Internal Disc Disruption | Degenerative Disc Disease | Mechanical Back Pain
- Discogenic pain = internal disc disruption with intact annulus but painful fissures
- Diagnosis requires concordant provocation discography - controversial gold standard
- 80% improve with 6-12 months conservative care - surgery last resort only
- Fusion indicated for single-level disease with concordant pain reproduction
- Disc replacement for preserved disc height, no facet arthropathy, under 60 years
- “Key distinction: discogenic pain (internal) vs herniation (external compression)
- “Modic changes on MRI correlate with discogenic pain (Type 1 = inflammation)
- “High-Intensity Zone (HIZ) = annular tear on MRI - 80% sensitivity for discogenic pain
- “MRC trial and Brox RCT: fusion no clearly better than intensive rehabilitation; NICE advises against fusion for low back pain outside a trial
No pathognomonic sign exists. Diagnosis is clinical exclusion plus provocative testing. Beware overdiagnosis - many asymptomatic adults have disc degeneration on MRI.
Modic Type 1 changes (marrow edema) correlate best with pain. High-Intensity Zone (HIZ) = annular tear. Pfirrmann Grade 4-5 = advanced degeneration.
Minimum 6 months structured conservative care before surgery. 80% improve without intervention. Surgery for failed conservative care with concordant pain only.
Fusion vs disc replacement: Single-level, preserved height, under 60, no facet disease = consider arthroplasty. Otherwise fusion. Adjacent segment disease occurs in both.
- MRI Findings
- Pfirrmann 3-4, HIZ+, Modic 1, preserved height
- Treatment
- Intensive PT × 6 months, then consider disc replacement
- Key Pearl
- Disc replacement preserves motion but needs intact facets
- MRI Findings
- Pfirrmann 4-5, Modic 1-2, moderate collapse
- Treatment
- PT × 6 months, then consider ALIF/TLIF fusion
- Key Pearl
- Fusion is gold standard - predictable pain relief
- MRI Findings
- Pfirrmann 4-5, facet arthropathy, instability
- Treatment
- PT, epidurals, avoid surgery unless neurological deficit
- Key Pearl
- Multi-level fusion high morbidity - manage expectations
MODICModic Changes on MRI
Hook:MODIC changes = Marrow edema (Type 1) is the Most Painful type, converts to Osseous fat over time!
REPLACEIndications for Fusion vs Disc Replacement
Hook:REPLACE criteria = when you can REPLACE the disc instead of fusing - young, single-level, intact facets, preserved height!
Overview and Epidemiology
Discogenic back pain represents internal disc disruption (IDD) - a degenerative condition where the nucleus pulposus loses hydration and the annulus fibrosus develops painful fissures, but without frank herniation causing neural compression. This is a mechanical and chemical pain syndrome from disrupted disc architecture.
Discogenic pain is axial low back pain originating from internal disc disruption with an intact but damaged annulus. The nucleus pulposus loses proteoglycan content, causing dehydration and loss of disc height. Annular tears propagate from the nucleus outward, reaching pain-sensitive outer annular fibers. Inflammatory cytokines (IL-6, TNF-alpha, PGE2) leak into tears, sensitizing nociceptors.
Pathological Cascade
Degenerative Progression
Nucleus pulposus loses proteoglycan and water content. Disc height maintained but internal architecture disrupted. Annular tears begin centrally.
Annular fissures propagate radially outward, reaching pain-sensitive outer one-third of annulus. High-Intensity Zone (HIZ) visible on MRI. Inflammatory mediators sensitize nociceptors.
Disc height loss with endplate changes (Modic). Biomechanical instability develops. Facet loading increases. May develop segmental instability.
Disc collapse with osteophyte formation. Paradoxical stabilization (auto-fusion). Pain may improve as motion decreases ("burning out").
- Inflammatory cytokines: IL-1, IL-6, TNF-alpha
- Matrix metalloproteinases: Degrade collagen and proteoglycans
- Nerve growth factor (NGF): Ingrowth into normally aneural inner annulus
- Substance P: Nociceptive neurotransmitter in painful discs
- Loss of disc height: Increased facet loading
- Annular incompetence: Abnormal stress distribution
- Segmental instability: Excessive translation/rotation
- Endplate fracture: Modic Type 1 changes
Epidemiology and Natural History
Natural history is variable - approximately 80% of patients improve with conservative care over 6-12 months. The disc may "burn out" with progressive collapse and fibrosis, reducing pain. Younger patients with single-level disease and Modic Type 1 changes have worse prognosis.
Pathophysiology and Anatomy
Disc Anatomy
The intervertebral disc consists of three components:
- Central gelatinous core - 80% water content in youth
- Proteoglycan matrix (aggrecan) retains water
- Type II collagen provides structure
- Aneural and avascular - nutrients via diffusion from endplates
- Concentric lamellae of type I collagen fibers
- Outer one-third is innervated (sinuvertebral nerve, dorsal rami)
- 15-25 layers alternating 30-degree fiber orientation
- Anchors to vertebral endplates via Sharpey fibers
- Interface between vertebral body and disc
- Nutrient diffusion pathway for avascular disc
- Load distribution across vertebral body
- Injury causes Modic changes and disc degeneration
The outer one-third of the annulus fibrosus is innervated by:
- Sinuvertebral nerve (recurrent branch of ventral ramus) - posterior and posterolateral annulus
- Grey rami communicantes - anterolateral annulus
- Dorsal rami - posterior annulus
Inner two-thirds is normally aneural. In discogenic pain, nerve growth factor (NGF) causes aberrant nerve ingrowth into inner annulus along radial tears, creating pain-sensitive tissue in normally aneural zones.
Biomechanics of Disc Degeneration
- Normal Disc
- 80% water content, high proteoglycan
- Degenerated Disc
- Reduced to 70% water, proteoglycan loss
- Clinical Effect
- Loss of shock absorption, increased annular stress
- Normal Disc
- Normal pressure distribution
- Degenerated Disc
- Altered load transfer, peak pressures
- Clinical Effect
- Annular tears propagate, endplate injury
- Normal Disc
- Normal height maintains lordosis
- Degenerated Disc
- Collapse causes kyphosis
- Clinical Effect
- Facet overload, foraminal stenosis, sagittal imbalance
- Normal Disc
- Controlled motion within physiologic range
- Degenerated Disc
- Abnormal translation/rotation or stiffening
- Clinical Effect
- Instability (early) or autofusion (late)
Load distribution: In flexion, sitting posture increases intradiscal pressure by 200-300% compared to standing. This explains why discogenic pain is characteristically worse with sitting and flexion activities.
Classification Systems
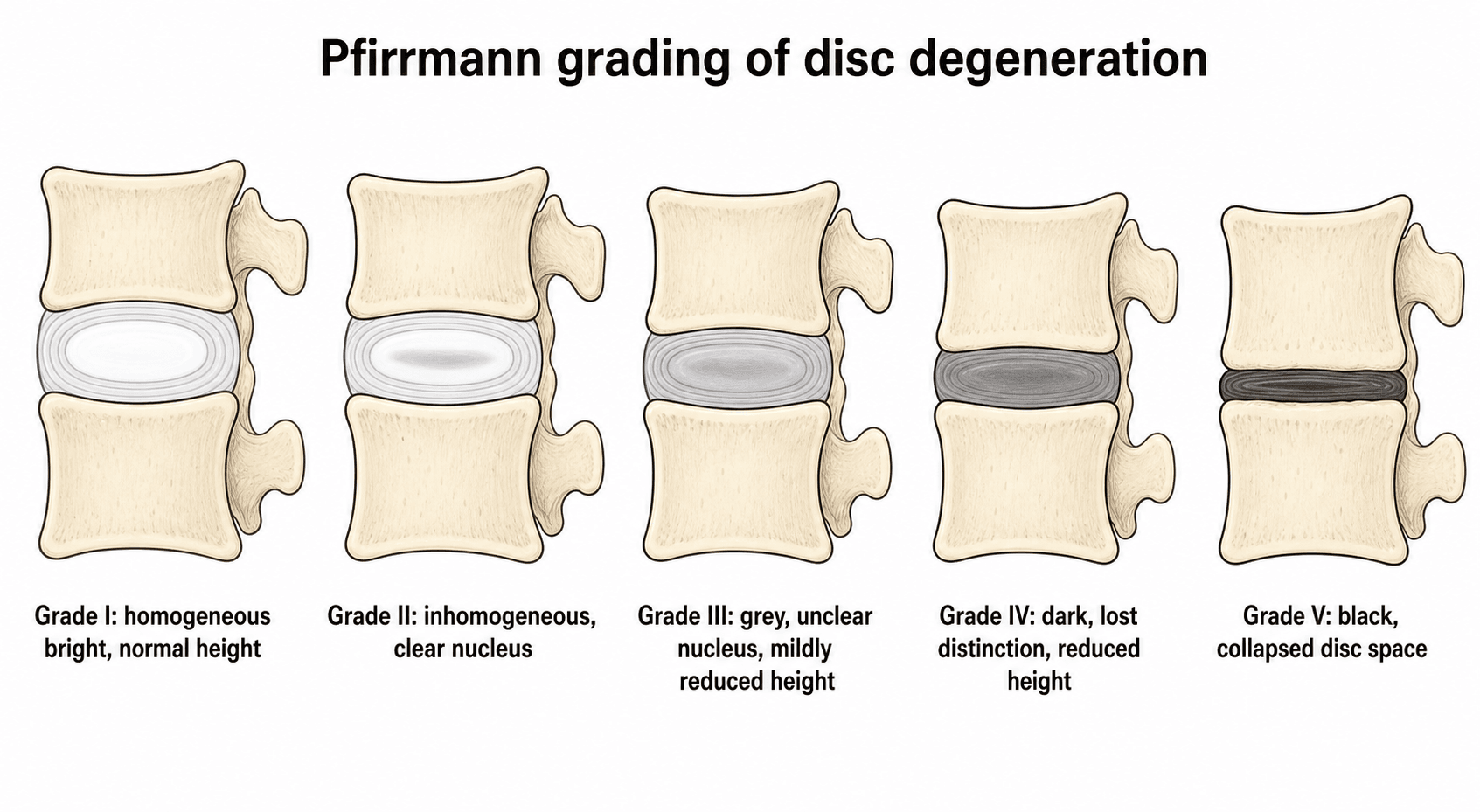
Pfirrmann MRI Classification
5-grade system based on T2 signal intensity, disc structure, and disc height. Most widely used MRI grading system for disc degeneration.
- Structure
- Homogeneous, bright white
- Distinction
- Clear nucleus-annulus distinction
- Height
- Normal
- Signal (T2)
- Hyperintense (bright)
- Structure
- Inhomogeneous with horizontal band
- Distinction
- Clear distinction maintained
- Height
- Normal
- Signal (T2)
- Hyperintense with central horizontal band
- Structure
- Inhomogeneous, grey
- Distinction
- Unclear distinction
- Height
- Normal to decreased
- Signal (T2)
- Intermediate (grey)
- Structure
- Inhomogeneous, dark grey
- Distinction
- Lost distinction
- Height
- Decreased
- Signal (T2)
- Intermediate to hypointense (dark grey)
- Structure
- Inhomogeneous, black
- Distinction
- Lost distinction
- Height
- Collapsed
- Signal (T2)
- Hypointense (black)
Grade 3-5 correlates with symptomatic disc degeneration, but Grade 3-4 changes are common in asymptomatic individuals over 40. Grade 4-5 with Modic Type 1 changes and HIZ has highest specificity for discogenic pain source.
Clinical Presentation and Assessment
- Axial low back pain: Mechanical, worse with flexion/sitting
- No radiculopathy: Pain does not radiate below knee
- Morning stiffness: Improves with movement
- Provocative activities: Prolonged sitting, bending, lifting
- Relief: Standing, walking, lying supine
- Normal neurological exam: No radiculopathy
- Range of motion: Painful flexion, limited by pain
- Straight leg raise: Negative (distinguishes from herniation)
- Provocative tests: Discogenic pain worse with flexion
- Facet loading: Negative (extension, rotation) - rules out facet source
Discogenic pain is a diagnosis of exclusion. Must rule out:
- Facet arthropathy: Pain worse with extension, positive facet loading tests
- Sacroiliac joint: Provocative SI tests (FABER, Gaenslen)
- Myofascial pain: Trigger points, muscle spasm
- Spondylolisthesis: Palpable step-off, instability on dynamic X-rays
- Red flags: Infection, tumor, fracture, cauda equina syndrome
Differential Diagnosis of Axial Low Back Pain
- Pain pattern
- Central axial, may refer to buttock/posterior thigh, not below knee
- Aggravating / relieving
- Worse with sitting and flexion; better standing/walking/lying
- Key positive finding
- Concordant pain on provocation; HIZ, Modic 1, Pfirrmann 3-5 at one level
- Discriminator from discogenic
- Reference standard for this topic
- Pain pattern
- Axial, paraspinal, may refer to buttock/thigh
- Aggravating / relieving
- Worse with extension and rotation; better with flexion
- Key positive finding
- Positive facet loading; relief with medial branch block
- Discriminator from discogenic
- Extension-worse (discogenic is flexion-worse)
- Pain pattern
- Below L5, over the joint, groin/buttock
- Aggravating / relieving
- Worse with transitional movements and single-leg loading
- Key positive finding
- Cluster of provocative tests (FABER, thigh thrust, Gaenslen, compression)
- Discriminator from discogenic
- Pain below L5 and positive SIJ cluster
- Pain pattern
- Dermatomal leg pain often exceeding back pain
- Aggravating / relieving
- Worse with sitting/Valsalva; positive tension signs
- Key positive finding
- Positive SLR/femoral stretch, dermatomal deficit, nerve-root compression on MRI
- Discriminator from discogenic
- Neurological signs and leg-dominant pain
- Pain pattern
- Insidious, age under 45, alternating buttock pain
- Aggravating / relieving
- Worse with rest and at night; better with exercise; prolonged morning stiffness
- Key positive finding
- Raised CRP, HLA-B27, sacroiliitis on MRI/X-ray
- Discriminator from discogenic
- Inflammatory rhythm (rest pain, night pain, AM stiffness)
- Pain pattern
- Constant, progressive, may be night pain
- Aggravating / relieving
- Often unrelated to posture
- Key positive finding
- Red flags - fever, weight loss, malignancy history, focal tenderness, neurology
- Discriminator from discogenic
- Red flags and constitutional symptoms - exclude first
Pain Characteristics
- Worse with sitting (intradiscal pressure highest)
- Worse with flexion (increased annular stress)
- Better with standing, walking, lying supine
- No nocturnal pain (unlike tumor)
- No constitutional symptoms (unlike infection)
- Centered in low back (L4-5 or L5-S1)
- May refer to buttocks or posterior thighs
- Does NOT radiate below knee (rules out radiculopathy)
- Not dermatomal distribution
Investigations
Imaging Protocol
AP and lateral standing X-rays. Assess disc height loss, alignment, instability. Flexion-extension views if instability suspected. Limited sensitivity for early discogenic pain.
T1 and T2 sequences. Assess disc morphology (Pfirrmann grading), High-Intensity Zone (HIZ), Modic endplate changes. Sensitivity 80-90% when combined with clinical correlation.
Intradiscal contrast injection with pressure monitoring. Concordant pain reproduction at affected level, negative at control levels. Gold standard but controversial due to potential disc injury.
Facet blocks or SI joint injections to exclude alternative pain sources. Over 50% pain relief suggests non-discogenic source.
Imaging Atlas



MRI Findings
- Description
- 5-grade system based on T2 signal and disc height
- Clinical Correlation
- Grade 4-5 = advanced degeneration, Grade 3 = intermediate
- Sensitivity
- High sensitivity (90%) but low specificity (many asymptomatic have degeneration)
- Description
- Hyperintense focal area in posterior annulus on T2
- Clinical Correlation
- Annular tear - 80% correlation with discogenic pain
- Sensitivity
- 80% sensitivity, 80% specificity for concordant discography
- Description
- Hypointense T1, hyperintense T2 in vertebral endplate
- Clinical Correlation
- Marrow edema, inflammation - correlates with pain
- Sensitivity
- 70% sensitivity for active discogenic pain
- Description
- Reduced disc space height compared to adjacent levels
- Clinical Correlation
- Advanced degeneration, may indicate instability
- Sensitivity
- Moderate correlation with pain (biomechanical loading)
Modic Type 1 (hypointense T1, hyperintense T2) = marrow edema and inflammation - correlates BEST with discogenic pain and is considered "active" inflammatory process.
Modic Type 2 (hyperintense T1, iso-hyperintense T2) = fatty replacement - chronic change, less painful.
Modic Type 3 (hypointense T1 and T2) = sclerosis - end-stage, stable.
Type 1 can progress to Type 2 with treatment or over time as inflammation resolves.
Discography - Controversial Gold Standard
Indications (highly selective):
- Failed 6+ months conservative care
- Single-level MRI abnormality with clinical correlation
- Considering fusion or disc replacement
- Multi-level degeneration - need to identify pain generator
Technique:
- Intradiscal contrast injection under fluoroscopy
- Measure opening pressure and pain reproduction
- Concordant pain = reproduces exact clinical pain at low pressure (under 15 psi above opening)
- Control levels should be negative
Controversy:
- Risk of iatrogenic disc injury (accelerated degeneration)
- High false-positive rate (20-40% in asymptomatic volunteers)
- Poor inter-rater reliability
- Many surgeons no longer perform due to concerns
DISCOGENICDiagnostic Criteria for Discogenic Pain
Hook:DISCOGENIC pain requires proving the DISC is the source - concordant provocation with all other causes excluded!
Management Algorithm
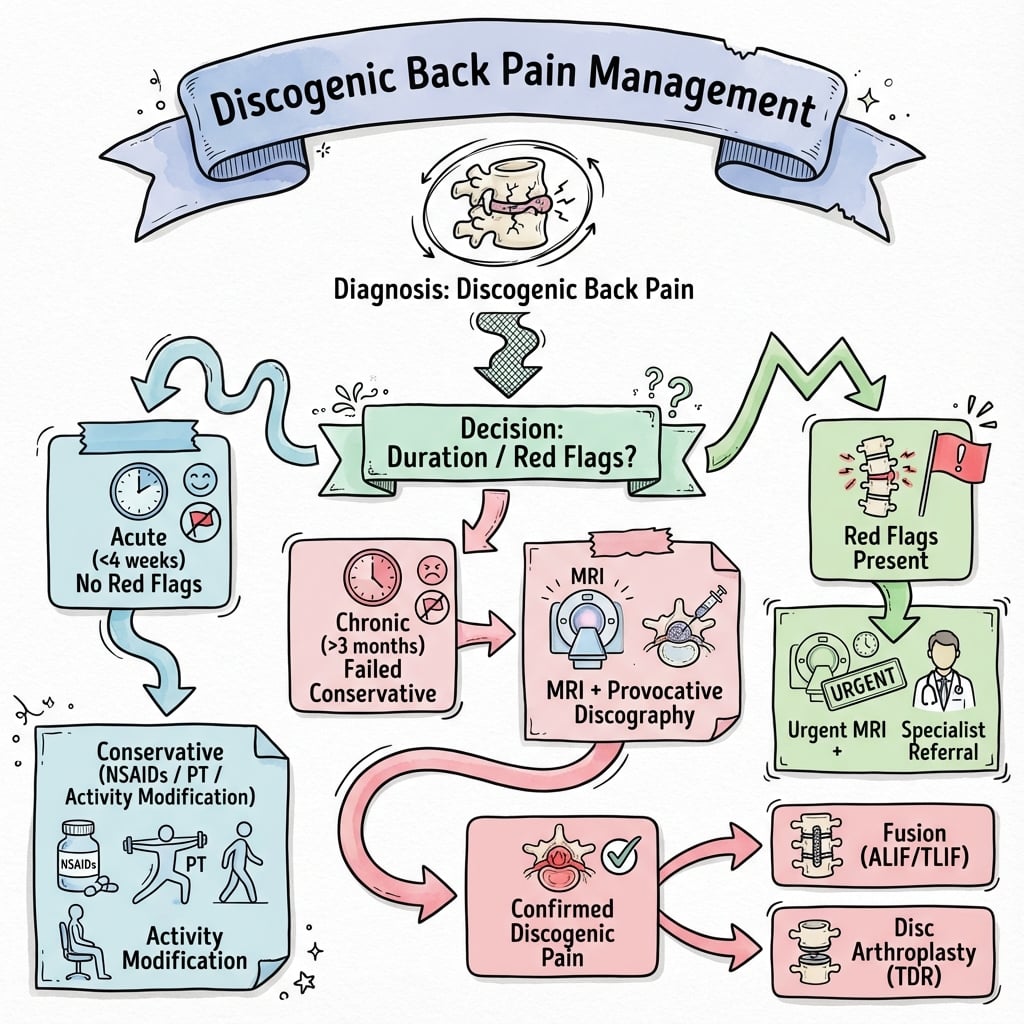
Conservative Management - First Line (Minimum 6 Months)
Conservative care is the mainstay - 80% of patients improve without surgery. Structured multimodal approach over minimum 6-12 months before considering intervention.
Conservative Treatment Pathway
Goals: Pain control, activity modification, patient education.
- NSAIDs + acetaminophen for analgesia
- Relative rest (avoid bed rest - maintain activity as tolerated)
- Patient education on natural history and prognosis
- Postural advice (avoid prolonged sitting)
Structured physical therapy program:
- Core strengthening and spinal stabilization exercises
- Flexion-based program (Williams) vs extension-based (McKenzie) - individualized
- Aerobic conditioning
- Functional restoration
If inadequate response:
- Epidural steroid injections (limited role - no direct disc effect)
- Cognitive behavioral therapy for pain coping
- Weight loss if obese (reduces biomechanical load)
- Smoking cessation (smoking impairs disc nutrition)
Assess response to conservative care. If persistent severe disability despite compliance with 6 months structured program, consider surgical evaluation. Reassess diagnosis - may not be discogenic source.
Consider surgical evaluation if:
- Severe disabling pain (VAS over 7/10) despite 6+ months conservative care
- Documented compliance with structured PT program
- Single-level MRI abnormality with concordant clinical findings
- Significant functional impairment (unable to work, ADLs compromised)
- Patient psychologically appropriate (realistic expectations, no catastrophizing)
A modern, minimally invasive option that specifically targets the endplate-mediated (vertebrogenic) component that the Modic changes above represent is basivertebral nerve (BVN) ablation (e.g. the Intracept procedure). The basivertebral nerve runs within the vertebral body and carries nociceptive fibres from the degenerate, inflamed endplates; a transpedicular radiofrequency probe ablates this nerve, denervating the painful endplates without any fusion or implant. The defined indication is chronic (over 6 months) axial low back pain with Modic Type 1 or Type 2 changes at L3-S1 that has failed conservative care — that is, it selects the same Modic-endplate subgroup identified earlier as the most painful. RCT and sham-controlled data (the SMART and INTRACEPT trials) show durable improvements in pain and disability, and it is motion-preserving (nothing is fused), making it a genuine alternative to fusion in the carefully-selected vertebrogenic patient. The exam point: when the pain generator is the Modic endplate rather than the disc itself, BVN ablation treats the nerve, not the joint.
A genuinely controversial but examinable idea is that some Modic Type 1 changes reflect a chronic low-grade disc infection by anaerobic, low-virulence skin commensals — principally Cutibacterium (formerly Propionibacterium) acnes — that seed the disc (for example after an annular tear or prior surgery) and drive the endplate inflammation. On this basis, prolonged oral antibiotics (long-course amoxicillin-clavulanate, around 3 months) — "Modic Antibiotic Spine Therapy (MAST)" — were proposed, and the original Albert RCT (2013) reported benefit in chronic low back pain with Modic Type 1 changes following a previous disc herniation. The status to convey in a viva is deliberately cautious: the hypothesis is biologically plausible and supported by some culture data, but it is confounded by skin-commensal contamination, has not been consistently reproduced, and prolonged antibiotics carry real harms and resistance concerns, so MAST is not standard care and remains investigational. The exam point: know that the C. acnes / Modic-1 antibiotic hypothesis exists and why it is unproven, rather than recommending antibiotics for back pain.
Interventional and Surgical Management
Surgical Patient Selection
Surgery is reserved for highly selected patients with failed conservative care and confirmed discogenic source.
- Single-level disc degeneration (L4-5 or L5-S1)
- Failed 6+ months structured conservative care
- Concordant MRI findings (HIZ, Modic 1, Pfirrmann 4-5)
- Positive discography (if performed) - concordant pain
- Normal neurological exam - no radiculopathy
- Age under 60 (for disc replacement consideration)
- Psychologically appropriate - realistic expectations
- No litigation or workers' compensation
- Multi-level disease (poor outcomes)
- Facet arthropathy or spondylolisthesis (needs fusion)
- Psychosocial factors (depression, catastrophizing)
- Smoking (fusion non-union risk)
- Obesity (worse outcomes)
- Active litigation (poor prognostic factor)
- Inadequate conservative trial (under 6 months)
- Unclear pain generator (multi-source pain)
Surgical outcomes for discogenic pain are less predictable than decompression for stenosis or herniation. Patient selection is critical.
Complications
- Incidence
- 5-15% (higher in smokers)
- Risk Factors
- Smoking, obesity, multi-level, diabetes, NSAID use
- Management
- Revision fusion with bone grafting, biologics (BMP), address risk factors
- Incidence
- 15-30% at 10 years
- Risk Factors
- Pre-existing degeneration, biomechanical stress, age
- Management
- Conservative care first, revision fusion if symptomatic with failed conservative care
- Incidence
- 1-5%
- Risk Factors
- Anterior approach, vessel mobilization
- Management
- Immediate vascular repair, access surgeon on standby, hemodynamic resuscitation
- Incidence
- 1-5% males
- Risk Factors
- Superior hypogastric plexus injury during L5-S1 approach
- Management
- Irreversible - counsel preoperatively, consider sperm banking
- Incidence
- 1-3%
- Risk Factors
- Neural retraction, instrumentation malposition
- Management
- Decompress if hematoma, remove hardware if malpositioned, observation if neuropraxia
- Incidence
- 3-10%
- Risk Factors
- Posterior approaches, revision surgery
- Management
- Primary repair, fibrin glue, bed rest, consider lumbar drain if persistent CSF leak
- Incidence
- 5-10%
- Risk Factors
- Osteoporosis, oversizing, endplate injury
- Management
- Observation if asymptomatic, revision to fusion if symptomatic with height loss
- Incidence
- 1-3% (higher with fusion)
- Risk Factors
- Obesity, diabetes, prolonged surgery, revision
- Management
- Antibiotics, washout and debridement if deep, hardware retention if stable fusion
Adjacent segment disease (ASD) develops in 15-30% of patients at 10 years post-fusion. Risk factors include pre-existing degeneration (MRI changes at index surgery), biomechanical stress transfer, and older age. Disc replacement theoretically reduces ASD by preserving motion, but long-term clinical benefit unclear. Many cases of ASD are asymptomatic radiographic degeneration - only 5-10% require revision surgery.
Outcomes and Prognosis
Fusion Outcomes
Success rates: 60-70% good to excellent outcomes at 2-5 years in well-selected patients. Results are less predictable than decompression surgery for stenosis or herniation.
Predictors of poor outcome:
- Multi-level disease
- Psychosocial factors (depression, catastrophizing, litigation)
- Smoking (doubles pseudarthrosis risk)
- Obesity
- Workers' compensation or litigation status
- Inadequate conservative trial (under 6 months)
- Unclear pain generator (multiple sources)
Disc Replacement Outcomes
Success rates: 70-80% good to excellent outcomes at 5 years, similar to fusion. Lower adjacent segment disease radiographically (15% vs 30%), but unclear if clinically significant.
Failures: Facet arthropathy develops in 10-15% (contraindication to ADR). Implant loosening or wear over long-term (over 10 years) unknown.
Natural History Without Surgery
80% of patients improve with conservative care over 6-12 months. Disc may "burn out" with progressive collapse and fibrosis. Younger patients with Modic Type 1 changes have worse natural history.
Guidelines, Registries & Global Practice
Global Epidemiology
Low back pain is the single leading cause of years lived with disability worldwide; global disability from low back pain rose by 54% between 1990 and 2015, driven mainly by population growth and ageing, with the steepest rise in low- and middle-income countries (Hartvigsen, Lancet 2018). For the large majority of patients no specific nociceptive cause can be identified, and only a small minority have a clearly defined pathology such as fracture, malignancy or infection. Discogenic (internal disc disruption) pain is therefore a sub-diagnosis applied to a fraction of chronic axial low back pain, and degenerative MRI findings - including disc desiccation, anular tears, high-intensity zones and Modic changes - are common in entirely asymptomatic adults, rising in prevalence with age (Kjaer, Spine 2005). Physically demanding work, smoking, obesity, psychological distress and low socioeconomic status are the most consistent risk factors for reporting disabling low back pain.
Major Guidelines Side by Side
- Core recommendation
- Exercise programmes, manual therapy within a package, psychological (CBT) therapy; offer combined physical and psychological programme for persistent disabling pain
- Stance on fusion for discogenic / non-specific pain
- Do NOT offer spinal fusion for low back pain except as part of a randomised controlled trial; imaging only if it would change management
- Evidence strength
- Strong - based on RCTs including the MRC trial
- Core recommendation
- First-line non-pharmacological care (exercise, CBT, multidisciplinary rehabilitation); NSAIDs as first-line drug therapy
- Stance on fusion for discogenic / non-specific pain
- Fusion an option only in carefully selected patients after exhaustive non-operative care; outcomes less predictable than for radiculopathy or instability
- Evidence strength
- Moderate - conflicting RCTs (Fritzell positive, Brox and MRC neutral)
- Core recommendation
- Active rehabilitation and self-management; reserve surgery for a minority with concordant single-level disease
- Stance on fusion for discogenic / non-specific pain
- Arthroplasty acceptable in strictly selected single-level patients with intact facets and preserved height; otherwise non-operative or fusion
- Evidence strength
- Moderate - registry and IDE-trial informed
- Core recommendation
- Education, staying active and simple analgesia emphasised; advanced imaging and surgery scarce
- Stance on fusion for discogenic / non-specific pain
- Fusion and arthroplasty rarely available; conservative care is the default pathway
- Evidence strength
- Pragmatic - resource-driven
The world standard of care for chronic non-specific and discogenic low back pain is active rehabilitation, exercise and psychologically informed management, not surgery. NICE explicitly advises against fusion for low back pain outside a trial. Fusion may help a narrowly selected subgroup (single concordant level, exhausted conservative care), but RCTs that used genuine active rehabilitation (Brox, MRC) showed no clear surgical advantage, whereas the older Swedish trial (Fritzell) - which compared fusion with unstructured physiotherapy - favoured surgery. Quoting these three trials and their differing comparators is high-yield.
Registry and Device-Trial Evidence
- Arthroplasty IDE trials: The CHARITE and ProDisc-L FDA investigational device exemption RCTs underpin regulatory approval of lumbar total disc replacement, showing non-inferiority to fusion at 2 and 5 years with preserved segmental motion in selected single-level patients (Guyer, Spine J 2008).
- Spine registries (for example Sweden's Swespine, the British Spine Registry and several national arthroplasty/spine registries) collect patient-reported outcomes and revision data; they consistently show that outcomes of fusion for axial low back pain are less predictable than for decompression of radiculopathy or stenosis, and that careful patient selection drives results.
Practice Variation
Rates of lumbar fusion vary several-fold between and within countries for similar presentations, reflecting differences in reimbursement, surgeon preference, access to multidisciplinary rehabilitation and medicolegal climate rather than differences in disease. High-resource systems show rising arthroplasty and fusion volumes; lower-resource systems rely almost entirely on conservative care. This unexplained variation is itself an argument for adhering to guideline thresholds and shared decision-making.
Consent and Documentation (Globally Applicable)
- Approach-specific (ALIF): vascular injury (1-5%), retrograde ejaculation in males (1-5%), sympathetic and visceral injury
- General fusion / arthroplasty: pseudarthrosis (5-15%, doubled by smoking), adjacent segment disease (15-30% radiographic at 10 years), nerve injury (1-3%), infection (1-3%)
- Realistic outcome: roughly 60-70% good result, less predictable than decompression; persistent pain in a substantial minority
- Record the duration and modalities of failed conservative care (active rehabilitation, psychological therapy, analgesia)
- Confirm a concordant single pain generator and exclusion of facet, sacroiliac and psychosocial contributors
- Document shared decision-making and that guideline thresholds were met before offering surgery
- Identify poor prognostic factors (psychological distress, ongoing compensation/litigation) and address before surgery
Discogenic back pain surgery has high medicolegal risk due to less predictable outcomes compared to decompression surgery. Critical documentation includes:
- Informed consent: realistic expectations, 60-70% success rate, risk of persistent pain
- Conservative trial: minimum 6 months documented structured PT, medications, injections
- Patient selection: psychological screening, exclude catastrophizing, litigation, workers comp
- Surgical planning: concordant MRI findings, consider discography if multi-level degeneration
- Approach-specific risks: ALIF retrograde ejaculation (1-5% males), vascular injury (1-5%)
MCQ Practice Points
Q: Which Modic change type on MRI correlates BEST with active discogenic pain? A: Modic Type 1 (hypointense T1, hyperintense T2) represents marrow edema and inflammation, correlating most strongly with active discogenic pain. Type 2 (fatty replacement) is chronic and less painful. Type 3 (sclerosis) is end-stage.
Q: What is the High-Intensity Zone (HIZ) on MRI and what is its clinical significance? A: HIZ is a hyperintense focal area in the posterior annulus on T2-weighted MRI, representing an annular tear. It has 80% sensitivity and 80% specificity for concordant pain on discography. Correlates with full-thickness radial annular tears reaching pain-sensitive outer annulus.
Q: What percentage of patients with discogenic back pain improve with conservative care, and what is the minimum trial period before considering surgery? A: 80% of patients improve with structured conservative care over 6-12 months. Minimum 6 months of structured PT, activity modification, and multimodal analgesia should be completed before surgical consideration. Surgery is reserved for failed conservative care with concordant MRI findings.
Q: What are the ideal patient criteria for lumbar disc replacement vs fusion? A: Disc replacement ideal criteria: age under 60, single-level L4-5 or L5-S1, preserved disc height (over 5mm), intact facet joints (no arthropathy), normal alignment (scoliosis under 11 degrees), no spondylolisthesis, normal bone quality. Fusion preferred if any contraindication present (facet disease, multi-level, instability, older age).
Q: What do the randomised trials show regarding fusion versus conservative care for chronic discogenic low back pain? A: The evidence hinges on the comparator. The Swedish Lumbar Spine Study (Fritzell 2001) found fusion better than unstructured physiotherapy (back pain reduced 33% vs 7%). However, when surgery was compared with genuine active rehabilitation, the Brox RCT (2003) and the MRC Spine Stabilisation Trial (Fairbank 2005) found no clear advantage of fusion - the MRC ODI difference of -4.1 only just reached the minimal clinical difference. This underpins NICE NG59, which advises against fusion for low back pain outside a trial.
Q: What is the incidence of adjacent segment disease after lumbar fusion and what are the risk factors? A: Adjacent segment disease (ASD) develops in 15-30% of patients at 10 years post-fusion (radiographic). Only 5-10% require revision surgery. Risk factors include pre-existing degeneration on MRI at index surgery, biomechanical stress transfer from fused segment, and older age. Disc replacement theoretically reduces ASD by preserving motion (16% vs 28% in studies), but clinical significance unclear.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old office worker presents with 18 months of mechanical low back pain. Pain is worse with sitting and bending, better with standing. No leg pain. Failed physiotherapy and NSAIDs. MRI shows Pfirrmann Grade 4 degeneration at L5-S1 with High-Intensity Zone (HIZ) and Modic Type 1 changes. What is your diagnosis and management?”
“The patient from Scenario 1 has now completed 8 months of structured conservative care including PT, weight loss, and medications, but continues to have severe disabling pain (VAS 8/10). Discography performed shows concordant pain at L5-S1 at low pressure, negative at L4-5. Facet joints appear intact on MRI and CT. The patient is 35 years old, non-smoker, psychologically appropriate. Discuss your surgical options and decision-making.”
“You performed an ALIF fusion at L5-S1 for discogenic pain in a 45-year-old male. At 12 months post-op, the patient has persistent pain similar to preoperative levels. CT scan shows lucency around the interbody cage with no bridging bone. What is your assessment and management?”
Key Pathophysiology
- Internal disc disruption (IDD) = nucleus dehydration + annular tears WITHOUT frank herniation
- Inflammatory cytokines (IL-6, TNF-alpha) in annular tears sensitize nociceptors
- Nerve ingrowth into normally aneural inner annulus (NGF-mediated)
- Modic Type 1 (marrow edema) = most painful, Type 2 (fatty replacement) = chronic, Type 3 (sclerosis) = end-stage
MRI Classification
- Pfirrmann Grade 1-2 = normal to early degeneration (bright T2 signal)
- Pfirrmann Grade 3 = intermediate degeneration (grey T2 signal)
- Pfirrmann Grade 4-5 = advanced degeneration (dark T2 signal, collapsed)
- HIZ (High-Intensity Zone) = annular tear, 80% sensitivity/specificity for discogenic pain
- Modic Type 1 = hypointense T1, hyperintense T2 = inflammation = most painful
Diagnosis
- Diagnosis of EXCLUSION - rule out facet, SI joint, myofascial sources
- Mechanical axial pain worse with sitting/flexion, better with standing/walking
- Normal neurological exam - NO radiculopathy (distinguishes from herniation)
- Provocative discography = concordant pain reproduction (controversial - 20-40% false positive)
Treatment Algorithm
- Conservative FIRST - minimum 6 months structured PT, core strengthening, multimodal analgesia
- 80% improve with conservative care - surgery is last resort
- Surgery if: failed 6+ months conservative, concordant MRI findings, single-level, no psychosocial red flags
- Fusion vs disc replacement: ADR if age under 60, preserved height, intact facets, single-level
Surgical Pearls
- ALIF preferred for L5-S1 (large footprint, lordosis restoration, direct access)
- TLIF for L4-5 or if need decompression (unilateral approach, single position)
- Disc replacement: requires REPLACE criteria (Range, Early, Posterior facets, Level, Age, Coronal, Endplates)
- Supplement with posterior pedicle screws for stability (fusion rate over 95% vs 70-80% stand-alone)
Complications
- Pseudarthrosis 5-15% (doubles in smokers) - revise with posterior fusion + bone graft + BMP
- Adjacent segment disease 15-30% radiographic at 10 years (5-10% need revision surgery)
- ALIF specific: vascular injury 1-5%, retrograde ejaculation 1-5% (counsel males, sperm banking)
- Outcomes: 60-70% success with fusion, less predictable than decompression surgery
Evidence Base and Key Trials
Pfirrmann MRI Grading of Disc Degeneration - Original Classification
- Reliability study deriving a 5-grade T2 MRI classification of lumbar disc degeneration from 300 discs in 60 patients
- Grades defined by nucleus signal and structure, nucleus-annulus distinction and disc height
- Intra-observer agreement kappa 0.84-0.90 and inter-observer kappa 0.69-0.81 (substantial to excellent)
- Complete agreement in 83.8% of discs, a one-grade difference in 15.9%
- Now the most widely used grading system for disc degeneration in research and practice
Modic Vertebral Endplate Changes - Original Description
- Defined the MR signal patterns of vertebral body marrow change adjacent to degenerating discs
- Type 1: hypointense T1, hyperintense T2 - marrow oedema and inflammation (most associated with pain)
- Type 2: hyperintense T1, iso/hyperintense T2 - fatty marrow replacement
- Type 3: hypointense T1 and T2 - subchondral bony sclerosis (end-stage)
- Established that endplate marrow change reflects the bony response to disc degeneration
Brox RCT - Instrumented Fusion vs Cognitive Intervention and Exercise
- Single-blind RCT, 64 patients aged 25-60 with chronic low back pain over 1 year and L4-S1 disc degeneration
- Instrumented posterolateral fusion versus a brief cognitive intervention plus structured exercise
- Oswestry Disability Index improved 41 to 26 after fusion versus 42 to 30 after cognitive intervention and exercise
- Mean between-group ODI difference only 2.3 (95% CI -6.7 to 11.4, P=0.33) - no significant advantage of fusion
- Success rate 70% (surgery) versus 76% (non-operative); early surgical complication rate 18%
MRC Spine Stabilisation Trial - Fusion vs Intensive Rehabilitation
- Multicentre RCT, 349 patients aged 18-55 with chronic low back pain over 1 year, candidates for fusion (15 UK centres)
- Lumbar spinal fusion versus an intensive rehabilitation programme based on cognitive behavioural principles
- Oswestry Disability Index at 24 months: surgery 46.5 to 34.0 vs rehabilitation 44.8 to 36.1
- Mean ODI difference -4.1 (95% CI -8.1 to -0.1, P=0.045), only just reaching the predefined minimal clinical difference
- No significant difference in the shuttle walking test or any secondary outcome
Swedish Lumbar Spine Study (2001 Volvo Award) - Fusion vs Non-surgical Care
- Multicentre RCT, 294 patients aged 25-65 with chronic low back pain over 2 years and disc degeneration at L4-L5 and/or L5-S1 (19 Swedish centres)
- Three fusion techniques (pooled) versus continued physiotherapy
- At 2 years back pain fell 33% in the surgical group versus 7% non-surgical (P=0.0002)
- Oswestry Disability Index fell 25% (47 to 36) versus 6% (48 to 46); 63% rated themselves much better/better versus 29% (P less than 0.0001)
- Net return-to-work rate 36% versus 13% (P=0.002); early surgical complication rate 17%
CHARITE Artificial Disc vs ALIF - FDA IDE 5-Year Follow-up
- Prospective multicentre RCT (375 originally enrolled; 133 randomised patients completed 5-year follow-up) for single-level L4-S1 degenerative disc disease unresponsive to non-operative care
- CHARITE total disc replacement versus ALIF with BAK cages and iliac crest autograft
- Overall success at 5 years 57.8% (CHARITE) versus 51.2% (BAK) - non-inferiority maintained from the 2-year data
- Mean index-level range of motion preserved at 6.0 degrees (CHARITE) versus 1.0 degree (BAK)
- Additional index-level surgery 7.7% (CHARITE) versus 16.3% (BAK); long-term disability 8.0% versus 20.9% (P=0.044)
MRI Findings and Low Back Pain in 40-Year-Olds
- Cross-sectional general-population cohort - lumbar MRI in 412 forty-year-old men and women
- MRI read blind to symptoms; associations with low back pain quantified by odds ratios
- Modic changes and anterolisthesis showed the strongest associations with low back pain (odds ratios greater than 4)
- Hypointense disc signal, reduced disc height and Modic changes were significantly positively associated with all low back pain variables
- Nerve root compromise, Modic changes and central stenosis were each present in fewer than 25% of this population
Discography in Previously Asymptomatic Subjects - Iatrogenic Pain and False Positives
- Prospective controlled study, 26 subjects without pre-existing low back pain observed for 1 year after experimental lumbar discography
- No subject with normal psychometric testing reported persistent pain after discography (0 of 11)
- Six of 15 subjects (40%) with abnormal psychometric testing reported significant new low back pain at 1 year
- Persistent pain occurred in 0% of the pain-free group, 20% with chronic neck pain, and 66% with somatisation disorder
- Psychological profile and occupational disability strongly predicted a painful response - the core driver of false positives