Glenohumeral Internal Rotation Deficit (GIRD)
An internal-rotation deficit alone can mislead - the thrown shoulder trades IR for ER. Compare TOTAL rotational motion (IR + ER): if the IR loss is matched by an ER gain (total motion symmetrical), the GIRD is usually physiologic and benign. Pathologic GIRD loses total motion.
Measure IR/ER supine at 90° abduction with the scapula stabilised. Failing to stabilise it lets scapulothoracic motion falsely inflate internal rotation and miss the deficit - a classic examination error.
Overview & Epidemiology
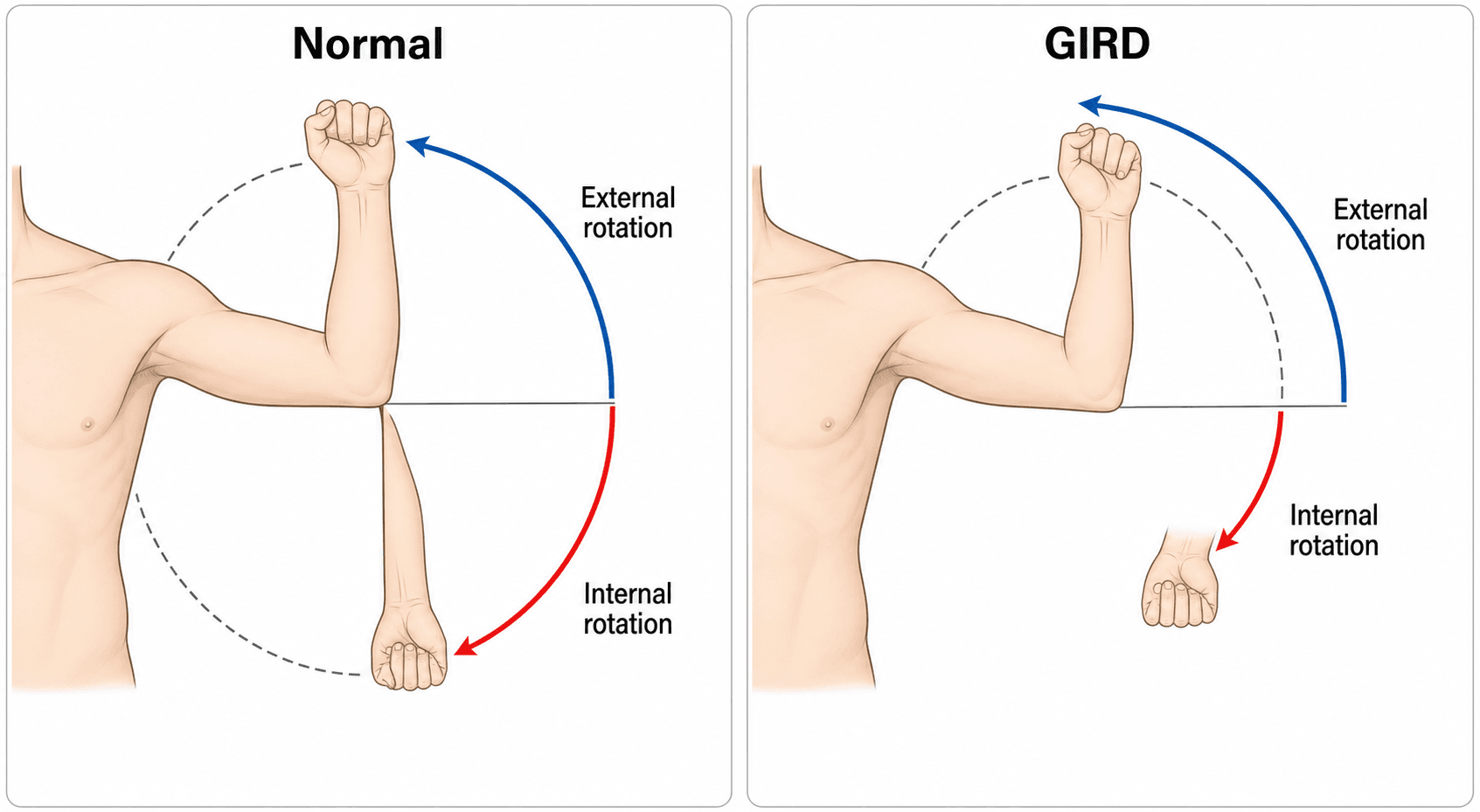
The repetitive overhead throwing motion — especially the late-cocking phase of maximal external rotation and abduction — places enormous torsional and tensile load on the shoulder. Over time the dominant shoulder adapts: it gains external rotation and loses internal rotation. GIRD names this loss of internal rotation, conventionally a deficit of more than 20° compared with the non-throwing shoulder. Two mechanisms contribute: a bony adaptation (increased humeral retroversion, which shifts the rotational arc and is generally physiologic), and a soft-tissue adaptation (posterior capsular and rotator-cuff tightness/contracture, which is the pathologic driver).
IR loss from bony humeral retroversion, matched by an external-rotation gain, so total rotational motion is symmetrical with the other side. Typically asymptomatic — an expected throwing adaptation that does not necessarily need treatment.
IR loss from posterior capsule/rotator-cuff tightness with a loss of total rotational motion (and/or a large IR deficit). Symptomatic and linked to internal impingement, peel-back, SLAP/labral and articular-sided cuff lesions — this is what you rehabilitate.

Because the throwing shoulder trades internal for external rotation, the absolute IR loss alone can mislead. What matters is the total rotational motion (TRM) = internal + external rotation. If the IR deficit is balanced by an equal ER gain so that TRM is symmetrical with the other side, the GIRD is usually physiologic and benign. Pathologic GIRD is defined by a loss of total rotational motion (the IR loss is not compensated) — the picture associated with injury. Always measure and compare both rotations, scapula stabilised, at 90° of abduction.
The definition worth carrying is an IR deficit of more than 20° versus the contralateral shoulder — but the diagnosis of the pathologic form turns on a loss of total ROMIR + ER, not the IR number in isolation.
Pathophysiology: The Thrower's Shoulder
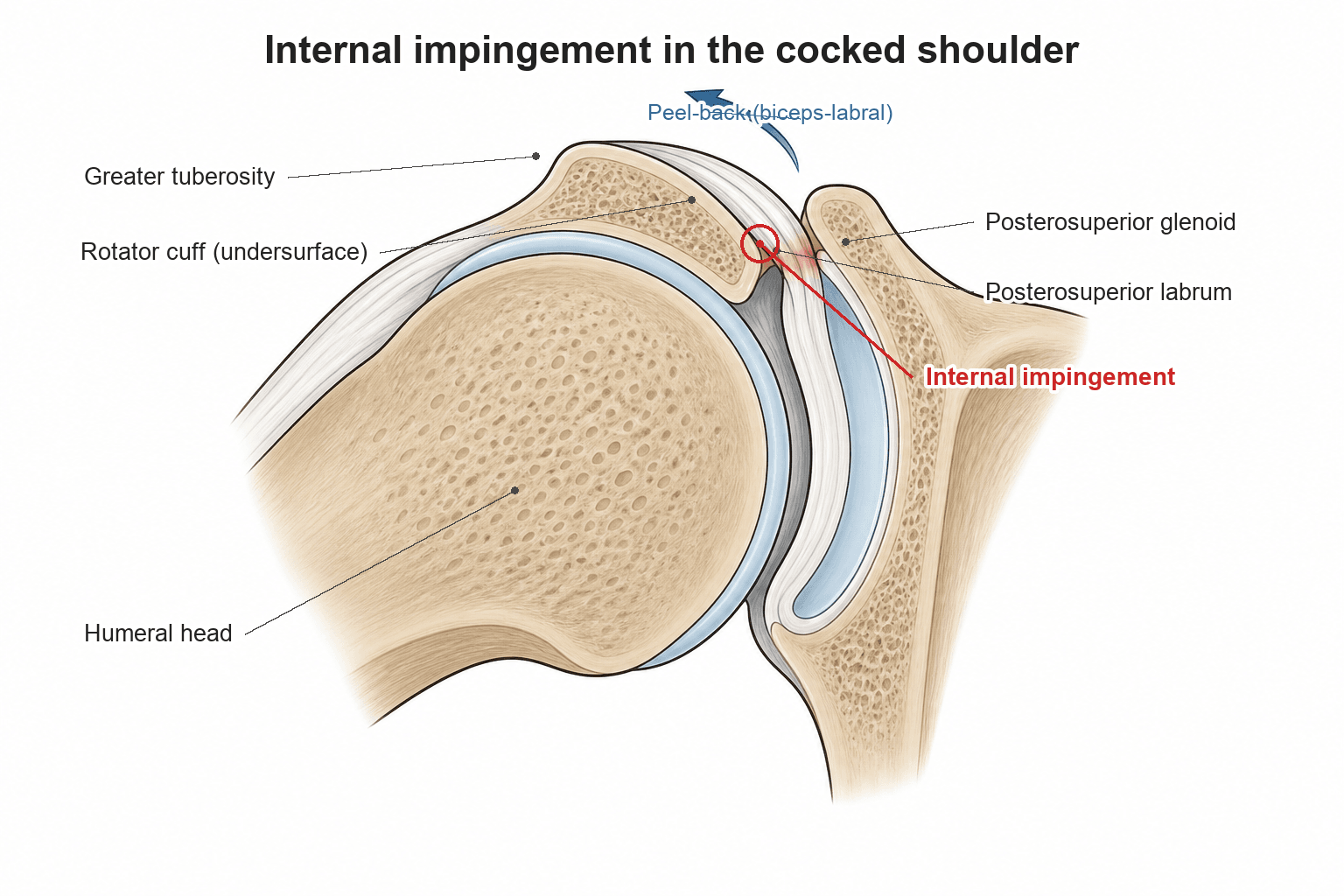
Two linked mechanisms explain why pathologic GIRD damages the shoulder. In the cocked position of abduction and maximal external rotation, the rotator cuff and posterosuperior labrum are pinched between the greater tuberosity and the posterosuperior glenoid — internal (posterosuperior) impingement. A tight posterior-inferior capsule also shifts the humeral head's rotational point postero-superiorly, increasing the torsional peel-back force on the biceps–superior labrum complex (Burkhart and Morgan's mechanism) — driving SLAP and posterosuperior labral tears and articular-sided cuff tears.
GIRD rarely acts alone. Kibler and Burkhart's "disabled throwing shoulder" describes how posterior capsular tightness, scapular dyskinesis and GIRD compound to cause injury. Look for the SICK scapula — Scapular malposition, Inferior medial border prominence, Coracoid pain, and dysKinesis of scapular movement — because correcting scapular mechanics is part of curing GIRD, not an afterthought.
Clinical Presentation & Examination
The typical patient is an overhead/throwing athlete (baseball pitcher, tennis, volleyball, handball) with posterior shoulder tightness, a dead-arm feeling or pain in the late-cocking phase, and loss of internal rotation on the dominant side. Symptoms range from a vague performance drop to frank internal-impingement or labral pain.
- Measure IR and ER at 90° of abduction, supine, with the scapula stabilised (a hand over the coracoid/anterior shoulder prevents scapulothoracic compensation falsely raising IR)
- Calculate the IR deficit and the total rotational motion, comparing both sides
- Assess for posterior capsular tightness, scapular dyskinesis (SICK scapula), and signs of internal impingement / labral pathology
A treatable mimic to keep in mind: isolated infraspinatus wasting with external-rotation weakness in an overhead athlete points to suprascapular nerve compromise at the spinoglenoid notch - classically a paralabral (ganglion) cyst arising from a posterosuperior / SLAP labral tear, or repetitive nerve traction (volleyball players and throwers). Because the branch to infraspinatus is affected selectively at the spinoglenoid notch, the supraspinatus is spared (contrast a suprascapular-notch lesion, which affects both). Confirm with MRI (the cyst, infraspinatus oedema/atrophy) and nerve conduction studies/EMG, and treat by addressing the underlying labral tear and decompressing the cyst (often arthroscopically). This is a distinct, fixable cause of the weak/painful thrower's shoulder - not part of GIRD's capsular mechanism.
Investigations & Imaging
- GIRD itself is a clinical/ROM diagnosis — no imaging confirms it
- MRI/MR arthrography if an associated lesion is suspected — posterosuperior labral/SLAP tears, partial articular-sided cuff tears, internal impingement changes (cyst/oedema at the posterosuperior humeral head/glenoid)
- Measuring humeral retroversion (e.g. on ultrasound/CT) can help explain a large IR deficit with preserved total motion as a physiologic, bony adaptation
Management
- 1Confirm it is pathologicMeasure both rotations with the scapula stabilised; pathologic GIRD = IR loss WITH lost total rotational motion and symptoms. Asymptomatic physiologic GIRD with preserved total motion needs no treatment.
- 2Stretch the posterior capsule (first line)Sleeper stretch and cross-body adduction stretch to restore internal rotation. The mainstay — most throwers regain IR and total motion with a dedicated programme.
- 3Restore scapular and cuff mechanicsScapular stabiliser and rotator-cuff strengthening, address the SICK scapula/dyskinesis, and correct throwing mechanics. GIRD is part of the disabled throwing shoulder, not an isolated tight capsule.
- 4Operate only for failure or a structural lesionArthroscopy for a symptomatic SLAP/articular-sided cuff lesion after failed rehab; arthroscopic posterior capsular release is RARELY needed. In a high-level thrower, aim to restore baseline with the minimum intervention.
The cheapest treatment is prevention. Many programmes pre-season screen overhead athletes' bilateral IR/ER and total rotational motion, flagging those who have lost total motion for a targeted posterior-capsule and scapular programme before symptoms appear, and prescribe off-season and post-throwing stretching to limit the adaptive contracture. Return to throwing is graded and criteria-based - restoring internal rotation and total motion, a pain-free examination and a normalised scapular rhythm - rather than purely time-based, with a structured interval throwing programme to rebuild load. Treating GIRD is therefore as much about monitoring and load management across a season as it is about the stretch itself.
The mainstay: posterior capsular stretching — the sleeper stretch and cross-body adduction stretch — to restore internal rotation, plus scapular stabiliser and rotator-cuff strengthening and correction of throwing mechanics. Most athletes improve, regaining IR and total motion; a structured programme also addresses scapular dyskinesis. Prevention/screening and off-season stretching are part of care.
A systematic review and meta-analysis (2195 athletes, 17 studies) found that, although results trended toward more upper-extremity injuries in overhead athletes with GIRD (mean difference 3.11°, P = 0.06), with loss of total motion and external-rotation gain, the associations did not reach statistical significance. So GIRD is best seen as one risk factor within the thrower's-shoulder picture — particularly when it reflects lost total rotational motion — rather than a guaranteed cause of injury.
Complications & Associated Pathology
Pathologic GIRD does not occur in isolation - it sits at the centre of the thrower's-shoulder spectrum, and the "complications" examiners want are the structural lesions it is linked to (and, untreated, the career-limiting dead arm).
- Relationship to GIRD
- Cuff/labrum pinched between greater tuberosity and posterosuperior glenoid in abduction–external rotation
- Relationship to GIRD
- From repetitive contact/peel-back in the cocking position
- Relationship to GIRD
- Superior labrum anterior-to-posterior; the peel-back mechanism (Burkhart–Morgan)
- Relationship to GIRD
- Undersurface (articular) supraspinatus/infraspinatus tears
- Relationship to GIRD
- The functional endpoint - loss of velocity/control and pain that ends throwing if untreated
A classic examinable extra-articular lesion: the Bennett lesion is a posteroinferior glenoid ossification / exostosis seen in throwing athletes, attributed to chronic traction of the posterior band of the inferior glenohumeral ligament and posterior capsule (Bennett originally implicated the triceps). It is associated with posterior labral and undersurface rotator-cuff pathology and with the same posterior-capsular tightness/GIRD picture. It is seen as a crescentic posteroinferior glenoid mineralisation on an axillary or Stryker-notch radiograph or on CT. Most are asymptomatic and managed non-operatively as for GIRD; arthroscopic excision is reserved for a genuinely symptomatic lesion - so the Bennett lesion is often best read as a radiographic marker of the chronic throwing adaptation rather than a lesion that itself demands surgery.
Mnemonics & Memory Aids
GIRDGIRD core
Hook:GIRD: internal rotation gone — check total motion, blame the posterior capsule, stretch it out.
THROWManaging the thrower
Hook:The THROWer's GIRD: total motion, retroversion, rehab, operate rarely, watch mechanics.
SICKThe SICK scapula
Hook:A SICK scapula travels with GIRD: malposition, Inferior border prominence, Coracoid pain, dysKinesis.
Exam & revision
Everything below condenses GIRD for revision and viva practice — the high-yield points, memory hooks, worked vivas, and a one-screen cheat sheet.
- GIRD = more than 20° IR loss vs the other side, measured at 90° abduction, scapula stabilised.
- Compare TOTAL rotational motion (IR + ER) — preserved total motion (ER gain matches IR loss) is usually physiologic; lost total motion is the red flag.
- Physiologic = bony humeral retroversion; pathologic = posterior capsule/cuff tightness.
- Mechanism: internal impingement + peel-back (Burkhart–Morgan) → SLAP, posterosuperior labral and articular-sided cuff tears.
- First-line treatment = posterior capsular stretch (sleeper/cross-body) + scapular/cuff strengthening + mechanics; surgery rarely.
- Stabilise the scapula when measuring, or you falsely overestimate IR.
Viva practice
Practise clinical reasoning and management decisions out loud
“A 19-year-old baseball pitcher has posterior shoulder tightness and reduced internal rotation on the throwing side. What is GIRD, how do you decide whether it is physiologic or pathologic, and how do you examine for it?”
“What conditions is GIRD associated with, and how would you manage a symptomatic thrower with pathologic GIRD?”
Definition
- Loss of glenohumeral internal rotation in the throwing shoulder (over 20° vs contralateral)
- Measured at 90° abduction, supine, scapula stabilised
- Compare TOTAL rotational motion (IR + ER), not just absolute IR
Physiologic vs pathologic
- Physiologic: bony humeral retroversion, ER gain, total motion preserved, asymptomatic
- Pathologic: posterior capsule/cuff tightness, LOSS of total motion, injury-associated
- Total-motion loss is the red flag
Mechanism & associations
- Internal (posterosuperior) impingement; peel-back (Burkhart–Morgan)
- Posterosuperior labral & SLAP tears; partial articular-sided cuff tears
- Disabled throwing shoulder + SICK scapula compound the problem
Management
- First line: posterior capsular stretch (sleeper/cross-body) + scapular/cuff strengthening + mechanics
- Arthroscopy only if rehab fails / symptomatic lesion; capsular release rarely
- Evidence: GIRD a contributory risk factor (esp. with lost total motion), not a definitive cause
Evidence
The disabled throwing shoulder: spectrum of pathology Part I: pathoanatomy and biomechanics
- The landmark unified concept of the disabled throwing shoulder, rejecting microinstability in favour of posterior-inferior capsular contracture and GIRD as the primary drivers.
- Describes the peel-back mechanism by which a tight posterior capsule shifts the humeral rotational point posterosuperiorly, increasing torsional load on the biceps-labral complex.
- Links the cascade to internal impingement, SLAP/posterosuperior labral tears and articular-sided cuff tears - the pathoanatomic basis of the topic.
Glenohumeral internal rotation deficit in throwing athletes: current perspectives
- GIRD is commonly defined as a loss of more than 20 degrees of internal rotation versus the contralateral shoulder; total rotational motion may matter more than the absolute IR loss.
- Pathologic GIRD = loss of IR combined with loss of total rotational motion, driven by posterior capsular and rotator-cuff tightness from repetitive cocking.
- Associated with posterosuperior labral tears, partial articular-sided cuff tears and SLAP tears; mainstay treatment is posterior capsular stretching and scapular strengthening, with arthroscopy if non-operative care fails.
Glenohumeral Internal Rotation Deficit and Risk of Upper Extremity Injury in Overhead Athletes: A Meta-Analysis and Systematic Review
- Pooled 2195 overhead athletes (17 studies); shoulders with GIRD trended toward upper-extremity injury (mean difference 3.11°, P = 0.06) but did not reach statistical significance.
- Loss of total rotational motion and external-rotation gain also favoured injury without reaching significance.
- Supports viewing GIRD as one contributory risk factor (especially when total motion is lost) rather than a definitive cause of injury.
The effects of sleeper stretch vs. crossbody stretch in overhead athletes with shoulder pain and glenohumeral internal rotation deficit: a randomized controlled trial
- Double-blind RCT in 35 symptomatic overhead athletes with GIRD: both the sleeper stretch and the cross-body stretch (3x/week for 4 weeks) significantly reduced pain and improved internal rotation.
- GIRD was attenuated by about 14.7 degrees in both groups, with no significant difference between the two techniques.
- Both were well tolerated and safe, supporting either posterior-capsule stretch in conservative management.
The peel-back/pathoanatomy comes from the Burkhart-Morgan-Kibler disabled-throwing-shoulder paper (Arthroscopy, DOI), the definition and total-rotational-motion framework from the Rose & Noonan review (DOI), the (non-significant) injury-association data from the Keller meta-analysis (DOI), and the Level-1 stretching evidence from the de Araújo RCT (DOI). The disabled-throwing-shoulder and SICK-scapula concepts are well-established sports-shoulder teaching. (See also our SLAP Tears topic.)