Wagner Classification | Texas Classification | Infection Control | Amputation Levels
Wagner Classification (Depth)
Critical Must-Knows
- Wagner classification = depth (0-5); Texas = depth + ischemia + infection
- Probe-to-bone test: positive likelihood ratio 6.4 for osteomyelitis
- IDSA guidelines: antibiotics for infection, NOT colonization
- Transtibial amputation has better healing (80-90%) than transmetatarsal (50-70%)
- Multidisciplinary team approach reduces amputation rate by 50%
Clinical Pearls
- "Texas classification adds ischemia/infection to Wagner depth grading
- "PEDIS system: Perfusion, Extent, Depth, Infection, Sensation
- "Offloading is THE critical treatment - total contact casting is gold standard
- "Major amputation mortality at 1 year: 30%; at 5 years: 50%
Clinical Imaging
Imaging Gallery



Critical Diabetic Foot Exam Points
Classification Systems
Know both Wagner AND Texas. Wagner = depth only (0-5). Texas = 4x4 grid (depth A-D, plus ischemia/infection grades 0-3). Examiners expect you to classify using BOTH systems and explain which guides treatment.
Infection vs Colonization
Antibiotics for infection, NOT colonization. IDSA criteria: purulence OR 2+ signs (warmth, erythema, lymphangitis, edema, pain). Swab cultures meaningless - tissue culture after debridement only.
Amputation Levels
Healing rates determine level. Toe: 90%, Ray: 80-90%, Transmetatarsal: 50-70%, Syme: 70-80%, Transtibial: 80-90%. Higher = better healing but worse function. Aim for most distal level with viable tissue.
Offloading
Offloading is treatment, not adjunct. Total contact casting reduces plantar pressure by 80-90%. Non-removable walker next best. Removable devices fail due to non-compliance. No offloading = no healing.
Quick Decision Guide: Wagner Classification
| Grade | Clinical Features | Treatment | Key Pearl |
|---|---|---|---|
| Grade 0 | Intact skin, callus, deformity | Prevention: orthotics, patient education | High-risk foot - prevent ulcer formation |
| Grade 1 | Superficial ulcer, no deeper structures | Offloading, sharp debridement, moist dressing | 90% heal with proper offloading alone |
| Grade 2 | Deep ulcer to tendon, bone, joint | Surgical debridement, antibiotics if infected | Probe-to-bone test - feel hard gritty bone |
| Grade 3 | Deep ulcer with abscess or osteomyelitis | Urgent surgical debridement, IV antibiotics | MRI if osteomyelitis uncertain - 90% sensitivity |
| Grade 4 | Forefoot gangrene (toes, metatarsals) | Partial foot amputation (toe, ray, transmetatarsal) | Revascularization first if ischemic |
| Grade 5 | Whole foot gangrene | Major amputation (Syme, transtibial, transfemoral) | 50% 5-year mortality - palliative care discussion |
Mnemonics and Memory Aids
WSTDAGWagner Classification (0-5 Depth)
| W | Well (Grade 0) Intact skin, high risk foot |
| S | Superficial (Grade 1) Ulcer without deeper structures |
| T | Tendon (Grade 2) Deep to tendon, capsule, or bone |
| D | Deep infection (Grade 3) Abscess or osteomyelitis |
| A | Anterior foot gangrene (Grade 4) Forefoot necrosis |
| G | Global foot gangrene (Grade 5) Whole foot necrosis |
| W | Well (Grade 0) Intact skin, high risk foot | T | Tendon (Grade 2) Deep to tendon, capsule, or bone | A | Anterior foot gangrene (Grade 4) Forefoot necrosis |
| S | Superficial (Grade 1) Ulcer without deeper structures | D | Deep infection (Grade 3) Abscess or osteomyelitis | G | Global foot gangrene (Grade 5) Whole foot necrosis |
Hook:Wagner Starts Treating Deep Abscesses Globally - each grade adds a layer of complexity!
WELPIDSA Infection Criteria
| W | Warmth Local temperature elevation |
| E | Erythema Redness extending beyond ulcer |
| L | Lymphangitis Red streaking proximally |
| P | Purulence Pus discharge from wound |
| W | Warmth Local temperature elevation | L | Lymphangitis Red streaking proximally |
| E | Erythema Redness extending beyond ulcer | P | Purulence Pus discharge from wound |
Hook:When you need hELP, look for infection signs - purulence OR 2+ of WELP!
TRSTAmputation Level Selection
| T | Toe (90%) Single or multiple toe amputation |
| R | Ray (80-90%) Toe plus metatarsal resection |
| S | Syme (70-80%) Ankle disarticulation |
| T | Transtibial (80-90%) Below-knee amputation |
| T | Toe (90%) Single or multiple toe amputation | S | Syme (70-80%) Ankle disarticulation |
| R | Ray (80-90%) Toe plus metatarsal resection | T | Transtibial (80-90%) Below-knee amputation |
Hook:TRuST the healing rates - higher level = better healing but worse function!
PEDISPEDIS Classification System
| P | Perfusion Arterial supply assessment |
| E | Extent Ulcer size and location |
| D | Depth Tissue layers involved |
| I | Infection Signs of infection present |
| S | Sensation Neuropathy severity |
| P | Perfusion Arterial supply assessment | I | Infection Signs of infection present |
| E | Extent Ulcer size and location | S | Sensation Neuropathy severity |
| D | Depth Tissue layers involved |
Hook:PEDIS walks you through systematic foot ulcer assessment - used in research!
Overview and Epidemiology
Why Diabetic Foot Matters
Diabetic foot disease is the leading cause of non-traumatic lower limb amputation worldwide. The pooled global prevalence of diabetic foot ulceration is about 6.3%, and the lifetime risk of an ulcer in a person with diabetes is estimated at 19-34% (Armstrong, NEJM 2017). The combination of neuropathy (trauma without pain awareness) and peripheral arterial disease (impaired healing) creates a perfect storm, and 5-year mortality after an ulcer rivals that of several common cancers. Multidisciplinary care reduces amputation rates by roughly 50% - making this a global public health priority.
Pathophysiology Triad
Neuropathy: Loss of protective sensation - patients don't feel injuries. Motor neuropathy causes intrinsic muscle atrophy, leading to claw toes and pressure points.
Ischemia: Peripheral arterial disease affects tibial vessels preferentially. Calcified vessels reduce perfusion.
Infection: Polymicrobial, often involving anaerobes. Biofilm formation prevents healing.
Together, these create chronic non-healing ulcers.
Global Burden
Epidemiology (Zhang 2017; Armstrong 2017):
- Pooled global ulcer prevalence 6.3% (highest North America 13%, lowest Oceania 3%)
- Lifetime ulcer risk in diabetes 19-34%
- Recurrence ~40% at 1 year, ~65% at 5 years after healing
- Diabetic foot is the commonest cause of non-traumatic amputation worldwide
Equity gap: Indigenous and lower-resource populations carry a disproportionately high amputation burden.
Key message: Prevention and early intervention are cost-effective everywhere.
Pathophysiology and Mechanisms
Neuropathic Changes
Sensory neuropathy: Loss of protective sensation (LOPS) - patients don't feel injuries. 10g monofilament test diagnostic.
Motor neuropathy: Intrinsic muscle atrophy leads to imbalanced forces - claw toes, prominent metatarsal heads, high plantar pressure.
Autonomic neuropathy: Dry skin (anhidrosis) leads to cracks and fissures - entry points for infection.
Charcot neuroarthropathy: Repetitive microtrauma without pain leads to bone/joint destruction.
Neuropathy removes pain as a warning signal - injuries go unnoticed.
Vascular Changes
Peripheral arterial disease: Preferential involvement of tibial vessels (anterior tibial, posterior tibial, peroneal). Spares profunda femoris.
Medial calcification (Monckeberg sclerosis): Calcium deposits in arterial media - non-obstructive but reduces vessel compliance. Makes ABI falsely elevated.
Microvascular disease: Thickened capillary basement membrane reduces oxygen diffusion.
Impaired angiogenesis: Diabetic wounds have reduced VEGF response, poor collateral formation.
Ischemia prevents healing even when infection controlled.
Biomechanics of Plantar Ulceration
Normal plantar pressure: 200-300 kPa. In diabetic foot with neuropathy and motor imbalance, pressure at metatarsal heads increases to 700-1000 kPa (7-10 times higher). Callus forms as protective response but increases local pressure further (callus is THICK and non-compressible). Repetitive high pressure + loss of sensation = ulcer formation at pressure points. This is WHY offloading (TCC) is critical - reduces pressure by 80-90% to below ulceration threshold.
Foot Deformities and Ulcer Risk
| Deformity | Mechanism | High-Risk Zone | Prevention |
|---|---|---|---|
| Claw toes | Intrinsic muscle atrophy, unopposed long extensors/flexors | Plantar metatarsal heads, dorsal PIP joints | Achilles lengthening, toe straightening, custom orthotics |
| Charcot midfoot collapse | Bone/joint destruction from repetitive trauma without pain | Medial midfoot (rocker-bottom deformity) | Total contact casting during acute phase, custom AFO |
| Hallux valgus | Bunion formation, first MTP prominence | Medial first MTP, plantar first metatarsal head | Wide toe-box shoes, bunion pads, surgical correction if severe |
| Pes cavus (high arch) | Fixed deformity, concentrated pressure points | Plantar heel, metatarsal heads, lateral border | Custom molded orthotics redistributing pressure |
Classification Systems
Wagner Classification (Depth-Based)
The original and most widely used system. Simple, reproducible, focuses on ulcer depth and tissue involvement.
| Grade | Definition | Clinical Features | Treatment Approach |
|---|---|---|---|
| Grade 0 | Intact skin at risk | Callus, deformity, Charcot foot, prior ulcer | Prevention: custom orthotics, patient education, regular foot checks |
| Grade 1 | Superficial ulcer | Partial or full thickness skin loss, no deeper structures visible | Offloading (total contact cast), sharp debridement, moist dressing |
| Grade 2 | Deep ulcer to bone/tendon | Ulcer extends to ligament, tendon, joint capsule, or bone | Surgical debridement, probe-to-bone test, consider antibiotics |
| Grade 3 | Deep with abscess/osteomyelitis | Deep-tissue abscess, osteomyelitis, or septic arthritis | Urgent surgical debridement, IV antibiotics, prolonged therapy |
| Grade 4 | Localized gangrene | Necrosis of forefoot (toes, metatarsals), demarcated | Partial foot amputation (toe, ray, transmetatarsal) |
| Grade 5 | Extensive gangrene | Necrosis involving entire foot, not salvageable | Major amputation (transtibial, transfemoral) |
Wagner Limitations
Wagner classification does NOT account for ischemia or infection severity. A Wagner Grade 2 ulcer can be clean without infection, or it can have severe necrotizing fasciitis. Similarly, perfusion status (critical limb ischemia vs adequate flow) dramatically affects healing. This led to development of Texas and PEDIS classifications.
Wagner classification guides treatment urgency and predicts amputation risk.
Clinical Assessment
History
Diabetes control: HbA1c, duration of diabetes, complications
Ulcer timeline: When first noticed, progression, prior ulcers
Symptoms: Pain (neuropathic vs ischemic), numbness, tingling
Function: Walking ability, distance before claudication
Red flags: Fever, rigors, confusion (systemic infection)
Social: Living situation, mobility, compliance capacity
Neuropathic ulcers are painless - ischemic ulcers are painful.
Examination
Inspection: Ulcer location (pressure points), size, depth, base (granulation vs slough vs necrotic), edge (undermined, callused)
Perfusion: Pulses (DP, PT), capillary refill, temperature, ABI, toe pressure
Sensation: 10g monofilament (LOPS), vibration (tuning fork), proprioception
Infection signs: Erythema extent (measure and mark), warmth, purulence, lymphangitis, crepitus
Probe-to-bone test: Sterile probe inserted - if bone felt (hard, gritty), osteomyelitis likely
Always examine the contralateral foot for risk assessment.
Probe-to-Bone Test - The 6.4 Likelihood Ratio
The probe-to-bone test has a positive likelihood ratio of 6.4 for osteomyelitis (Grayson et al, JAMA 1995). If bone is felt with a sterile probe, the probability of osteomyelitis increases substantially. However, negative test does NOT exclude osteomyelitis - MRI is gold standard if clinical suspicion remains high. The test is operator-dependent and requires adequate debridement first.
Neuropathic vs Ischemic Ulcers
| Feature | Neuropathic | Ischemic |
|---|---|---|
| Pain | Painless (loss of protective sensation) | Painful, worse with elevation, relieved by dependency |
| Location | Plantar pressure points (metatarsal heads, heel) | Distal tips of toes, lateral malleolus, heel |
| Ulcer appearance | Deep, punched out, surrounded by callus | Shallow, irregular, pale base, no callus |
| Skin | Warm, dry (autonomic neuropathy), good pulses | Cool, hairless, atrophic, absent pulses |
| Healing capacity | Good if offloaded and infection controlled | Poor without revascularization |
Differential Diagnosis of the Diabetic Foot Presentation
| Condition | How it mimics | Key discriminator | Confirmatory test |
|---|---|---|---|
| Acute Charcot neuroarthropathy | Warm, swollen, erythematous foot - looks like infection or cellulitis | Often no ulcer/portal of entry; erythema settles on elevation; bony deformity | X-ray (fragmentation/dislocation), MRI bone oedema, temperature difference greater than 2°C |
| Osteomyelitis vs uninfected deep ulcer | Deep ulcer probing to bone without systemic signs | Probe-to-bone positive, chronicity, sausage toe, raised ESR | MRI (90% sensitive) and bone biopsy with culture/histology |
| Cellulitis / soft-tissue infection | Spreading erythema and warmth | Diffuse, no underlying bone involvement, responds to antibiotics | Clinical; tissue culture; imaging to exclude deep collection |
| Acute gout / crystal arthropathy | Hot, red, painful first MTP joint | Severe pain (preserved sensation), rapid onset, prior attacks | Serum urate, joint aspirate for negatively birefringent crystals |
| Deep vein thrombosis | Unilateral swelling, warmth, erythema | Calf involvement, no ulcer, risk factors | Duplex ultrasound, D-dimer |
| Pure ischaemic / venous / pressure ulcer | Non-healing ulcer in a diabetic | Location and surrounding skin (tips/lateral vs gaiter vs heel), pulses, oedema | ABI/TBI, toe pressure, venous duplex |
Investigations
Investigation Protocol
Monofilament test: 10g Semmes-Weinstein at 9 sites. Unable to feel at 4 or more sites = LOPS.
Probe-to-bone: After debridement, sterile probe inserted. Hard gritty sensation = bone.
Capillary glucose: Assess current control, guide insulin therapy.
These simple tests guide immediate treatment decisions.
Ankle-Brachial Index (ABI): 0.9-1.3 normal. Less than 0.9 suggests PAD. Greater than 1.3 suggests calcified vessels (common in diabetes - use toe pressure instead).
Toe-Brachial Index (TBI): More reliable in diabetes. TBI less than 0.6 suggests critical ischemia.
Toe Pressure: Less than 30 mmHg = critical ischemia, revascularization needed.
TcPO2 (transcutaneous oxygen): Less than 30 mmHg suggests poor healing potential.
Duplex ultrasound: If abnormal non-invasive studies, map arterial disease for revascularization planning.
Vascular assessment is ESSENTIAL - determines if healing is possible.
Plain radiographs (AP, lateral, oblique): Look for gas in soft tissues (necrotizing infection), bone destruction (osteomyelitis), Charcot changes (fragmentation, dislocation).
MRI (gold standard for osteomyelitis): Sensitivity 90%, specificity 80%. T1-weighted: dark signal in bone marrow. T2/STIR: bright signal. Gadolinium enhancement.
CT with contrast: If MRI contraindicated. Less sensitive for osteomyelitis but good for surgical planning.
Nuclear medicine (WBC scan): If MRI/CT inconclusive. Labeled WBC accumulate in infection.
MRI is gold standard but plain films are first-line screening.
HbA1c: Assess glycemic control over 3 months. Target less than 7% for healing.
FBC: Leukocytosis suggests systemic infection. Anemia common in chronic disease.
CRP/ESR: Elevated in infection (CRP more specific, ESR more sensitive). Trend to assess response.
Renal function (eGFR): Diabetic nephropathy common, affects antibiotic dosing.
Blood cultures: If systemic signs (fever, rigors, tachycardia, hypotension).
Tissue culture (post-debridement): Deep tissue specimen after debridement. Swab cultures unreliable.
Laboratory markers guide antibiotic choice and duration.
Osteomyelitis Diagnosis Triad
Q: What is the diagnostic triad for diabetic foot osteomyelitis?
A: (1) Probe-to-bone test positive (positive LR 6.4), (2) ESR greater than 70 mm/h (sensitivity 28%, specificity 92%), and (3) Plain radiograph showing bone destruction (late sign, 50% sensitive). MRI is gold standard (90% sensitive, 80% specific) but requires all three clinical features for high pre-test probability. Bone biopsy with culture is definitive but rarely needed.
Management Algorithm
Wagner Grade 0-1 Algorithm
Grade 0: Intact skin at high risk
Prevention Protocol
IWGDF Risk Categories:
- Low: Normal sensation + pulses
- Moderate: LOPS OR PAD
- High: LOPS + PAD, or prior ulcer/amputation
All diabetics need annual screening.
Daily foot inspection (use mirror for plantar surface)
Proper footwear: Avoid barefoot walking, check inside shoes daily for foreign objects
Immediate reporting: New wounds, redness, warmth, drainage
Nail care: Straight across, podiatry referral for thick nails
Education reduces ulcer incidence by 30-50%.
Regular podiatry: Callus debridement, nail care
Custom orthotics: Redistribute pressure (reduces recurrence 50%)
Accommodative footwear: Extra depth shoes, rocker soles
Prophylactic surgery: Consider Achilles lengthening if persistent forefoot overload
Prevention is most cost-effective intervention.
Grade 1: Superficial ulcer
Treatment Protocol
Sharp debridement: Remove ALL callus and slough to bleeding base
Offloading: Total contact cast (gold standard) or instant TCC
Wound dressing: Moist environment (hydrocolloid, foam, hydrogel)
No antibiotics unless signs of infection
90% heal with proper offloading alone.
Debridement: Repeat weekly or more if needed
Measure ulcer: Length × width, photograph for documentation
Assess healing: 50% size reduction by 4 weeks predicts healing
Monitor infection: Any new erythema, purulence, warmth
Most heal in 6-12 weeks with compliant offloading.
Re-evaluate: Check compliance with offloading, glucose control, nutrition
Rule out osteomyelitis: Probe-to-bone, plain X-ray, consider MRI
Vascular assessment: If not already done - ABI, toe pressure
Consider advanced therapy: VAC, bioengineered skin if appropriate
Non-healing suggests underlying problem - don't just continue same treatment.
Prevention and early treatment prevent progression to deeper grades.
Infection Management
Infectious Diseases Society of America (IDSA) Classification
| Severity | Clinical Features | Microbiology | Antibiotic Duration |
|---|---|---|---|
| Uninfected | No purulence or inflammation | Colonization only (do NOT treat) | No antibiotics |
| Mild | Local infection: erythema less than 2 cm from ulcer edge, superficial | Gram-positive (S. aureus, Streptococcus) | 1-2 weeks oral antibiotics |
| Moderate | Local infection: erythema greater than 2 cm, OR deep tissue involvement | Polymicrobial (add Gram-negative) | 2-3 weeks (IV initially, then oral) |
| Severe | Systemic signs (SIRS) OR metabolic instability | Polymicrobial + anaerobes | 4-6 weeks IV antibiotics, may need longer |
IDSA Key Principle: Infection Requires Treatment, Colonization Does Not
Infection diagnosis requires: Purulence OR 2 or more of: warmth, erythema, lymphangitis, edema, pain. A diabetic foot ulcer with bacteria on swab but NO signs of infection is COLONIZED, not infected. Antibiotics treat infection, NOT colonization. Swab cultures are unreliable - tissue biopsy after debridement is gold standard for culture.
IDSA guidelines are the international standard for diabetic foot infection management.
Surgical Management and Amputation Levels
Toe and Ray Amputations
Partial Foot Amputation Levels
| Level | Indications | Healing Rate | Functional Impact |
|---|---|---|---|
| Toe (single) | Isolated toe gangrene, osteomyelitis confined to phalanx | 90% | Minimal - great toe removal affects push-off slightly |
| Ray (toe + metatarsal) | Osteomyelitis involving metatarsal, web space infection | 80-90% | Good if single ray; multiple rays cause transfer lesions |
| Transmetatarsal (TMA) | Forefoot gangrene, multiple ray involvement, salvageable hindfoot | 50-70% | Requires orthotics, equinus deformity risk |
| Lisfranc (tarsometatarsal) | Extensive forefoot necrosis, Charcot midfoot | 40-60% | Poor function, high revision to BKA rate |
Surgical Principles:
Adequate Resection
- Resect all infected/necrotic tissue until bleeding healthy bone
- Leave no exposed bone at amputation site
- Create viable soft tissue flap for coverage
- Avoid tension on closure
Incomplete resection leads to failure.
Perfusion Assessment
- Toe pressure greater than 30 mmHg predicts healing
- TcPO2 greater than 30 mmHg at amputation level
- Bleeding bone ends (paprika sign)
- Consider revascularization first if borderline
Ischemic tissue will not heal - revascularize first.
Transmetatarsal Amputation (TMA) Key Point
TMA preserves weight-bearing on plantar hindfoot but requires adequate perfusion (toe pressure greater than 40 mmHg). Post-TMA, Achilles tendon is relatively stronger than dorsiflexors, causing equinus deformity. Patients need custom ankle-foot orthosis (AFO) or rocker-bottom shoe to prevent plantar ulceration at the stump. Failure to offload = new ulcer = revision to BKA.
Partial foot amputations preserve length but require good perfusion.
Complications
| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| Recurrent ulceration | 30-40% at 1 year, 60-70% at 5 years | Continued neuropathy, poor offloading, non-compliance | Lifelong foot surveillance, custom orthotics, patient education |
| Osteomyelitis | 20-30% of deep ulcers (Wagner 2+) | Probe-to-bone positive, chronic ulcer over 2 weeks | Surgical debridement (curative) or 6-12 weeks antibiotics |
| Charcot neuroarthropathy | 0.1-0.9% of diabetics annually | Peripheral neuropathy, trauma (often unrecognized) | Acute phase: TCC immobilization; chronic: custom AFO, possible fusion |
| Amputation wound breakdown | 15-30% (higher in TMA) | Ischemia, infection, tension on closure, malnutrition | Debridement, VAC therapy, revision to higher level if needed |
| Contralateral limb ulcer/amputation | 30-50% at 3 years | Bilateral neuropathy and PAD, increased weight-bearing on contralateral side | Aggressive surveillance, bilateral offloading, glycemic control |
| Sepsis and mortality | 5-10% of severe infections | Necrotizing infection, delayed treatment, immunocompromised | ICU admission, source control, broad-spectrum antibiotics, organ support |
| Phantom limb pain | 50-80% post-amputation | Pre-amputation pain, acute trauma, inadequate analgesia | Gabapentin, pregabalin, mirror therapy, TENS, psychological support |
| Psychological distress | 30-50% (depression, anxiety) | Loss of limb, loss of independence, chronic illness burden | Screen for depression, psychology referral, peer support groups |
Recurrent Ulceration is the Norm, Not the Exception
Even after successful ulcer healing, 60-70% of diabetic patients develop a new ulcer within 5 years. This is because the underlying pathology (neuropathy, ischemia, biomechanical abnormalities) persists. Lifelong surveillance and prevention are essential - custom orthotics reduce recurrence by 50% but patient compliance is challenging. Every healed ulcer patient needs a prevention plan.
Charcot Foot Recognition
Acute Charcot: Warm, swollen, red foot in a neuropathic diabetic - easily mistaken for infection or DVT. Key difference: X-ray shows bone fragmentation and joint dislocation (not normal in infection). MRI shows bone edema. Management is NON-weight-bearing with TCC for 3-6 months until temperature difference less than 2°C. Walking on an acute Charcot foot causes irreversible deformity. Chronic Charcot with rocker-bottom deformity needs custom AFO or possible reconstructive surgery (realignment arthrodesis).
Postoperative Care and Rehabilitation
After Surgical Debridement or Minor Amputation
Wound Healing Timeline
Wound management: Open wound packed with gauze soaked in saline or antiseptic
Offloading: Total contact cast or non-weight-bearing
Antibiotics: Continue culture-directed antibiotics (duration based on infection severity)
Glucose control: Target glucose 6-10 mmol/L (hyperglycemia impairs healing)
Nutrition: High-protein diet, vitamin C and zinc supplementation
DVT prophylaxis: LMWH if not ambulating
Initial phase focuses on infection control and wound preparation.
Serial debridement: Return to OR or bedside debridement if necrotic tissue appears
VAC therapy: Consider for deep wounds - promotes granulation, reduces edema
Dressing changes: Daily to every 2-3 days based on exudate
Monitor healing: Wound measurements, photographs, signs of infection
Mobilization: Non-weight-bearing or protected weight-bearing with device
Granulation tissue should appear by week 1-2.
Wound contraction: Measure weekly - expect 50% reduction by 4 weeks
Secondary healing vs closure: Small wounds heal by secondary intention; large wounds may need skin graft or flap
Progressive weight-bearing: Gradual transition from non-weight-bearing to protected weight-bearing
Rehabilitation: ROM exercises, gait training
Most wounds heal or are ready for closure by 4-6 weeks.
Custom orthotics: Once healed, custom insoles to prevent recurrence
Accommodative footwear: Extra depth shoes with rocker soles
Surveillance: Monthly podiatry for first 3 months, then every 3 months
Patient education: Daily foot checks, immediate reporting of new problems
Transition to prevention mode - recurrence is common.
Post-debridement care is intensive and prolonged - requires patient commitment.
Outcomes and Prognosis
Prognostic Factors for Healing
| Factor | Good Prognosis | Poor Prognosis |
|---|---|---|
| Perfusion | Toe pressure greater than 40 mmHg, palpable pulses | Toe pressure less than 30 mmHg, critical ischemia |
| Infection | Uninfected or mild infection | Severe infection with systemic signs, osteomyelitis |
| Ulcer size | Less than 2 cm diameter | Greater than 5 cm diameter (longer healing time) |
| Ulcer duration | Less than 2 weeks | Greater than 3 months (chronic wound, biofilm) |
| Glycemic control | HbA1c less than 7.5% | HbA1c greater than 10% (impaired healing) |
| Nutrition | Albumin greater than 35 g/L | Albumin less than 30 g/L (malnutrition) |
| Compliance | Adheres to offloading and follow-up | Non-compliant (removes devices, misses appointments) |
Predictors of Poor Outcome
Key predictors of amputation or mortality:
- Texas D3 classification (infected + ischemic): 50% amputation risk at 1 year
- Chronic kidney disease (eGFR less than 30): Doubles mortality risk
- Cardiac disease (prior MI, CCF): Major cause of death post-amputation
- Age greater than 75 years: Higher perioperative mortality, lower rehabilitation potential
- Albumin less than 30 g/L: Marker of malnutrition and frailty
Patients with 3 or more of these factors have very poor prognosis - palliative care discussion essential.
Survival After Major Amputation
Mortality rates (Aulivola 2004):
- 30-day: BKA 10%, AKA 15%
- 1-year: 30%
- 3-year: 40%
- 5-year: 50%
Causes of death: Cardiac disease (50%), stroke (15%), renal failure (10%), sepsis (10%)
Comparison: Similar to many Stage III cancers
Major amputation is a marker of advanced systemic disease.
Quality of Life
Functional outcomes:
- BKA: 60-80% ambulate with prosthesis
- AKA: 30-50% ambulate with prosthesis
- Bilateral: Less than 20% ambulate
Independence: 40-60% maintain independent living
Return to work: Less than 20% if working before amputation
Depression: 30-50% meet criteria for major depression
QoL impairment is substantial - psychological support essential.
Discussing Prognosis with Patients
Many patients and families do not understand the poor prognosis after major amputation. It is our responsibility to explain: "After a below-knee amputation, about 1 in 3 patients will have died within 1 year, and about half within 5 years. Most deaths are from heart disease or stroke. About 6-8 out of 10 patients will be able to walk with a prosthetic leg, but it requires months of rehabilitation. Some patients may choose to focus on quality of life rather than limb salvage attempts." Document these discussions carefully for medicolegal protection.
Offloading and Wound Care
Offloading is Treatment, Not Adjunct
Offloading reduces plantar pressure by 80-90% and is THE most important intervention for plantar diabetic foot ulcers. Total contact casting (TCC) is gold standard. Removable devices (CAM walker, half-shoe) fail due to non-compliance - patients remove them at home. Non-removable devices work. Without offloading, ulcers do NOT heal regardless of other treatments.
Offloading Modalities
| Method | Pressure Reduction | Compliance | Indications |
|---|---|---|---|
| Total Contact Cast (TCC) | 80-90% | 100% (non-removable) | Gold standard for plantar neuropathic ulcers |
| Instant Total Contact Cast (iTCC) | 75-85% | 100% (non-removable) | Fiberglass wrap over CAM walker - easier application |
| CAM walker (removable) | 30-50% | 30-50% (patients remove it) | Non-plantar ulcers, patient preference (but expect failure) |
| Custom orthotics | 20-40% | Variable | Prevention (Grade 0), healed ulcer recurrence prevention |
| Felted foam padding | 40-60% | Good (adhesive keeps in place) | Adjunct to other modalities, small ulcers |
Wound Care Principles:
Sharp Debridement
- Remove all callus, slough, necrotic tissue
- Debride to bleeding healthy tissue
- Perform weekly or more frequently
- Send deep tissue for culture if infected
Debridement converts chronic to acute wound.
Moist Wound Healing
- Avoid dry gauze (desiccates wound bed)
- Use hydrogel, hydrocolloid, foam, alginate
- Select based on exudate level
- Change per manufacturer instructions
Moist environment promotes epithelialization.
Negative Pressure (VAC)
- For deep wounds post-debridement
- Promotes granulation tissue
- Reduces edema and bacterial load
- Change every 48-72 hours
VAC is adjunct, not replacement for debridement.
Advanced Therapies
- Hyperbaric oxygen: Controversial, limited evidence
- Growth factors (becaplermin): Modest benefit
- Bioengineered skin: Apligraf, Dermagraft
- Stem cells: Experimental
Most advanced therapies have limited evidence.
Multidisciplinary Team Approach
Multidisciplinary Care Reduces Amputations by 50%
Evidence from multiple RCTs and cohort studies shows that multidisciplinary diabetic foot clinics reduce major amputation rates by 50% compared to usual care. Key is coordination between podiatry, vascular surgery, endocrinology, infectious disease, orthopaedics, and rehabilitation. Weekly team meetings to review complex cases improve outcomes.
Core Team Members
Podiatrist: Wound assessment, debridement, offloading
Vascular surgeon: Revascularization assessment
Endocrinologist: Glucose control optimization
Infectious disease: Antibiotic stewardship
Orthopaedic surgeon: Amputation, Charcot reconstruction
Each discipline contributes specialized expertise.
Support Services
Diabetes educator: Self-management training
Dietitian: Nutrition optimization
Physiotherapist: Mobility, gait training
Occupational therapist: ADL adaptation
Prosthetist: Post-amputation limb fitting
Support services enable independence.
System Level
Outpatient clinic: Weekly multidisciplinary rounds
Inpatient service: Acute admissions, surgical cases
Home nursing: Wound care, monitoring
Community liaison: Ensure follow-up compliance
Database: Track outcomes, quality improvement
Organized systems deliver coordinated care.
Prevention Strategies
Diabetic Foot Prevention Protocol
Risk stratification using IWGDF categories:
- Low risk: Normal sensation, palpable pulses
- Moderate risk: LOPS or PAD (not both)
- High risk: LOPS + PAD, or prior ulcer/amputation
Examination: Monofilament, pulses, deformity, callus, footwear
Screen all diabetics annually - identify high-risk feet.
Daily foot inspection: Use mirror to check plantar surface
Immediate reporting: Any new wound, redness, warmth
Footwear: Proper fit, avoid barefoot walking, check inside shoes daily
Nail care: Straight across, no self-treatment of callus
Education empowers patients to prevent ulcers.
Regular debridement: Callus removal every 4-6 weeks
Custom orthotics: Redistribute pressure away from high-risk areas
Accommodative footwear: Extra depth, cushioned insoles
Prophylactic surgery: Consider Achilles lengthening if forefoot overload
Podiatry reduces ulcer incidence in high-risk feet.
Target HbA1c less than 7% for most patients
Avoid hypoglycemia: Relaxed targets in elderly (less than 8%)
Multifactorial risk reduction: BP, lipids, smoking cessation
Good diabetes control prevents neuropathy progression.
Evidence Base and Key Trials
Guidelines on the Prevention of Foot Ulcers in Persons with Diabetes (IWGDF 2019 update)
- GRADE-based international guideline; supersedes the 2015 IWGDF prevention guideline
- Screen very-low-risk patients annually for loss of protective sensation and PAD; screen higher-risk patients more frequently
- Prescribe therapeutic footwear with a demonstrated plantar-pressure-relieving effect to prevent recurrence of plantar ulcers
- Provide integrated foot care for high-risk patients to prevent ulcer recurrence
- Suggests against nerve decompression procedures for prevention
Irremovable vs Removable Cast Walkers for Diabetic Foot Wounds (Armstrong 2005 RCT)
- RCT: 50 patients with University of Texas grade 1A neuropathic plantar ulcers
- 12-week healing (intention-to-treat): instant total contact cast (iTCC) 82.6% vs removable cast walker 51.9% (P = 0.02)
- Among healed ulcers, iTCC healed faster: 41.6 vs 58.0 days (P = 0.02)
- Rendering a removable walker irremovable enforces adherence and improves healing
2012 Infectious Diseases Society of America Clinical Practice Guideline for Diabetic Foot Infections
- Infection defined by 2 or more classic signs of inflammation or purulence; all wounds are colonised, so colonisation alone is not treated
- Severity classification: uninfected, mild, moderate, severe - drives admission, imaging and surgery decisions
- Obtain a post-debridement tissue specimen for aerobic and anaerobic culture; swabs are unreliable
- MRI is far more sensitive and specific than plain films for osteomyelitis; bone culture plus histology is the optimal standard
- Multidisciplinary foot teams improve outcomes
Major Lower Extremity Amputation: Outcome of a Modern Series (Aulivola 2004)
- Retrospective series of 959 major amputations in 788 patients (704 BKA, 255 AKA)
- Overall 30-day mortality 8.6%; worse for AKA (16.5%) than BKA (5.7%)
- Overall survival 69.7% at 1 year and 34.7% at 5 years
- Survival worse with diabetes (30.9% at 5 years) and end-stage renal disease (14.4% at 5 years)
- Only 9.4% of BKAs required conversion to AKA
Global Epidemiology of Diabetic Foot Ulceration: Systematic Review and Meta-analysis (Zhang 2017)
- Global pooled diabetic foot ulcer prevalence 6.3% (95% CI 5.4-7.3%)
- Higher in men (4.5%) than women (3.5%), and in type 2 (6.4%) than type 1 (5.5%) diabetes
- Marked regional variation: North America 13.0%, Africa 7.2%, Asia 5.5%, Europe 5.1%, Oceania 3.0%
- Ulcer patients were older, had longer diabetes duration, and more hypertension, retinopathy and smoking
Diabetic Foot Ulcers and Their Recurrence (Armstrong, Boulton & Bus 2017)
- Authoritative review: lifetime incidence of foot ulcers in diabetes is estimated at 19-34%
- Recurrence is the norm - roughly 40% within 1 year and around 65% within 5 years of healing
- Five-year mortality after a diabetic foot ulcer is comparable to several common cancers
- Offloading, structured prevention and integrated foot care are the cornerstones of reducing recurrence
Probing to Bone in Infected Pedal Ulcers: A Clinical Sign of Osteomyelitis (Grayson 1995)
- Prospective study of 76 infected pedal ulcers in 75 hospitalised diabetic patients
- Palpable bone on probing had 66% sensitivity and 85% specificity for osteomyelitis
- Positive predictive value 89% in this high-prevalence (66%) inpatient population
- A positive probe-to-bone test makes additional imaging often unnecessary in this setting
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Wagner Classification and Initial Management (2-3 min)
"A 62-year-old man with type 2 diabetes (duration 15 years) presents with a 3-week history of a non-healing ulcer on the plantar aspect of his right first metatarsal head. He has no pain but noticed drainage on his sock. On examination, there is a 2 cm diameter ulcer with surrounding callus. You probe the ulcer and feel bone. There is no erythema beyond 1 cm from the ulcer edge, no purulent discharge. Pulses are palpable. What is your assessment and management?"
Scenario 2: Infected Diabetic Foot with Ischemia (3-4 min)
"A 70-year-old woman with diabetes presents with 48 hours of worsening right foot pain, swelling, and fevers (38.5°C). She has a chronic ulcer on her lateral forefoot. On examination, there is extensive erythema to mid-foot, purulent discharge, and crepitus in the forefoot. Her foot is cool with absent DP and PT pulses. Her WCC is 18, CRP 250. Plain radiograph shows gas in soft tissues and bone destruction of the 4th and 5th metatarsals. How would you manage this patient?"
Scenario 3: Amputation Level Selection (2-3 min)
"You have performed extensive debridement for forefoot gangrene in a 68-year-old diabetic man. After removing the 1st, 2nd, and 3rd rays, the residual foot has viable hindfoot tissue but questionable perfusion. Toe pressure is 32 mmHg. The patient asks whether you will be able to save the remaining foot or if he needs a below-knee amputation. How do you counsel him and what determines your decision?"
MCQ Practice Points
Classification Question
Q: A diabetic foot ulcer extending to bone but without signs of infection or ischemia is which Texas classification?
A: Texas C0 (depth grade C = penetrates to bone, stage 0 = no infection and no ischemia). This is equivalent to Wagner Grade 2 but with the added information that there is no infection or ischemia. Treatment is surgical debridement and offloading, with imaging to rule out osteomyelitis.
Infection Diagnosis Question
Q: What are the IDSA diagnostic criteria for diabetic foot infection?
A: Purulence OR 2 or more of: warmth, erythema, lymphangitis, edema, pain. Importantly, a positive swab culture WITHOUT these clinical signs is colonization, not infection, and does not require antibiotics. Tissue culture after debridement is more reliable than swab culture.
Offloading Question
Q: What is the gold standard offloading method for plantar diabetic foot ulcers?
A: Total contact cast (TCC), which reduces plantar pressure by 80-90%. The key advantage is that it is non-removable, ensuring 100% compliance. Removable devices (CAM walker, half-shoe) have poor compliance as patients remove them at home. Instant TCC (fiberglass wrap over CAM walker) is an easier alternative with similar efficacy.
Osteomyelitis Question
Q: What is the sensitivity and specificity of MRI for diabetic foot osteomyelitis?
A: Sensitivity 90%, specificity 80%. MRI is the gold standard imaging modality. Look for: T1-weighted dark signal in bone marrow (edema), T2/STIR bright signal (inflammation), and gadolinium enhancement. Plain radiographs have 50% sensitivity (late sign - bone destruction visible after 2-4 weeks). Probe-to-bone test has positive likelihood ratio of 6.4.
Amputation Healing Question
Q: What toe pressure predicts healing after transmetatarsal amputation?
A: Toe pressure greater than 40 mmHg predicts reliable healing (some sources use greater than 30 mmHg as minimum threshold, but greater than 40 mmHg is more reliable). TcPO2 greater than 30 mmHg at the amputation level is also predictive. If perfusion is inadequate, revascularization (angioplasty or bypass) should be performed before amputation.
Evidence Question
Q: What is the evidence for multidisciplinary diabetic foot care?
A: Multiple studies show 50% reduction in major amputation rate with multidisciplinary foot clinics compared to usual care. Key elements: podiatry, vascular surgery, endocrinology, infectious disease, orthopaedics working together. IWGDF guidelines (2019) give this a Grade A recommendation based on systematic review evidence.
Guidelines, Registries & Global Practice
Global Epidemiology
Burden (Zhang 2017 meta-analysis):
- Pooled global diabetic foot ulcer prevalence 6.3%
- Estimated lifetime ulcer risk in diabetes 19-34% (Armstrong NEJM 2017)
- Recurrence ~40% at 1 year, ~65% at 5 years after healing
Marked regional variation:
- North America 13.0%, Africa 7.2%, Asia 5.5%, Europe 5.1%, Oceania 3.0%
- Indigenous and lower-resource populations carry disproportionate amputation burden
Universal screening with region-tailored prevention is the consistent message.
Where Guidelines Converge
Shared international principles (IWGDF, IDSA, NICE, AAOS/ACFAS):
- Annual risk stratification (loss of protective sensation + PAD)
- Treat infection, not colonisation; post-debridement tissue culture
- Non-removable offloading for plantar neuropathic ulcers
- Integrated multidisciplinary foot care to prevent amputation
Differences are mainly in antibiotic agents and service organisation, not principles.
Major Guidelines Side by Side
| Body (region) | Scope / emphasis | Key recommendation | Evidence basis |
|---|---|---|---|
| IWGDF (international) | Prevention, classification (SINBAD/WIfI), offloading | Risk-based screening; pressure-relieving therapeutic footwear; non-removable offloading first-line | GRADE systematic reviews (mixed certainty) |
| IDSA (USA) | Diabetic foot infection and osteomyelitis | Infection = 2+ inflammatory signs; severity-based empiric therapy; MRI for osteomyelitis | Consensus guideline, low-moderate quality evidence |
| NICE NG19 (UK) | Whole-pathway diabetic foot care | Refer active diabetic foot problems to a multidisciplinary foot service within 1 working day | Guideline with health-economic modelling |
| ACFAS / AAOS (USA) | Surgical management, amputation, Charcot | Most distal viable amputation level; revascularise marginal perfusion before definitive level | Expert consensus + cohort evidence |
Classification Beyond Wagner/Texas
Modern international guidance increasingly uses SINBAD (Site, Ischaemia, Neuropathy, Bacterial infection, Area, Depth) for audit and communication, and WIfI (Wound, Ischaemia, foot Infection) for limb-threat and revascularisation-benefit stratification. Wagner and Texas remain the classic exam systems, but be able to mention SINBAD and WIfI as the contemporary registry/vascular tools.
Practice Variation by Setting
High-resource settings emphasise revascularisation (endovascular or bypass), total contact casting, negative-pressure wound therapy and multidisciplinary clinics. Limited-resource settings see later presentation, higher rates of major amputation, less access to vascular intervention and offloading, and greater reliance on primary amputation for source control. Antibiotic choice also varies with local resistance patterns and formularies (e.g. flucloxacillin plus metronidazole vs amoxicillin-clavulanate vs co-trimoxazole for mild infection) - the principle of severity-based, culture-directed, de-escalated therapy is universal even where the specific agent differs.
Medicolegal Considerations
Key documentation requirements:
- Annual foot screening: Document monofilament test, pulses, deformity. Failure to screen is negligent.
- High-risk foot referral: Document referral to podiatry or high-risk foot service. Delayed referral for high-risk foot is common litigation trigger.
- Informed consent for amputation: Document discussion of amputation level options, healing rates, functional outcomes, alternative of limb salvage vs definitive amputation. Patients must understand tradeoffs.
- DVT prophylaxis: All diabetic foot patients admitted with infection are high VTE risk. Document prophylaxis or reason for omission.
- Multidisciplinary involvement: Document vascular, infectious disease, endocrinology input for complex cases. Solo decision-making for complex limb salvage is high-risk.
Common litigation scenarios: Delayed amputation leading to sepsis; inadequate informed consent for amputation level; failure to attempt revascularization before amputation; amputation at wrong level (too distal) leading to failure and revision.
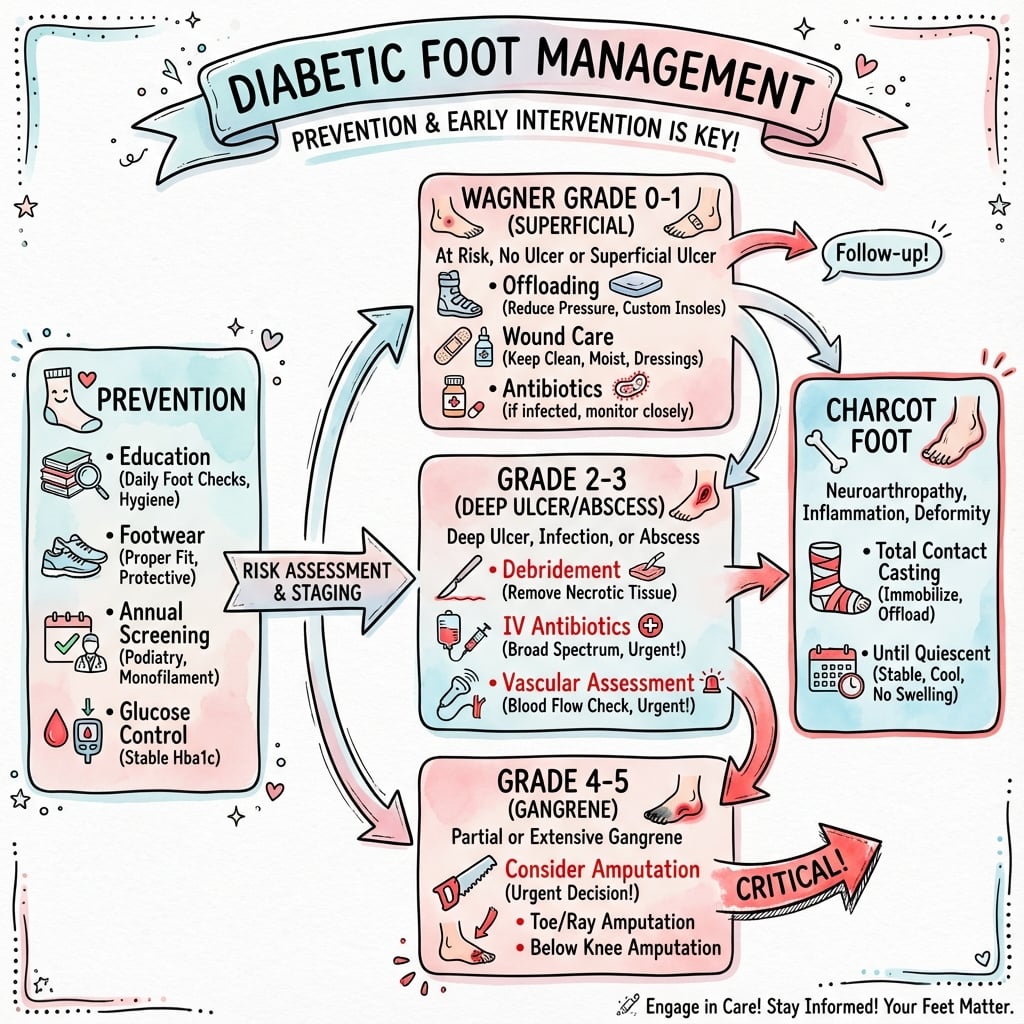
DIABETIC FOOT MANAGEMENT
Clinical summary
Key Classifications
- •Wagner Grade 0 = intact skin (prevent); 1 = superficial; 2 = deep to bone; 3 = abscess/osteomyelitis; 4 = forefoot gangrene; 5 = whole foot gangrene
- •Texas = 4x4 grid: Depth A-D (superficial, tendon, bone, infected) + Stage 0-3 (clean, infection, ischemia, both)
- •IDSA infection: Mild (less than 2 cm erythema), Moderate (greater than 2 cm or deep), Severe (systemic signs)
- •PEDIS = Perfusion + Extent + Depth + Infection + Sensation (research classification)
Diagnostic Tests
- •Probe-to-bone: positive LR 6.4 for osteomyelitis (sterile probe feels hard gritty bone)
- •MRI: gold standard for osteomyelitis (90% sensitive, 80% specific)
- •Monofilament: 10g at 9 sites - unable to feel at 4+ sites = LOPS
- •Toe pressure: greater than 30 mmHg minimum, greater than 40 mmHg reliable for healing
Treatment Algorithm
- •Uninfected ulcer: offloading (TCC) + sharp debridement + moist dressing (NO antibiotics)
- •Mild infection: oral antibiotics 1-2 weeks (cefalexin or amoxicillin-clavulanate)
- •Severe infection: IV broad-spectrum (pip-tazo + vancomycin) + urgent surgical debridement
- •Osteomyelitis: surgical debridement (curative) OR 6-12 weeks antibiotics (conservative)
Amputation Levels
- •Toe 90%, Ray 80-90%, Transmetatarsal 50-70%, Syme 70-80%, Transtibial 80-90%, Transfemoral 90-95% healing
- •Higher level = better healing but worse function - aim for most distal viable level
- •TMA needs toe pressure greater than 40 mmHg + AFO post-op (prevent equinus ulcer)
- •BKA mortality: 10% at 30 days, 30% at 1 year, 50% at 5 years
Critical Interventions
- •Offloading: TCC reduces pressure 80-90%, non-removable ensures compliance
- •Revascularization: do AFTER infection control (not before - risks spreading infection)
- •Multidisciplinary care: reduces amputation by 50% (podiatry, vascular, endo, ID, ortho)
- •Prevention: annual screening, custom orthotics, patient education (85% amputations preventable)