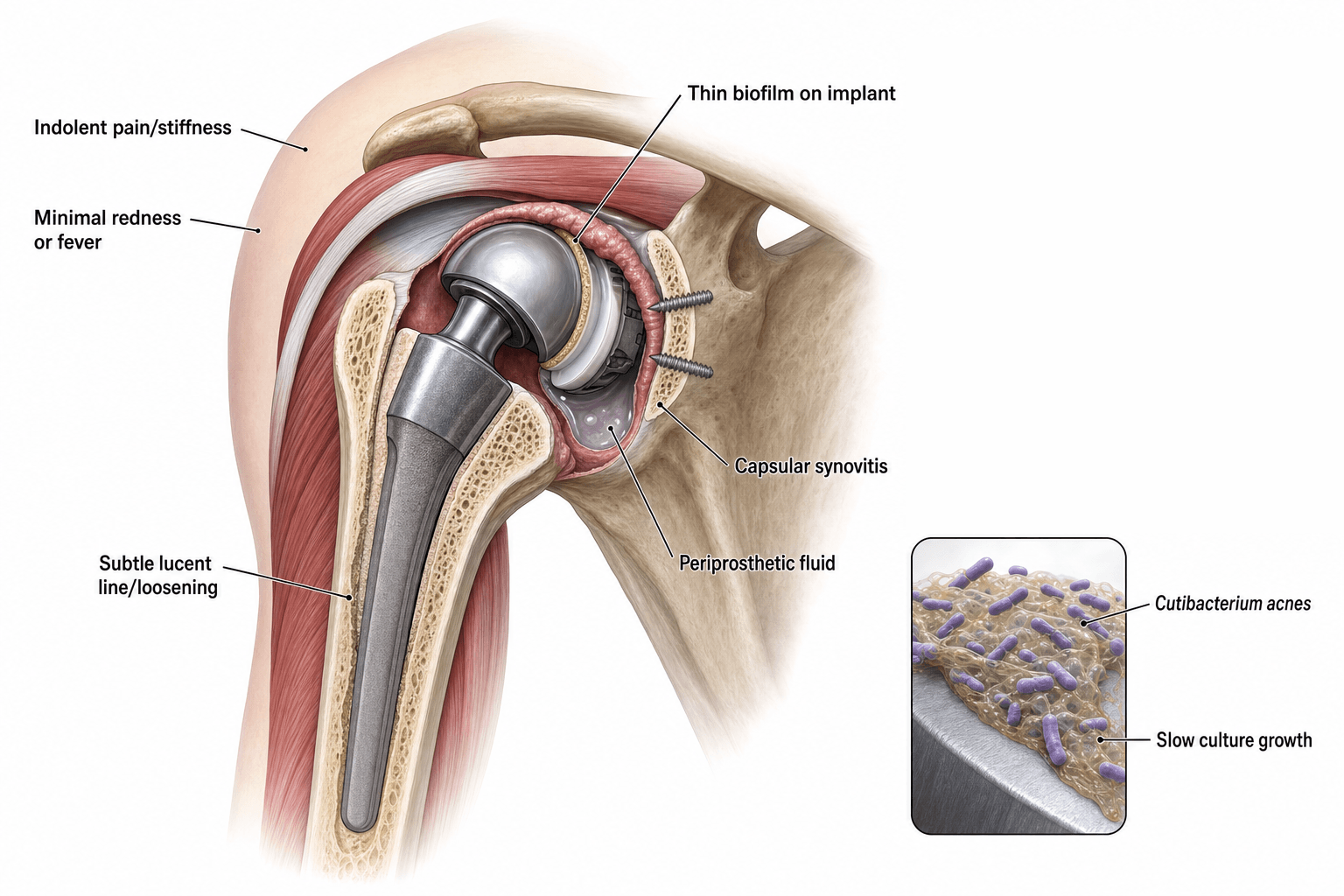
Indolent Periprosthetic Infection | Low-Virulence Organism | Diagnostic Challenge
- C. acnes is the most common organism in shoulder PJI, overtaking Staphylococcus species
- Normal CRP, ESR, and WCC do NOT exclude C. acnes PJI
- Culture all tissue samples for a minimum of 14-21 days in anaerobic conditions
- Male patients predominate (hair follicles of upper trunk and shoulder)
- Sonication of explanted components increases culture yield
- “Think C. acnes in any painful shoulder arthroplasty with normal inflammatory markers
- “Prolonged anaerobic culture (14-21 days) is mandatory, not optional
- “Male sex + shoulder arthroplasty + unexplained pain = culture for C. acnes
- “Sonication of explanted prosthesis significantly improves detection
CRP and ESR are frequently normal or only mildly elevated in C. acnes PJI. Do not rely on serum inflammatory markers to exclude the diagnosis. A high index of suspicion is essential in any painful shoulder arthroplasty.
Standard 5-day cultures miss the majority of C. acnes infections. All tissue and fluid samples from revision shoulder surgery must be cultured for 14-21 days under anaerobic conditions to detect this slow-growing organism.
C. acnes preferentially colonises the hair follicles and sebaceous glands of the upper trunk, shoulder, and proximal arm. Males are affected significantly more than females, likely due to greater pilosebaceous density in this region.
Sonication of explanted prosthetic components disrupts the biofilm and significantly increases culture yield for C. acnes compared with periprosthetic tissue culture alone. Request it whenever components are removed.
- Diagnosis
- Joint aspirate + prolonged culture (14-21 d)
- Treatment
- Revision surgery + targeted antibiotics
- Key Pearl
- Normal bloods does NOT exclude C. acnes
- Diagnosis
- Multiple tissue samples + sonication
- Treatment
- Antibiotics alone or with component exchange
- Key Pearl
- Always culture for C. acnes in revision cases
- Diagnosis
- Aspiration, CRP, blood cultures
- Treatment
- DAIR + prolonged antibiotics (6-8 weeks)
- Key Pearl
- Only scenario where DAIR is reasonable
CULTUREDiagnosing C. acnes Shoulder PJI
Hook:CULTURE for 21 days — because C. acnes will NOT grow on routine 5-day plates!
SHOULDERRisk Factors for C. acnes PJI
Hook:SHOULDER infections are different — think C. acnes when the presentation is indolent!
Overview and Epidemiology
Cutibacterium acnes (formerly Propionibacterium acnes) is the most common causative organism in shoulder periprosthetic joint infection, responsible for approximately 30-60 percent of all shoulder PJIs. Its indolent, low-virulence nature means it frequently presents with normal inflammatory markers and no systemic features, making it a diagnostic trap. Examiners test this topic because it illustrates the principle that "normal bloods does not exclude infection."
- Gram-positive anaerobic bacillus (formerly Propionibacterium acnes)
- Slow-growing: requires 14-21 days of anaerobic culture
- Biofilm-forming: adheres to implant surfaces, resistant to host immunity
- Low virulence: minimal local inflammation, no systemic response typically
- Skin commensal: deep hair follicles and sebaceous glands of upper trunk
- Male predominance: males affected more than females (greater pilosebaceous density)
- Most common shoulder PJI organism: overtakes Staphylococcus aureus and coagulase-negative staphylococci
- Increasing recognition: improved culture techniques and longer incubation have revealed true prevalence
- Risk factors: male sex, prior shoulder surgery, haematoma, prolonged operative time
Pathophysiology
C. acnes is a skin commensal that colonises the deep hair follicles and sebaceous glands of the upper back, shoulder, and proximal arm. During shoulder surgery, the organism can be inoculated into the surgical field despite standard skin preparation, because it resides deep within pilosebaceous units that antiseptic solutions may not fully penetrate. Once in contact with an implant surface, C. acnes forms a biofilm — a structured extracellular polymeric matrix that protects bacteria from both the host immune response and antibiotic penetration. This biofilm renders the organism resistant to conventional antibiotic courses and is the fundamental reason why surgical intervention (with component removal or exchange) is usually required for eradication.
- C. acnes PJI
- Indolent, low-grade, months to years
- Staphylococcal PJI
- Acute, often fulminant, days to weeks
- C. acnes PJI
- Often normal
- Staphylococcal PJI
- Usually elevated
- C. acnes PJI
- Absent (no fever, no wound breakdown)
- Staphylococcal PJI
- Fever, wound erythema, drainage common
- C. acnes PJI
- 14-21 days anaerobic incubation
- Staphylococcal PJI
- Grows within 48-72 hours on standard media
- C. acnes PJI
- Prominent, thin biofilm on implant
- Staphylococcal PJI
- Thick biofilm (S. aureus) or slime layer (CoNS)
- C. acnes PJI
- Strong male predominance
- Staphylococcal PJI
- No sex predilection
Unique anatomy: The shoulder region has the highest density of pilosebaceous units harboring C. acnes on the human body. Standard chlorhexidine or povidone-iodine skin preparation does not fully eradicate organisms from deep follicles. Intra-operative contamination rates of 15-30 percent have been reported from tissue cultures taken during primary shoulder arthroplasty.
Protected state: Within biofilm, C. acnes exists in a metabolically quiescent state that is resistant to cell-wall active antibiotics. Minimum biofilm eradication concentration (MBEC) can be 100-1000 times greater than planktonic minimum inhibitory concentration (MIC). This is why antibiotics alone rarely cure established implant-related C. acnes infection.
Because the organism lives deep in pilosebaceous units that surface antiseptic cannot reach, contamination is the problem to attack before it becomes an infection - and the examinable point is what actually reduces it:
- Benzoyl peroxide (topical, applied for several days pre-operatively) is the single most effective measure - it penetrates the follicle and significantly lowers the C. acnes skin and dermal burden; chlorhexidine and povidone-iodine alone do not eradicate deep follicular organisms.
- Standard chlorhexidine/alcohol skin prep is necessary but insufficient - even after a textbook prep, dermal punch-biopsy cultures remain positive in a substantial proportion of patients, and the dermis (not the surface) is the reservoir.
- Hydrogen peroxide applied to the skin/dermis after the incision has been shown to reduce C. acnes culture positivity from the wound.
- Standard prophylactic cefazolin covers C. acnes (it is penicillin/cephalosporin-sensitive); some units add clindamycin or vancomycin in high-risk cases, though the evidence for the addition is limited.
- Male sex cannot be modified, so the modifiable levers are the skin/dermal antiseptic protocol, meticulous technique and minimising operative time and haematoma.
The trap: assuming a normal-looking surgical prep has sterilised the field - the dermal reservoir means the field is never truly sterile for C. acnes, which is why these adjuncts and a low threshold for intra-operative culture both matter.
Classification and Types
Classification by Timing (Adapted from Tsukayama)
- Timing
- Within 3 months of index surgery
- Presentation
- Acute wound inflammation, pain, possible drainage
- Treatment Approach
- DAIR + targeted antibiotics (if stable implant)
- Timing
- Greater than 3 months, indolent course
- Presentation
- Gradually worsening pain, loosening, normal CRP
- Treatment Approach
- One-stage or two-stage revision + antibiotics
- Timing
- Sudden onset in previously well-functioning arthroplasty
- Presentation
- Acute pain, systemic features possible
- Treatment Approach
- DAIR if less than 3 weeks of symptoms + stable implant
- Timing
- Found during revision for presumed aseptic loosening
- Presentation
- No pre-operative suspicion of infection
- Treatment Approach
- Targeted antibiotics +/- staged revision based on findings
The "unexpected positive" category is particularly relevant to C. acnes, as it is frequently identified only after prolonged incubation of tissue samples sent during revision for presumed aseptic failure.
Clinical Assessment
- Pain: Persistent or worsening pain after shoulder arthroplasty (most common presenting symptom)
- Timing: May present months to years after index surgery
- Stiffness: Progressive loss of range of motion
- No wound problems: Typically no erythema, warmth, or drainage
- No systemic features: Afebrile, no rigors, no malaise
- Inspect: Well-healed wounds, no erythema or sinus
- Palpate: May have mild tenderness around implant, often unremarkable
- Range of motion: Decreased, often with pain at end ranges
- Instability: Component loosening may cause subtle instability
- Neurovascular: Usually intact, no specific deficit
The presentation of C. acnes shoulder PJI is virtually indistinguishable from aseptic loosening on clinical and basic radiographic assessment. Both present with gradual-onset pain, stiffness, and possible radiographic lucency. The distinction depends entirely on microbiological culture (prolonged anaerobic incubation). Always send tissue for 14-21 day culture at every revision shoulder arthroplasty, regardless of pre-operative suspicion.
- CRP/ESR
- Normal in many cases
- Key Discriminator
- Indolent pain, male, normal bloods, loosening
- Definitive Test
- Prolonged tissue culture (14-21 d) + sonication
- CRP/ESR
- Normal
- Key Discriminator
- Mechanical pain, lucency on X-ray, no infection
- Definitive Test
- Negative culture (must culture to exclude C. acnes)
- CRP/ESR
- Elevated
- Key Discriminator
- Acute presentation, wound changes, systemic features
- Definitive Test
- Standard culture (48-72 h), blood cultures
- CRP/ESR
- Normal
- Key Discriminator
- Weakness, inability to elevate arm, instability
- Definitive Test
- Ultrasound or MRI (gadolinium)
- CRP/ESR
- Normal or mildly elevated
- Key Discriminator
- Painless effusion, pseudotumour, metal-on-metal bearing
- Definitive Test
- Metal ion levels, MRI, histology
- CRP/ESR
- Normal
- Key Discriminator
- Episodes of dislocation or subluxation
- Definitive Test
- Stress radiographs, CT for component version
Always suspect C. acnes in:
- Any male patient with a painful shoulder arthroplasty and normal inflammatory markers
- Any revision shoulder arthroplasty — even if pre-operative workup is negative for infection
- Any "aseptic loosening" that progresses more rapidly than expected
- Persistent pain after arthroscopic or open shoulder surgery with implants in situ
Investigations
Investigation Protocol
CRP, ESR, FBC: Frequently normal in C. acnes PJI. Do NOT be reassured by normal values.
Interleukin-6: May be more sensitive than CRP for low-grade PJI but not universally available.
Procalcitonin: Not sensitive for low-virulence infections; not recommended for C. acnes screening.
Key point: Normal serum markers cannot exclude C. acnes shoulder PJI. They are useful if positive (supportive) but meaningless if negative.
Views: AP, axillary lateral, and scapular-Y of the shoulder
Look for: Radiolucent lines at bone-cement or bone-implant interface, component migration or subsidence, osteolysis, periosteal reaction (rare in C. acnes)
Clinical correlation: Radiographic loosening in C. acnes PJI is indistinguishable from aseptic loosening on X-ray alone.
Technique: Ultrasound-guided or fluoroscopic-guided aspiration preferable (dry tap common without imaging guidance)
Send for: Cell count and differential, gram stain, aerobic AND anaerobic culture (request 14-21 day incubation)
Synovial fluid WCC: Thresholds for shoulder are lower than hip/knee; greater than 1000-2000 cells/microlitre is considered suspicious
Alpha-defensin: Has shown promise for shoulder PJI diagnosis but sensitivity for C. acnes specifically is variable
CT scan: Assess component position, version, bone stock, and osteolysis pattern for revision planning
MRI (with gadolinium): May show periprosthetic fluid collection, synovitis, or abscess formation in low-grade PJI. Metal artefact reduction sequences are essential.
Nuclear medicine (PET-CT, labelled leukocyte scan): Limited evidence specific to C. acnes shoulder PJI; may be used in equivocal cases.
The single most important investigation is tissue culture with prolonged (14-21 day) anaerobic incubation. All other investigations (bloods, imaging, even aspiration) may be negative. At revision surgery, send a minimum of 5 tissue samples from different periprosthetic sites for prolonged culture. A single positive C. acnes culture in the right clinical context is considered significant.
- Specimen
- 5 or more tissue samples from different sites
- Duration
- 14-21 days anaerobic
- Sensitivity for C. acnes
- Moderate — dependent on sampling and technique
- Specimen
- Removed prosthesis placed in sterile container
- Duration
- 14-21 days anaerobic after sonication
- Sensitivity for C. acnes
- High — disrupts biofilm, increases yield significantly
- Specimen
- Synovial fluid aspirate
- Duration
- 14-21 days anaerobic
- Sensitivity for C. acnes
- Lower — dry taps common, biofilm not sampled
- Specimen
- Any specimen
- Duration
- 5 days (routine)
- Sensitivity for C. acnes
- POOR — misses the majority of C. acnes
Management Algorithm
Chronic C. acnes PJI (Greater than 3 Months or Indolent)
Goal: Eradicate infection with component exchange and targeted antibiotic therapy
Management Protocol
Workup: Aspiration with prolonged culture, CT for bone stock, plan for revision
Consent: Discuss one-stage vs two-stage options, functional outcomes, antibiotic duration
Templating: Prepare for both scenarios (bone loss may dictate approach intra-operatively)
Approach: Deltopectoral (extend prior incision)
Samples: Send minimum 5 tissue samples from different sites for 14-21 day anaerobic culture
Sonication: All explanted components sent for sonication
Debridement: Thorough irrigation and debridement of all infected tissue
Decision: One-stage (exchange at same operation) vs two-stage (spacer placement, delayed reimplantation)
Antibiotics: IV pathogen-directed therapy for 4-6 weeks based on culture sensitivities
C. acnes sensitivities: Usually sensitive to penicillin G, cephalosporins, clindamycin, vancomycin; often resistant to metronidazole
If two-stage: Antibiotic spacer in situ, monitor inflammatory markers (though may remain normal)
Re-aspire: Joint aspiration with culture before reimplantation to confirm eradication
Tissue samples again: Send multiple samples at reimplantation surgery
Oral suppression: Some protocols use prolonged oral suppressive antibiotics after reimplantation
One-stage exchange is increasingly favoured for C. acnes PJI when: the organism is known pre-operatively, bone stock is adequate, the patient is not immunocompromised, and thorough debridement can be achieved. Two-stage exchange remains the gold standard for: extensive bone loss, unclear organism, multi-organism infection, or significant soft tissue compromise. Current evidence suggests similar eradication rates for C. acnes with both approaches when appropriate antibiotic therapy is used.
CAPSManagement of C. acnes PJI
Hook:CAPS — Culture, Antibiotics, Prosthesis exchange, Sonication!
Antibiotic Management
- Route
- IV
- Duration
- 4-6 weeks
- Notes
- First-line if susceptible; check MIC
- Route
- IV
- Duration
- 4-6 weeks
- Notes
- Alternative if penicillin-susceptible but penicillin not tolerated
- Route
- IV
- Duration
- 4-6 weeks
- Notes
- For penicillin-allergic patients or resistant strains
- Route
- IV then oral
- Duration
- 4-6 weeks total
- Notes
- Good bone penetration; step-down to oral; check inducible resistance
- Route
- Oral
- Duration
- Added to primary agent
- Notes
- Biofilm penetration; ALWAYS use in combination (never monotherapy)
- Route
- Any
- Duration
- N/A
- Notes
- NOT effective against C. acnes — do not use
C. acnes is an anaerobe but is resistant to metronidazole — a classic exam trap. It is usually susceptible to penicillin, cephalosporins, clindamycin, and vancomycin. Rifampicin is used as a combination agent for its biofilm-penetrating properties, never as monotherapy (rapid resistance development).
Complications
- Incidence / Risk
- 5-20 percent after revision
- Risk Factors
- Inadequate debridement, retained biofilm, immunocompromise
- Management
- Repeat revision with aggressive debridement + antibiotics
- Incidence / Risk
- Common presentation of PJI
- Risk Factors
- Biofilm-mediated osteolysis, chronic inflammation
- Management
- Revision arthroplasty with component exchange
- Incidence / Risk
- Variable, may be extensive
- Risk Factors
- Chronic infection, osteolysis, multiple revisions
- Management
- Bone grafting, allograft, or reverse shoulder arthroplasty
- Incidence / Risk
- Common after revision surgery
- Risk Factors
- Multiple operations, capsular scarring, prolonged immobilisation
- Management
- Structured physiotherapy, manipulation under anaesthesia if needed
- Incidence / Risk
- Dependent on agent and duration
- Risk Factors
- Prolonged IV access, rifampicin hepatotoxicity, C. difficile
- Management
- Monitor LFTs, renal function, therapeutic drug levels
C. acnes PJI has a recurrence rate of approximately 5-20 percent after revision surgery, which is generally lower than more virulent organisms. However, recurrence may present late and with the same indolent pattern. Long-term clinical and microbiological surveillance is essential. Any recurrence of pain after revision should prompt repeat investigation with aspiration and prolonged culture.
Outcomes and Prognosis
- Eradication Rate
- 85-95 percent (C. acnes specific)
- Functional Outcome
- Good — single surgery, faster recovery
- Key Consideration
- Organism identified, adequate bone stock, thorough debridement
- Eradication Rate
- 85-95 percent
- Functional Outcome
- Good — but requires two surgeries
- Key Consideration
- Extensive bone loss, uncertain organism, immunocompromise
- Eradication Rate
- 60-80 percent
- Functional Outcome
- Good if successful — retains original components
- Key Consideration
- Only for acute infection (under 3 months) with stable implants
- Eradication Rate
- Variable, not curative
- Functional Outcome
- Palliative — suppresses but does not eradicate
- Key Consideration
- Unfit for surgery, minimal symptoms, patient preference
Favourable prognosis: C. acnes (low virulence), one-stage or two-stage revision with appropriate antibiotics, adequate bone stock, single organism, immunocompetent patient
Poor prognosis: Multi-organism infection, extensive bone loss requiring allograft, multiple prior revisions, immunocompromised patient, inadequate culture (organism not identified)
Key principle: C. acnes PJI has better outcomes than Staphylococcus aureus or fungal PJI when properly managed with surgical revision and targeted antibiotics.
Guidelines, Registries & Global Practice
- C. acnes is the most common organism in shoulder PJI worldwide, with prevalence estimates of 30-60 percent across North American, European, and Australasian series
- Male predominance is consistent across all geographic populations studied
- Intra-operative contamination rates of 15-30 percent during primary shoulder arthroplasty are reported in studies from multiple continents
- Recognition increasing globally as culture techniques (prolonged incubation, sonication) become standard
- Europe: Strong trend toward one-stage exchange for C. acnes PJI, supported by multicentre data from France, Germany, and Scandinavia
- North America: Two-stage exchange remains more commonly performed, though one-stage is gaining acceptance
- Australasia: Individualised approach based on organism, bone stock, and surgeon preference
- Universal principle: Prolonged anaerobic culture (14-21 days) and multiple tissue samples are mandatory regardless of region
- Culture Recommendation
- 14-21 day anaerobic culture; sonication recommended
- Surgical Approach
- Two-stage preferred; one-stage in selected cases
- Antibiotic Duration
- 4-6 weeks IV followed by oral suppression
- Culture Recommendation
- Prolonged culture mandatory for all revision shoulder cases
- Surgical Approach
- One-stage increasingly supported for C. acnes
- Antibiotic Duration
- Minimum 6 weeks pathogen-directed therapy
- Culture Recommendation
- Minimum 14 days anaerobic culture; sonication of explants
- Surgical Approach
- One-stage acceptable for known C. acnes with adequate bone stock
- Antibiotic Duration
- 4-6 weeks IV/oral; rifampicin combination recommended
- Culture Recommendation
- Prolonged culture + sonication standard of care
- Surgical Approach
- One- or two-stage based on individual case factors
- Antibiotic Duration
- 4-6 weeks targeted therapy + clinical monitoring
National joint registries (NJR UK, AOANJRR Australia, AJRR US) capture revision for infection but generally do not distinguish C. acnes from other organisms at the organism-specific level. The evidence base for C. acnes shoulder PJI is predominantly from specialist shoulder unit case series rather than registry data. This means clinical judgement and protocol-driven culture techniques remain more important than population-level data for individual patient management.
In every revision shoulder arthroplasty, regardless of pre-operative suspicion:
- Send a minimum of 5 tissue samples from different periprosthetic sites
- Request 14-21 day anaerobic culture (not standard 5-day)
- Sonicate any explanted components
- Do not dismiss C. acnes growth as contamination without clinical correlation
- Normal CRP and ESR do not exclude C. acnes PJI
These principles apply globally and are not resource-dependent — the culture duration request costs nothing additional.
Controversies & Areas of Uncertainty
Current evidence suggests comparable eradication rates for one-stage and two-stage revision in C. acnes PJI. One-stage avoids a second surgery and may offer faster functional recovery. Two-stage remains traditional for cases with extensive bone loss, uncertain microbiology, or soft tissue compromise. No high-quality RCT exists to definitively guide the choice.
Debate continues about whether a single positive C. acnes culture (of 5 or more samples) represents true infection or contamination. Most authorities now treat it as significant in the appropriate clinical context (male, shoulder, indolent pain), but the threshold for intervention varies between centres.
Optimal antibiotic duration is not established by RCT evidence. Protocols range from 4 weeks to greater than 12 weeks of combined IV and oral therapy. Some centres use prolonged oral suppression for 6-12 months in high-risk patients. The role of rifampicin combination therapy for C. acnes biofilm is extrapolated from Staphylococcus data.
The MSIS criteria were developed for hip and knee PJI and have poor sensitivity for shoulder infections. Proposed shoulder-specific thresholds (lower synovial WCC, lower neutrophil percentage) have not been universally validated. An international consensus on shoulder-specific PJI diagnostic criteria is still evolving.
MCQ Practice Points
Q: What is the mandatory minimum culture duration for suspected C. acnes shoulder PJI? A: 14-21 days under anaerobic conditions. Standard 5-day cultures miss the majority of C. acnes infections. This is the single most frequently tested fact about this organism.
Q: Can C. acnes PJI be excluded with normal CRP and ESR? A: No. CRP and ESR are frequently normal in C. acnes shoulder PJI. The diagnosis should be suspected clinically (male patient, shoulder arthroplasty, indolent pain) and confirmed by prolonged tissue culture. Normal bloods cannot exclude this infection.
Q: What is the antibiotic of choice for C. acnes PJI? A: Penicillin G (IV) or ceftriaxone/cefazolin if the organism is susceptible. Vancomycin for penicillin-allergic patients. Clindamycin is an alternative with good bone penetration for step-down therapy. Rifampicin is added as a combination agent for biofilm penetration. Metronidazole is NOT effective against C. acnes despite it being an anaerobe — this is a classic trap.
Q: When is DAIR appropriate for C. acnes shoulder PJI? A: Only in acute infection (within 3 months of index surgery or acute haematogenous with less than 3 weeks of symptoms) with stable, well-fixed components. For chronic C. acnes PJI, revision with component exchange (one-stage or two-stage) is required because biofilm on retained implants cannot be eradicated by antibiotics alone.
Q: What is the role of sonication in C. acnes PJI? A: Sonication disrupts the biofilm on explanted prosthetic components, releasing bacteria into the surrounding fluid for culture. It significantly increases the detection rate of C. acnes compared with periprosthetic tissue culture alone. It should be requested whenever components are removed during revision shoulder surgery.
Clinical Imaging
Cutibacterium acnes Shoulder Infection
Imaging findings in C. acnes shoulder PJI are often subtle and nonspecific. Radiographs may show only mild radiolucent lines or component loosening without overt signs of infection. This indolent presentation is a hallmark of the organism and contributes to delayed diagnosis.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 62-year-old man presents with gradually worsening pain in his right shoulder arthroplasty performed 3 years ago. He has no fever, no wound issues, and examination shows a well-healed scar with reduced range of motion. CRP is 4 mg/L, ESR is 12 mm/hr. X-rays show a radiolucent line around the glenoid component. How would you investigate and manage this?”
“You are performing a revision shoulder arthroplasty for presumed aseptic loosening in a 58-year-old man. You send 6 tissue samples as routine. At 10 days post-operatively, the microbiology lab phones to say 3 of 6 tissue samples have grown Cutibacterium acnes on anaerobic culture. The patient is making good post-operative progress. How do you manage this?”
Microbiology Essentials
- Gram-positive anaerobic bacillus (formerly Propionibacterium acnes)
- Slow-growing: requires 14-21 day anaerobic culture
- Biofilm-forming: adheres to implants, resistant to antibiotics and host immunity
- Skin commensal in deep hair follicles and sebaceous glands of upper trunk
- Resistant to metronidazole — do NOT use as anti-anaerobic cover
Diagnosis
- CRP and ESR are frequently NORMAL — cannot exclude PJI
- Male sex + shoulder arthroplasty + indolent pain = suspect C. acnes
- Prolonged anaerobic culture (14-21 days) of minimum 5 tissue samples is mandatory
- Sonication of explanted components increases sensitivity significantly
- Shoulder-specific synovial WCC thresholds (greater than 1000-2000) are lower than hip/knee
Treatment Algorithm
- Acute (under 3 months) = DAIR + 4-6 weeks targeted antibiotics
- Chronic = one-stage or two-stage revision + 4-6 weeks antibiotics
- Unexpected positive = antibiotics alone if 1 sample, full PJI protocol if 2 or more
- Antibiotics: penicillin G / ceftriaxone / vancomycin / clindamycin + rifampicin combination
- Metronidazole is INEFFECTIVE against C. acnes — classic exam trap
One-Stage vs Two-Stage
- One-stage: known organism, adequate bone stock, thorough debridement achievable
- Two-stage: extensive bone loss, uncertain organism, immunocompromised patient
- Eradication rates similar (85-95 percent) for C. acnes with both approaches
- One-stage gaining favour in European centres for C. acnes specifically
- C. acnes has better outcomes than S. aureus or fungal PJI
Exam Traps
- Normal CRP/ESR does NOT exclude C. acnes shoulder PJI
- Standard 5-day culture will miss C. acnes — must request 14-21 day anaerobic
- Metronidazole does NOT work against C. acnes despite anaerobe classification
- A single positive C. acnes culture may be significant — do not dismiss as contaminant
- C. acnes is the most common shoulder PJI organism, not Staphylococcus
Evidence Base and Key Trials
Propionibacterium acnes: an agent of prosthetic joint infection and colonization
- Retrospective series demonstrating that C. acnes is the most common organism isolated in shoulder PJI
- Normal CRP and ESR in a significant proportion of confirmed C. acnes PJI cases
- Prolonged anaerobic culture (14-21 days) was essential for organism identification
- Male sex was the predominant risk factor
Microbiologic diagnosis of prosthetic shoulder infection by use of implant sonication
- Sonication of removed prosthetic components significantly increased culture yield for P. acnes compared with periprosthetic tissue culture alone
- Biofilm disruption by sonication enabled detection of organisms not isolated from tissue samples
- Recommended as an adjunct to tissue culture in all revision shoulder arthroplasties
One-stage revision for infected shoulder arthroplasty: prospective, observational study of 37 patients
- One-stage exchange with thorough debridement and targeted antibiotics achieved eradication rates comparable to two-stage exchange for shoulder PJI including C. acnes
- Functional outcomes were favourable with a single surgical intervention
- Appropriate for patients with known organism, adequate bone stock, and no severe soft tissue compromise
Propionibacterium acnes: an underestimated pathogen in implant-associated infections
- Comprehensive review of P. acnes pathogenesis, from skin commensal to implant pathogen
- Intra-operative contamination rates during arthroplasty are significant
- Biofilm formation is central to pathogenesis and antibiotic resistance
- Recommended minimum 14-day anaerobic culture for all revision cases
How is infection diagnostic criteria for shoulder periprosthetic joint infection reported in literature: systematic review
- Standard MSIS criteria have poor sensitivity for shoulder PJI, particularly for low-virulence organisms like C. acnes
- Diagnostic criteria for shoulder PJI are inconsistently reported and applied across studies
- Prolonged culture duration and sonication are essential adjuncts for shoulder PJI diagnosis
- Clinical context (male sex, indolent presentation, shoulder arthroplasty) should weigh heavily in diagnosis