Flowing Anterior Ossification | The 'Rigid Spine' That Fractures From a Trivial Fall
- DISH is a non-inflammatory enthesopathy: new bone forms at ligaments/entheses, classically the anterior longitudinal ligament.
- Diagnosis is RADIOGRAPHIC (Resnick): flowing ossification over 4+ levels, PRESERVED discs, and SPARED SI/facet joints.
- It is NOT ankylosing spondylitis: DISH spares the SI joints, is HLA-B27 negative, and is non-inflammatory.
- The exam danger: an ankylosed DISH spine behaves like a long bone and fractures (usually transverse, extension-type) from low-energy trauma.
- These fractures are highly unstable, easily missed on plain films, and carry high rates of spinal cord injury and mortality.
- “Strongly associated with type 2 diabetes, obesity, and the metabolic syndrome.
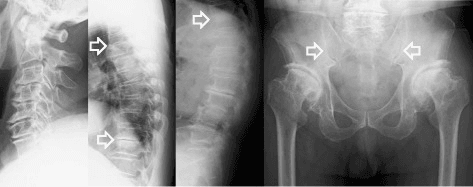
- “Right-sided thoracic predominance is attributed to the pulsatile descending aorta inhibiting left-sided ossification.
- “Anterior cervical osteophytes are a classic cause of mechanical dysphagia (Forestier dysphagia).
- “In any rigid spine with new pain after a minor fall, assume a fracture until CT proves otherwise.
Overview and Epidemiology
Definition DISH (Forestier's disease) is a systemic, non-inflammatory enthesopathy characterised by progressive calcification and ossification of ligaments and entheses, most prominently the anterior longitudinal ligament of the spine. It produces flowing, "candle-wax" new bone that bridges vertebrae and stiffens the spine.
Key concept
- It is a disease of abnormal new bone formation at entheses, not of inflammation or of the disc.
- Because the discs and facet/SI joints are spared, DISH is distinguished from both ankylosing spondylitis and degenerative spondylosis (according to PubMed, Mader et al., RMD Open 2020).
Epidemiology
- Common in older adults; prevalence rises steeply with age and varies widely by definition and population.
- Male predominance (roughly 2:1) and a peak in the 6th decade onward.
- Strong, reproducible associations with type 2 diabetes mellitus, obesity, higher BMI, hyperuricaemia and the metabolic syndrome (according to PubMed, Sarzi-Puttini & Atzeni, Curr Opin Rheumatol 2004; Brikman et al., Semin Arthritis Rheum 2023).
- Increasingly recognised in younger obese patients - in one bariatric cohort, 18% of obese patients aged 50 or under met Resnick criteria, far above the expected general-population rate (according to PubMed, Brikman et al., 2023).
Why it matters for the orthopaedic exam
- Most DISH is asymptomatic and incidental, but candidates are tested on three orthopaedic consequences: the ankylosed-spine fracture, mechanical dysphagia from cervical osteophytes, and the distinction from ankylosing spondylitis.
Pathophysiology and Anatomy
The enthesis and new bone formation
- The primary lesion is at the enthesis (the insertion of ligament/tendon into bone).
- New bone forms through both endochondral and membranous ossification pathways, driven by metabolic and growth-factor signalling rather than inflammation (according to PubMed, Sarzi-Puttini & Atzeni, Curr Opin Rheumatol 2004).
- Candidate metabolic mediators include insulin/IGF-1 (linking to diabetes and obesity) and matrix Gla protein.
The anterior longitudinal ligament (ALL)
- Runs along the front of the vertebral bodies.
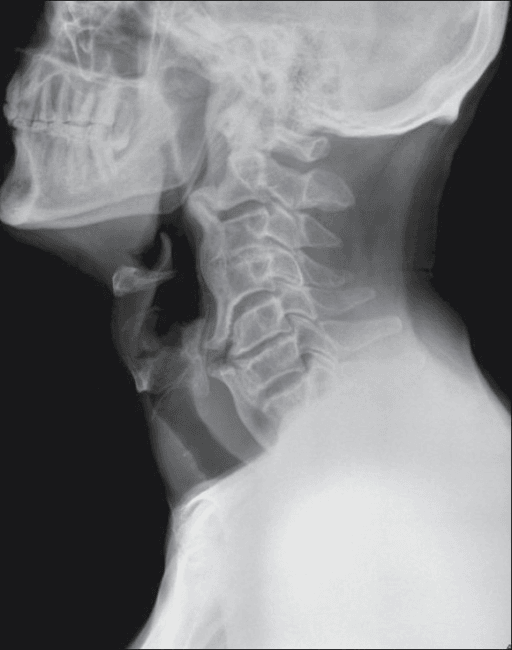
- In DISH it ossifies into a thick anterolateral band that bridges across discs - giving the flowing "dripping candle wax" appearance.
- The disc itself is spared, which is why disc heights stay relatively normal.
The thoracic right-sided predominance
- DISH characteristically favours the right side of the thoracic spine (around T7-T11).
- The classic explanation is mechanical: the pulsatile descending thoracic aorta lies on the left and is thought to suppress ossification on that side, so new bone forms preferentially on the right.
The biomechanics of rigidity
- As segments bridge, the spine loses its normal shock-absorbing flexibility and behaves like a single long bone.
- Combined with age-related osteoporosis, this creates a long, brittle lever arm - the central reason ankylosed spines fracture from trivial force.
Classification Systems
Resnick & Niwayama Criteria (the reference standard)
DISH is diagnosed radiographically when all three are present:
- Flowing ossification along the anterolateral aspect of at least 4 contiguous vertebral bodies.
- Relative preservation of disc height at the involved levels (excludes degenerative spondylosis).
- Absence of apophyseal (facet) joint ankylosis and of sacroiliac erosion, sclerosis or fusion (excludes ankylosing spondylitis).
A systematic review confirmed that no consensus exists for diagnosing early DISH; over 20 partly overlapping criteria sets exist, but spinal hyperostosis is required by all (according to PubMed, Kuperus et al., Rheumatology 2017).
Clinical Assessment
Most patients are asymptomatic - DISH is frequently an incidental finding on chest or abdominal imaging.
When symptomatic, think in three buckets:
- Axial: thoracolumbar stiffness and a dull ache; reduced spinal range of motion; reduced chest expansion if extensive.
- Mechanical compression (cervical):
- Dysphagia from large anterior cervical osteophytes compressing the pharynx/oesophagus (Forestier dysphagia).
- Rarely stridor, hoarseness or difficult intubation from anterior cervical mass effect.
- Neurological: usually only when DISH coexists with OPLL (posterior ossification) producing canal stenosis and myelopathy, or after a fracture.
The acute presentation that must never be missed
- An older patient with a stiff spine who has new spinal pain after a seemingly trivial fall.
- Pain may be the only sign initially; deficits can appear or progress hours to days later.
In a patient with known or suspected DISH (or ankylosing spondylitis), treat any new neck or back pain after even a minor fall as a fracture. Image the WHOLE spine with CT - non-contiguous and second fractures are common, and plain films routinely miss the injury.
Imaging and Investigations
Workup Protocol
- Lateral spine films show the flowing anterolateral ossification - apply the Resnick criteria here.
- Look specifically for preserved disc heights and normal SI joints to separate from spondylosis and AS.
- In trauma, plain films are unreliable - the fracture is often hidden by overlying bone.
- CT the entire spine for any suspected ankylosed-spine fracture; it best shows the bony fracture line and three-column involvement.
- Defines fracture morphology (commonly transverse/extension type) for surgical planning.
- Add MRI when there is a neurological deficit, unexplained pain, or to exclude spinal epidural haematoma.
- In DISH trauma, spinal epidural haematoma is common and may itself require decompression (according to PubMed, Vierunen et al., Eur Radiol 2023).
- One large series found routine MRI changed management in only a minority, so reserve it for deficits or suspected disco-ligamentous/canal pathology rather than performing it reflexively in every case (according to PubMed, Tavolaro et al., Spine J 2019).
- HLA-B27 and inflammatory markers help exclude ankylosing spondylitis (expected normal/negative in DISH).
- Screen for diabetes and metabolic syndrome given the strong association.

Differential Diagnosis
- Key Distinguishing Feature
- Non-inflammatory enthesopathy; SI joints and discs spared
- Imaging Clue
- Flowing anterolateral ossification over 4+ levels, right thoracic predominance
- Typical Pattern
- Older, male, diabetic/obese, often asymptomatic
- Key Distinguishing Feature
- Inflammatory; fuses SI joints; HLA-B27 positive
- Imaging Clue
- Thin vertical syndesmophytes (bamboo spine), squared vertebrae, fused SI joints
- Typical Pattern
- Younger, inflammatory back pain, raised CRP
- Key Distinguishing Feature
- Disc degeneration is primary
- Imaging Clue
- Reduced disc height, discrete horizontal osteophytes, vacuum phenomenon
- Typical Pattern
- Older, mechanical pain
- Key Distinguishing Feature
- Ossification of the POSTERIOR longitudinal ligament
- Imaging Clue
- Ossified strip behind the vertebral bodies in the canal; frequently coexists with DISH
- Typical Pattern
- Myelopathy more than axial pain, East Asian predominance
- Key Distinguishing Feature
- Inflammatory, asymmetric, peripheral enthesitis
- Imaging Clue
- Chunky asymmetric syndesmophytes, sacroiliitis
- Typical Pattern
- Skin/nail or post-infective history
- Key Distinguishing Feature
- Growth-hormone driven bony overgrowth
- Imaging Clue
- Posterior vertebral scalloping, enlarged sella, widened disc spaces
- Typical Pattern
- Acral enlargement, soft-tissue changes
Non-Operative Management
For the common, stable, symptomatic patient:
- Education and reassurance - most DISH is benign and incidental.
- Analgesia (paracetamol, NSAIDs with caution given comorbidity) and physiotherapy for stiffness.
- Metabolic optimisation: weight loss, glycaemic control - the modifiable associations.
- Dysphagia: dietary modification, upright posture, anti-reflux measures and speech/swallow therapy before considering surgery.
Non-operative care of fractures is largely abandoned for unstable three-column injuries because of high rates of displacement, secondary neurology and mortality; it is reserved only for genuinely stable injuries or patients unfit for any surgery, and even then needs close monitoring.
Management Algorithm
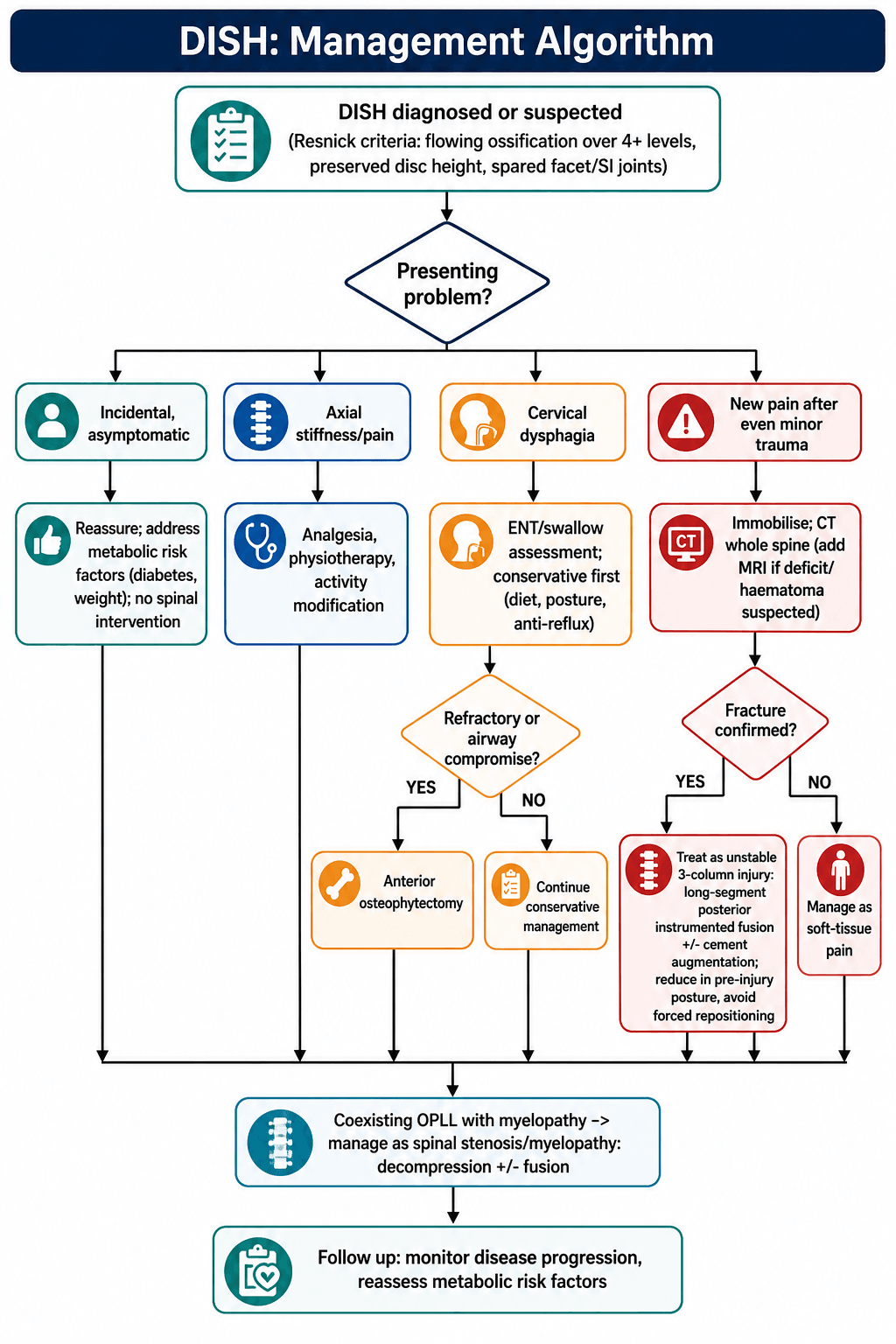
Decision pathway
- Incidental, asymptomatic DISH: reassure and address metabolic risk factors (diabetes, weight). No spinal intervention.
- Axial stiffness/pain: analgesia, physiotherapy, activity modification.
- Cervical dysphagia: ENT/swallow assessment; conservative first (diet, posture, anti-reflux); anterior osteophytectomy if refractory or causing airway compromise.
- Suspected fracture (any new pain after trauma): immobilise, CT whole spine, add MRI if deficit/haematoma suspected, then surgical stabilisation for unstable injuries.
- Coexisting OPLL with myelopathy: manage as a stenosis/myelopathy problem (decompression with or without fusion).
Surgical Technique
Long-segment posterior instrumented fusion
- Goal: neutralise the long rigid lever arm and prevent displacement of an inherently unstable fracture.
- Construct: pedicle screws spanning at least 3 levels above and 3 below the fracture (long constructs resist the cantilever forces of a fused spine).
- Augmentation: PMMA cement augmentation of screws improves purchase in osteoporotic ankylosed bone; percutaneous placement limits blood loss and wound problems in frail patients (according to PubMed, Buxbaum et al., 2021).
- Positioning: transfer and position carefully in the pre-injury alignment; never force a kyphotic/hyperextended spine flat.
- Decompression: add if there is cord compression or an epidural haematoma.
Airway and Anaesthetic Considerations
The topic repeatedly flags "difficult intubation", "airway compromise" and "anticipate a difficult airway" but the airway itself is a distinct, examinable hazard in the DISH patient coming for any operation - not just cervical surgery. Two problems combine: a rigid, ankylosed cervical spine that will not extend, and bulky anterior osteophytes that distort and narrow the laryngopharynx, anteriorly displacing the pharynx and trachea.
Key points
- Routine airway assessment under-predicts the difficulty. In a reported DISH case the Mallampati score was class III yet video laryngoscopy, direct laryngoscopy, a laryngeal mask and an optical stylet all failed - an unexpected posterior pharyngeal bulge from the osteophyte blocked tube placement, and only flexible fibreoptic nasal intubation succeeded (according to PubMed, Zhang et al., Ann Transl Med 2021).
- Awake flexible fibreoptic intubation with a small-calibre tube is the reliable technique in a spine bridged from C2 to C7, preserving spontaneous ventilation and avoiding forced neck manoeuvres (according to PubMed, Gosavi et al., Asian J Neurosurg 2018).
- Do not force neck extension in the fused cervical spine, and involve senior anaesthesia and ENT early; preoperative CT (and, in complex cases, 3D assessment) helps map osteophyte size and location before induction.
- Generic difficult-airway ladders and general anaesthetic principles belong to the dedicated anaesthesia topics - here the message is that cervical DISH is a specific "difficult airway" flag that standard bedside tests can miss.
Q: A patient with cervical DISH and dysphagia is listed for surgery - what is your airway plan? A: Anticipate a difficult airway that standard bedside assessment and plain films may under-predict. The safest default is awake flexible fibreoptic intubation with a small-calibre tube, avoiding forced neck extension; do not rely on video or direct laryngoscopy, which can be defeated by osteophyte-related laryngopharyngeal distortion.
A rare case of unexpected difficult airway management in a DISH patient and post-operative airway evaluation with 3D printing
- Radiographic imaging did not predict airway compromise and the Mallampati score was only class III.
- Video laryngoscopy, direct laryngoscopy, laryngeal mask and optical stylet all failed; only flexible fibreoptic nasal intubation succeeded.
- A patient-specific 3D-printed model showed eccentric cervical osteophytes occupying the laryngopharynx and blocking tube passage.
Airway Management in Case of Diffuse Idiopathic Skeletal Hyperostosis
- DISH bridging the cervical spine from C2 to C7 made conventional intubation hazardous.
- The airway was secured with an awake fibreoptic technique and a small-sized endotracheal tube.
- Cervical hyperostosis can make intubation difficult in multiple ways, warranting a planned approach.
Complications
- Why It Happens
- Long rigid lever arm + osteoporosis behaves like a brittle long bone
- Mitigation
- High index of suspicion; CT whole spine for any new pain
- Why It Happens
- Three-column instability, displacement, epidural haematoma
- Mitigation
- Early stabilisation; MRI if deficit; avoid forced repositioning
- Why It Happens
- Bleeding into the canal after fracture in a rigid spine
- Mitigation
- MRI when deficit/unexplained pain; decompress if compressive (Vierunen 2023)
- Why It Happens
- Fracture line hidden by flowing bone; second fractures common
- Mitigation
- Image the entire spine, not just the painful region
- Why It Happens
- Bulky anterior cervical osteophytes and airway distortion
- Mitigation
- Swallow assessment; anticipate difficult airway; osteophytectomy if refractory
- Why It Happens
- Older, diabetic, often osteoporotic, multiple comorbidities
- Mitigation
- Cement-augmented and percutaneous fixation to cut blood loss (Buxbaum 2021)
Heterotopic Ossification Risk in Hip Arthroplasty
DISH is described throughout this topic as a systemic bone-forming diathesis with peripheral enthesopathy ("whiskering" of the pelvis, olecranon, calcaneus). The surgically important consequence of that diathesis is rarely spelled out: a DISH patient is at increased risk of heterotopic ossification (HO) after total hip arthroplasty, and this changes perioperative planning.
Key points
- Increased HO after total hip arthroplasty is a recognised extraspinal manifestation of DISH, and prophylaxis to prevent it may be indicated in these patients (according to PubMed, Belanger & Rowe, JAAOS 2001).
- In HO risk stratification for hip and knee arthroplasty, DISH sits in the moderate-risk group (alongside ankylosing spondylitis and Paget's disease); the highest-risk groups are men with bilateral hypertrophic osteoarthritis, prior HO in either hip, and post-traumatic hypertrophic osteophytosis (according to PubMed, Iorio & Healy, JAAOS 2002).
- Prophylaxis options are a single fraction of peri-operative radiation or an NSAID regimen, given before the fifth postoperative day and optimally within 24 to 48 hours; recurrence after surgical excision should be expected unless prophylaxis is used (according to PubMed, Iorio & Healy, 2002).
- When radiation is chosen for a high-risk patient (a category that includes DISH), a randomised trial found 700 cGy superior to 400 cGy in preventing HO progression on the Brooker scale after total hip arthroplasty, with no wound complications (according to PubMed, Liu et al., J Arthroplasty 2016).
- The generic HO pathophysiology, Brooker grading and full radiotherapy protocols live in the dedicated heterotopic-ossification topics; the DISH-specific message is simply to flag these patients preoperatively and plan prophylaxis.
Q: A patient with DISH is having a total hip replacement - what extra step should you plan and why? A: Heterotopic ossification prophylaxis. DISH is a bone-forming diathesis and a recognised (moderate) HO risk group, so give single-dose peri-operative radiation or an NSAID within 24 to 48 hours (before the fifth postoperative day); recurrence is likely after excision if prophylaxis is omitted.
Diffuse idiopathic skeletal hyperostosis: musculoskeletal manifestations
- Radiographic findings are almost universally seen on the RIGHT side of the thoracic spine, making it the critical area to image.
- Extraspinal manifestations include an increased risk of heterotopic ossification after total hip arthroplasty.
- Prophylaxis to prevent heterotopic ossification may be indicated in DISH patients undergoing hip arthroplasty.
Heterotopic ossification after hip and knee arthroplasty: risk factors, prevention, and treatment
- DISH is a moderate-risk condition for HO after hip/knee arthroplasty, alongside ankylosing spondylitis and Paget's disease.
- Radiation and NSAID prophylaxis are effective and should be given before the fifth postoperative day, optimally within 24 to 48 hours.
- Recurrence after surgical excision of HO should be expected unless prophylaxis is administered.
Heterotopic Ossification Prophylaxis After Total Hip Arthroplasty: Randomized Trial of 400 vs 700 cGy
- High-risk patients (DISH, hypertrophic osteoarthritis, ankylosing spondylitis or prior HO) were randomised to 400 or 700 cGy of postoperative radiation.
- 700 cGy was significantly superior to 400 cGy in preventing Brooker progression of HO, with no wound complications.
- No preoperative factor predicted a higher rate of HO progression.
Postoperative Care
- Mobilise as early as the construct and comorbidities allow; these elderly patients deteriorate quickly with immobility (pneumonia, VTE, delirium, pressure injury).
- VTE prophylaxis, careful glycaemic control, and aggressive medical co-management - postoperative medical complications occur in a large minority of ankylosed-spine fracture patients (according to PubMed, Buxbaum et al., 2021).
- Monitor neurology closely for delayed deficit (haematoma, displacement) in the first days.
- Watch the airway and swallowing closely in the early postoperative period (oedema can transiently worsen dysphagia).
- Counsel that symptoms usually improve but the osteophyte can recur over time.
Outcomes and Prognosis
- Incidental DISH has an excellent prognosis - it is the associated metabolic disease (cardiovascular risk, diabetes) that drives long-term health, not the spinal ossification itself.
- Dysphagia from osteophytectomy generally improves, though recurrence is possible because the underlying disease continues.
- Ankylosed-spine fractures carry a sobering prognosis: high rates of spinal cord injury, neurological deterioration, medical complications and mortality, reflecting both the injury and the comorbid, elderly population.
- In post-traumatic DISH MRI series, spinal cord injury was present in the majority of those imaged, and spinal epidural haematoma was a frequent, potentially treatable contributor (according to PubMed, Vierunen et al., Eur Radiol 2023).
Guidelines, Registries & Global Practice
Global epidemiology
- DISH is common in older adults worldwide; prevalence rises with age and is reported across all populations, with figures varying widely because criteria differ (according to PubMed, Kuperus et al., Rheumatology 2017).
- Consistent male predominance (~2:1) and strong associations with type 2 diabetes, obesity, hypertension and the metabolic syndrome are seen internationally (according to PubMed, Sarzi-Puttini & Atzeni 2004; Brikman et al. 2023).
- Increasingly diagnosed in younger obese patients as CT use rises - 18% in one obese under-50 cohort (according to PubMed, Brikman et al., 2023).
Side-by-side guideline / consensus positions
- Position on DISH
- Diagnose on flowing ossification over 4+ contiguous vertebrae, preserved discs, and spared SI/facet joints - still the global standard.
- Position on DISH
- Acknowledge no agreed criteria for early DISH; call for criteria capturing the progressive phases of new bone formation.
- Position on DISH
- Treat fractures of the ankylosed spine (DISH or AS) as unstable three-column injuries; CT the whole spine; favour long-segment instrumented stabilisation.
- Position on DISH
- Most DISH is managed non-operatively; surgery is reserved for fractures, refractory cervical dysphagia, and coexisting myelopathy.
Registry / outcome evidence
- There is no dedicated DISH implant registry; the evidence base is retrospective cohorts and case series (e.g. MRI trauma cohorts, percutaneous fixation series).
- These consistently show frequent epidural haematoma and spinal cord injury after low-energy trauma and good union with cement-augmented, often percutaneous, long constructs in frail patients (according to PubMed, Vierunen 2023; Buxbaum 2021).
High- vs limited-resource practice variation
- High-resource settings: whole-spine CT (and selective MRI) for any ankylosed-spine trauma; percutaneous, cement-augmented long-segment fixation; multidisciplinary frailty co-management.
- Limited-resource settings: greater reliance on plain films (which miss these fractures) and open surgery; the universal priority everywhere is a low threshold to image the whole spine in a rigid spine with new pain.
Controversies and Areas of Uncertainty
- No agreed criteria for early DISH - more than 20 criteria sets exist and disagree, hampering research and earlier diagnosis (according to PubMed, Kuperus et al., Rheumatology 2017).
- Routine MRI in every ankylosed-spine trauma? Evidence suggests MRI changes management in only a minority, supporting a selective (deficit/unexplained pain) rather than reflexive approach (according to PubMed, Tavolaro et al., Spine J 2019).
- Optimal construct length and the role of percutaneous/cement-augmented fixation continue to evolve, balancing biomechanical stability against the morbidity of open surgery in frail patients.
- Aetiology remains "idiopathic" - metabolic and genetic drivers are implicated but no specific disease-modifying drug exists (according to PubMed, Sarzi-Puttini & Atzeni, Curr Opin Rheumatol 2004).
Mnemonics
FDSResnick Diagnostic Criteria
Hook:All three are required - 'FDS': Flowing bone, Discs intact, SI joints Spared.
DISHDISH versus AS
Hook:Spell DISH to recall the four features that separate it from ankylosing spondylitis.
RIGIDWhy the DISH Spine Is Dangerous
Hook:A RIGID spine fractures, hides the fracture, and then does badly - hence aggressive imaging and fixation.
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“You are shown a lateral thoracolumbar radiograph of a 68-year-old man with a 'fused-looking' spine. How do you decide whether this is DISH or ankylosing spondylitis?”
“A 78-year-old man with known DISH trips on a rug and complains of new mid-back pain. Neurology is intact. Plain films look 'unchanged'. What do you do?”
“A 74-year-old man with DISH has dysphagia from large anterior cervical osteophytes. Conservative measures have failed and he wants surgery. The CT also shows multilevel OPLL with canal stenosis. How does that change your plan?”
MCQ Practice Points
Q: What are the Resnick criteria for DISH? A: All three of: flowing ossification over at least 4 contiguous vertebral bodies, relative preservation of disc height, and absence of SI joint and facet joint fusion/erosion.
Q: What single radiographic feature best separates DISH from ankylosing spondylitis? A: The sacroiliac joints. They are spared in DISH and fused/eroded in ankylosing spondylitis.
Q: Why does thoracic DISH favour the right side? A: The pulsatile descending thoracic aorta on the left is thought to inhibit left-sided ossification, so new bone forms preferentially on the right (around T7-T11).
Q: Which metabolic conditions are strongly associated with DISH? A: Type 2 diabetes mellitus, obesity and the metabolic syndrome (also hyperuricaemia).
Q: What is the most dangerous orthopaedic consequence of DISH and its classic mechanism? A: An unstable spinal fracture - typically a transverse, extension-type three-column injury from low-energy trauma (e.g. a ground-level fall), easily missed on plain films.
At a Glance
- DISH (Forestier)
- Non-inflammatory enthesopathy/ossification
- Ankylosing Spondylitis
- Inflammatory (HLA-B27, axial spondyloarthritis)
- Spondylosis (degenerative)
- Degenerative disc/facet disease
- DISH (Forestier)
- Preserved at involved levels
- Ankylosing Spondylitis
- Preserved early, then fuses
- Spondylosis (degenerative)
- Reduced (disc degeneration)
- DISH (Forestier)
- Spared (key rule)
- Ankylosing Spondylitis
- Eroded then fused
- Spondylosis (degenerative)
- Normal or degenerative
- DISH (Forestier)
- Bulky, flowing, anterolateral ('candle wax')
- Ankylosing Spondylitis
- Thin vertical syndesmophytes (bamboo)
- Spondylosis (degenerative)
- Discrete horizontal osteophytes
- DISH (Forestier)
- Older, male, diabetic/obese
- Ankylosing Spondylitis
- Younger, inflammatory back pain
- Spondylosis (degenerative)
- Older, mechanical pain
Exam Day Cheat Sheet
Key Concepts
- Non-inflammatory enthesopathy
- Anterior longitudinal ligament ossification
- Flowing 'candle-wax' bone
- Linked to diabetes / obesity / metabolic syndrome
Resnick Criteria (all 3)
- Flowing ossification over 4+ levels
- Preserved disc heights
- SI and facet joints spared
- Right thoracic predominance (aorta)
DISH vs AS
- SI joints SPARED (DISH) vs fused (AS)
- HLA-B27 negative (DISH)
- Bulky osteophytes vs thin syndesmophytes
- Non-inflammatory vs inflammatory
Danger / Management
- Unstable fracture from minor fall
- CT whole spine - films miss it
- Long-segment instrumented fusion
- Anterior osteophytectomy for refractory dysphagia
Evidence Base
Diffuse Idiopathic Skeletal Hyperostosis of the Spine: Pathophysiology, Diagnosis, and Management
- Defines DISH radiographically as flowing ossification along the anterior spine spanning at least 4 vertebral bodies.
- Emphasises strong associations with diabetes mellitus and metabolic derangements despite unknown aetiology.
- Highlights that spinal ankylosis predisposes to unstable fractures from low-energy trauma requiring careful management.
Classification criteria for diffuse idiopathic skeletal hyperostosis: a lack of consensus
- All 24 reviewed criteria sets require spinal hyperostosis for the diagnosis of DISH.
- Major disagreement persists over the threshold number of vertebrae and over defining early disease.
- More than half of criteria sets are dichotomous and ignore the progressive nature of DISH.
Post-traumatic spinal hematoma in diffuse idiopathic skeletal hyperostosis (DISH)
- Spinal epidural haematoma occurred in 49% and spinal cord injury in 61% of post-traumatic DISH patients.
- Ground-level fall (69%) was the commonest mechanism; a transverse AO type B fracture (39%) was the commonest injury.
- Spinal canal narrowing and cord impingement correlated with worse pre-treatment neurological (Frankel) grade.
Is routine MRI of the spine necessary in trauma patients with ankylosing spinal disorders or is a CT scan sufficient?
- MRI revealed an additional injury not seen on CT in only 6 of 124 patients (4.8%).
- Management changed after MRI in just 3.2% (4/124), mostly disco-ligamentous hyperextension injuries.
- Authors recommend selective MRI (neurological deficit or possible disco-ligamentous injury) rather than routine use.
Percutaneous, PMMA-augmented, pedicle screw instrumentation of thoracolumbar ankylotic spine fractures
- Mean age 76 with a mean of 14 ankylosed levels; all had at least one comorbidity.
- Percutaneous cement-augmented fixation gave short operative times (mean 131 min) and low transfusion needs.
- All fractures united without loss of reduction; all retained pre-op ASIA grade and three improved.
High prevalence of diffuse idiopathic skeletal hyperostosis (DISH) among obese young patients
- DISH was present in 18% of young obese patients, far above the expected ~5-10% for this age.
- DISH was associated with hypertension, smoking and obstructive sleep apnoea.
- Supports DISH as an obesity- and metabolic-syndrome-related musculoskeletal complication.