A Low-Grade Cutaneous Sarcoma with a Tendency to Recur
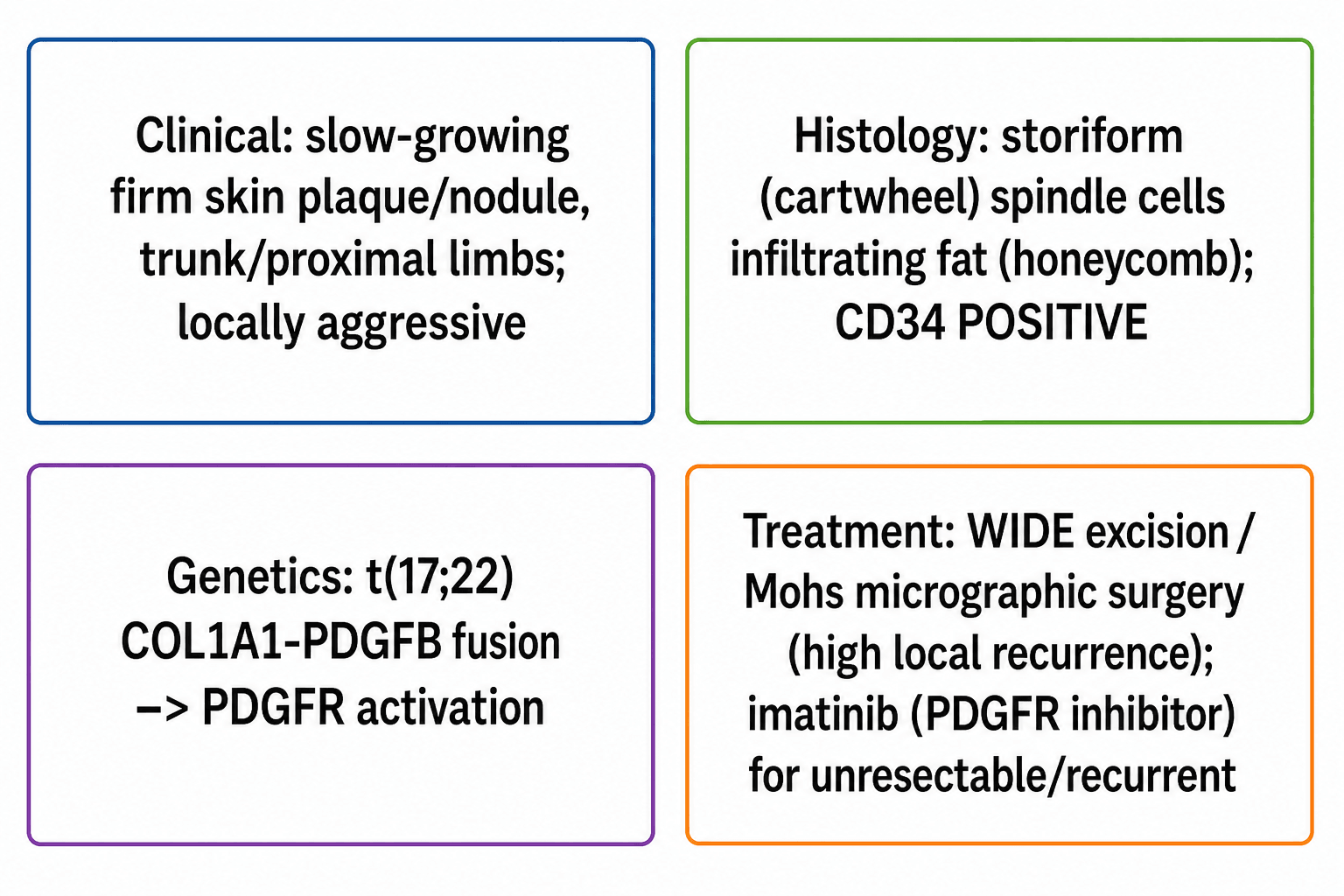
- Dermatofibrosarcoma protuberans (DFSP) is a rare LOW-GRADE cutaneous soft-tissue sarcoma arising in the dermis/subcutis, typically a slow-growing firm plaque or nodule (often skin-coloured to violaceous) on the TRUNK or proximal limbs of middle-aged adults; it is often present for years and is frequently mistaken for a benign lesion (dermatofibroma, scar, cyst) before the protuberant nodular phase.
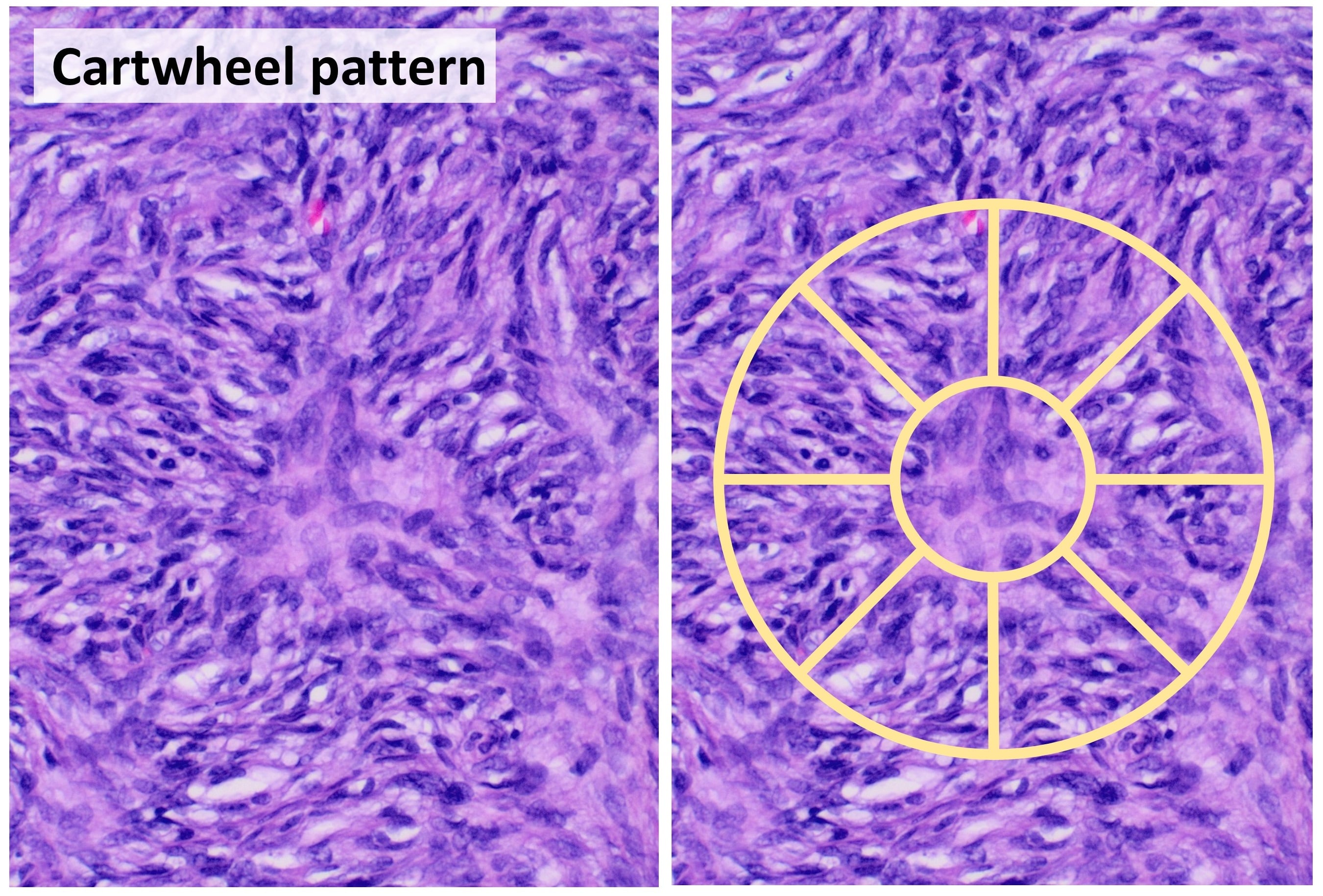
- The histology is characteristic: monomorphic SPINDLE CELLS arranged in a STORIFORM ('cartwheel') pattern that INFILTRATE the subcutaneous fat in a lacy 'honeycomb' fashion, and the tumour is CD34 POSITIVE - which helps distinguish it from a benign dermatofibroma (CD34-negative, factor XIIIa-positive).
- DFSP is driven by a specific GENETIC lesion - the translocation t(17;22)(q22;q13) producing the COL1A1-PDGFB FUSION gene, which causes constitutive PLATELET-DERIVED GROWTH FACTOR B signalling and PDGF-receptor activation, stimulating tumour proliferation - and this is the molecular TARGET for imatinib.
- Its behaviour is LOW-grade but with a VERY HIGH LOCAL RECURRENCE rate, because the tumour spreads with finger-like INFILTRATIVE projections well beyond the clinically apparent margin; distant METASTASIS is RARE in conventional DFSP but the FIBROSARCOMATOUS variant (DFSP-FS) has a higher metastatic risk (around 8-29%).
- TREATMENT is primarily SURGICAL: WIDE local excision with adequate margins or MOHS MICROGRAPHIC SURGERY, which gives the best margin control and the lowest recurrence - achieving clear margins is the key to cure given the infiltrative growth; radiotherapy is an adjunct for close/positive margins.
- IMATINIB (a PDGFR tyrosine kinase inhibitor that targets the COL1A1-PDGFB fusion product) is used for UNRESECTABLE, RECURRENT or METASTATIC disease and as NEOADJUVANT therapy to shrink large tumours before surgery; long-term follow-up is needed because of the recurrence risk.
- “DFSP = low-grade cutaneous sarcoma; storiform (cartwheel) spindle cells, CD34 POSITIVE (vs dermatofibroma CD34-negative).
- “t(17;22) COL1A1-PDGFB fusion -> PDGFR activation = the imatinib target.
- “Very high LOCAL recurrence (infiltrative margins) -> wide excision / Mohs (margin control is key); imatinib for unresectable/recurrent/metastatic; fibrosarcomatous variant metastasises.
DFSP infiltrates with finger-like projections beyond the visible edge -> very high local recurrence. Wide excision / Mohs for clear margins is the cure.
t(17;22) COL1A1-PDGFB fusion drives PDGFR signalling - imatinib is used for unresectable, recurrent or metastatic disease (and neoadjuvant).
Epidemiology, Natural History & Variants
DFSP is rare - of the order of a few cases per million people per year - and accounts for roughly one in a hundred soft-tissue sarcomas, but it is the commonest sarcoma to arise primarily in the skin. It presents most often between the third and fifth decades, in adults of any sex, and has a recognised predilection for darker skin, in whom the pigmented variant is over-represented. Site distribution matters because it predicts the reconstructive problem: roughly half arise on the trunk, about a third on the proximal limbs, and the remainder on the head and neck, where tissue is scarce and margin-sparing technique becomes decisive. A minority arise at sites of previous trauma, burns, scars or vaccination, which is one reason a "scar" that thickens, spreads laterally or becomes nodular after years of stability deserves biopsy rather than reassurance.
The natural history explains the classic late presentation. The tumour begins as a firm, indurated plaque that enlarges over years - often described by the patient as a bruise or a scar that never settled - before entering the protuberant phase, in which one or more nodules rise from the plaque and growth accelerates. Median symptom duration before diagnosis is measured in years, and the lesion is frequently excised marginally as a presumed cyst or dermatofibroma before the diagnosis is made. Such an unplanned excision does not change the biology, but it does convert a straightforward wide excision into a re-excision of a contaminated field: the whole previous scar and any drain sites must be taken with the specimen. Our Soft-Tissue Masses & Sarcoma Referral topic covers that referral pathway in full.
Variants worth naming
- Fibrosarcomatous DFSP (FS-DFSP) - transformation to a higher-grade tumour, arising either at presentation or in a recurrence. The storiform pattern gives way to fascicular, herringbone architecture with markedly higher mitotic activity and, importantly, loss of CD34 staining in the transformed areas. It is the one variant with real metastatic potential and the one that changes staging and follow-up.
- Pigmented DFSP (Bednar tumour) - conventional DFSP containing scattered melanin-laden dendritic cells, giving the lesion a brown or blue-black hue that can suggest melanoma clinically. Behaviour is that of conventional DFSP; the pigment is not adverse.
- Giant cell fibroblastoma - the juvenile counterpart, carrying the same COL1A1-PDGFB fusion, with pseudovascular spaces lined by multinucleate giant cells. It can recur as conventional DFSP and DFSP can recur as giant cell fibroblastoma, which is why the two are regarded as one entity across the age spectrum.
- Myxoid and sclerosing areas are common focally and matter mainly because they can mislead a small biopsy away from the diagnosis.
Clinical Features & Histology
DFSP presents as a slow-growing, firm plaque or nodule on the trunk or proximal limbs, often skin-coloured or violaceous and present for years, so it is commonly mistaken for a dermatofibroma, scar or cyst until it enters the protuberant nodular phase. The histology is distinctive: monomorphic spindle cells in a storiform (cartwheel) pattern that infiltrate subcutaneous fat in a lacy 'honeycomb' manner, and the tumour is CD34 POSITIVE - which, with the cartwheel pattern, distinguishes it from a benign dermatofibroma (CD34-negative, factor XIIIa-positive). The molecular hallmark is the t(17;22) COL1A1-PDGFB fusion.
Diagnosis: Biopsy, Imaging and Molecular Confirmation
Because DFSP is a soft-tissue sarcoma, it obeys sarcoma biopsy rules: a core needle or incisional biopsy placed so that the tract lies within the future resection specimen, oriented longitudinally on a limb, performed by or in consultation with the unit that will resect it. A shave biopsy is the specific trap here - it samples the dermal plaque only, may show bland spindle cells, and can return a report of dermatofibroma while the diagnostic subcutaneous infiltration sits below the sampled tissue. The general principles are set out in Biopsy Principles & Techniques.
Imaging does not make the diagnosis but plans the operation. MRI shows the true extent - characteristically a dermal and subcutaneous mass, low to intermediate on T1 and high on T2, with tail-like subcutaneous extensions - and answers the questions that decide the resection: does it reach or breach the deep fascia, does it involve muscle, and how far do the projections run beyond the palpable edge? Staging for distant disease is not routine in conventional DFSP, given how rarely it metastasises, but a CT chest is warranted when the histology is fibrosarcomatous, in large or recurrent tumours, and before starting systemic therapy. Spread, when it occurs, is haematogenous to lung; nodal involvement is distinctly unusual.
Molecular confirmation is available and is worth requesting when the immunohistochemistry is equivocal, when a small biopsy shows myxoid or fibrosarcomatous areas without diagnostic storiform architecture, or before committing a patient to systemic therapy. FISH for the COL1A1-PDGFB rearrangement (or RT-PCR, or a fusion panel) detects the fusion - typically as a supernumerary ring chromosome derived from chromosomes 17 and 22 - in the great majority of cases. A small minority of otherwise typical DFSP has no detectable COL1A1-PDGFB fusion, and that matters therapeutically rather than diagnostically: those tumours are not expected to respond to imatinib.
The CD34-Positive Cutaneous Spindle-Cell Differential
DFSP (CD34 positive) is classically set against a benign dermatofibroma (CD34 negative, factor XIIIa positive), but a storiform CD34-positive cutaneous spindle-cell lesion has a wider differential than that pair. Some mimics are also CD34 positive, so the immunohistochemical and molecular panel below is what resolves it.
- CD34
- POSITIVE
- Discriminating marker / clue
- Factor XIIIa negative; COL1A1-PDGFB fusion confirms it
- What it means for management
- Wide excision with generous margins or Mohs surgery - the tumour spreads in finger-like projections well beyond the visible edge, which is why narrow excision recurs. Imatinib targets the PDGFB fusion in unresectable or metastatic disease
- CD34
- Negative
- Discriminating marker / clue
- Factor XIIIa POSITIVE; well-circumscribed, no fat infiltration
- What it means for management
- Benign - reassure, or simple excision if symptomatic or the diagnosis is uncertain. No margins, no surveillance
- CD34
- POSITIVE
- Discriminating marker / clue
- STAT6 POSITIVE (NAB2-STAT6 fusion) - the key discriminator
- What it means for management
- Complete excision and long-term surveillance - behaviour is unpredictable, and even histologically bland tumours can metastasise late, so this is not a lesion to discharge
- CD34
- Negative
- Discriminating marker / clue
- S100 / SOX10 POSITIVE; atypia, junctional component
- What it means for management
- The one that changes the prognosis entirely - melanoma staging, sentinel node discussion and oncology referral. Desmoplastic melanoma is the classic mimic caught only by S100/SOX10, so never accept a spindle-cell diagnosis without it
- CD34
- Variable
- Discriminating marker / clue
- S100 POSITIVE; neural architecture
- What it means for management
- Benign, but check for neurofibromatosis 1 - and a plexiform neurofibroma that becomes painful or grows rapidly needs imaging for malignant transformation to MPNST
CD34 separates DFSP (positive) from a dermatofibroma (negative, factor XIIIa positive) - but solitary fibrous tumour is also CD34 positive, so use STAT6 to exclude it, S100/SOX10 for melanoma, and the COL1A1-PDGFB fusion (FISH or RT-PCR) as the confirmatory test when the immunohistochemistry is ambiguous.
Behaviour & Treatment
DFSP is low-grade and rarely metastasises, but it has a very high LOCAL recurrence rate because it spreads with infiltrative, finger-like projections far beyond the clinically obvious margin. The FIBROSARCOMATOUS variant (DFSP-FS) is more aggressive, with higher mitotic activity and a real risk of distant metastasis (reported around 8-29%), so it warrants closer staging and follow-up.
- Wide local excision with adequate margins, or MOHS MICROGRAPHIC SURGERY, which provides the best circumferential and deep margin control and the lowest recurrence - clearing margins is the key to cure given the infiltrative growth.
- Radiotherapy as an adjunct for close or positive margins or where wide excision is not feasible.
- Imatinib (a PDGFR tyrosine kinase inhibitor targeting the COL1A1-PDGFB fusion product) for unresectable, recurrent or metastatic disease, and as NEOADJUVANT therapy to shrink large tumours before surgery.
- Long-term follow-up for local recurrence; image and stage the fibrosarcomatous variant for metastasis.
Getting the Margin Right: Wide Excision, Mohs and Reconstruction
Margin control is the cure, so be ready with the specifics behind "adequate margins" - how wide, how deep, and how reconstruction is sequenced - because the finger-like infiltration is exactly why a casual excision fails.
- Wide local excision with a generous peripheral margin (commonly cited as around 2 to 3 cm) taken down to and including the deep fascia, because the tumour tracks along the subcutis and fascial plane.
- Mohs / complete circumferential peripheral and deep margin assessment (CCPDMA) examines the entire margin and gives the lowest recurrence while sparing tissue - especially valuable on the head/neck or where tissue is at a premium.
- Stage the reconstruction: in a "slow Mohs"/staged excision, leave the defect open or temporarily covered and delay definitive reconstruction (flap/graft) until margins are confirmed clear, so a flap is not laid over residual tumour.
- Fibrosarcomatous variant: the same wide approach plus staging/imaging for metastasis and closer follow-up, given its distant-spread potential.
"Adequate margins" means a wide peripheral margin down to and through the deep fascia, or Mohs/CCPDMA for complete margin control; confirm clear margins before definitive flap reconstruction. Margin status, not the low grade, determines the outcome.
What the margin buys, and what follows it
The reported difference between techniques is the number to have ready. Series of conventional wide local excision report local recurrence in the region of five to twenty per cent, the spread reflecting how wide the margin was and whether the deep fascia was taken; Mohs or staged CCPDMA excision, which examines the whole margin rather than sampled sections of it, reports recurrence in low single figures. That is the argument for complete margin assessment, and it is strongest exactly where wide margins are unaffordable - the face, scalp, hands and feet. Where neither is available, the fallback is a generous excision with careful orientation of the specimen and a low threshold for re-excision rather than acceptance of a close margin.
Recurrence is overwhelmingly local and most often declares itself within the first three years, so surveillance is clinical: inspection and palpation of the scar and the surrounding skin, roughly six-monthly for the first few years and then annually, continued long-term because late recurrence beyond five years is described. Routine imaging of the primary site is not required after a clear margin; cross-sectional imaging is reserved for a suspicious clinical finding. Fibrosarcomatous disease is the exception that earns interval chest imaging alongside clinical review.
Where imatinib is used, it is given as a continuous daily tyrosine-kinase inhibitor in the neoadjuvant, unresectable or metastatic setting, and it is a cytoreductive agent rather than a curative one - responses are common but partial, so the plan should be to convert an unresectable tumour into a resectable one and then operate, not to substitute drug for surgery. Two practical caveats follow from that: confirm the fusion before committing, since fusion-negative tumours are not expected to respond, and time the operation to the response plateau rather than continuing indefinitely.
Mnemonics & Memory Aids
DFSP
Hook:DFSP: Dermal, Fusion (COL1A1-PDGFB), Storiform CD34+, Protuberant/recurrent.
CD34
Hook:CD34-positive + cartwheel = DFSP (not dermatofibroma).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is dermatofibrosarcoma protuberans, what are its key histological and genetic features, and how is it treated?”
“Why does DFSP recur locally so often, and how does that influence surgical management?”
Clinical
- Low-grade cutaneous sarcoma; slow-growing firm plaque/nodule
- Trunk and proximal limbs; middle-aged adults
- Often mistaken for benign lesion until protuberant phase
Histology & genetics
- Storiform (cartwheel) spindle cells infiltrating fat (honeycomb)
- CD34 POSITIVE (vs dermatofibroma CD34-negative/factor XIIIa+)
- t(17;22) COL1A1-PDGFB fusion -> PDGFR activation
- Variants: FS (herringbone, LOSES CD34), pigmented Bednar, giant cell fibroblastoma
Behaviour
- Very high LOCAL recurrence (infiltrative margins)
- Conventional DFSP rarely metastasises
- Fibrosarcomatous variant (DFSP-FS): metastatic risk ~8-29%
Treatment
- Wide local excision / Mohs micrographic surgery (margin control = cure)
- Radiotherapy for close/positive margins
- Imatinib for unresectable/recurrent/metastatic + neoadjuvant; long-term follow-up
Evidence & Key Studies
Dermatofibrosarcoma protuberans: COL1A1-PDGFB fusion, Mohs surgery and imatinib
- DFSP is locally aggressive, with proliferating spindle cells infiltrating the reticular dermis and subcutis, giving high local recurrence rates.
- The t(17;22)(q22;q13) translocation forms the COL1A1-PDGFB fusion gene that stimulates tumour proliferation.
- First-line treatment is surgical excision with Mohs micrographic surgery for margin control; imatinib (a tyrosine kinase inhibitor) is used for unresectable tumours and recurrences.
Fibrosarcomatous DFSP with distant metastasis: a rare case report
- Conventional DFSP rarely metastasises, but the fibrosarcomatous variant (DFSP-FS) shows a higher incidence of distant spread (reported 8-29%).
- DFSP is associated with the COL1A1-PDGFB fusion gene driving tumour growth.
- Wide excision with negative margins is the cornerstone, with Mohs surgery for optimal local control; advanced cases benefit from imatinib and radiotherapy.
The COL1A1-PDGFB fusion from t(17;22), the high local recurrence, and the roles of Mohs surgery and imatinib come from the cited Barrios Barreto case, and the higher metastatic potential of the fibrosarcomatous variant and the wide-margin/Mohs/imatinib treatment from the cited Elsherif case. The storiform CD34-positive histology and the distinction from dermatofibroma are standard, well-established soft-tissue-pathology teaching. (See also our Soft-Tissue Sarcoma Referral, Liposarcoma and Synovial Sarcoma topics.)