Post-ACL Reconstruction Arthrofibrosis | Loss of Extension | Anterior Nodule
- Cyclops lesion = localised anterior arthrofibrotic nodule at the ACL graft tibial tunnel entrance
- Presents with loss of terminal extension after ACL reconstruction, typically 3-12 months post-operatively
- Named for its appearance: a bulbous fibrous nodule with a central dimple resembling a single eye
- Diagnosis is clinical (extension deficit) plus MRI (nodule anterior to tibial tunnel, graft impingement)
- Arthroscopic excision restores extension in the great majority of cases
- “Loss of terminal extension after ACLR is never normal and must be investigated
- “The nodule wedges between the graft and the intercondylar roof in full extension, causing a mechanical block
- “MRI sensitivity is high but clinical suspicion is the key to ordering the right scan
- “Arthroscopic findings are pathognomonic: a firm nodular mass with a pale fibrous surface at the tibial tunnel aperture
Cyclops lesion = localised fibrovascular nodule at the tibial tunnel aperture after ACLR. The nodule forms from organised scar tissue at the anterior opening of the tibial bone tunnel, anterior to the ACL graft. It causes a mechanical block to terminal extension by impinging between the graft and the femoral intercondylar notch roof.
Isolated loss of terminal extension with a hard end-point, typically 10-30 degrees. Flexion is preserved. The ACL graft remains intact (negative Lachman, negative pivot shift). Presentation is 3-12 months after ACL reconstruction. This is a post-surgical complication, not a new injury.
Well-circumscribed nodular mass anterior to tibial tunnel entrance. Low signal on T1 and T2 (dense fibrous tissue). The ACL graft posterior to it is intact and continuous. The nodule is seen impinging between the graft and the intercondylar roof. Gadolinium enhancement is not required.
Arthroscopic excision is definitive. Non-operative treatment has a very limited role because the block is mechanical. Excision with shaver and radiofrequency restores extension in over 90 percent of cases. Immediate post-operative extension rehabilitation is critical.
- Diagnosis
- MRI: low-signal nodule at tibial tunnel, graft intact
- Treatment
- Arthroscopic excision with immediate extension rehab
- Key Pearl
- Cyclops lesion = mechanical block, not rehab failure
- Diagnosis
- Clinical: hamstring tightness, capsular contracture
- Treatment
- Aggressive physiotherapy, quadriceps strengthening
- Key Pearl
- Soft end-point responds to rehab; hard end-point needs imaging
- Diagnosis
- MRI: diffuse scar in Hoffa fat pad and suprapatellar pouch
- Treatment
- Arthroscopic release + aggressive rehab
- Key Pearl
- Diffuse arthrofibrosis is a different entity from cyclops
CYCLOPSCyclops Lesion Core Features
Hook:CYCLOPS = Can't You See the Cyclops Lesion Obstructing the Posterolateral Slot!
TUNNELPredisposing Factors for Cyclops Lesion
Hook:TUNNEL = get the tunnel right and you avoid the cyclops!
REMOVEArthroscopic Excision Steps
Hook:REMOVE = Recognise, Examine, Mechanical block, Operate, Verify, Ensure graft safe!
Overview and Epidemiology
Loss of terminal extension after ACL reconstruction is one of the most common reasons for re-operation and prolonged rehabilitation. Cyclops lesion is a specific, treatable cause. The examining surgeon who recognises this entity can spare the patient months of misdirected physiotherapy and offer a definitive arthroscopic solution. It is a favourite exam topic because it bridges graft biology, imaging interpretation, and arthroscopic decision-making.
- Overall incidence: 1-2 percent of all ACL reconstructions
- Risk factors: Non-anatomic tunnel placement (tibial tunnel too anterior), aggressive early rehabilitation, graft impingement against the intercondylar roof, use of patellar tendon autograft (higher reported rates), and excessive soft tissue debris left at the tibial tunnel aperture
- Peak presentation: 3-12 months post-ACLR, once scar tissue has matured into a discrete nodule
- Sex: No strong sex predilection reported
- Extension deficit: The hallmark finding, typically 10-30 degrees
- Pain: Anterior knee pain, worse with terminal extension attempts
- Giving way: Not typical (the ACL graft is intact), but mechanical block can be perceived as instability
- Functional limitation: Inability to lock the knee straight; difficulty with running, cycling, stairs descent
- Arthrofibrosis risk: If missed, the nodule perpetuates inflammation and can contribute to diffuse scarring
Pathophysiology
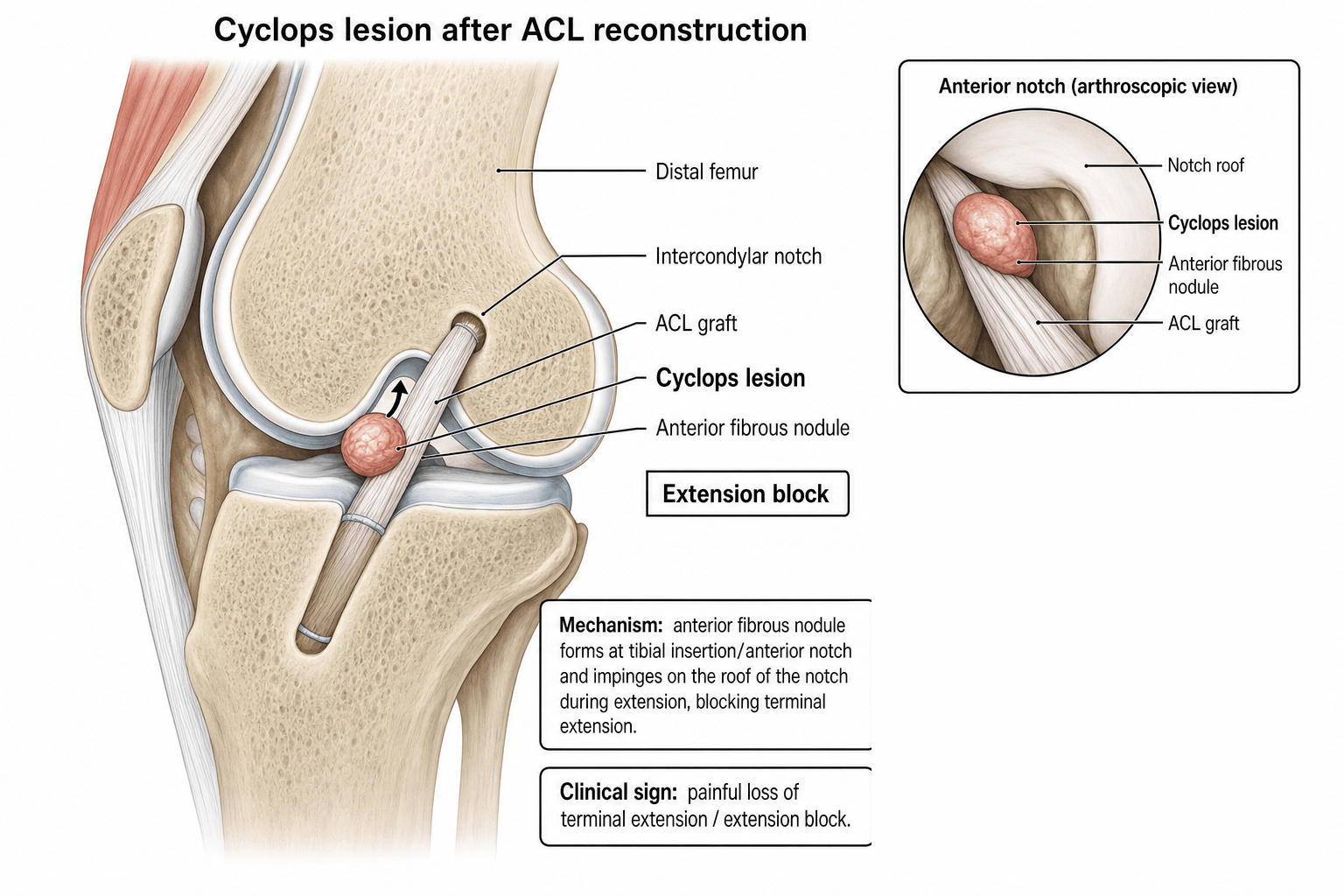
A cyclops lesion is a localised nodular mass of fibrovascular scar tissue that forms at the entrance of the tibial bone tunnel, anterior to the reconstructed ACL graft. The scar tissue arises from debris at the tibial tunnel aperture (remnant ACL fibres, cancellous bone debris, synovial tissue, and graft material) that organises into a firm nodule. In terminal extension, this nodule is trapped between the ACL graft and the femoral intercondylar notch roof, producing a mechanical block to full extension. The name derives from its arthroscopic appearance: a pale, bulbous mass with a central dimple resembling a single eye (cyclops).
- Process
- Bone debris, remnant ACL fibres, and synovial tissue accumulate at the tibial tunnel aperture at the time of drilling or graft passage
- Key Detail
- More debris with larger tunnels, non-anatomic placement, and aggressive graft preparation
- Process
- The debris acts as a scaffold for fibroblast and vascular ingrowth, forming a nodular scar mass over weeks to months
- Key Detail
- This is the body's healing response to intra-articular foreign material
- Process
- The scar organises into a firm, discrete nodule attached to the anterior margin of the tibial tunnel, with a characteristic pale fibrous surface
- Key Detail
- Usually reaches mature size by 3-9 months, which is when the mechanical block becomes clinically apparent
- Process
- In terminal knee extension, the nodule is wedged between the ACL graft (which lies posterior to it) and the femoral intercondylar roof
- Key Detail
- This creates a hard end-point block that physiotherapy cannot overcome
- Nodule position: Anterior to the tibial tunnel aperture, between the graft and the intercondylar notch
- Graft: Intact and functional; the problem is the nodule, not graft failure
- Roof impingement: The nodule abuts the femoral intercondylar roof in full extension, replicating the mechanism of notch impingement
- Notchplasty relevance: Inadequate notchplasty at index surgery predisposes by reducing clearance
- Fibrous tissue: Dense collagen with fibroblasts, consistent with scar
- Vascular channels: Active fibrovascular tissue in early lesions, becoming more fibrotic as the lesion matures
- Occasional bone fragments: Cancellous bone debris from tunnel drilling may be embedded
- No graft involvement: The nodule is separate from the ACL graft itself, which remains viable
Classification and Types
Classification by Anatomic Location
- Location
- Nodule at tibial tunnel entrance, anterior to ACL graft
- Frequency
- Most common (majority of cases)
- Clinical Features
- Isolated extension deficit, hard end-point
- Location
- Nodule at proximal exit of tibial tunnel
- Frequency
- Less common
- Clinical Features
- Similar presentation, higher on the tibial slope
- Location
- Nodule plus surrounding scar tissue
- Frequency
- Uncommon, may occur with delayed diagnosis
- Clinical Features
- Both extension and flexion loss; harder to treat
A genuine examinable nuance is that not every nodule seen on post-ACLR MRI is a true symptomatic cyclops - the Tonin histological subdivision matters:
- True cyclops lesion: a firm nodule with a central core of bone and/or fibrocartilage within the fibrovascular tissue. It is harder, larger and mechanically symptomatic - it produces the classic hard-end-point extension block and is the lesion that needs excision.
- Cyclopoid lesion: composed of soft fibrous granulation tissue only, without the bone/cartilage core. It is softer and frequently asymptomatic - often an incidental MRI finding that does NOT cause a mechanical block.
Why this matters clinically: an MRI report of "a small nodule anterior to the graft" in a patient with full, pain-free extension may be an incidental cyclopoid lesion and does NOT mandate surgery. The decision to excise is driven by the clinical mechanical block (hard-end-point extension deficit), not by the mere presence of a nodule on the scan.
Exam point: treat the patient (a hard-end-point extension block) not the scan; a true cyclops (firm, fibrocartilaginous/bony core) is symptomatic and excised, whereas a soft cyclopoid nodule is often incidental and asymptomatic.
Clinical Assessment
- Previous ACL reconstruction within the last 3-12 months (rarely beyond 24 months)
- Progressive loss of terminal extension that did not improve despite physiotherapy
- Anterior knee pain on extension
- Mechanical blocking or catching sensation reported by the patient
- No new trauma: This is a post-surgical complication, not a new injury
- Extension deficit: The single most important finding. Typically 10-30 degrees. Compare with the contralateral knee
- Hard end-point: The block is mechanical (not soft/elastic from hamstring tightness or capsular contracture)
- Flexion preserved: Distinguishes from diffuse arthrofibrosis which affects both flexion and extension
- Effusion: May be present but is mild
- Lachman and pivot shift: Should be negative (graft is intact)
Hard end-point = mechanical block (cyclops nodule, loose body, meniscal tear, hardware impingement). Requires imaging and likely arthroscopy.
Soft end-point = soft tissue restriction (hamstring tightness, capsular contracture, patellofemoral tightness). May respond to physiotherapy.
Cyclops lesion produces a hard end-point. This distinction is the single most important examination finding that directs the investigation pathway.
- What to Do
- Look for fixed flexion deformity, antalgic gait, quadriceps wasting
- Key Finding in Cyclops Lesion
- Knee held in slight flexion; patient cannot achieve full lock
- What to Do
- Supine, heel on flat surface, compare both knees
- Key Finding in Cyclops Lesion
- Hard end-point block of 10-30 degrees on the reconstructed side
- What to Do
- Measure passive and active flexion range
- Key Finding in Cyclops Lesion
- Flexion is typically preserved (distinguishes from diffuse arthrofibrosis)
- What to Do
- Palpate tibial tunnel area for fullness or tenderness
- Key Finding in Cyclops Lesion
- Occasional palpable firm nodule anterior to tibial tunnel
- What to Do
- Lachman, anterior drawer, pivot shift
- Key Finding in Cyclops Lesion
- Should be negative (intact graft); positive tests suggest graft failure, not cyclops
- What to Do
- Patella mobility, hamstring tightness, effusion
- Key Finding in Cyclops Lesion
- Patella mobility typically preserved; helps exclude infrapatellar contracture
- Extension
- Lost (10-30 deg)
- Flexion
- Preserved
- End-Point
- Hard (mechanical)
- Key Discriminator
- MRI: nodule at tibial tunnel; graft intact
- Extension
- Lost
- Flexion
- Also lost
- End-Point
- Hard or soft
- Key Discriminator
- MRI: diffuse scar throughout Hoffa fat pad and suprapatellar pouch
- Extension
- Lost
- Flexion
- Lost
- End-Point
- Soft (capsular)
- Key Discriminator
- Patella baja, decreased patellar mobility, anterior knee pain
- Extension
- Lost
- Flexion
- Preserved
- End-Point
- Hard
- Key Discriminator
- MRI: graft against roof but no cyclops mass; anterior tunnel placement
- Extension
- Mildly lost
- Flexion
- Preserved
- End-Point
- Soft (elastic)
- Key Discriminator
- Improves with stretching; MRI normal; no nodule
- Extension
- Variable
- Flexion
- Variable
- End-Point
- Variable
- Key Discriminator
- Positive Lachman / pivot shift; MRI shows graft discontinuity
In any patient who has had an ACL reconstruction and presents with loss of terminal extension, cyclops lesion must be on the differential. The cardinal features are: (1) isolated loss of extension (flexion preserved), (2) hard end-point, (3) intact graft on stability testing, (4) timeline of 3-12 months post-ACLR. If the patient has global stiffness (loss of both flexion and extension), think diffuse arthrofibrosis instead.
Investigations
Imaging Protocol
Sequence: Sagittal T1, sagittal PD fat-sat, coronal PD fat-sat, axial PD fat-sat
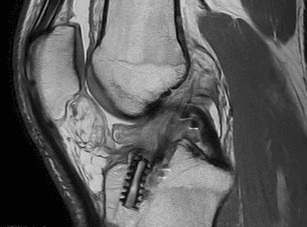
What to look for: A well-circumscribed nodular soft-tissue mass at the anterior opening of the tibial tunnel, anterior to the ACL graft. The mass is typically low-to-intermediate signal on T1 and low signal on T2 (reflecting dense fibrous tissue). The graft itself should appear intact in continuity with tibial and femoral tunnels. The nodule is seen impinging between the graft and the intercondylar roof.
Key measurement: Extension deficit on clinical examination should correlate with the nodule size impinging the notch
Sensitivity: MRI is highly sensitive for cyclops lesions when the appropriate protocol is used. Gadolinium enhancement is not required.
Indication: MRI artefact from hardware (interference screws) obscuring the tibial tunnel region
Findings: Filling defect at the tibial tunnel aperture corresponding to the fibrous nodule
Use: Rarely needed if MRI is performed with metal artefact reduction sequences
Views: AP, lateral, Rosenberg (45-degree PA flexion weight-bearing)
Purpose: Rule out hardware complications (screw migration, tunnel widening, loose body). Assess tunnel position. Look for anterior tibial tunnel placement (tunnel too far anterior predisposes to cyclops lesion and graft impingement).
Limitation: The cyclops lesion is soft tissue and not visible on plain radiographs
On sagittal MRI, the cyclops lesion appears as a nodular mass just anterior to the tibial tunnel entrance, lying between the ACL graft and the intercondylar notch roof. It is typically low signal on all sequences (because it is dense fibrous scar). The ACL graft posterior to it should be intact and continuous. The nodule may demonstrate mild peripheral enhancement post-gadolinium. The finding is most conspicuous on sagittal sequences where the relationship to the notch roof in extension is visible. Do not confuse it with a meniscal cyst (different location) or graft hypertrophy (the graft itself, not a separate nodule).
- Location
- Anterior to tibial tunnel, between graft and roof
- MRI Signal
- Low signal on T1 and T2 (fibrous)
- Key Distinguishing Feature
- Discrete nodule with central dimple; graft intact; extension block
- Location
- Graft against intercondylar roof
- MRI Signal
- Graft signal normal or mildly increased
- Key Distinguishing Feature
- No discrete nodule; may respond to notchplasty; no cyclops mass
- Location
- Throughout the joint, especially infrapatellar
- MRI Signal
- Low signal scar throughout Hoffa fat pad and suprapatellar pouch
- Key Distinguishing Feature
- Global ROM loss, not just extension; thickened scar, not a nodule
- Location
- Adjacent to meniscus body or horn
- MRI Signal
- High T2 signal (fluid)
- Key Distinguishing Feature
- Communicates with meniscal tear; different location; not at tibial tunnel
- Location
- Hoffa fat pad region
- MRI Signal
- Variable, often intermediate signal
- Key Distinguishing Feature
- Less defined than cyclops; no discrete nodule; no mechanical block pattern
Management Algorithm
Non-Operative Management
Role: Limited. A cyclops lesion is a mechanical block caused by a discrete fibrous nodule, which physiotherapy cannot resolve. Non-operative management is appropriate only for:
- Very early lesions (under 3 months) where the scar tissue may still be immature and could potentially remodel
- Mild extension deficits (less than 5 degrees) that are not functionally limiting
- Patients unfit for surgery
Non-Operative Protocol (If Trial Warranted)
Focus: Aggressive quadriceps control, patellar mobilisation, hamstring stretching, posterior glide mobilisations Goal: Improve soft-tissue component of extension deficit Monitor: Serial extension measurements every 2-4 weeks Threshold for surgery: No improvement after 6-8 weeks of focused physiotherapy
If the patient has a clear mechanical block with a hard end-point and MRI confirms a cyclops nodule, continued physiotherapy is futile and delays definitive treatment. The lesion is a physical obstruction that requires removal. Prolonged conservative treatment risks allowing the lesion to mature further and promotes secondary arthrofibrosis from chronic inflammation.
Complications
- Incidence
- Reported but uncommon
- Risk Factors
- Incomplete excision, ongoing impingement, predisposing tunnel position
- Management
- Revision arthroscopic excision; consider tunnel repositioning if anterior placement confirmed
- Incidence
- 5-10 percent
- Risk Factors
- Inadequate rehabilitation, concurrent capsular contracture, incomplete excision
- Management
- MUA + aggressive physiotherapy; revision arthroscopy if mechanical block persists
- Incidence
- Rare but possible
- Risk Factors
- Graft adherent to nodule, poor visualisation, over-aggressive shaver use
- Management
- Minor: protect and monitor; major: revision ACL reconstruction
- Incidence
- Low if treated promptly
- Risk Factors
- Delayed diagnosis, prolonged inflammation from impingement
- Management
- More aggressive rehabilitation; rare cases require further arthroscopic release
- Incidence
- Standard arthroscopy risk (less than 1 percent)
- Risk Factors
- Immunocompromised, prolonged procedure, wound contamination
- Management
- Urgent arthroscopic washout + antibiotics
Cyclops lesion is largely a preventable complication. At the time of ACL reconstruction: (1) place the tibial tunnel at the anatomic centre of the native ACL footprint (not too anterior), (2) perform adequate notchplasty if the intercondylar notch is narrow, (3) thoroughly irrigate the joint and debride debris from the tibial tunnel aperture after graft passage, and (4) avoid aggressive forced extension in the early post-operative period. These steps dramatically reduce the risk.
Beyond the index-surgery technical steps, the single biggest preventable driver of post-ACLR stiffness (cyclops and diffuse arthrofibrosis) is operating on the wrong knee at the wrong time:
- Do not reconstruct the acutely swollen, stiff, inflamed knee. Shelbourne's classic teaching is that ACL reconstruction performed on a knee that is hot, effused and lacking full extension carries a markedly higher arthrofibrosis/cyclops rate.
- "Quiet the knee first": defer reconstruction until the knee has regained full (symmetric) extension and near-full flexion, the effusion has settled, and the patient has good quadriceps control ("prehabilitation"). This is more important than a fixed number of days/weeks from injury.
- Full extension is the priority: pre-operative and immediate post-operative emphasis on achieving full terminal extension (heel-prop, prone hangs) is the most protective rehabilitation goal - a knee that never regains extension is the one that scars.
- Why it fits cyclops: a quiet knee with good ROM and meticulous tunnel technique is the combination that minimises the fibrovascular response at the tunnel aperture.
Exam point: reduce cyclops/arthrofibrosis by reconstructing a "quiet" knee (full extension, settled effusion, good quad control) rather than an acutely inflamed stiff one, and prioritise regaining full extension before and immediately after surgery.
Outcomes and Prognosis
- Typical Result
- Full or near-full extension restored in over 90 percent
- Key Point
- Mechanical block removed; most patients regain full extension
- Typical Result
- Greater than 90 percent return to pre-injury sport level
- Key Point
- Rehabilitation usually 2-3 months after excision
- Typical Result
- ACL graft remains stable and functional
- Key Point
- The graft is separate from the lesion; excision does not compromise graft
- Typical Result
- Low with complete excision
- Key Point
- Higher if predisposing factors (anterior tunnel) not addressed
- Typical Result
- High, as the operation is minimally invasive and effective
- Key Point
- Patients are often relieved to have a definitive mechanical explanation
Best prognosis: Early diagnosis (within 12 months), discrete nodule without diffuse fibrosis, complete arthroscopic excision, and immediate post-operative extension rehabilitation. Worse prognosis: Delayed diagnosis (over 24 months), associated diffuse arthrofibrosis, incomplete excision, and anterior tunnel malposition that is not corrected.
Guidelines, Registries & Global Practice
- Cyclops lesion is reported worldwide following ACL reconstruction across all graft types and fixation methods
- Incidence is declining in centres using anatomic ACL reconstruction techniques with precise tunnel positioning
- Higher historical incidence was associated with transtibial drilling techniques that produced anterior tibial tunnels
- No strong geographic or ethnic variation; incidence relates to surgical technique rather than patient factors
- High-resource: MRI is readily available; early diagnosis; arthroscopic excision as day-case surgery with structured rehabilitation
- Limited-resource: Diagnosis may rely more on clinical examination and plain radiographs; CT arthrogram if MRI unavailable; excision still possible with basic arthroscopy equipment
- Universal principle: outcome depends on early recognition of the extension deficit and prompt arthroscopic intervention
- Prevention: Meticulous tunnel placement and joint debridement at index surgery are achievable in all settings
- Prevention emphasis
- Anatomic single-bundle or anatomic double-bundle ACLR; adequate notchplasty; debridement of tunnel debris
- Diagnosis
- MRI for persistent extension deficit after ACLR; clinical hard end-point is key finding
- Treatment
- Arthroscopic excision; structured post-operative rehabilitation with immediate extension focus
- Prevention emphasis
- Individualised anatomic tunnel placement using fluoroscopic or navigation guidance; graft harvesting and preparation to minimise debris
- Diagnosis
- MRI with fat-suppressed sequences; correlate with clinical examination for hard end-point block
- Treatment
- Arthroscopic excision recommended; rehabilitation guided by sport-specific timelines
- Prevention emphasis
- Anatomic ACLR techniques emphasised in BOAST guidelines; notchplasty as needed
- Diagnosis
- Clinical suspicion drives imaging request; MRI first-line for any unexplained post-ACLR stiffness
- Treatment
- Arthroscopic excision as day-case procedure; physiotherapy-led rehabilitation
- Prevention emphasis
- Tunnel positioning at native ACL footprint; soft tissue debridement; careful graft passage technique
- Diagnosis
- MRI protocol for post-operative knee; assess tunnel position on radiographs
- Treatment
- Arthroscopic debridement of the nodule; consider tunnel revision if malpositioned
There is no dedicated registry for cyclops lesions. However, national ACL reconstruction registries (Danish ACL Registry, Swedish National Knee Ligament Register, Norwegian Knee Ligament Registry, NZJR) capture re-operation rates after ACLR, which include arthroscopic procedures for cyclops lesions. Registry data suggest that re-operation for stiffness and arthrofibrosis after ACLR accounts for a small but important proportion of all re-operations. The trend toward anatomic ACL reconstruction is reflected in declining re-operation rates for extension loss in registry data.
Record in every ACL reconstruction follow-up:
- Passive and active extension range measured against the contralateral knee
- Whether the end-point is hard (mechanical) or soft (capsular/muscular)
- If a hard block is present, document suspicion for cyclops lesion and order MRI
- At index surgery, document tunnel positions, notchplasty performed, and adequacy of joint lavage
Failure to diagnose a cyclops lesion after months of physiotherapy for a mechanical block is a recurring theme in clinical negligence claims. Always investigate a persistent extension deficit after ACLR with imaging rather than attributing it to rehabilitation failure.
Controversies & Areas of Uncertainty
There is no consensus on the minimum interval after index ACLR before performing cyclops excision. Most surgeons wait at least 3 months to allow the nodule to mature into a discrete, excisable mass, but earlier intervention may prevent secondary arthrofibrosis. The balance is between nodule maturity (easier excision when well-formed) and preventing chronic impingement.
There is limited evidence for pharmacological prevention of cyclops lesion. Some centres use NSAIDs or steroid injections post-operatively to modulate scar formation, but this is not evidence-based for cyclops prevention specifically and carries its own risks.
Whether routine notchplasty should be performed at all ACL reconstructions to prevent cyclops and graft impingement, or only when the notch is objectively narrow, remains debated. Routine notchplasty may increase bone debris and potentially paradoxically contribute to cyclops formation if debris is not adequately cleared.
Some early series reported higher cyclops rates with patellar tendon bone-tendon-bone autograft, but contemporary anatomic techniques using hamstring autograft also report cyclops lesions. The relative risk by graft type is not definitively established, and surgical technique (tunnel position, debridement) likely matters more than graft choice.
MCQ Practice Points
Q: What is a cyclops lesion? A: A cyclops lesion is a localised nodular mass of fibrovascular scar tissue that forms at the entrance of the tibial bone tunnel, anterior to the reconstructed ACL graft, after ACL reconstruction. It causes a mechanical block to terminal extension by impinging between the graft and the intercondylar notch roof. Named for its arthroscopic appearance resembling a single eye.
Q: How do you diagnose a cyclops lesion? A: Clinical: Isolated loss of terminal extension (10-30 degrees) with a hard end-point after ACLR, preserved flexion, intact graft (negative Lachman). MRI: Well-circumscribed low-signal nodule on T1 and T2 at the anterior tibial tunnel entrance, anterior to an intact ACL graft, impinging on the intercondylar roof. The diagnosis is clinical plus imaging; arthroscopy is both diagnostic and therapeutic.
Q: What is the definitive treatment for cyclops lesion? A: Arthroscopic excision using shaver and radiofrequency ablation. The nodule is debulked from its base at the tibial tunnel aperture while protecting the ACL graft posterior to it. Post-operative rehabilitation emphasises immediate extension regain. Non-operative treatment has a very limited role because the block is mechanical. Over 90 percent of patients regain full extension after excision.
Q: How do you distinguish cyclops lesion from diffuse arthrofibrosis after ACLR? A: Cyclops lesion: Isolated loss of extension with preserved flexion, hard end-point, discrete nodule on MRI, excellent response to excision. Diffuse arthrofibrosis: Global loss of both flexion and extension, diffuse scar throughout the Hoffa fat pad and suprapatellar pouch on MRI, guarded prognosis, requires more extensive arthroscopic release.
Q: What are the key preventable risk factors for cyclops lesion at ACLR? A: Anterior tibial tunnel placement (the single most important factor), inadequate notchplasty leaving insufficient roof clearance, debris left at the tibial tunnel aperture after drilling and graft passage, and aggressive forced terminal extension in early post-operative rehabilitation. Prevention is achieved by anatomic tunnel positioning, adequate notchplasty, thorough joint irrigation and debridement, and guided rehabilitation.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old netball player had an ACL reconstruction 6 months ago using hamstring autograft. She has made good progress with flexion but cannot fully extend her left knee. Examination reveals a 15-degree extension deficit with a hard end-point. Her Lachman test is negative. She is frustrated because her physiotherapist says she is not working hard enough. What is your assessment and management?”
“A 30-year-old footballer had an ACL reconstruction 4 years ago. Two years after the reconstruction, he underwent arthroscopic excision of a cyclops lesion with good initial restoration of extension. He now presents again with a 10-degree extension deficit and similar symptoms. MRI suggests a recurrent cyclops-like nodule. How would you manage this recurrence?”
Definition and Pathogenesis
- Cyclops lesion = localised anterior arthrofibrotic nodule at the tibial tunnel entrance after ACLR
- Named for arthroscopic appearance: bulbous nodule with central dimple (single eye)
- Forms from organised fibrovascular scar on a scaffold of tunnel debris, remnant ACL, and bone dust
- Nodule wedges between the ACL graft and the intercondylar roof in full extension, causing mechanical block
Clinical Presentation
- Isolated loss of terminal extension (10-30 degrees) with preserved flexion, typically 3-12 months post-ACLR
- Hard end-point block (not soft/elastic), anterior knee pain on extension
- ACL graft is intact: negative Lachman, negative pivot shift (this distinguishes from graft failure)
- Incidence approximately 1-2 percent of ACL reconstructions
Risk Factors
- Anterior tibial tunnel placement (the single most important modifiable factor)
- Inadequate notchplasty leaving insufficient roof clearance
- Debris left at the tibial tunnel aperture after drilling and graft passage
- Aggressive forced terminal extension in early post-operative rehabilitation
Investigations
- MRI (first-line): low-signal nodule on T1 and T2 at tibial tunnel entrance, anterior to graft
- Plain radiographs: rule out hardware issues and assess tunnel position
- CT arthrogram: reserved for cases where MRI artefact from screws obscures the region
Treatment
- Non-operative: very limited role; mechanical block requires physical removal
- Arthroscopic excision: definitive treatment, restores extension in over 90 percent
- Technique: shaver and radiofrequency excision from base at tibial tunnel, protect graft, check extension under vision
- Post-op: immediate extension rehabilitation, aggressive quadriceps work, return to sport 2-3 months after excision
Complications
- Recurrence (uncommon if complete excision; higher if tunnel malposition persists)
- Persistent extension deficit (incomplete excision or concurrent capsular contracture)
- Graft damage during excision (rare; graft lies immediately posterior to nodule)
- Progression to diffuse arthrofibrosis if diagnosis delayed
Evidence Base and Key Trials
Cyclops syndrome: loss of extension following intra-articular anterior cruciate ligament reconstruction
- Original description of the cyclops syndrome as a cause of loss of extension after intra-articular ACL reconstruction
- Reported nodular scar tissue at the tibial tunnel aperture producing a mechanical block to full extension
- Named the lesion for its arthroscopic appearance: a bulbous nodule resembling a single eye (cyclops)
- Demonstrated that arthroscopic excision restored extension in affected patients
MR imaging evaluation of the postoperative knee
- Comprehensive review of MRI findings after ACL reconstruction including cyclops lesion appearance
- Described the cyclops lesion as a low-signal nodular mass at the tibial tunnel entrance on sagittal sequences
- Emphasised that the lesion is separate from the ACL graft and the graft itself remains intact
- Discussed MRI protocol optimisation to minimise artefact from interference screws
Localized anterior arthrofibrosis (cyclops lesion) after reconstruction of the anterior cruciate ligament: MR imaging findings
- First dedicated study of MRI findings in cyclops lesions after ACL reconstruction
- Described the cyclops lesion as a focal nodular soft-tissue mass anterior to the ACL graft at the tibial tunnel aperture
- Demonstrated low signal on T1-weighted and intermediate-to-low signal on T2-weighted images consistent with fibrous tissue
- Established MRI criteria for distinguishing cyclops lesion from graft impingement and other post-operative masses
Cyclops Lesions of the Knee: A Narrative Review of the Literature
- Reviewed the literature on incidence (1-2 percent of ACLR), risk factors (anterior tunnel placement, debris), and management
- Summarised that tibial tunnel position and thorough debridement at index surgery are the most important preventable factors
- Confirmed that arthroscopic excision with immediate extension rehabilitation is the gold standard treatment
- Noted that recurrence is rare when complete excision is achieved
Classification and management of arthrofibrosis of the knee after anterior cruciate ligament reconstruction
- Distinguished cyclops lesion (localised nodule) from diffuse arthrofibrosis following ACL reconstruction
- Cyclops lesions presented with isolated extension loss while diffuse arthrofibrosis affected both flexion and extension
- Patients with cyclops lesions responded better to arthroscopic excision than those with diffuse fibrosis
- Emphasised the importance of early recognition and treatment to prevent progression to diffuse scarring