Congenital Variant | Snapping Knee in Children | Watanabe / Ahn Classification
- Lateral much greater than medial discoid meniscus in Western populations (reversed in East Asian cohorts)
- Snapping / clicking knee in a child under 10 should raise suspicion
- MRI: 3 or more consecutive sagittal bow-tie slices is the classic diagnostic criterion
- Asymptomatic discoid menisci are observed; saucerisation is reserved for symptoms or instability
- Wrisberg type needs stabilisation, not just reshaping - missing this causes persistent symptoms
- “Wrisberg type = unstable posterior horn = no tear but still symptomatic
- “Saucerisation preserves a 6-8 mm peripheral rim - total meniscectomy is never acceptable in children
- “Often bilateral; image the contralateral knee if a discoid meniscus is found
- “Watanabe and Ahn classifications are complementary - Ahn adds instability subtypes
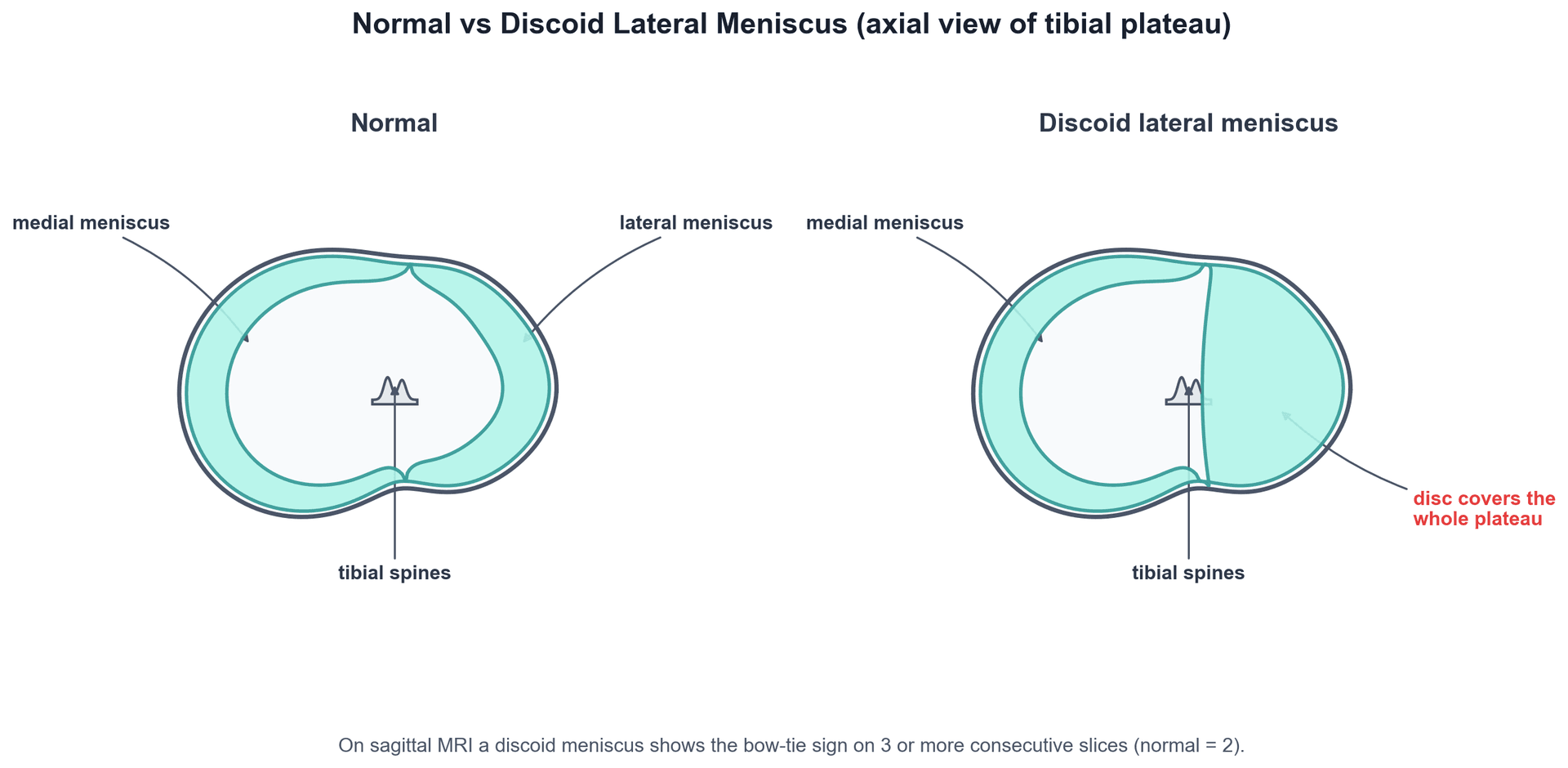
Failure of central meniscal resorption during embryogenesis produces a disc-shaped meniscus. Most discoid menisci are lateral; medial discoid meniscus is rare in Western populations (1-2 percent of discoid menisci) but more common in East Asian cohorts.
Snapping, clicking, or locking in a child aged 5-12 is the classic presentation. Snapping is usually audible and may be visible. Locking (inability to fully extend) suggests a peripheral tear or unstable Wrisberg variant.
3 or more consecutive sagittal slices showing the meniscus as a continuous bow-tie is the most reliable MRI criterion. A coverage ratio of greater than 50 percent of the tibial plateau on coronal images supports the diagnosis.
Total meniscectomy is contraindicated in children. Saucerisation should leave a 6-8 mm peripheral rim of stable meniscal tissue to distribute load and protect the lateral compartment from early osteoarthritis.
- Diagnosis
- MRI bow-tie greater than 3 slices, no tear
- Treatment
- Observe, parental reassurance, return precautions
- Key Pearl
- Most discoid menisci found incidentally never need surgery
- Diagnosis
- Complete or incomplete discoid, stable peripheral rim
- Treatment
- Arthroscopic saucerisation to normal crescent
- Key Pearl
- Preserve 6-8 mm peripheral rim; check stability at end
- Diagnosis
- Wrisberg type or peripheral tear on MRI
- Treatment
- Saucerisation + stabilisation / repair of posterior horn
- Key Pearl
- Reshaping alone in Wrisberg type leaves instability untreated
SAUCERSaucerisation Technique
Hook:SAUCER: six steps to a stable, well-shaped lateral meniscus in a child.
Overview and Epidemiology
Discoid lateral meniscus is the most common congenital meniscal variant and the leading cause of mechanical snapping knee in children. Most discoid menisci are asymptomatic and discovered incidentally, but symptomatic cases are characterised by early lateral compartment overload, clicking, and progressive tearing. Early recognition and rim-preserving surgery protect the lateral compartment from premature osteoarthritis.
- Incidence: 3-5 percent in Western populations; up to 13-17 percent in East Asian cohorts
- Lateral much greater than medial in Western practice; the reverse is true in East Asian series
- Bilateral in 15-25 percent of cases
- Age at presentation: 5-15 years; often first noticed with sport
- Sex: Slight male predominance reported in most series
- Snapping knee: Most common cause in children; audible click with flexion / extension
- Locking: Suggests peripheral tear or unstable Wrisberg variant
- Lateral pain and swelling: Effusion after activity, intermittent limp
- Premature OA: Total meniscectomy leads to severe lateral compartment arthritis within 15-20 years
- Functional limitation: Squatting, kneeling, pivoting sports become difficult
Pathophysiology
The meniscus originates from a continuous disc of mesenchymal tissue in the fetal knee. Failure of central resorption during weeks 8-14 of gestation leaves a disc-shaped lateral meniscus that covers most or all of the tibial plateau. Biomechanically, a discoid meniscus has abnormal hoop-stress distribution, transmits higher contact stresses to the lateral cartilage, and is prone to intrasubstance degeneration. The Wrisberg type is further compromised by the absence of a posterior tibial attachment, leaving the meniscus free to translate anteriorly and to produce a dynamic block to extension.
- Normal meniscus
- Crescent, semilunar
- Discoid meniscus
- Disc, covers greater than 50 percent of plateau
- Clinical consequence
- Loss of normal wedge and hoop function
- Normal meniscus
- Firm tibial insertion
- Discoid meniscus
- Wrisberg type lacks tibial attachment
- Clinical consequence
- Hypermobility, snapping, locking
- Normal meniscus
- Approximately 50 percent coverage
- Discoid meniscus
- Greater than 80 percent coverage
- Clinical consequence
- Increased focal cartilage stress
- Normal meniscus
- Longitudinal, radial, flap
- Discoid meniscus
- Horizontal cleavage common, intrasubstance
- Clinical consequence
- Degenerative, often central
Abnormal hoop stress: Reshaped disc transmits load centrally rather than circumferentially
Impingement: Thick central tissue catches between femur and tibia in extension
Hypermobility: Wrisberg type slides anteriorly and blocks terminal extension
Tear risk: Degenerate central tissue is prone to horizontal cleavage
Cartilage wear: Even untreated asymptomatic discoid meniscus accelerates lateral compartment wear
Subchondral change: Cupped lateral tibial plateau, squaring of the femoral condyle
Early OA: After total meniscectomy, lateral compartment arthritis is near-universal by 20 years
Alignment: Long-standing cases may develop valgus alignment from lateral compartment collapse
The whole rim-preservation and repair strategy rests on meniscal vascularity. Blood reaches the meniscus from the perimeniscal capillary plexus (geniculate branches) only at its periphery, defining three zones: the red-red zone (peripheral, roughly the outer 3 mm, fully vascular - heals well, ideal for repair), the red-white zone (middle, junctional vascularity - variable healing), and the white-white zone (inner third, avascular, nourished only by synovial diffusion - poor healing, where tears are generally resected rather than repaired). This is exactly why saucerisation resects the avascular central disc but preserves a 6-8 mm peripheral (red-red) rim, and why a peripheral or Wrisberg-zone tear is repairable while a degenerate central horizontal cleavage usually is not. In children the meniscus is relatively more vascular than in adults, improving healing potential - a further reason to favour repair over resection.
Classification and Types
Watanabe Classification (1969)
The original arthroscopic classification, still the most widely cited system.
- Anatomy
- Disc covers entire tibial plateau, no semilunar shape
- Stability
- Stable, attached peripherally
- Typical management
- Saucerisation if symptomatic
- Anatomy
- Semilunar but broader than normal, partial coverage
- Stability
- Stable, attached peripherally
- Typical management
- Saucerisation if symptomatic
- Anatomy
- Posterior horn attached only by Wrisberg ligament
- Stability
- Unstable, hypermobile
- Typical management
- Saucerisation + stabilisation / repair
The Wrisberg type is the only inherently unstable variant. Distinguishing it is critical because saucerisation alone is insufficient.
The Wrisberg-type discoid meniscus is named after one of the two meniscofemoral ligaments, and the examiner will expect you to name both. They run from the posterior horn of the lateral meniscus to the medial femoral condyle, straddling the PCL: the ligament of Humphrey passes anterior to the PCL and the ligament of Wrisberg passes posterior to the PCL (mnemonic: "Humphrey is in front, Wrisberg is at the rear"). They are accessory stabilisers of the lateral meniscus posterior horn. In the Wrisberg-variant discoid meniscus the normal posterior tibial (coronary/root) attachment is absent, so the posterior horn is anchored only by the ligament of Wrisberg - leaving it free to translate anteriorly and snap, which is exactly why reshaping alone fails and posterior-horn reattachment is required. At least one meniscofemoral ligament is present in most knees; both are present in a minority.
CIWWatanabe Classification
Hook:CIW: Complete, Incomplete, Wrisberg - the only three Watanabe types you need to know.
Clinical Assessment
- Snapping / clicking / clunking audible to parents or child, often with flexion / extension
- Intermittent locking in fixed flexion; child may unlock with a twist
- Lateral knee pain worsened by squatting, pivoting, stairs
- Effusion after activity; intermittent limp
- Giving way in unstable Wrisberg variant
- No major trauma in most cases
- Snapping test: Audible / palpable click as knee flexes and extends; correlate with symptoms
- McMurray: May produce palpable clunk at lateral joint line
- Thessaly test: Useful for meniscal pathology, well tolerated in older children
- Effusion: Mild to moderate lateral compartment swelling
- Range of motion: Usually full; block to extension suggests Wrisberg or peripheral tear
- Joint line tenderness: Lateral joint line, often localised
A child with an audible snapping knee should be taken seriously, even if the parents describe it as harmless or the child has full range of motion. The most common cause of true snapping knee in a child under 12 is a discoid lateral meniscus; delayed diagnosis risks progressive tear and early cartilage damage. Document the snap, examine under anaesthesia if needed, and arrange MRI.
- Technique
- Repeated flexion / extension while palpating lateral joint line
- Positive finding
- Audible / palpable click that reproduces symptoms
- Notes
- Best single clinical clue in a child
- Technique
- Flexion to 90 degrees, internal rotation, varus, then extend
- Positive finding
- Palpable clunk at lateral joint line
- Notes
- Less reliable than in adults; often equivocal
- Technique
- Single-leg stance, flex 20 degrees, rotate body
- Positive finding
- Joint line discomfort or locking
- Notes
- Good sensitivity in older children and adolescents
- Technique
- Attempt passive full extension
- Positive finding
- Mechanical block to terminal extension
- Notes
- Suggests Wrisberg variant or large peripheral tear
- Key clue
- Snapping, locking, intermittent
- Discriminating test
- MRI bow-tie greater than 3 slices, posterior horn position
- Typical imaging
- MRI diagnostic
- Key clue
- Acute injury, effusion, joint line tenderness
- Discriminating test
- MRI shows normal shape meniscus with tear
- Typical imaging
- MRI shows tear in normal-sized meniscus
- Key clue
- Insidious lateral pain, intermittent swelling
- Discriminating test
- MRI shows subchondral lesion, may have fragment
- Typical imaging
- MRI or CT diagnostic
- Key clue
- Anterior pain, activity-related, no snap
- Discriminating test
- Negative MRI for meniscal pathology
- Typical imaging
- MRI of patellofemoral joint
- Key clue
- Posterolateral pain, no snap, overuse
- Discriminating test
- Clinical, MRI may show tendon oedema
- Typical imaging
- MRI helpful but not always diagnostic
- Key clue
- Lateral pain with running, no true snap
- Discriminating test
- Ober test, MRI may show ITB oedema
- Typical imaging
- MRI supportive
A discoid meniscus may be present for years without tearing, but when a peripheral tear develops the child often presents acutely with locking and effusion. The combination of a discoid meniscus on MRI plus a high intrasubstance or peripheral signal reaching the articular surface is the strongest predictor that saucerisation alone will fail - add repair.
Investigations
Imaging Protocol
Views: Weight-bearing AP, lateral, skyline, tunnel / notch views
Look for: Widened lateral joint space, cupped lateral tibial plateau, hypoplastic or squared lateral femoral condyle
Purpose: Exclude other pathology, provide baseline alignment, occasionally raise suspicion
Protocol: Standard knee MRI with sagittal, coronal, axial PD / T2 fat-sat
Diagnostic criteria: Bow-tie sign on 3 or more consecutive sagittal slices; coronal coverage greater than 50 percent of tibial plateau; anteriorly displaced posterior horn (Wrisberg)
Identify tears: High intrasubstance signal reaching articular surface; peripheral signal
Advantage: Non-invasive, no radiation, defines anatomy for surgical planning
Indication: Suspected Wrisberg variant or complex tear, equivocal standard MRI
Findings: Anterior translation of posterior horn, absent posterior tibial attachment
Use: Confirms instability subtype and guides need for stabilisation
X-rays in a child with a discoid meniscus are often normal; do not be reassured by a normal X-ray. MRI is the definitive investigation, and the 3-sagittal-slice bow-tie sign is the most reliable sign - it reflects the meniscus wrapping continuously across the lateral compartment. A coverage ratio of greater than 50 percent on the coronal view provides supportive evidence.
SNAPSnapping Knee Workup
Hook:SNAP the diagnosis: see the snap, feel the click, take the MRI, plan the scope.
Management Algorithm
Asymptomatic Discoid Meniscus (Incidental Finding)
Goal: Avoid unnecessary surgery while monitoring for symptom development.
Management Plan
Reassure parents and child that incidental discoid menisci are common
Avoid sport restriction unless symptoms develop; encourage normal activity
Document baseline examination, imaging, and counselling
Return precautions: Snapping, locking, pain, swelling, limp
Reassess symptoms and function
No imaging unless new symptoms
Discharge if asymptomatic and family understands return precautions
Convert to symptomatic pathway - MRI if not already recent
Proceed to arthroscopy if mechanical symptoms or persistent pain
Asymptomatic discoid menisci do not need prophylactic surgery; the natural history in the absence of symptoms is usually benign.
Complications
- Incidence
- 5-15 percent in paediatric series
- Risk factors
- Thin rim, vigorous sport, missed instability
- Management
- Revision repair if symptomatic; consider partial regrowth
- Incidence
- 5-10 percent after saucerisation
- Risk factors
- Wrisberg variant unrecognised, inadequate stabilisation
- Management
- Revision with stabilisation if instability confirmed
- Incidence
- 10-30 percent by 20 years
- Risk factors
- Total meniscectomy history, cartilage damage at index surgery
- Management
- Activity modification, cartilage repair, realignment if needed
- Incidence
- Less than 1 percent
- Risk factors
- Posterior horn repair, deep suture passage
- Management
- Careful technique, neurolysis if exposed
- Incidence
- 2-5 percent
- Risk factors
- Prolonged protected rehab, immature patients
- Management
- Aggressive physiotherapy, MUA if persistent
- Incidence
- 10-20 percent in children
- Risk factors
- Higher than adult meniscal surgery
- Management
- Plan for second look if symptoms recur
Total meniscectomy in a child with a discoid meniscus leads to severe, premature lateral compartment osteoarthritis - often within 15-20 years - and is a recognised cause of early joint replacement in young adults. Even when the meniscus is extensively torn, preserve as much peripheral vascular tissue as possible and combine saucerisation with repair. In unsalvageable cases, meniscal allograft transplantation is a salvage option in skeletally mature adolescents.
Outcomes and Prognosis
- Treatment
- Saucerisation only
- Expected outcome
- 80-90 percent symptom resolution
- Long-term function
- Good sport return, low reoperation
- Treatment
- Saucerisation + repair
- Expected outcome
- 70-85 percent good outcome
- Long-term function
- Good if instability addressed; better than resection alone
- Treatment
- Saucerisation + repair
- Expected outcome
- 75-90 percent good outcome
- Long-term function
- Good if repair heals; revision possible
- Treatment
- Saucerisation + repair / partial
- Expected outcome
- 60-80 percent good outcome
- Long-term function
- Variable; higher reoperation rate
Best prognosis: Watanabe I/II, stable, isolated central disc, healthy articular cartilage, motivated child and family, single-stage saucerisation.
Poor prognosis: Wrisberg variant missed at index surgery, pre-existing cartilage damage, unsalvageable circumferential tear, low-compliance rehabilitation, return to high-demand pivoting sport before adequate healing.
Key threshold: Recognising and stabilising the Wrisberg variant at the first operation. Missing instability is the commonest cause of reoperation and persistent symptoms.
Guidelines, Registries & Global Practice
- 3-5 percent incidence in Western populations; up to 13-17 percent in East Asian cohorts
- Lateral dominates in Western series; medial discoid is more common in East Asian series
- Bilateral in 15-25 percent of cases - image the contralateral knee when one is identified
- Common age of presentation 5-15 years; symptomatic cases are often sports-related
- Sex: Slight male predominance in most published series
- High-resource: Arthroscopy with rim-preserving saucerisation is the standard; MRI is widely available for diagnosis and planning
- Limited-resource: Clinical diagnosis with X-ray may be the only option; open meniscectomy has been used historically but accelerates OA
- Universal principle: Preserve as much peripheral meniscal tissue as possible; the operation can be done with standard arthroscopy equipment
- Rehabilitation: Hinged bracing and physiotherapy protocols are similar across centres
- Diagnosis emphasis
- Snapping knee in a child, MRI bow-tie greater than 3 slices
- Surgical principle
- Saucerisation preserving 6-8 mm peripheral rim; repair if unstable
- Special notes
- Counsels families on higher reoperation rate than adults
- Diagnosis emphasis
- Watanabe and Ahn classifications, MRI for unstable subtypes
- Surgical principle
- Rim-preserving saucerisation, repair for Wrisberg or peripheral tear
- Special notes
- Strong evidence against total meniscectomy in children
- Diagnosis emphasis
- MRI criteria, classify instability under anaesthesia
- Surgical principle
- Saucerisation with or without repair based on stability
- Special notes
- Return-to-sport criteria based on stability and rehab progression
- Diagnosis emphasis
- Higher prevalence in East Asian cohorts, medial variant more common
- Surgical principle
- Saucerisation principles the same; technical adaptations for medial variant
- Special notes
- Greater emphasis on medial discoid meniscus compared with Western practice
There is no dedicated meniscal registry analogous to the arthroplasty registries. Evidence for discoid meniscus management is dominated by retrospective case series and operative technique descriptions; randomised trials are not feasible because of low incidence and varied subtypes. Major arthroplasty registries (NJR, AJRR, AOANJRR) inform the long-term OA risk of total meniscectomy, which is the primary reason to preserve the rim in children.
Record in every discoid meniscus case:
- Watanabe and Ahn subtype; whether stable or unstable
- Peripheral rim width at end of procedure (6-8 mm target)
- Whether repair was performed; number of sutures; technique
- Status of articular cartilage at index procedure
- Post-operative plan: weight-bearing status, brace, physiotherapy, return-to-sport timeline
A missed Wrisberg variant and a total meniscectomy in a child are recognised sources of complaint and medico-legal claim worldwide. Document instability testing and rim preservation carefully.
Controversies & Areas of Uncertainty
Some authors argue that all complete discoid menisci should be reshaped prophylactically to prevent future tearing and chondral damage. Others observe asymptomatic discoid menisci because the natural history is often benign. There is no level 1 evidence; decisions are typically based on morphology, age, and family preference.
The classic teaching is 6-8 mm of peripheral rim, but the precise minimum is not defined by high-quality trials. Biomechanical studies suggest leaving as much vascularised tissue as possible; some surgeons preserve the entire peripheral zone and resect only degenerate central tissue. Long-term cartilage outcomes are rarely reported.
Inside-out, outside-in, and all-inside techniques all have proponents. Inside-out provides a strong, reliable repair but requires a posterolateral incision and risks peroneal nerve injury. All-inside is faster and avoids the incision but is more expensive and may have lower load to failure in some studies. Choice is often surgeon preference.
Meniscal allograft transplantation is a salvage option in skeletally mature adolescents with unsalvageable discoid menisci or post-meniscectomy syndrome. Outcomes are favourable in selected patients, but the procedure is technically demanding, requires careful sizing, and is not universally available. Long-term outcome data in children are limited.
MCQ Practice Points
Q: What embryological event produces a discoid meniscus? A: Failure of central resorption of the mesenchymal meniscal disc in the fetal knee (around weeks 8-14 of gestation). This leaves a disc-shaped meniscus that covers most or all of the tibial plateau.
Q: Which Watanabe type is inherently unstable and which is the most common? A: Watanabe III (Wrisberg type) is the only inherently unstable type - it lacks a posterior tibial attachment and is restrained only by the Wrisberg meniscofemoral ligament. Watanabe I (complete) is the most common morphological type. Ahn classification adds instability subtypes (3 and 4) that help guide treatment.
Q: What is the most reliable MRI criterion for a discoid meniscus? A: 3 or more consecutive sagittal slices showing a continuous meniscal bow-tie. A normal meniscus shows a bow-tie on only 2 consecutive slices. Coronal coverage of greater than 50 percent of the tibial plateau is supportive. Anterior translation of the posterior horn suggests the Wrisberg variant.
Q: What is the principle of arthroscopic saucerisation and what rim width should be left? A: Reshape the central disc to a normal crescent, leaving a 6-8 mm peripheral rim of stable meniscal tissue. Aim for a wider anterior horn tapering to a thinner posterior horn. Total meniscectomy is contraindicated in children because of premature lateral compartment osteoarthritis. Wrisberg variants require additional stabilisation / repair.
Q: When is stabilisation required in addition to saucerisation? A: Wrisberg variant (Ahn 3) and any peripheral tear (Ahn 2 or 4) require stabilisation. Reshaping alone leaves the meniscus hypermobile and symptoms will persist. Techniques include inside-out, outside-in, and all-inside suture repair of the posterior horn to the tibial footprint.
Q: What is the most important long-term complication of total meniscectomy in a child? A: Premature lateral compartment osteoarthritis, often severe and visible on radiographs within 15-20 years. This is why total meniscectomy is contraindicated in children, and meniscal allograft transplantation may be considered as a salvage option in skeletally mature adolescents.
Clinical Imaging
Imaging Appearance of Discoid Lateral Meniscus
This section summarises the imaging appearance of discoid lateral meniscus; the dedicated image atlas is added by a separate pipeline and is not embedded in this MDX.
On plain radiographs, the lateral compartment may show widening of the lateral joint space, a cupped or sloped lateral tibial plateau, a hypoplastic lateral femoral condyle, and squaring of the lateral femoral condyle in long-standing cases. Crucially, plain films are often normal in early disease, and any child with mechanical lateral knee symptoms should proceed to MRI.
- Widened lateral joint space (greater than 5-6 mm)
- Cupping / sloping of the lateral tibial plateau
- Hypoplastic lateral femoral condyle
- Squaring of the lateral femoral condyle (chronic overload)
- Normal films do not exclude discoid meniscus
- Bow-tie sign: 3 or more consecutive sagittal slices show continuous meniscal bow-tie (normal is 2)
- Coverage: Meniscus covers greater than 50 percent of the tibial plateau on coronal view
- Disproportionate size: Ratio of meniscus to tibia is greater than normal
- Absent or truncated posterior horn suggests Wrisberg variant
- High intrasubstance signal may indicate an associated tear
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 9-year-old boy is brought in by his parents because they can hear his right knee clicking when he walks. The clicking has been present for several months, is occasionally painful, and he has begun to limp after football. Examination shows a small effusion, a palpable clunk at the lateral joint line as the knee flexes and extends, and full range of motion. What is the most likely diagnosis, what investigation would you arrange, and what would you tell the parents?”
“A 12-year-old girl had an arthroscopic saucerisation of a discoid lateral meniscus 6 months ago. Her snapping and locking have improved, but she continues to have lateral pain and gives way when pivoting. Examination shows mild effusion, lateral joint line tenderness, and the knee is stable to Lachman and pivot shift. Repeat MRI shows a well-reshaped meniscus, no re-tear, but the posterior horn appears anteriorly translated relative to the original tibial footprint. What has likely been missed, and how would you manage it?”
Key Anatomy and Pathology
- Failure of central resorption of the fetal meniscal disc
- Lateral much more common than medial in Western populations (reversed in East Asian)
- Often bilateral (15-25 percent); image the contralateral knee
- Wrisberg variant has no posterior tibial attachment - inherently unstable
Watanabe and Ahn Classification
- Watanabe I (complete): disc covers entire plateau, stable
- Watanabe II (incomplete): broader than normal semilunar, stable
- Watanabe III (Wrisberg): no posterior tibial attachment, unstable
- Ahn adds instability subtypes 2 (peripheral tear), 3 (Wrisberg), 4 (circumferential tear)
Clinical Presentation and Diagnosis
- Snapping / clicking / locking lateral knee in a child aged 5-15
- Intermittent pain, effusion, limp; sport-related in many cases
- MRI: 3 or more consecutive sagittal bow-tie slices is diagnostic
- Coronal coverage greater than 50 percent and anteriorly translated posterior horn are supportive
Treatment Algorithm
- Asymptomatic incidental finding: observe, return precautions
- Symptomatic stable: arthroscopic saucerisation, 6-8 mm peripheral rim
- Unstable / Wrisberg: saucerisation + posterior horn reattachment
- Avoid total meniscectomy in children - rim preservation is mandatory
Surgical Pearls
- Probe the posterior horn before and after reshaping - instability must be addressed
- Inside-out sutures are the workhorse for posterior horn reattachment
- Document rim width, stability, cartilage status at end of procedure
- Hinged brace and protected weight-bearing after repair
Complications and Outcomes
- Re-tear 5-15 percent; higher if instability missed
- Persistent symptoms in Wrisberg variant unrecognised at first operation
- Premature lateral compartment OA after total meniscectomy is the worst outcome
- Saucerisation + repair gives 70-90 percent good outcomes at mid-term follow-up
Evidence Base and Key Trials
Arthroscopic treatment of the discoid lateral meniscus. Technique and long-term results
- First description of arthroscopic partial meniscectomy (saucerisation) for symptomatic discoid lateral meniscus
- Recommended resection of the central disc with preservation of a peripheral rim
- Symptom relief reported in the majority of treated children at short-term follow-up
- Established the principle of rim preservation that remains standard today
Congenital discoid lateral meniscus in children. A follow-up study and evolution of management
- Landmark follow-up series of congenital discoid lateral meniscus in children managed in a single specialist centre
- Evolution of management from open total meniscectomy toward arthroscopic rim-preserving surgery
- Documented the high long-term risk of lateral compartment degeneration after total meniscectomy in the young
- Supported the modern shift to arthroscopic saucerisation in symptomatic children
Discoid lateral meniscus: prevalence of peripheral rim instability
- Retrospective paediatric series highlighting a high prevalence of peripheral rim instability in symptomatic discoid lateral menisci
- Instability was often under-recognised on pre-operative imaging and only confirmed at arthroscopy
- Pre-existing chondral injury at index surgery was associated with worse outcome
- Authors emphasised probing every discoid meniscus to detect instability before deciding on resection alone
Long-term results of arthroscopic reshaping for symptomatic discoid lateral meniscus in children
- Long-term follow-up of children with symptomatic discoid lateral meniscus treated by arthroscopic reshaping (saucerisation), with repair added in unstable subtypes
- Good to excellent clinical outcomes sustained at long-term follow-up in the majority of patients
- Outcomes were superior when peripheral instability was recognised and stabilised at the index procedure
- Provides outcome data underpinning the Ahn instability-based classification (no tear / peripheral tear / Wrisberg / circumferential tear)
Arthroscopic treatment of symptomatic discoid meniscus in children: classification, technique, and results
- Paediatric series using a stability-based classification to guide saucerisation with or without repair
- Sustained symptom relief and return to sport in the majority of patients at mid-term follow-up
- Radiographic signs of lateral compartment wear in a minority, but rarely symptomatic in adolescence
- Reoperation related mainly to instability subtype and pre-existing tear