-90 percent of valgus cases
- Range / Notes
- Remodelling may take 2-3 years
Pathophysiology
No single mechanism fully explains the Cozen phenomenon - multiple factors likely contribute. The most-cited theories are:
- Asymmetric growth stimulation (Cozen, 1953) - the fracture healing response hyperaemically stimulates the medial proximal tibial physis, producing relative medial overgrowth.
- Tibial tubercle apophysis overgrowth (Ogden) - the tibial tubercle is a continuation of the proximal tibial physis, and asymmetric apophyseal growth contributes to the valgus moment.
- Soft-tissue tethering (Skak) - interposed periosteum, pes anserinus tendons, or an intact fibula tethers the lateral side, allowing the medial side to grow unopposed.
- Salter-Harris V (crush) injury to the lateral physis - a sub-radiographic crush of the lateral physis slows lateral growth and produces asymmetric valgus.
In practice: more than one mechanism is likely operative in any given child. The implication is that growth disturbance may persist for years - a critical reason to defer corrective osteotomy.
- Mechanism
- Hyperaemia from fracture stimulates medial proximal tibial physis
- Supporting Evidence
- Original clinical series; consistent timing of valgus at 6-12 months
- Implication
- Predicts medial overgrowth is the driver
- Mechanism
- Overgrowth of lateral tibial tubercle apophysis
- Supporting Evidence
- Anatomic and radiographic studies of the apophysis
- Implication
- Valgus moment generated distal to the physis
- Mechanism
- Pes anserinus or periosteum tethers medial side; intact fibula acts as a strut
- Supporting Evidence
- Operative and anatomic observations
- Implication
- Release of tether (where feasible) may help
- Mechanism
- Sub-radiographic injury to lateral physis slows lateral growth
- Supporting Evidence
- MRI studies show lateral physeal signal change in some cases
- Implication
- Undetected at initial injury; valgus emerges with growth
Time course: Valgus usually appears 6-12 months after injury, peaks around 12-18 months, and then remodels
Growth dependence: As long as the proximal physis is open and the child has significant growth remaining, asymmetric growth can re-equilibrate
Heel of the curve: Skeletal immaturity is the best friend of the patient with Cozen valgus
Biology wins: Most remodels in 2-3 years without intervention
Persistent asymmetry: The growth disturbance causing the valgus persists for years
Recurrence rate: Up to 50 percent of early tibial osteotomies recur
Double deformity risk: A child with a recurrence may end up with both an osteotomy scar and a worse deformity than the original
Surgical scarring: Each osteotomy adds scar, infection risk, and stiffness to a problem that nature was correcting
VALGUSMechanism of Late Valgus
Hook:Cozen VALGUS - even an undisplaced fracture can drive the knee into knock-knee months later.
Classification and Types
Classification of the Acute Fracture
- Description
- Compression of medial or lateral metaphyseal cortex
- Risk of Late Valgus
- Low
- Initial Treatment
- Cast 3-4 weeks, observe
- Description
- Tibial cortex disrupted laterally, medial cortex and periosteum intact, angulated into valgus
- Risk of Late Valgus
- Moderate-high
- Initial Treatment
- Closed reduction in slight varus, cast
- Description
- Both cortices disrupted, often fibula intact or also fractured
- Risk of Late Valgus
- Moderate
- Initial Treatment
- Anatomic reduction, cast
- Description
- Translation, overlap, or rotation
- Risk of Late Valgus
- Lower if anatomically reduced
- Initial Treatment
- Closed or open reduction, possible internal fixation
The risk of post-traumatic valgus is paradoxically higher in the less-displaced or greenstick variants - this is a recurring exam point.
Clinical Assessment
- Mechanism: Valgus force vs axial load vs twist
- Energy: Low-energy (playground) vs high-energy (fall, MVC)
- Inability to bear weight: Usually present acutely
- Knee pain and swelling: May dominate the presenting complaint
- Prior injury or deformity: Always document pre-injury alignment if known
- Inspection: Bruising, swelling, angular deformity, open wound
- Palpation: Localised metaphyseal tenderness, not joint-line tenderness
- Neurovascular: Document distal pulses, capillary refill, sensation, motor (especially peroneal nerve)
- Compartment assessment: Serial review for the first 24-48 hours, especially after casting
- Knee ligaments: Difficult to assess acutely; examine under anaesthesia if reduction required
Proximal tibial fractures in children can produce a tibial compartment syndrome that is easily missed in a distressed, non-cooperating child. Always:
- Re-examine at 12-24 hours after cast application
- Split the cast if there is any concern about swelling
- Admit for observation in children with high-energy mechanisms
- Treat the three As - Analgesia escalation, Anxiety, Agitation (the 3 As of missed compartment syndrome in children) as a red flag
- How to Perform
- Patient standing, knees extended, goniometer over patella to tibial tubercle
- Normal Value
- Mild valgus (5-7 degrees) under age 7 is physiological
- Significance
- Valgus greater than 10 degrees or asymmetric warrants concern
- How to Perform
- Standing with knees / ankles touching
- Normal Value
- Age-dependent: 0-2 cm under age 8
- Significance
- Tracks valgus progression and resolution
- How to Perform
- Plumb line from anterosuperior iliac spine on AP long-leg film
- Normal Value
- Should pass through centre of knee
- Significance
- Most reliable measure of deformity
- How to Perform
- Measure on AP long-leg film
- Normal Value
- LDFA ~87, MPTA ~87
- Significance
- Localises deformity to femur or tibia
Always compare to the contralateral side. Children have a wide range of physiological valgus (up to 7 degrees between ages 3-6). The most useful exam finding is asymmetry between the injured and uninjured sides. A 10 degree valgus on the injured side with a 5 degree valgus on the other side is more significant than a 7 degree valgus bilaterally.
Investigations
Imaging Protocol
Views: AP and lateral of the tibia (include knee and ankle), plus AP pelvis-to-ankle long-leg film in older children for deformity assessment
Acute role: Confirm fracture, displacement, angulation, fibular involvement
Follow-up role: Measure tibio-femoral angle, mechanical axis, MPTA, LDFA
Reason: Confirm union, document any early deformity, and provide a baseline for the 6-month review
Look for: Early tibial asymmetry, physeal widening, tubercle overgrowth
Indication: Document the deformity quantitatively, calculate mechanical axis deviation
Frequency: Every 6 months until resolution or until a clear plateau is reached
Indication: Assess for occult lateral physeal bar or Salter-Harris V injury if deformity is severe or progressive
Modality: Coronal T1 and gradient echo / PD fat-sat sequences through the physis
Limits: Sedation often required in young children
Indication: Pre-operative planning for complex or recurrent deformity
Role: Defines bony anatomy for osteotomy design (closing wedge, opening wedge, dome)
Plain radiographs are the cornerstone. The diagnosis of Cozen phenomenon is clinical-radiographic, not MRI-dependent. Reserve advanced imaging for cases that progress unexpectedly or fail to remodel. Long-leg standing films are the gold standard for measuring mechanical axis and tracking deformity in the growing child.
- Onset
- 6-12 months after proximal metaphyseal fracture
- Discriminating Feature
- History of preceding fracture, asymmetric valgus
- Key Test / Imaging
- Long-leg standing film, MRI if severe
- Onset
- Insidious onset, no preceding fracture
- Discriminating Feature
- Varus then progressive valgus; characteristic medial tibial epiphyseal changes
- Key Test / Imaging
- Langenskiold staging on AP knee film
- Onset
- Symmetric, peaks at 3-4 years, then resolves
- Discriminating Feature
- No preceding trauma, no asymmetric findings
- Key Test / Imaging
- Observation, no imaging required unless asymmetric
- Onset
- Months to years after physeal injury
- Discriminating Feature
- Progressive deformity, may be multiplanar
- Key Test / Imaging
- MRI confirms bar; maps location and size
- Onset
- Gradual deformity without preceding trauma
- Discriminating Feature
- Palpable mass, characteristic imaging appearance
- Key Test / Imaging
- Radiographs, MRI for soft-tissue variants
- Onset
- Bilateral, gradual, other signs of metabolic disease
- Discriminating Feature
- Widened physis, cupped metaphyses, low phosphate / low vitamin D
- Key Test / Imaging
- Bone profile, wrist and knee films, endocrinology workup
Management Algorithm
Management of the Acute Fracture
Goal: Achieve union in acceptable alignment and counsel the family about the natural history
Acute Treatment Protocol
Assessment: Clinical exam, neurovascular status, pain control, two-view radiographs of tibia including knee and ankle
Tetanus and antibiotic prophylaxis if open fracture
Counselling at first visit: Explain that a knock-knee appearance may develop months later, but it usually self-corrects - this is the most important single conversation of the episode
Cast: Above-knee cast, knee in slight flexion, ankle at neutral; moulded to hold the fracture
Reduction: If greenstick in valgus, gently complete the fracture and reduce in slight varus to lower the late valgus risk
Cast splitting: If any concern about swelling, split the cast and reapply after swelling settles
Cast removal: When clinical and radiographic union is achieved, typically 4-6 weeks in this age group
Review radiographs: Confirm union, document alignment, provide a baseline for future comparison
Remobilisation: Encourage weight-bearing and gradual return to activity
Clinical review: 3, 6, and 12 months post-injury
Radiographic review: Standing long-leg film at 6 months and 12 months, or sooner if deformity becomes obvious
Document and reassure: Note any emerging valgus; counsel that it usually remodels
For greenstick fractures angulated into valgus, many paediatric orthopaedic surgeons complete the fracture (reverse the intact cortex) and reduce the tibia in slight varus. This is thought to lower the rate of post-traumatic valgus by allowing more uniform physeal stimulation. Document the reduction manoeuvre clearly.
Complications
- Incidence
- Up to 50-90 percent in some series (variable severity)
- Risk Factors
- Younger age (3-8), greenstick in valgus, undisplaced fracture
- Management
- Observe; surgical correction only if persistent beyond maturity
- Incidence
- Up to 50 percent if osteotomy done before skeletal maturity
- Risk Factors
- Premature surgery with persistent growth asymmetry
- Management
- Re-osteotomy after maturity, hemi-epiphysiodesis if growth remains
- Incidence
- Less than 1 percent, but catastrophic if missed
- Risk Factors
- High-energy mechanism, tight circumferential cast, delayed presentation
- Management
- Split cast, urgent fasciotomy if suspected
- Incidence
- Rare, usually neurapraxia
- Risk Factors
- High-energy injury, displaced fracture, surgical exploration
- Management
- Observation, foot splint, nerve conduction studies if persistent
- Incidence
- Uncommon, often subclinical initially
- Risk Factors
- Salter-Harris III-V injury, missed at initial presentation
- Management
- MRI for diagnosis, bar excision if greater than 50 percent of physis and significant growth remains
- Incidence
- Mild, rarely clinically significant
- Risk Factors
- Asymmetric growth stimulation, physeal injury
- Management
- Observe; epiphysiodesis of the contralateral side if clinically significant at maturity
- Incidence
- Rare in this age group
- Risk Factors
- High-energy mechanism, knee dislocation equivalent
- Management
- Examine under anaesthesia, MRI if any suspicion
Pillar 1: Counsel at presentation. Every family should leave the first visit understanding that a knock-knee may develop and that the appropriate response is observation, not surgery.
Pillar 2: Document the conversation. Write a brief clinic note that the family was counselled about the Cozen phenomenon, the natural history, and the rationale for observation. This protects the surgeon, the family, and the child.
If you skip counselling, you will be the surgeon who is asked to "fix" a valgus that was always going to correct, and you may end up doing an osteotomy that then recurs.
Outcomes and Prognosis
- When Used
- Skeletally immature, asymptomatic valgus
- Expected Outcome
- 85-90 percent spontaneous correction over 2-3 years
- Long-term Function
- Excellent: normal knee, normal gait
- When Used
- Immature child with persistent valgus, growth remaining
- Expected Outcome
- Gradual correction over 12-18 months, plate removed at neutral
- Long-term Function
- Good; mild rebound possible if removed early
- When Used
- Mature patient with persistent valgus
- Expected Outcome
- Reliable correction, low recurrence if growth complete
- Long-term Function
- Good; risk of stiffness, hardware irritation
- When Used
- Inappropriate but historically common
- Expected Outcome
- Up to 50 percent recurrence, sometimes worse than original
- Long-term Function
- Variable; multiple surgeries often needed
Favourable prognostic factors:
- Younger age with substantial growth remaining
- Mild to moderate initial valgus (under 10 degrees tibio-femoral angle)
- Improving mechanical axis on serial films
- Asymptomatic child with normal function
Unfavourable prognostic factors:
- Age greater than 10 years at injury (less remodelling potential)
- Persistent or progressive valgus on serial films
- Symptomatic deformity (pain, gait abnormality)
- Skeletal maturity reached without correction
Guidelines, Registries & Global Practice
- Paediatric tibial fractures are among the most common lower-limb fractures in children worldwide, with peak incidence in the 3-10 year age group
- Proximal metaphyseal involvement is reported from every region where paediatric imaging is available
- Mechanism varies by setting: low-energy falls and sport in HICs, higher-energy traffic-related and fall-from-height mechanisms in LMICs
- The Cozen phenomenon is described in North American, European, Asian, African, and Australasian series - it is a universal paediatric orthopaedic entity
- High-resource settings: routine long-leg standing films at follow-up, MRI available for atypical cases, 8-Plate and external fixator systems for guided growth
- Limited-resource settings: clinical measurement of intermalleolar / intercondylar distance, plain radiographs alone, conventional staples or screw hemi-epiphysiodesis
- Universal principle: the appropriate response is observation and counselling regardless of resource - the biology is the same in every setting
- Surgery: corrective osteotomy is concentrated in tertiary paediatric centres; outcome data is more abundant from these centres
- Diagnosis emphasis
- Clinical-radiographic; long-leg standing film is the gold standard for measuring mechanical axis
- Acute treatment
- Cast immobilisation 4-6 weeks; counsel family about Cozen phenomenon at presentation
- Surgery / reconstruction
- Hemi-epiphysiodesis in the immature child with persistent deformity; osteotomy only at maturity
- Diagnosis emphasis
- Clinical; AP and lateral of tibia acutely, long-leg film at follow-up
- Acute treatment
- Cast, ensure anatomic or slight-varus reduction in greenstick fractures
- Surgery / reconstruction
- Reserved for symptomatic persistent deformity at or near maturity
- Diagnosis emphasis
- Distinguish Cozen from Blount, physiological valgus, and physeal bar
- Acute treatment
- Standard cast; emphasise parental counselling and serial review
- Surgery / reconstruction
- Guided growth preferred over osteotomy in skeletally immature children
- Diagnosis emphasis
- Resource-adapted: clinical and plain radiographic assessment in most settings
- Acute treatment
- Cast immobilisation, follow-up at 3, 6, and 12 months
- Surgery / reconstruction
- Hemi-epiphysiodesis (8-Plate, staples) or osteotomy depending on maturity and resources
There is no dedicated fracture or deformity registry for the Cozen phenomenon specifically. Evidence comes from case series published by individual paediatric centres (Cozen, Skak, Ogden, Green, Tuten, Robert) and from textbook synthesis (Tachdjian, Lovell and Winter, Rockwood and Wilkins). The consistency of the message across decades and continents is striking: observe, counsel, and avoid premature osteotomy. Where uncertainty exists, it is in the relative contribution of the four competing mechanisms - not in the management principle.
Record in every proximal tibial metaphyseal fracture seen acutely:
- Mechanism of injury and energy
- Initial tibio-femoral angle or mechanical axis if measurable
- Cast type, moulding, and any reduction manoeuvre
- Family counselled about the Cozen phenomenon and the natural history of late valgus
- Follow-up plan at 3, 6, and 12 months (and beyond if valgus appears)
A missed Cozen discussion is a recurring source of complaints and medicolegal claims in paediatric orthopaedic practice worldwide. The cost of ten minutes of counselling is a fraction of the cost of an unnecessary osteotomy.
Controversies & Areas of Uncertainty
Four theories (Cozen, Ogden, Skak, Salter-Harris V) are all supported by some evidence. It is likely that more than one mechanism operates in any given child. The relative contribution of each remains undetermined and may explain why no single preventive measure (over-reduction, fibular osteotomy, pes release) has consistently eliminated the valgus.
Some surgeons advocate completing greenstick fractures and reducing in slight varus to lower the late valgus rate. Evidence is mixed; the manoeuvre is not universally practised, and anatomic or near-anatomic reduction is also acceptable. The principle is sound but the magnitude of effect is uncertain.
There is no absolute degree of valgus that mandates surgery. The decision integrates magnitude, trend on serial films, skeletal maturity, and functional impact. Some surgeons offer hemi-epiphysiodesis at 10 degrees of valgus in a 10-year-old with 2 years of growth remaining; others watch a similar deformity in a 7-year-old and expect remodelling.
Most cases resolve. Whether a small subset of patients with persistent valgus into adulthood develop premature lateral compartment osteoarthritis is plausible but not well-quantified. Adult deformity correction is sometimes offered for this reason, but the natural history beyond skeletal maturity is not rigorously documented.
MCQ Practice Points
Q: What is a Cozen fracture? A: A proximal tibial metaphyseal fracture in a young child (typically 3-8 years) that is followed by progressive valgus deformity of the tibia 6-12 months after the fracture has united. The fracture itself is often unremarkable, but the late valgus can be striking.
Q: What is the most likely mechanism of the post-traumatic valgus? A: It is probably multifactorial. The leading theories are (1) asymmetric stimulation of the proximal tibial physis by fracture hyperaemia (Cozen), (2) overgrowth of the lateral tibial tubercle apophysis (Ogden), (3) soft-tissue tethering on the medial side by pes anserinus, periosteum, or an intact fibula (Skak), and (4) sub-radiographic Salter-Harris V crush of the lateral physis. In practice, more than one mechanism is likely operative.
Q: What is the appropriate management of post-traumatic tibia valga in a 5-year-old? A: Observation with serial clinical and radiographic review. Most cases spontaneously remodel over 2-3 years. Corrective osteotomy is reserved for persistent deformity at or near skeletal maturity because early osteotomy carries a recurrence rate of up to 50 percent.
Q: How do you distinguish Cozen phenomenon from Blount disease? A: Cozen follows a proximal tibial metaphyseal fracture and appears 6-12 months later; Blount is insidious, with no preceding fracture, and shows characteristic changes in the medial proximal tibial epiphysis and metaphysis (Langenskiold staging). Physiological valgus is symmetric, peaks at 3-4 years, and resolves by age 7.
Q: When is corrective surgery indicated for Cozen valgus? A: When the deformity persists beyond skeletal maturity, is symptomatic (pain, gait abnormality, functional limitation), or is severe and progressive (greater than 15-20 degrees of tibio-femoral valgus). In a skeletally immature child, hemi-epiphysiodesis (guided growth) is the preferred temporising measure; definitive osteotomy is deferred.
Q: What is the most important complication of premature corrective osteotomy for Cozen valgus? A: Recurrence of the valgus deformity in up to 50 percent of cases, because the underlying growth disturbance persists until skeletal maturity. This can produce a worse deformity than the original, with the additional burden of surgical scarring, stiffness, and infection risk from the unnecessary operation.
TALKInitial Counselling Points
Hook:TALK to every family at the first visit - the parents of a child with a Cozen fracture must understand the natural history.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 5-year-old boy sustained a minimally displaced proximal tibial metaphyseal fracture 8 months ago after a fall from a slide. The fracture united uneventfully, but his mother brings him back concerned about a progressive knock-knee deformity on the injured side. Examination shows 12 degrees of valgus on the injured side and 5 degrees on the contralateral side. The child is asymptomatic and active. What is your diagnosis, and how would you manage this?”
“A 4-year-old girl has an undisplaced buckle fracture of the proximal tibial metaphyseal region after a low-energy fall. You are about to apply an above-knee cast in the emergency department. The mother is anxious and asks whether her daughter will be 'normal again'. Outline what you would say, what consent you would obtain, and what your follow-up plan would be.”
Definition & Scope
- Cozen fracture = proximal tibial metaphyseal fracture in a child (peak age 3-8) followed by late valgus deformity
- Originally described by L. Cozen in 1953
- Late valgus appears 6-12 months after union, often despite a well-reduced fracture
- Affects up to 50-90 percent of children in this age group, with variable severity
Mechanism Theories
- Cozen - asymmetric physeal stimulation from fracture hyperaemia (medial overgrowth)
- Ogden - lateral tibial tubercle apophysis overgrowth contributes to valgus moment
- Skak - soft-tissue tethering (pes anserinus, periosteum, intact fibula) on the medial side
- Salter-Harris V - sub-radiographic crush of the lateral physis slows lateral growth
Diagnosis & Imaging
- Acute diagnosis is clinical and radiographic - AP and lateral tibia including knee and ankle
- Long-leg standing film is the gold standard for measuring mechanical axis and tracking deformity
- MRI reserved for atypical or progressive cases to assess the physis for a bar
- Differential: Blount disease, physiological valgus, physeal bar, rickets, osteochondroma
Acute Management
- Cast immobilisation 4-6 weeks; moulded to hold the fracture
- Consider completing greenstick fractures and reducing in slight varus
- Split the cast if there is any concern about swelling - watch for compartment syndrome
- Counselling at presentation is the single most important intervention
Late Valgus Management
- Observation is the default in the skeletally immature child
- Document and counsel the family; serial clinical and radiographic review every 6 months
- Most cases spontaneously remodel over 2-3 years (approximately 85-90 percent)
- Hemi-epiphysiodesis if growth remains and deformity persists; osteotomy only at maturity
Pitfalls & Pearls
- Do NOT offer a corrective osteotomy in the immature child - recurrence rate up to 50 percent
- Document the counselling about Cozen phenomenon at the first visit
- Compare the injured and uninjured sides; asymmetry is more significant than absolute valgus
- Re-examine at 12-24 hours for compartment syndrome - the three As (Analgesia, Anxiety, Agitation) are red flags in children
Evidence Base and Key Trials
Fracture of the proximal portion of the tibia in children followed by valgus deformity
- Original description of post-traumatic valgus deformity following proximal tibial metaphyseal fracture in children
- Cozen proposed asymmetric physeal stimulation from fracture hyperaemia as the mechanism
- Documented a series of children in whom valgus appeared 6-12 months after the fracture
- Cautioned against premature corrective osteotomy, recognising the natural remodelling potential
Valgus deformity following proximal tibial metaphyseal fracture in children
- Retrospective series documenting late valgus after proximal metaphyseal fractures in children
- Proposed soft-tissue tethering (intact fibula, pes anserinus, interposed periosteum) as a contributing mechanism
- Most cases remodelled spontaneously, supporting a conservative approach
- Stressed the importance of distinguishing true growth disturbance from soft-tissue imbalance
Posttraumatic tibia valga in children. A long-term follow-up note
- Long-term follow-up of children with post-traumatic proximal tibial valgus
- Confirmed Ogden's hypothesis that the tibial tubercle apophysis contributes to the valgus moment
- Demonstrated that most cases spontaneously corrected with continued growth
- Highlighted the dangers of early osteotomy and the high rate of recurrence
Tibial valgus deformity following proximal metaphyseal fracture in childhood
- Series of children with proximal tibial metaphyseal fractures followed for valgus deformity
- Confirmed that even undisplaced or minimally displaced fractures can produce striking late valgus
- Most cases resolved with growth; severe persistent deformity was uncommon
- Recommended serial clinical and radiographic follow-up rather than early surgery
Cozen's deformity: resolved by guided growth
- Case series of children with persistent post-traumatic proximal tibial valgus treated with temporary hemi-epiphysiodesis (guided growth)
- Demonstrated reliable correction of Cozen deformity without recourse to corrective osteotomy
- Supported guided growth as a less invasive alternative to osteotomy in skeletally immature children with persistent valgus
- Reinforced the principle of deferring definitive osteotomy until skeletal maturity whenever growth remains