Elbow UCL Injury (Tommy John)
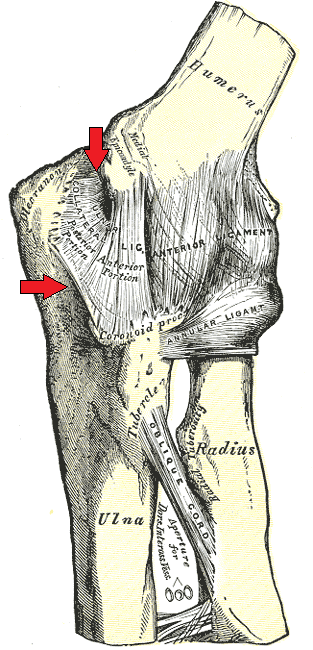
- The anterior bundle inserts on the SUBLIME TUBERCLE of the ulna (not "the coronoid" loosely) and originates on the medial epicondyle — get the precise footprints right, because they define the graft tunnels in reconstruction.
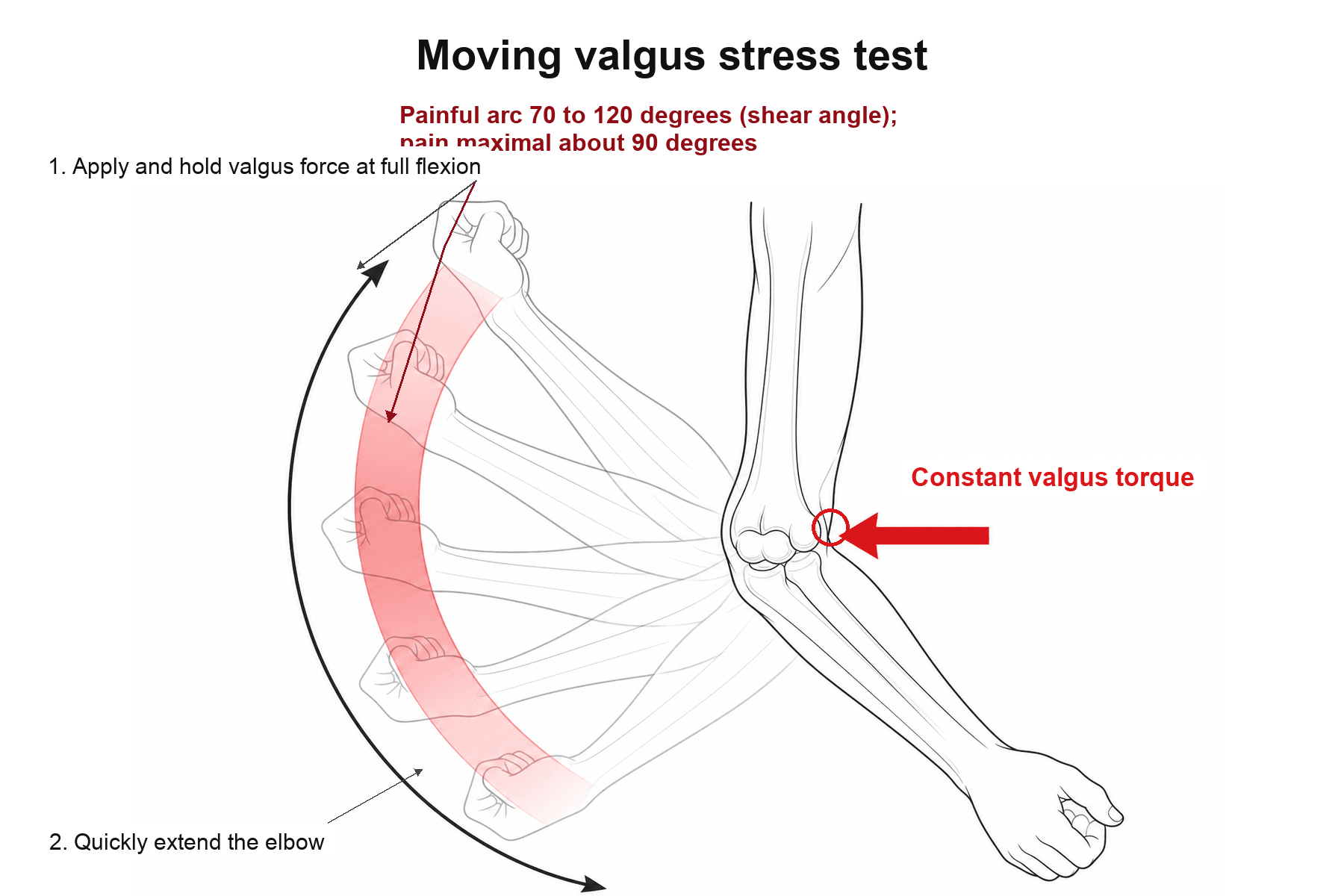
- The MOVING valgus stress test is the high-yield exam, not the static valgus test alone — a positive test reproduces the patient's pain through the 70–120° "shear angle" arc. Forgetting it is the commonest viva slip.
- Always examine the ULNAR NERVE. Ulnar neuritis coexists in a large minority and changes the operation (transposition); missing it is a classic completeness failure.
- Do not reconstruct every tear. A partial/low-grade tear gets a non-operative kinetic-chain trial first; reconstruction is for a complete tear or failed rehab in a thrower who wants to keep throwing.
- Tommy John is a RECONSTRUCTION (free tendon graft), not a repair. Direct repair ± internal brace is a distinct, narrower indication (acute avulsion, good tissue, younger athlete) — conflating the two loses marks.
- The "T sign" is a PARTIAL undersurface (deep) tear on MR arthrography — contrast tracking around the sublime tubercle — not a complete rupture.
Overview & Epidemiology
Ulnar collateral ligament (UCL) injury is the archetypal "thrower's elbow" — historically career-ending until Frank Jobe reconstructed the ligament in pitcher Tommy John in 1974, since when the eponym has become shorthand for the operation. It is overwhelmingly an overuse injury of the overhead athlete: baseball pitchers dominate every series, with javelin throwers, tennis servers, gymnasts and other overhead athletes contributing the remainder.
- Demographics: young, competitive overhead athletes — adolescents through professionals. Baseball pitchers are the prototype; pitch velocity and volume are the dominant risk factors.
- A rising incidence, most steeply in adolescents, attributed to early single-sport specialisation, year-round throwing, showcase culture and chasing velocity — which is why prevention (pitch counts, rest, mechanics) is now examinable, not just treatment.
- Risk factors: high pitch counts and innings, pitching while fatigued, year-round play, higher ball velocity, breaking pitches at a young age, and poor kinetic-chain mechanics that shift load onto the medial elbow.
- Why examiners care: it cleanly tests applied anatomy, a specific clinical test, MR interpretation, and a graded operative/non-operative decision in one athletic-population case.
Anatomy & mechanism
The medial (ulnar) collateral ligament complex has anterior, posterior and transverse bundles. The anterior bundle — from the medial epicondyle of the humerus to the sublime tubercle of the ulna — is the primary restraint to valgus and the clinically important structure. During the overhead throwing motion, especially the late-cocking and early-acceleration phases, the elbow experiences enormous valgus torque; the anterior bundle is loaded close to its tensile limit with every pitch. Repetitive valgus overload therefore causes attritional microtearing and, ultimately, failure — a chronic partial tear or an acute complete rupture.
Pathophysiology: valgus overload & the failure cascade
The throwing elbow is a biomechanical paradox: the valgus torque generated during late-cocking and acceleration is estimated to exceed the tensile strength of the native UCL on a single maximal throw. The ligament survives only because the surrounding dynamic stabilisers (the flexor-pronator mass) and the kinetic chain share the load. When that protection fails — through fatigue, volume or poor mechanics — the anterior bundle absorbs supraphysiological stress and begins to fail.
- Repetitive submaximal valgus load produces attritional microtearing of the anterior bundle faster than it can heal — a chronic degenerative process, not usually a single traumatic event.
- The deep (undersurface) fibres tear first, producing the partial undersurface tear that shows the "T sign" on MR arthrography, before progressing to full-thickness failure.
- Valgus instability shifts load — medial tension overload (UCL, flexor-pronator, ulnar nerve traction), lateral compression (radiocapitellar → capitellar OCD in the young), and posteromedial shear (valgus extension overload → posteromedial olecranon osteophytes). This triad explains the associated conditions.
- In the skeletally immature, the weak link is the medial epicondyle apophysis rather than the ligament — repetitive valgus traction causes "little league elbow" (medial epicondyle apophysitis/avulsion) instead of a mid-substance UCL tear.
Presentation & examination
- Medial elbow pain with throwing (often a 'pop' in acute rupture)
- Loss of velocity/control, pain in late-cocking/acceleration
- Overhead athlete (classically a baseball pitcher); also javelin
- Ulnar nerve symptoms (paraesthesia in ring/little fingers) are common
- Valgus stress test (at ~30° of flexion) — laxity/pain
- Moving valgus stress test — pain reproduced over the 70–120° arc (most useful)
- Milking manoeuvre — valgus stress with the elbow flexed
- Assess the ulnar nerve and the flexor-pronator origin
Investigations
- What it shows
- Partial undersurface tear = the 'T sign' (contrast tracking around the sublime tubercle); full-thickness gap in complete tears
- Role
- The imaging STANDARD; arthrography increases sensitivity for partial deep tears
- What it shows
- Medial joint gapping under valgus load; ligament thickening/calcification
- Role
- Operator-dependent but cheap, dynamic and ideal for serial assessment and the asymptomatic-laxity baseline
- What it shows
- Traction spurs, loose bodies, posteromedial olecranon osteophytes, avulsed fragment, OCD capitellum
- Role
- First-line bony survey; AP/lateral ± axial
- What it shows
- Quantify medial joint-space opening vs the contralateral side
- Role
- Adjunct to confirm functional valgus instability
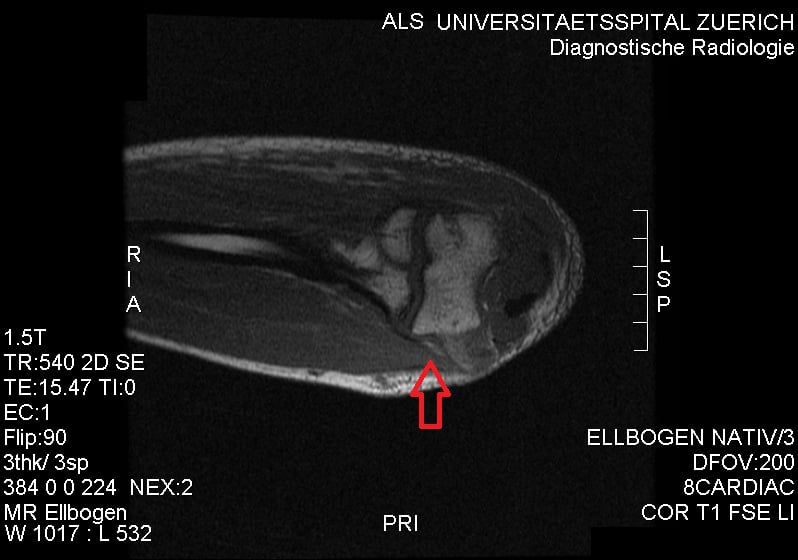
MRI, often with MR arthrography, is the imaging standard. A partial undersurface tear classically shows the 'T sign' — contrast tracking between the distal UCL and the sublime tubercle. Dynamic ultrasound demonstrates valgus laxity (medial gapping under stress) and is excellent for serial assessment, but interpret laxity against the contralateral elbow, since asymptomatic throwers develop adaptive UCL thickening and some baseline laxity. Plain radiographs may show traction spurs, loose bodies or an avulsed fragment, and stress views can quantify medial opening.
Management
- 1Grade the tear and the demandPartial/low-grade tear, lower-demand or in-season athlete → non-operative trial. Complete tear, or partial that fails rehab, in a competitive overhead athlete who wants to keep throwing → reconstruction.
- 2Non-operative trial first for partial tearsRest from throwing, then a structured kinetic-chain rehabilitation programme (scapular/core stability, flexor-pronator strengthening), graded return-to-throwing, mechanics correction, ± PRP. Many partial tears return to throwing.
- 3Reconstruction (Tommy John) for complete/failedFree tendon graft (palmaris longus or gracilis) through humeral and ulnar tunnels recreating the anterior bundle (docking / figure-of-eight techniques); protect or transpose the ulnar nerve. Return to throwing takes ~9–12 months.
- 4Repair ± internal brace for select avulsionsAn acute proximal/distal avulsion with good tissue, typically in a younger athlete, may be repaired (± suture-tape internal brace) for a faster return than reconstruction. Patient selection is key.
A trial of non-operative care suits partial/low-grade tears and many in-season athletes: a period of rest from throwing, then a structured rehabilitation programme addressing the entire upper-extremity kinetic chain (scapular and core stability, flexor-pronator strengthening), a gradual return-to-throwing progression, and attention to throwing mechanics. Orthobiologics (PRP) are used as an adjunct for partial tears, with reasonable return-to-throwing in selected cases.
Reconstruction restores valgus stability with return to play around 80–90%; a systematic review of adolescent throwers found ~84% returned to the same level or higher, with low complication (~3.9%) and reoperation (~1.8%) rates (though reported return-to-play across the literature ranges widely, 33–92%). Given a markedly rising incidence (especially in adolescents), prevention is emphasised: pitch-count limits, adequate rest, avoiding year-round single-sport throwing, and mechanics optimisation.
The original Jobe technique (1986) passed a figure-of-eight graft through humeral and ulnar tunnels, detached the flexor-pronator origin and routinely submuscularly transposed the ulnar nerve - effective but with a high rate of ulnar-nerve complications. Two refinements followed: the muscle-splitting (modified Jobe) approach, which avoids detaching the flexor-pronator mass; and the docking technique (Altchek), which uses a single humeral tunnel into which the graft is docked and tied over a bony bridge, with the limbs brought out through two small ulnar exit holes - simplifying graft tensioning and lowering complications. The ulnar nerve is now handled selectively (transposed only if symptomatic or subluxing) rather than routinely, and hybrid interference-screw constructs also exist. Whatever the technique, the graft recreates the anterior bundle from the medial-epicondyle footprint to the sublime tubercle.
The workhorse graft is the ipsilateral palmaris longus tendon, but it is congenitally absent in roughly 10-15% of people, so you must test for it pre-operatively: ask the patient to oppose the thumb to the little finger and flex the wrist - the tendon stands out at the volar wrist (absent if no tendon appears). If it is absent or too small, alternatives include the gracilis (or semitendinosus) hamstring tendon, the contralateral palmaris, plantaris, or a toe-extensor tendon. Confirming graft availability is a basic pre-operative planning step examiners expect you to mention.
Associated conditions
- Relationship
- Valgus instability + traction; common — examine and address the nerve
- Relationship
- Posteromedial olecranon osteophytes and chondral wear from valgus + extension
- Relationship
- The dynamic medial stabilisers fatigue/fail alongside the UCL
- Relationship
- Repetitive extension/valgus stress in throwers
- Relationship
- The lateral compression counterpart in the young thrower
Complications
Complications arise both from the untreated injury and from reconstruction — examiners may ask either, so separate them clearly.
- Complication
- Chronic valgus instability + inability to throw
- Note / management
- The functional end-point that drives surgery in a committed thrower
- Complication
- Ulnar neuritis / cubital tunnel symptoms
- Note / management
- Traction + instability; assess and address (decompress/transpose)
- Complication
- Valgus extension overload, loose bodies, capitellar OCD
- Note / management
- Secondary posteromedial impingement and lateral compression sequelae
- Complication
- Ulnar nerve symptoms
- Note / management
- The MOST common complication; mitigated by careful handling/transposition when indicated
- Complication
- Medial antebrachial cutaneous (MABC) nerve injury
- Note / management
- From the medial approach; causes a numb patch and painful neuroma if cut
- Complication
- Graft failure / persistent instability, stiffness, tunnel fracture, infection
- Note / management
- Re-tear in ~1-2% needing revision; meticulous tunnel placement avoids posteromedial blowout
- Complication
- Failure to return to prior performance
- Note / management
- RTP is high (~80-90%) but velocity/level is not guaranteed; counsel realistically
The ulnar nerve is the structure most often harmed in UCL surgery. Identify and protect it at every step, transpose it when it is symptomatic or subluxing, and warn the athlete pre-operatively about transient ulnar paraesthesiae and the small numb forearm patch from medial antebrachial cutaneous nerve branches.
Mnemonics & Memory Aids
- Anterior bundle (medial epicondyle → sublime tubercle) = primary valgus restraint and the structure injured.
- Mechanism: repetitive valgus overload (late-cocking/early-acceleration), classically baseball pitchers.
- Moving valgus stress test (pain through the 70–120° arc) is the most useful test — and assess the ulnar nerve.
- MR arthrogram 'T sign' = partial undersurface tear; dynamic US shows valgus laxity.
- Partial → non-op (kinetic-chain rehab ± PRP); complete/failed → reconstruction (palmaris/gracilis graft); repair ± internal brace for select acute avulsions.
- RTP ~80–90%; rehab ~9–12 months; prevention via pitch counts and mechanics.
VALGUSThe injury
Hook:VALGUS overload kills the Anterior bundle - test with moving Valgus stress, check the Ulnar nerve, Scan with MRI.
TOMMYThe management
Hook:TOMMY John: tear-based decision, graft reconstruction, moving valgus test, mind the ulnar nerve, ~1-year rehab.
PITCHPrevention pearls
Hook:PITCH safely: counts, no fatigue, time off, delay breaking balls, good mechanics - prevention is now examinable given the rising adolescent incidence.
Viva practice
Viva practice
Practise clinical reasoning and management decisions out loud
“A 17-year-old baseball pitcher has medial elbow pain and reduced throwing velocity. What is the relevant anatomy, how do you examine him, and how do you confirm a UCL injury?”
“How would you manage this pitcher's UCL injury, and what determines whether you reconstruct or repair? What outcomes and prevention would you discuss?”
Exam cheat sheet
Anatomy & mechanism
- Anterior bundle (medial epicondyle → sublime tubercle) = primary valgus restraint
- Repetitive valgus overload in throwing (late cocking/early acceleration)
- Baseball pitchers; acute rupture or chronic attritional failure
Diagnosis
- Medial elbow pain + reduced velocity; check ULNAR NERVE
- Valgus stress, MOVING valgus stress (pain 70-120 deg), milking manoeuvre
- MRI/MR arthrogram standard ('T sign' = partial undersurface tear); dynamic US for laxity
Management
- Partial/low-grade → non-op (rest, kinetic-chain rehab, mechanics, +/- PRP)
- Complete/failed in competitive thrower → reconstruction (Tommy John; palmaris/gracilis)
- Repair +/- internal brace for select acute avulsions (younger athletes)
Outcomes & associations
- RTP ~80-90% after reconstruction (adolescents ~84% same level or higher)
- Associations: ulnar neuritis, valgus extension overload, flexor-pronator injury, OCD capitellum
- Prevention: pitch counts, rest, mechanics (rising incidence)
Evidence Base
Elbow ulnar collateral ligament injuries in athletes: Can we improve our outcomes?
- UCL injury most commonly occurs in the overhead throwing athlete from valgus-overload pathomechanics.
- Conservative treatment is appropriate for partial injuries; improved operative reconstruction techniques and adjuncts are used for complete tears.
- Structured, sport-specific rehabilitation of the entire upper-extremity kinetic chain is central to returning to throwing.
The 'moving valgus stress test' for medial collateral ligament tears of the elbow
- Describes the moving valgus stress test: a constant moderate valgus torque is applied to the fully flexed elbow which is then quickly extended; positive if medial elbow pain is reproduced and maximal between 120 and 70 degrees (the 'shear angle').
- Against surgical/arthroscopic confirmation it was highly SENSITIVE (100%, 17/17) and SPECIFIC (75%, 3/4) for medial collateral ligament insufficiency.
- Mean painful arc 120 to 70 degrees; pain maximal at about 90 degrees of flexion.
Outcome of ulnar collateral ligament reconstruction of the elbow in 1281 athletes
- Largest series: 1281 athletes (1266 reconstruction, 15 repair) over 1988-2006 using a modification of the Jobe technique with subcutaneous ulnar nerve transposition.
- Of 743 followed at minimum 2 years, 617 (83%) returned to the previous level of competition or higher; mean time to throwing 4.4 months and to full competition 11.6 months.
- Complications occurred in 20% (16% minor, 4% major), with ulnar nerve symptoms the most frequent.
Ulnar Collateral Ligament Reconstruction in Adolescents: A Systematic Review
- Across 9 studies (414 adolescent throwers: 404 baseball, 10 javelin), 349/414 (84.3%) returned to the same level of competition or higher after UCL reconstruction.
- Complications were reported in 3.9% and reoperations in 1.8% of patients.
- Return-to-play rates across the literature range widely (33-92%); long-term outcome data in adolescents are still needed.
The valgus-overload mechanism and graded partial-vs-complete management come from Redler et al. (DOI); the moving valgus stress test and its sensitivity/specificity from O'Driscoll et al. (DOI); the benchmark reconstruction outcomes (83% RTP, ulnar nerve the leading complication) from Cain et al. (DOI); and the adolescent return-to-play figures from Hadley et al. (DOI). The anterior-bundle anatomy and the MRI 'T sign' are standard, well-established teaching. (See also our GIRD and Tennis Elbow material.)