DDH | Ortolani | Barlow | Pavlik Harness | Pelvic Osteotomy
BY AGE
Critical Must-Knows
- Ortolani reduces a dislocated hip
- Barlow dislocates an unstable hip
- Pavlik harness for under 6 months
- Open reduction if Pavlik fails or late diagnosis
- Acetabular dysplasia needs osteotomy
Clinical Pearls
- "Risk factors: breech, female, first-born, family history
- "Graf ultrasound classification
- "Pavlik success 90-95% if started under 6 weeks
- "Avascular necrosis is worst complication

Critical DDH Concepts
Ortolani Test
Reduces a dislocated hip. Abduct hip with anterior pressure on greater trochanter. Clunk = hip reducing into acetabulum. Positive = hip was dislocated.
Barlow Test
Dislocates an unstable hip. Adduct hip with posterior pressure. Clunk = hip dislocating posteriorly. Positive = hip is unstable/dislocatable.
Pavlik Harness
First-line for under 6 months. Maintains hip in flexion and abduction. 90-95% success if started early. Monitor for AVN.
AVN Risk
Most serious complication. Caused by forced abduction or reduction. Maintain safe zone (avoid excessive abduction).
At a Glance
DDH At a Glance
| Feature | Key Points |
|---|---|
| Definition | Spectrum of hip instability from dysplasia to dislocation |
| Risk factors | Breech, Female, First-born, Family history (BFFF) |
| Key tests | Ortolani (reduces) and Barlow (dislocates) - look for clunk, not click |
| First-line treatment | Pavlik harness under 6 months (90-95% success if started early) |
| Critical complication | AVN from forced abduction - maintain safe zone |
| Late presentation | Requires open reduction + osteotomy with higher complication risk |
Ortolani vs Barlow
| Test | What It Does | Positive Finding |
|---|---|---|
| Ortolani | Reduces dislocated hip | Clunk = hip reducing into acetabulum |
| Barlow | Dislocates unstable hip | Clunk = hip dislocating out |
BFFFDDH Risk Factors
| B | Breech presentation Strong risk factor |
| F | Female 4:1 female predominance |
| F | First-born Tight uterus |
| F | Family history 10x risk if sibling affected |
| B | Breech presentation Strong risk factor | F | First-born Tight uterus |
| F | Female 4:1 female predominance | F | Family history 10x risk if sibling affected |
Hook:BFFF - Breech First-born Female with Family history!
ORIRemember Ortolani vs Barlow
| O | Ortolani O for 'Out' - reduces hip that is out |
| R | Reduces Abduct and lift |
| I | In Hip goes IN to socket |
| O | Ortolani O for 'Out' - reduces hip that is out |
| R | Reduces Abduct and lift |
| I | In Hip goes IN to socket |
Hook:Ortolani Reduces In - brings hip back in!
FLEX ABDPavlik Harness Position
| F | Flexion 100-110 degrees Hip flexion maintained |
| L | Loose fit Not forced |
| E | Early start Under 6 weeks for best results |
| X | X-ray/US follow up Weekly monitoring |
| A | Abduction 50-70 degrees Avoids AVN |
| B | Both hips Even if unilateral DDH |
| D | Duration 6-12 weeks Until stable |
| F | Flexion 100-110 degrees Hip flexion maintained | X | X-ray/US follow up Weekly monitoring | D | Duration 6-12 weeks Until stable |
| L | Loose fit Not forced | A | Abduction 50-70 degrees Avoids AVN | ||
| E | Early start Under 6 weeks for best results | B | Both hips Even if unilateral DDH |
Hook:FLEX ABD - position for Pavlik success!
Overview and Epidemiology
Why Left Side More Common
Left hip is against mother's spine in utero. This position limits abduction and promotes dysplasia. Left side 60%, Right 20%, Bilateral 20%.
Anatomy and Pathophysiology
Hip Joint Development
In utero:
- Femoral head and acetabulum develop together
- Movement stimulates development
- Restricted movement causes dysplasia
Acetabular development:
- Triradiate cartilage contributes to growth
- Labrum deepens socket
- Shape influenced by femoral head position
Normal development requires hip in reduced position.
Pathology and Natural History
Acetabular Changes
- Primary Dysplasia: Shallow, saucer-shaped acetabulum with poor anterior and lateral coverage.
- Secondary Changes: In dislocation, the acetabulum fills with fibrofatty tissue (pulvinar).
- False Acetabulum: In high dislocation, a pseudo-acetabulum forms on the ilium, while the true acetabulum becomes shallow.
Dysplasia proceeds to dislocation if untreated.
Classification
Severity Classification
Dysplastic: Abnormal acetabulum but hip located - shallow socket with inadequate coverage Subluxed: Partial contact between femoral head and acetabulum - hip partially displaced Dislocated: No contact between femoral head and acetabulum - complete displacement
Teratologic DDH: Early in utero dislocation with severe soft tissue contractures (associated with syndromes like arthrogryposis). More resistant to treatment.
Severity guides treatment urgency and prognosis.

Clinical Assessment
Newborn Screening
- Ortolani test (abduct, lift)
- Barlow test (adduct, push posteriorly)
- Assess hip stability
- Look for limb length discrepancy
- Asymmetric skin folds (less reliable)
All newborns should be screened.
Older Infant/Child
- Limited hip abduction (most reliable)
- Galeazzi sign (limb length)
- Asymmetric gluteal folds
- Trendelenburg gait (walking age)
- Late presentation more challenging
Limited abduction is key sign in older infant.
Click vs Clunk
Soft clicks are common and usually benign. A clunk (palpable hip movement) is significant. DDH is a clunk, not a click.
Differential Diagnosis
Distinguishing DDH from Mimics
| Condition | Distinguishing Features | Key Discriminator |
|---|---|---|
| DDH (idiopathic) | Positive Ortolani/Barlow in neonate; limited abduction and Galeazzi sign later; otherwise well child | Isolated unstable/dislocated hip with normal neurology |
| Teratologic dislocation | Fixed, irreducible dislocation present in utero; rigid hip; associated syndrome (arthrogryposis, myelomeningocele) | NOT reducible by Ortolani; stiff joint, abnormal neurology |
| Neuromuscular hip displacement (cerebral palsy, spina bifida) | Progressive subluxation due to spasticity/muscle imbalance; abnormal tone and reflexes | Underlying neurological diagnosis; develops over time, not congenital |
| Proximal focal femoral deficiency / coxa vara | Short limb with abnormal femoral anatomy on radiograph; hip may be high but acetabulum often near normal | Femoral segment shortening; radiographic femoral dysgenesis |
| Septic arthritis of the hip (infant) | Unwell, febrile, pseudoparalysis, pain on movement, raised inflammatory markers | Systemic sepsis and pain - an emergency, not DDH |
| Benign hip click | Soft high-pitched click from ligament/tendon, hip stable, no instability | Click without clunk; stable on Ortolani/Barlow |
Investigations
Hip Ultrasound
Timing:
- Screening at 4-6 weeks if risk factors
- Diagnostic if clinical suspicion
Graf Classification:
- Type I: Normal (alpha greater than 60)
- Type II: Immature/dysplastic
- Type III: Dislocated, labrum everted
- Type IV: Dislocated, labrum inverted
Alpha angle measures acetabular coverage.
Management Algorithm
Pavlik Harness

First-line treatment for newborn DDH:
- Maintains hip in flexion (100-110 degrees) and abduction (50-70 degrees)
- Full-time wear initially (23 hours/day)
- Weekly follow-up with ultrasound to confirm reduction
Success factors:
- Age at initiation: 90-95% if started under 6 weeks, decreases to 50% after 3 months
- Type of dysplasia: Better for Graf II-III, poorer for Graf IV (inverted labrum)
- Bilateral cases may need longer treatment
Duration: Until stable on ultrasound, typically 6-12 weeks full-time, then part-time weaning
Complications to monitor:
- Femoral nerve palsy (excessive flexion)
- Inferior epiphyseal ischemia (AVN from forced abduction)
- Skin irritation and pressure sores
Discontinue if: No reduction after 3-4 weeks (Pavlik disease risk - inverted labrum prevents reduction and worsens with continued harness use).
Surgical Techniques
Approaches
Medial approach (under 12 months):
- Avoids capsulorrhaphy
- Less dissection
- Appropriate for younger infants
Anterior (Smith-Petersen) approach:
- Better visualization
- Allows capsulorrhaphy
- For older children
Clear obstacles to reduction: psoas, transverse ligament, ligamentum teres.
Complications
| Complication | Incidence | Prevention/Management |
|---|---|---|
| AVN | 0-5% Pavlik, higher with surgery | Avoid forced abduction, safe zone |
| Residual dysplasia | 10-20% | Osteotomy at appropriate age |
| Redislocation | Variable | Adequate immobilization |
| Femoral nerve palsy (Pavlik) | Rare | Proper harness application |
AVN Prevention
Avoid forced abduction. Safe zone = angle of reduction to redislocation. Keep hip in middle of safe zone. Excessive abduction compresses lateral epiphyseal vessels.
Postoperative Care
DDH Recovery Timeline
Hip spica cast for 6-12 weeks. Position: abduction and flexion within safe zone. Cast changes as needed.
Spica cast 6-12 weeks post-reduction. Cast changes for growth. X-ray to confirm reduction maintained.
Transition to abduction brace for 2-3 months. Night-time wear. Promotes hip stability.
Regular X-rays to assess acetabular development. Monitor for residual dysplasia until skeletal maturity. May need future osteotomy.
Follow-up Key
Monitor acetabular index until skeletal maturity. Residual dysplasia may require pelvic osteotomy at appropriate age (Salter 18mo-6yrs, PAO adolescent).
Outcomes
Prognostic Factors
Better outcomes: Early diagnosis (under 6 weeks), Pavlik treatment, concentric reduction.
Worse outcomes: Late diagnosis, open reduction, AVN, residual dysplasia.
Treatment Outcomes by Age
- Diagnosis under 6 weeks: 90-95% success with Pavlik harness alone
- Diagnosis 3-6 months: 70-80% success with Pavlik; may need closed reduction
- Diagnosis 6-12 months: Often requires closed reduction + spica
- Diagnosis 12-18 months: Usually needs open reduction + spica
- Diagnosis over 18 months: Open reduction + pelvic osteotomy + femoral osteotomy
Long-Term Considerations
Children treated for DDH require follow-up until skeletal maturity:
- Acetabular development: Monitor acetabular index; residual dysplasia may need pelvic osteotomy
- Avascular necrosis: May not manifest for 6-12 months post-treatment
- Hip function: Most treated hips function normally if reduction achieved early
- Osteoarthritis risk: Higher with residual dysplasia or AVN; may need THR in adulthood
Avascular Necrosis Risk
AVN is the most feared complication with rates varying by treatment:
- Pavlik harness: 0-5% (with proper technique)
- Closed reduction: 5-15%
- Open reduction: 10-25%
- Risk factors: Excessive abduction, prolonged immobilization, older age at treatment
Prevention of Avascular Necrosis
Avoiding AVN requires adherence to established principles:
- Maintain safe zone of abduction (Ramsey criteria)
- Avoid forced or excessive abduction during treatment
- Consider femoral shortening in older children to reduce reduction pressure
- Monitor closely during treatment for signs of vascular compromise
Controversies and Areas of Uncertainty
Universal vs Selective Ultrasound
The central screening debate. Universal ultrasound detects more dysplasia but generates overtreatment without a proven reduction in late dislocation (Rosendahl RCT). German-speaking Europe favours universal US; most other programmes use selective US for risk factors. Reasonable practitioners still disagree.
Optimal First-Line Device
The Pavlik harness is the default, but systematic review evidence suggests rigid splints (von Rosen) may achieve comparable or better success with less residual dysplasia. No adequately powered RCT settles the question.
Role of the Ossific Nucleus
Whether to delay reduction until the femoral ossific nucleus appears (to lower AVN) is contested. Meta-analysis (Niziol 2017) found no consistent protective effect overall, challenging routine delay.
Pre-reduction Traction
Historical practice held that traction before reduction lowers AVN and improves reducibility. Several modern cohorts dispute any benefit, and many centres have abandoned it. Evidence remains low quality.
Concentric Reduction Over Forced Reduction
Across all controversies the unifying principle is unchanged: achieve a gentle, concentric, stable reduction within the safe zone and avoid forced abduction. Where reduction requires excessive force in an older child, femoral shortening is preferred to brute reduction.
Evidence Base
Universal vs Selective Ultrasound Screening (Bergen RCT)
- Randomised controlled trial of 11,925 newborns: universal US vs selective US vs clinical only
- Universal US raised the treatment rate to 3.4% vs 2.0% (selective) and 1.8% (clinical only)
- Late subluxation/dislocation 0.3 vs 0.7 vs 1.3 per 1000 - the reduction with universal US was NOT statistically significant (p=0.11)
- Universal US substantially increased diagnostic and follow-up effort for at best marginal late-case reduction
Pavlik Harness - Success and Complication Range (Systematic Review)
- Pavlik harness remains the gold-standard first-line device for the reducible neonatal hip
- Reported success rates range widely from 7% to 99%, driven by initial severity (Graf type), age and compliance
- Avascular necrosis reported between 0% and 28% - the most devastating harness complication
- Beta angle, dynamic coverage index and superior/lateral head displacement predict likelihood of harness success
Pitfalls in the Use of the Pavlik Harness
- Classic series of 18 problem hips treated in a Pavlik harness
- Most common failure (12 of the dislocated hips) was failure to achieve reduction, usually from improper physician application
- In several infants 3-5 months elapsed before lack of reduction was recognised
- AVN developed in 3 infants; poor harness quality and poor compliance compounded failures
Open vs Closed Reduction and AVN Risk (Meta-analysis)
- PRISMA meta-analysis of 9 observational studies in children under 3 years (reduction without osteotomy)
- Open reduction carried higher odds of all-grade AVN than closed reduction (pooled OR 2.26, 95% CI 1.21-4.22)
- Grade II-IV AVN trend higher with open reduction (OR 2.46) but not statistically significant (95% CI 0.93-6.51)
- Closed reduction was associated with greater need for further surgery (OR for open reduction 0.30)
Reliability of the Bucholz-Ogden AVN Classification
- Seven raters graded 39 hips by the Bucholz-Ogden osteonecrosis classification, twice
- Inter-rater reliability was only fair (kappa 0.34; 0.31 among the three surgeons)
- Raters disagreed on grade in 26 of 39 hips (67%), most often confusing grades I and II
- Authors recommend caution interpreting DDH outcome studies based on this classification
Comparison of Abduction Devices for DDH Under 6 Months
- Systematic review (modified Cochrane method, PRISMA) of 30 studies comparing 5 abduction devices
- Devices compared: Pavlik harness, von Rosen splint, Tubingen brace, Frejka pillow, Aberdeen splint
- The von Rosen splint was superior for success rate and lower residual dysplasia (p<0.05)
- Authors stress the evidence base is flawed and a randomised trial is warranted
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Newborn DDH
"A newborn girl born breech has a positive Ortolani test on the left hip. What is your diagnosis and management?"
Scenario 2: Late Presenting DDH
"An 18-month-old girl presents with a limp. She has limited left hip abduction and a positive Galeazzi sign. X-ray shows a dislocated left hip with a shallow acetabulum. How do you manage this?"
Scenario 3: Residual Dysplasia
"A 5-year-old female is seen for follow-up. She was treated with a Pavlik harness as an infant. She is asymptomatic. X-ray shows the Acetabular Index is 30 degrees (normal less than 20). What is your management?"
Scenario 4: Pavlik Harness Failure
"A 4-month-old infant with DDH has been in a Pavlik harness for 4 weeks. Repeat ultrasound shows the hip remains dislocated (Graf Type IV). What is your management?"
MCQ Practice Points
Ortolani Test
Q: What does a positive Ortolani test indicate? A: The hip is dislocated but reducible. Abduction with anterior pressure reduces the femoral head into the acetabulum.
Barlow Test
Q: What does a positive Barlow test indicate? A: The hip is unstable and can be dislocated. Adduction with posterior pressure causes the hip to dislocate.
Treatment Question
Q: What is first-line treatment for DDH under 6 months? A: Pavlik harness. 90-95% success if started under 6 weeks.
AVN Risk
Q: What increases AVN risk in DDH treatment? A: Forced abduction. Compresses lateral epiphyseal vessels. Keep within safe zone.
Graf Type IV
Q: What is the significance of Graf Type IV? A: Labrum inverted into acetabulum. Poor prognosis with Pavlik harness - often requires open reduction to clear the inverted limbus.
Residual Dysplasia
Q: A 5-year-old has acetabular index greater than 25 degrees. What surgery is indicated? A: Pelvic osteotomy (Salter or Pemberton). Redirects or reshapes acetabulum to improve coverage and prevent early OA.
Guidelines, Registries & Global Practice
Global Epidemiology
- Clinical instability at birth: approximately 1-3 per 1000 live births stabilise spontaneously, leaving roughly 1-2 per 1000 with true dysplasia or dislocation requiring treatment.
- Sonographic dysplasia is far more common (immature/dysplastic hips in up to 15-20% of healthy neonates on early ultrasound), which is why universal early ultrasound generates substantial overtreatment.
- Marked geographic variation: very high prevalence in populations that swaddle with the hips extended/adducted (some Indigenous North American, Eastern European and Middle Eastern groups); very low rates where babies are carried abducted/straddled (parts of sub-Saharan Africa and Southeast Asia).
- Risk factors (BFFF): breech presentation, female sex (about 4:1), first-born, positive family history; also oligohydramnios and other packaging deformities (congenital muscular torticollis, metatarsus adductus, talipes).
Screening Strategy - Side by Side
| Body / Region | Screening Approach | Practical Emphasis |
|---|---|---|
| USPSTF (US) | Concludes evidence is insufficient (I statement) to recommend universal screening | Avoids universal US given overtreatment; relies on clinical exam |
| AAP / POSNA (US) | Clinical exam of all newborns; selective US for risk factors or equivocal exam | Image at 6 weeks not before, to reduce false positives |
| UK NIPE / BOA (UK) | Universal clinical exam (newborn + 6-8 weeks); selective US for breech, family history or unstable exam | Structured national newborn examination programme |
| German-speaking Europe (Graf) | Universal ultrasound screening of all newborns | Highest detection but greatest treatment/follow-up burden |
Universal vs Selective Screening
Most English-speaking programmes use universal clinical examination plus selective ultrasound for risk factors; German-speaking Europe uses universal ultrasound. The Bergen RCT (Rosendahl, Pediatrics 1994) showed universal US increases treatment rates with only a marginal, non-significant reduction in late cases - the evidence basis for the selective approach.
Treatment Guidance - Side by Side
| Source | Key Recommendation | Notable Position |
|---|---|---|
| AAOS Clinical Practice Guideline | Surveillance of stable hips with risk factors acceptable; treat dislocated/dislocatable hips | Stops short of mandating universal US; emphasises shared decision-making |
| POSNA / IHDI | Pavlik or rigid abduction brace first-line under 6 months; staged surgery thereafter | Promotes 'safe' (abducted, flexed) swaddling to reduce DDH |
| NICE / BOA (UK) | Selective US, treat under specialist; emphasise early detection to avoid open surgery | Late presentation audited as a quality marker |
| AO / European paediatric consensus | Concentric reduction is the priority; femoral shortening over forced reduction in older children | Avoid forced abduction to limit AVN |
Registry and Surveillance Data
- DDH is tracked through national paediatric surveillance units (e.g. UK and Australian/New Zealand paediatric surveillance units) that monitor late-presenting DDH (diagnosed after the newborn period) as a key quality indicator of screening performance.
- Late-presentation rates of roughly 0.5-1.5 per 1000 persist even in well-resourced programmes, underscoring that no screening strategy eliminates missed cases.
- Unlike arthroplasty, there is no implant registry for paediatric DDH; long-term data come from osteotomy cohort follow-up rather than registries.
High- vs Limited-Resource Practice
High-Resource Settings
Newborn clinical screening with selective (or universal, in German-speaking Europe) ultrasound, early Pavlik/brace treatment, EUA with arthrogram for irreducible hips, and access to paediatric orthopaedic subspecialists. Most cases detected and treated non-operatively before walking age.
Limited-Resource Settings
Screening may be absent or clinical-only, so children frequently present late, at or after walking age, with established dislocation. Management shifts toward open reduction plus femoral shortening and pelvic osteotomy. Public-health messaging promoting abducted carrying/swaddling is a low-cost, high-impact intervention.
Prevention Through Swaddling
Hip-healthy (abducted, flexed) swaddling lowers DDH risk; tight extended-leg swaddling increases it. This is the single most generalisable, resource-independent preventive message and is endorsed by POSNA and the International Hip Dysplasia Institute.
DEVELOPMENTAL DYSPLASIA OF THE HIP
Clinical summary
Risk Factors (BFFF)
- •Breech presentation
- •Female (4:1)
- •First-born
- •Family history
- •Oligohydramnios
- •Torticollis/foot deformity
Examination
- •Ortolani: reduces dislocated hip
- •Barlow: dislocates unstable hip
- •Clunk (not click) is significant
- •Limited abduction (older infant)
- •Galeazzi sign (limb length)
- •Trendelenburg gait (walking age)
Imaging
- •US under 4-6 months (Graf)
- •X-ray after 4-6 months
- •Alpha angle measures coverage
- •Shenton line disrupted
- •Acetabular index elevated
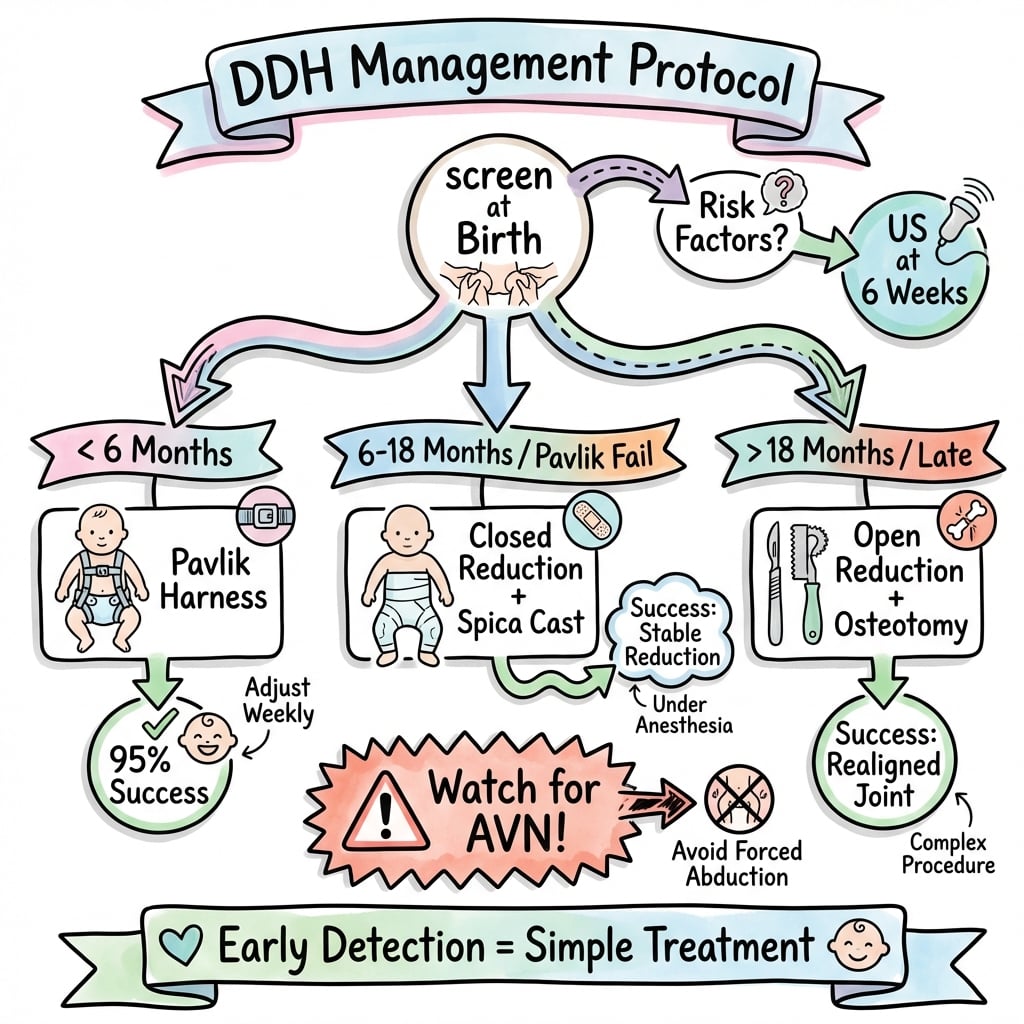
Treatment by Age
- •0-6 months: Pavlik harness
- •6-18 months: closed/open reduction
- •Walking age: open + osteotomy
- •Stop Pavlik if no reduction by 3-4 weeks
- •Femoral shortening for late cases
Pavlik Harness
- •Flexion 100-110 degrees
- •Abduction 50-70 degrees
- •90-95% success if under 6 weeks
- •Full-time wear initially
- •Weekly US follow-up
Complications
- •AVN (avoid forced abduction)
- •Residual dysplasia
- •Redislocation
- •Pavlik disease (late reduction)
- •Femoral nerve palsy