(and Distraction Interposition Arthroplasty)
- Interposition arthroplasty of the elbow is a JOINT-PRESERVING, BONE-PRESERVING alternative to total elbow arthroplasty (TEA), indicated mainly for the YOUNG, HIGH-DEMAND patient with end-stage elbow arthritis (most often POST-TRAUMATIC, sometimes inflammatory) - because TEA in a young, active patient has a high failure rate and imposes a strict lifelong lifting restriction (often around 2-5 kg), which such patients cannot accept.
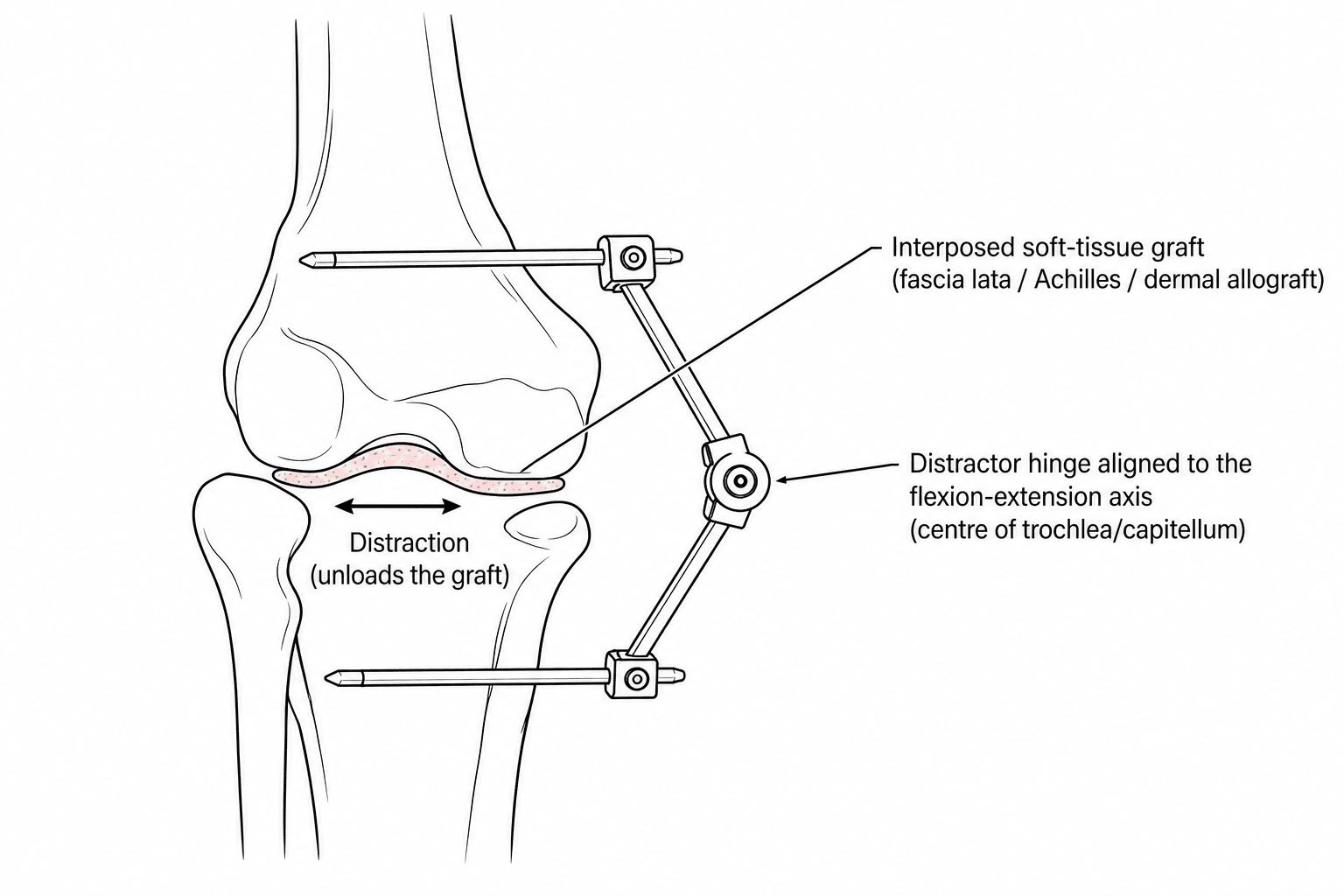
- The TECHNIQUE resurfaces the arthritic, debrided and contoured articular surface of the distal humerus with an INTERPOSED SOFT-TISSUE GRAFT - classically autologous FASCIA LATA, or an ACHILLES TENDON or DERMAL ALLOGRAFT - which acts as a biological resurfacing layer between the humerus and the ulna/radius, relieving pain while preserving bone and motion.
- DISTRACTION INTERPOSITION ARTHROPLASTY adds a HINGED DISTRACTION EXTERNAL FIXATOR (applied for around 3-4 weeks): the distractor separates the articular surfaces to UNLOAD and PROTECT the interposed graft and maintain the joint space, while its hinge (aligned to the elbow's flexion-extension axis) allows EARLY, protected MOTION - particularly valuable where there is instability or to protect the graft.
- The single most important determinant of success is ELBOW STABILITY: instability of the elbow, both before and after surgery, is strongly associated with UNSATISFACTORY results, so the collateral ligaments and the bony columns must be competent, and the distraction fixator helps protect a potentially unstable elbow during healing; note that in the largest series pre-operative instability did badly DESPITE attempted collateral reconstruction, so demonstrable instability - especially if both collaterals would need reconstructing - argues against the operation rather than for a larger one; modern practice may allow immediate protected motion in a hinged brace WITHOUT external distraction when ligamentous stability is good.
- OUTCOMES are MODEST but useful: reported satisfactory pain relief in roughly two-thirds of patients (e.g. about 69% satisfactory pain relief and 62% excellent/good Mayo scores in the classic series), with similar results for post-traumatic and inflammatory arthritis - but it is LESS RELIABLE than prosthetic replacement, and complications (including ulnar nerve problems and graft/fixator-related issues) are not uncommon, especially in post-traumatic cases.
- A key advantage is that interposition arthroplasty does NOT 'burn bridges': because it preserves bone, a FAILED interposition can be CONVERTED to a TOTAL ELBOW ARTHROPLASTY later (with good results in reported cases), so it is a reasonable joint-preserving first step for the young arthritic elbow, reserving the motion-and-load-limited but more reliable TEA for older/lower-demand patients or as the eventual salvage.
- “Elbow interposition arthroplasty = joint/bone-preserving alternative to TEA for the YOUNG, HIGH-DEMAND arthritic (usually post-traumatic) elbow (TEA has a strict lifelong lifting limit + high failure in the young).
- “Resurface the debrided distal humerus with an interposed SOFT-TISSUE graft (fascia lata, Achilles/dermal allograft); a HINGED DISTRACTION external fixator (~3-4 weeks) unloads/protects the graft and allows early motion.
- “STABILITY is critical (instability predicts failure - reconstruct ligaments/columns). Outcomes modest (~60-70% satisfactory), less reliable than TEA; a failed interposition CONVERTS to TEA.
For the young, high-demand patient with end-stage (usually post-traumatic) elbow arthritis where TEA is undesirable (lifelong lifting limit, high failure in the young).
Interpose a soft-tissue graft over the debrided distal humerus; a hinged distraction fixator unloads/protects it and allows early motion. Stability is critical; convertible to TEA.
Indication, Technique & the Stability Principle
Interposition arthroplasty is a joint- and bone-preserving alternative to total elbow arthroplasty for the young, high-demand patient with end-stage (usually post-traumatic) elbow arthritis, in whom TEA's high failure rate and strict lifelong lifting limit are unacceptable. The arthritic distal humerus is debrided and contoured and resurfaced with an interposed soft-tissue graft - fascia lata, or Achilles/dermal allograft - which biologically resurfaces the joint while preserving bone and motion. A hinged distraction external fixator (classically 3-4 weeks) may be added to unload and protect the graft and maintain the joint space while allowing early motion, especially where there is instability. The decisive factor is elbow STABILITY: instability before or after surgery predicts failure, so the ligaments and columns must be competent or reconstructed. Outcomes are modest (~60-70% satisfactory) and less reliable than TEA, but a failed interposition can be converted to TEA.
- Interposition (+/- distraction)
- Young, high-demand, end-stage (post-traumatic) arthritis
- Total elbow arthroplasty (TEA)
- Older, lower-demand (or RA); inflammatory arthritis
- Interposition (+/- distraction)
- Preserves bone; convertible to TEA
- Total elbow arthroplasty (TEA)
- Sacrifices bone; revision is harder
- Interposition (+/- distraction)
- No strict lifelong lifting limit
- Total elbow arthroplasty (TEA)
- Strict lifelong limit (~2-5 kg)
- Interposition (+/- distraction)
- Modest (~60-70% satisfactory)
- Total elbow arthroplasty (TEA)
- More reliable/predictable
- Interposition (+/- distraction)
- STABILITY essential; instability -> failure
- Total elbow arthroplasty (TEA)
- Polyethylene bushing wear, loosening, periprosthetic fracture
Contraindications & Choosing the Right Patient
- Active or recent infection. Post-traumatic elbows often carry a history of prior surgery and infection; active sepsis is a contraindication, and a prior deep infection demands confidence the elbow is quiescent before interposing a graft.
- Gross, uncorrectable instability or deficient columns. Because stability is the dominant determinant of success, an elbow that is grossly unstable with collateral ligaments and columns that cannot be reconstructed is a relative contraindication - the graft will not survive a sloppy, poorly-contained joint.
- A neuropathic (Charcot) joint. A destroyed, insensate joint is unsuitable for a soft-tissue resurfacing. (Charcot of the elbow is covered in our Neuropathic (Charcot) Elbow topic.)
- An inadequate soft-tissue envelope (poor skin, scarred or contracted soft tissues) that cannot support the graft or tolerate a fixator.
- Where it sits among the alternatives. Interposition is one rung on a ladder: simpler debridement ("ulnohumeral") arthroplasty suits impingement-type osteoarthritis with preserved joint space; arthrodesis is a definitive salvage for the very heavy labourer or the failed/infected elbow that cannot be reconstructed; and TEA remains the reliable choice for the older, lower-demand patient (and the eventual salvage of a failed interposition). (The osteoarthritis treatment ladder and debridement arthroplasty are developed in our Elbow Arthritis topic.) Interposition is chosen specifically for the young, high-demand patient who needs pain relief and retained load capacity without burning the bony bridges to a future TEA.
Contraindications: active/unsettled infection, gross uncorrectable instability / deficient columns, a neuropathic (Charcot) joint, and a poor soft-tissue envelope. Position it on the ladder - debridement arthroplasty for impingement-type OA, arthrodesis as a heavy-labourer/salvage definitive, TEA for the older/low-demand - with interposition reserved for the young high-demand elbow that must keep its bone stock.
Outcomes, Complications & Conversion
- Outcomes: roughly two-thirds satisfactory pain relief (e.g. ~69% satisfactory, ~62% excellent/good Mayo scores in the classic distraction-interposition series), similar for post-traumatic and inflammatory arthritis - less reliable than TEA.
- Stability is everything: competent or reconstructed collateral ligaments and bony columns; the distraction fixator protects an unstable elbow during healing; with good stability, immediate protected motion in a hinged brace without external distraction is feasible.
- Complications: ulnar nerve problems (consider decompression/transposition), instability, graft/fixator issues, pin-site problems, and the chance of persistent pain - more frequent in post-traumatic cases.
- Conversion: a failed interposition arthroplasty can be converted to a total elbow arthroplasty later, so it does not preclude future prosthetic replacement - a reasonable first step in the young arthritic elbow.
What the larger series actually shows
The "roughly two-thirds satisfactory" figure comes from a 13-patient series, and the largest published experience is more sobering. In 45 elbows at a mean of six years, the flexion-extension arc improved substantially (51 to 97 degrees) and the Mayo Elbow Performance Score rose from 41 to 65 - but 65 is a fair score, and when the results were graded only 13 were good or excellent against 14 fair, 11 poor and 7 revised. The authors' own conclusion is the one to quote in a viva: interposition neither completely eliminates pain nor restores full function, and is best presented to the patient as a salvage procedure that buys a functional arc and a better elbow rather than a normal one.
That series also sharpens the stability rule in a way that matters at the decision-making stage. Pre-operative instability was associated with poor scores despite attempted collateral reconstruction, and four of the five patients in whom both collateral ligaments were reconstructed ended up with a net decrease in Mayo score. The safer reading is therefore not "reconstruct the ligaments and proceed" but that demonstrable pre-operative instability is a reason not to do the operation - a bi-collateral reconstruction is a marker of an elbow too far gone for a soft-tissue resurfacing, not a step that rescues it.
Do not quote interposition as a two-thirds-good operation. Counsel it as a salvage that reliably improves the arc and partially improves pain, leaving a fair Mayo score, in exchange for keeping the bone stock that makes a later TEA possible. Pre-operative instability requiring both collateral ligaments to be reconstructed argues against the operation, not for a bigger one.
The decisive lesson of elbow interposition arthroplasty is that STABILITY determines success: instability of the elbow, present before surgery or resulting from the debridement, is strongly associated with unsatisfactory results, so the procedure must restore or rely on competent collateral ligaments and bony columns, and a hinged distraction external fixator is used to protect and unload the graft - and to protect an unstable elbow - during healing. It is offered to the young, high-demand patient specifically because total elbow arthroplasty is ill-suited to them (a strict lifelong lifting limit and a high failure rate), and its key advantages are bone preservation and the ability to be converted to a TEA later if it fails. But it must be presented honestly: the results are modest and less reliable than prosthetic replacement, complications such as ulnar neuropathy are not uncommon, and an unstable elbow is a relative contraindication unless the instability can be corrected.
The Operation, Step by Step
- Exposure. An extensile posterior approach is used, managing the triceps either by a triceps-reflecting/ triceps-splitting window or an olecranon-sparing exposure that preserves the extensor mechanism. The ulnar nerve is identified, protected and usually transposed/decompressed at the outset (ulnar neuropathy is the commonest neurological complication). (The detailed posterior approach is covered in our Surgical Approaches to the Shoulder & Elbow topic; ulnar nerve handling in our Ulnar Nerve topics.)
- Joint preparation. The arthritic distal humerus is debrided of osteophytes and devitalised cartilage and re-contoured to a smooth, congruent trochlea/capitellum shape; the olecranon and coronoid/radial head are addressed as needed. Enough bone is removed to relieve impingement and create a space for the graft while preserving the bony columns that confer stability.
- The interposition graft. Autologous fascia lata is harvested from the thigh (or an Achilles tendon or dermal allograft is used), draped over the contoured distal humerus and secured through drill holes in the humerus (and sometimes around the epicondyles) so it covers the articulating surface as a biological resurfacing layer.
- Restore stability. The medial and lateral collateral ligaments and the columns must be competent - repaired or reconstructed if deficient - because instability is the dominant predictor of failure. (Isolated collateral-ligament reconstruction is covered in our Elbow UCL Injury and Posterolateral Rotatory Instability topics.)
- The distractor and its axis. A hinged distraction external fixator is applied so its hinge lies on the elbow's true flexion-extension axis - a line through the centre of the trochlea and the centre of the capitellum (anterior and inferior to the lateral epicondyle). An axis pin placed along this line guides the hinge; the joint is then distracted a few millimetres to unload the graft while permitting early protected motion. The fixator is classically retained for around three to four weeks.
- Rehabilitation. Early protected motion (through the fixator hinge, or - when ligamentous stability is good - immediately in a hinged brace without a distractor) prevents stiffness while the graft incorporates.
Get the distractor hinge on the flexion-extension axis - a line through the centre of the trochlea and capitellum, anterior-inferior to the lateral epicondyle - or the construct fights motion and loads the graft. The other non-negotiables are a competent/reconstructed ligament-and-column complex and protecting the ulnar nerve (commonest neurological complication).
Postoperative Care, Complications and What to Warn About
The rehabilitation, which is part of the operation
The graft is a passive spacer that survives on an elbow that moves; a stiff post-operative elbow defeats the whole exercise, so rehabilitation begins within the first few days rather than after the fixator comes off. Where a hinged distractor has been applied, motion is performed through the hinge from the outset, with the joint held distracted a few millimetres so the graft is unloaded while it is being moved. Pin sites are cleaned daily and reviewed at every visit, since a neglected pin track is the commonest route to an infection sitting directly over a fresh soft-tissue graft. The frame typically comes off at around three to four weeks, after which motion continues in a hinged brace.
Beyond that, the pattern of therapy is the one used for any released stiff elbow: active and active-assisted motion in both flexion-extension and pronation-supination, static progressive or turnbuckle splinting to recover the end of the arc, and extension splinting at night, since it is extension that is lost first and regained last. Heterotopic ossification prophylaxis is worth considering in the elbow that has had multiple prior operations or a head injury, though the choice between indomethacin and radiation remains debated. Crucially, and unlike TEA, there is no permanent lifting restriction to impose once healing is complete - that freedom is the entire reason the patient accepted a less predictable operation.
The complications to consent for
- Ulnar neuropathy - the commonest neurological problem, which is why the nerve is identified and usually decompressed or transposed at the start rather than found late.
- Persistent pain - expect improvement, not abolition; this is the single most important expectation to set.
- Instability - either unmasked by the debridement or progressive afterwards, and the dominant predictor of a poor score.
- Pin-site infection and pin-track problems, including the rare pin-site stress fracture, and deep infection over the graft.
- Recurrent stiffness and heterotopic ossification, particularly in the multiply-operated post-traumatic elbow that is the usual candidate.
- Graft failure, resorption or progressive bone loss, with recurrence of symptoms.
- Triceps insufficiency where the extensor mechanism was taken down for exposure.
- Revision to TEA - a real and reasonably common endpoint, planned for from the outset rather than treated as a failure of judgement.
Mnemonics & Memory Aids
INTERPOSE
Hook:INTERPOSE: Interpose graft, Not a TEA candidate (young), Total elbow avoided, Early motion (distractor), Respect stability, Post-traumatic, Outcomes modest, Salvage to TEA.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 40-year-old manual worker has end-stage post-traumatic elbow arthritis. Why might you choose interposition arthroplasty over a total elbow replacement?”
“What is the role of the distraction external fixator, and what determines outcome?”
Why & who
- Joint/bone-preserving alternative to TEA
- Young, high-demand patient with end-stage (usually post-traumatic) elbow arthritis
- TEA avoided: strict lifelong lifting limit + high failure in the young
Technique
- Debride/contour distal humerus; interpose soft-tissue graft (fascia lata, Achilles/dermal allograft)
- Hinged distraction external fixator (~3-4 weeks) unloads/protects graft, allows early motion
- Modern: good stability -> immediate protected motion in a hinged brace without distractor
Key principle
- Stability is critical - instability (pre/post-op) predicts failure
- Restore/rely on competent collateral ligaments and columns
- Manage the ulnar nerve
Outcomes
- SALVAGE framing: improves the ARC reliably, pain only partially; larger series - Mayo 41 -> 65 (fair), arc 51 -> 97 degrees
- Graded results in the 45-elbow series: 13 good/excellent, 14 fair, 11 poor, 7 revised
- Pre-operative instability needing BOTH collaterals reconstructed argues AGAINST operating
- Failed interposition converts to TEA (bone preserved)
Evidence & Key Studies
Distraction interposition arthroplasty for the mobile, painful arthritic elbow (fascia lata)
- In 13 patients with mobile, painful arthritic elbows treated by distraction interposition arthroplasty using fascia lata (with an elbow distractor for 3-4 weeks), 69% had satisfactory pain relief and 62% an excellent/good Mayo Elbow Performance score at a mean 63 months.
- Instability of the elbow, both before and after surgery, was associated with unsatisfactory results; success was similar for inflammatory and post-traumatic arthritis (about 67%).
- Four of 13 required revision to total elbow arthroplasty (mean 30 months) with good results; it is a useful but less reliable option for young, high-demand patients.
Interposition arthroplasty with an Achilles tendon allograft as a salvage procedure for the elbow
- 45 elbows (34 post-traumatic, 11 inflammatory), mean age 39, mean 6-year follow-up: flexion-extension arc improved from 51 to 97 degrees and the Mayo Elbow Performance Score from 41 to 65 points.
- Results were sobering when graded: 13 good or excellent, 14 fair, 11 poor and 7 revised - the authors conclude interposition 'neither completely eliminates pain nor restores full function' and classify it as a salvage procedure.
- Pre-operative instability on examination (11 patients) was associated with low Mayo scores and high DASH scores DESPITE attempted collateral reconstruction, and 4 of the 5 patients who had BOTH collateral ligaments reconstructed had a NET DECREASE in Mayo score; the authors do not recommend the procedure in the presence of pre-operative instability.
Elbow interpositional arthroplasty using an Achilles tendon allograft (modern technique)
- Interpositional arthroplasty remains a viable option for post-traumatic elbow arthritis in young, high-demand patients, in whom total elbow arthroplasty is generally reserved for older patients.
- A high-demand patient with post-traumatic arthritis after multiple prior surgeries, treated with an Achilles tendon allograft interposition - allowed immediate protected range of motion in a hinged brace WITHOUT distraction external fixation because of good ligamentous stability - had significantly improved pain, motion and outcome scores.
- With good ligamentous stability, immediate protected motion can lead to excellent outcomes.
The distraction-interposition technique with fascia lata and a 3-4 week distractor, the modest outcomes (about 69% satisfactory pain relief, 62% excellent/good Mayo scores), the critical role of stability (instability predicting poor results), the similar results for post-traumatic and inflammatory arthritis, and conversion to TEA come from the cited Cheng & Morrey series; the larger 45-elbow experience - the improvement in arc from 51 to 97 degrees, the Mayo score rising only from 41 to 65, the graded results (13 good/excellent, 14 fair, 11 poor, 7 revised), the salvage framing, and the finding that pre-operative instability did badly despite collateral reconstruction with a net Mayo decrease in four of five bi-collateral reconstructions - from the cited Larson & Morrey series; the modern use of an Achilles tendon allograft with immediate protected motion in a hinged brace without external distraction when ligamentous stability is good, and the indication in young high-demand post-traumatic arthritis, from the cited Glazier case report. The bone-preserving rationale versus TEA (lifelong lifting limit, high young failure) is standard, well-established teaching. (See also our Total Elbow Arthroplasty and Post-Traumatic Elbow Stiffness topics.)