Motion-Preserving Wrist Arthrodesis | SLAC/SNAC Wrist | Capitate-Lunate-Hamate-Triquetrum Fusion | Radiolunate Joint Preserved | Dorsal Approach | Fixation Options
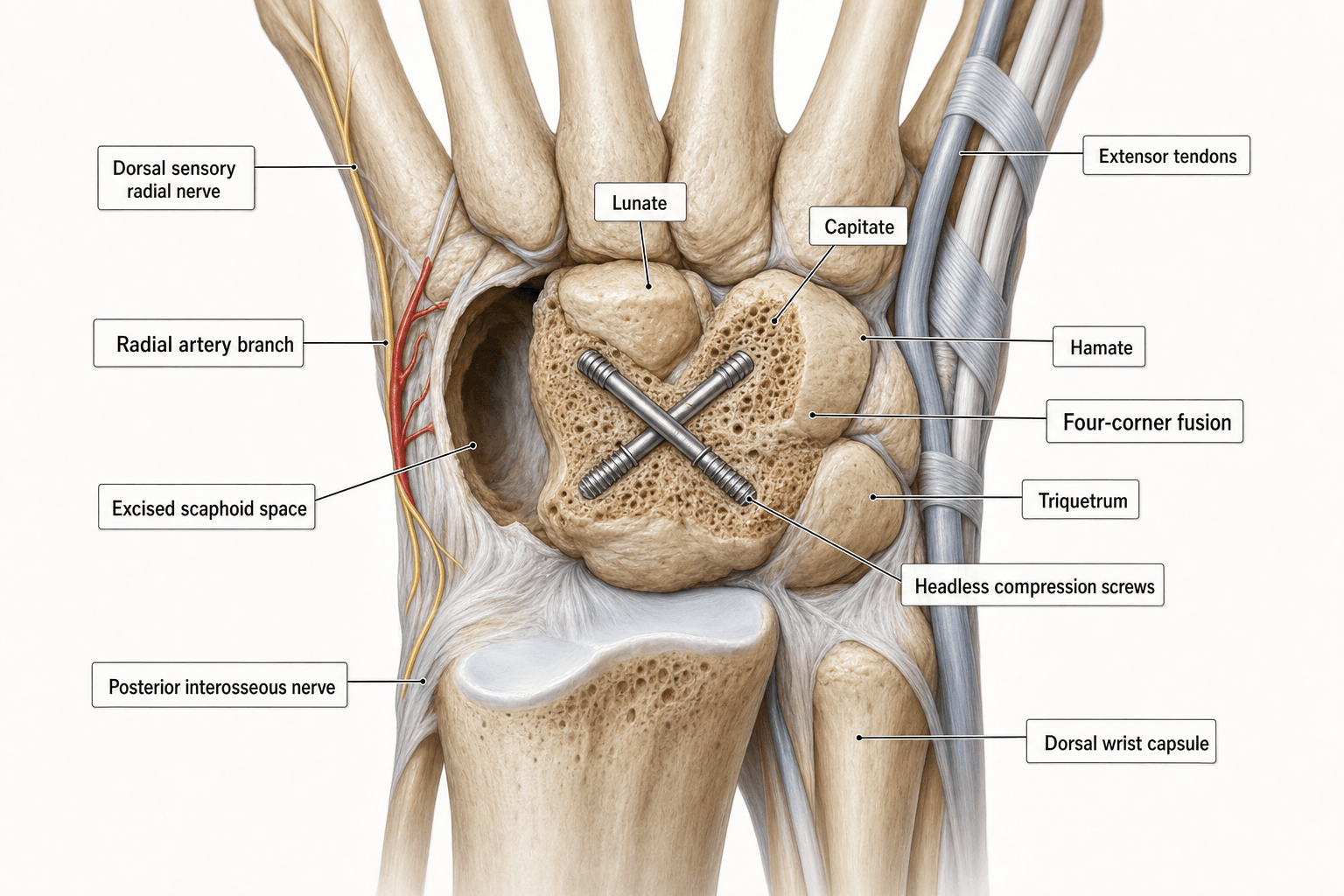
- Four-corner fusion (4CF) treats SLAC and SNAC wrist arthritis by excising the scaphoid and fusing the capitate, lunate, hamate, and triquetrum, preserving radiolunate and midcarpal motion
- The radiolunate joint must be preserved - if it is arthritic (stage III SLAC), four-corner fusion is contraindicated and total wrist arthrodesis or PRC should be considered
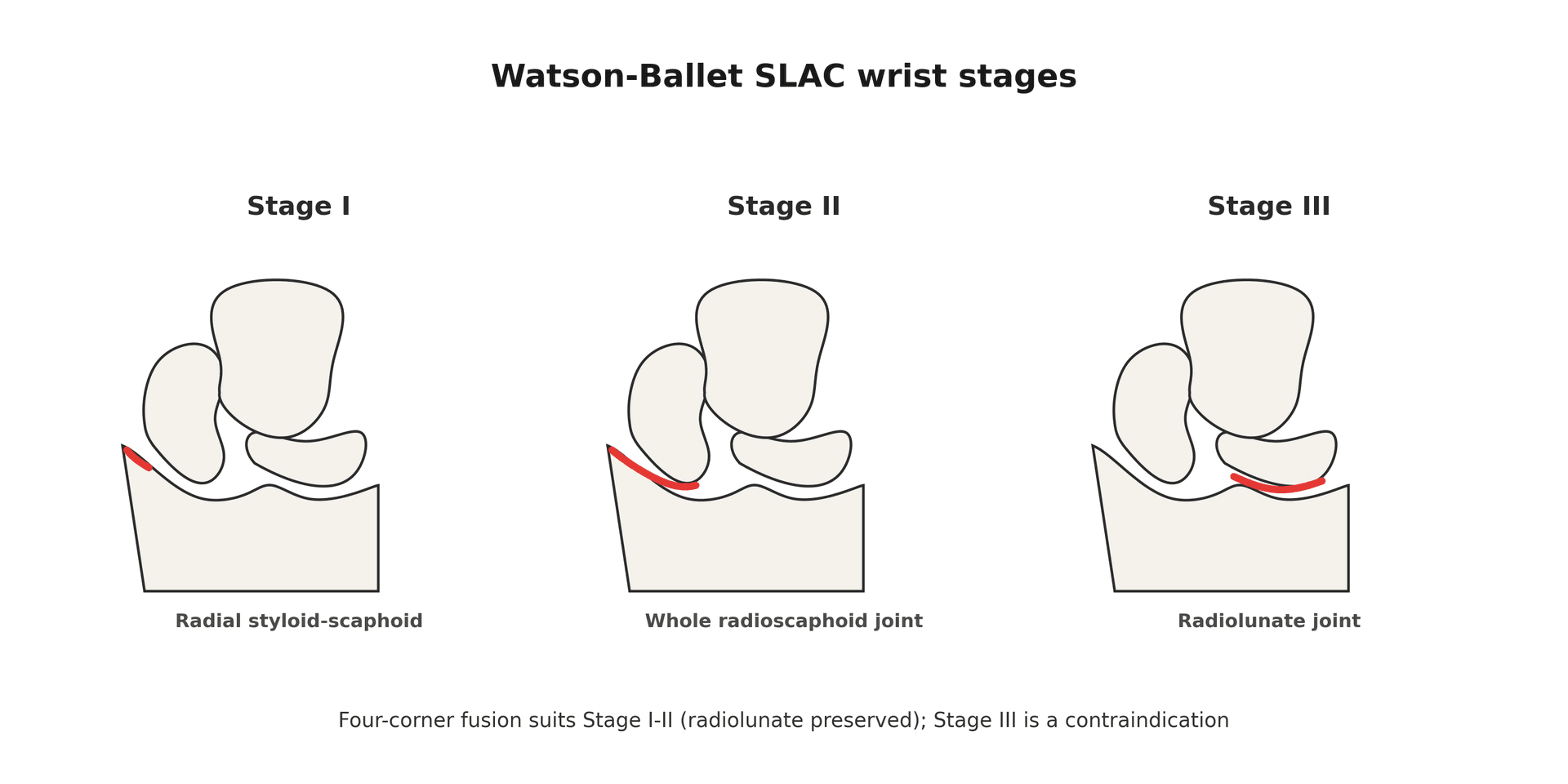
- SLAC wrist is the most common pattern of post-traumatic wrist arthritis, accounting for approximately 55-60% of cases, and follows a predictable pattern of joint degeneration described by Watson and Ballet
- Nonunion is the most significant complication - rates vary from 3-30% depending on fixation method, with circular plates historically associated with higher nonunion rates than K-wires
- Compared with proximal row carpectomy (PRC), four-corner fusion retains the native lunocapitate articulation and may provide better grip strength, but at the cost of a more complex procedure and higher complication rate
- “Always begin with the Watson and Ballet SLAC classification - examiners want to see you understand which stages are suitable for 4CF (stages I and II) versus which are not (stage III with radiolunate involvement)
- “The key decision point is the status of the radiolunate joint - if the lunate fossa of the radius and the proximal lunate are both preserved, 4CF is an option; if not, choose PRC (if capitate head is intact) or total wrist arthrodesis
- “Dorsal impingement is a common cause of persistent pain after 4CF - caused by the fused carpal mass impinging on the dorsal rim of the radius in extension; adequate scaphoid excision and dorsal lunate rim trimming reduce this risk
- “The radial styloid must be resected (styloidectomy) to prevent impingement on the fused carpus during radial deviation
Scaphoid Excision and Four-Corner Fusion
Four-corner fusion is contraindicated if the radiolunate joint is arthritic. In SLAC stage III, the arthritis has progressed to involve the radiolunate articulation, and fusing the four corners will not eliminate the pain source. Examiners want you to identify the stage first and then select the appropriate procedure. A patient with radiolunate arthritis needs PRC (if the capitate head cartilage is intact) or total wrist arthrodesis - not four-corner fusion.
- Best option
- Scaphoid excision and four-corner fusion
- Reasoning
- Preserves radiolunate motion; retains native lunocapitate joint for better load transfer; grip strength advantage over PRC in some studies
- Best option
- Proximal row carpectomy (PRC)
- Reasoning
- Removes the arthritic proximal row entirely; capitate articulates with lunate fossa of radius; simpler procedure, faster recovery, lower complication rate
- Best option
- Total wrist arthrodesis
- Reasoning
- Eliminates all wrist motion but provides reliable pain relief and stability; gold standard for end-stage arthritis; most reliable for heavy labourers
- Best option
- Scaphoid excision and four-corner fusion
- Reasoning
- In SNAC, the radioscaphoid joint may be preserved (unlike SLAC); the midcarpal joint around the scaphoid is destroyed; 4CF addresses the pathology while preserving radio carpal joints
Overview and Indications
Scaphoid excision and four-corner fusion (4CF) is a motion-preserving limited wrist arthrodesis performed for advanced carpal collapse secondary to scapholunate ligament insufficiency (SLAC wrist) or scaphoid nonunion (SNAC wrist). The procedure involves excising the scaphoid and fusing the capitate, lunate, hamate, and triquetrum into a single bony mass that articulates with the radius at the preserved radiolunate joint.
The concept was developed from the observation by Watson and Ballet (1984) that wrist arthritis follows predictable patterns. In SLAC wrist, the radiolunate joint is preserved until very late, meaning the lunate fossa of the radius and the proximal pole of the lunate remain healthy even as the scaphoid and its surrounding articulations degenerate. By excising the arthritic scaphoid and stabilising the remaining carpus, pain is relieved while a functional arc of motion is maintained.
the scaphoid is the mechanical keystone linking the proximal and distal carpal rows. When the scapholunate ligament fails or the scaphoid does not unite, the scaphoid flexes and collapses into a vertical position, the lunate extends into dorsiflexed intercalated segment instability (DISI), and the carpus collapses in a predictable proximal migration pattern. Removing the scaphoid eliminates the pain source; fusing the four corners stabilises the remaining carpus.
- SLAC wrist stages I and II with preserved radiolunate joint and intact lunocapitate cartilage
- SNAC wrist with arthritis confined to the scaphoid articulations and preserved radiolunate joint
- Chronic scapholunate instability with secondary degenerative changes, unsuitable for ligament reconstruction
- Scaphoid nonunion with secondary arthritis and a viable proximal pole that is unsalvageable
- Patient who desires motion preservation and understands the expected functional outcomes
- Patient willing to comply with prolonged immobilisation and rehabilitation (6-12 weeks protected mobilisation)
- Kienbock disease (late stage) with carpal collapse where radiolunate preservation is possible
- Preiser disease (avascular necrosis of the scaphoid) with secondary arthritis
Examiners test your ability to identify when 4CF is wrong. Key contraindications: radiolunate arthritis (SLAC stage III), inflammatory arthritis (RA, psoriatic), capitate head cartilage loss (reduces the point of 4CF vs PRC), active infection, severe osteoporosis (poor fixation), unwillingness to comply with immobilisation, and pre-existing CRPS. If the radiolunate joint is arthritic, the procedure will not relieve pain regardless of how well the fusion heals.
SNAC (scaphoid nonunion advanced collapse) has its own three-stage pattern analogous to SLAC but driven by a scaphoid-waist nonunion rather than scapholunate failure. SNAC I: arthritis between the radial styloid and the distal scaphoid fragment. SNAC II: arthritis extends to the scaphocapitate joint. SNAC III: arthritis involves the capitolunate (periscaphoid midcarpal) joint. The crucial difference from SLAC is that, because the fracture is at the waist, the proximal scaphoid fragment stays congruent in the scaphoid fossa, so the proximal-pole radioscaphoid articulation (and the radiolunate joint) is spared longer than in SLAC — which is why a SNAC wrist can still have a usable radiocarpal joint when the midcarpal joint is destroyed. As in SLAC, the radiolunate joint must be preserved for four-corner fusion to be appropriate; if it is involved, choose PRC or total wrist fusion.
Total (or partial) wrist denervation answers "what else could you offer?". It relieves pain by interrupting the joint's afferent innervation without altering bone, cartilage or motion — the classic Wilhelm procedure divides up to ten articular nerve branches, but the practical, commonly performed version is a combined anterior and posterior interosseous neurectomy (AIN + PIN) through one or two small incisions. Its appeal is that it preserves the entire range of motion and grip, is low-morbidity, and burns no bridges (4CF, PRC or fusion all remain possible later). Indications: a patient with painful SLAC/SNAC arthritis who wants to keep maximal motion, a poor candidate for major reconstruction, or as an adjunct. Limitations: it does not address the underlying mechanical collapse and pain relief is variable and may diminish over time; a diagnostic local-anaesthetic block of the AIN/PIN that abolishes the pain helps predict who will benefit.
Relevant Anatomy and Biomechanical Principles
- The wrist functions as two carpal rows. The proximal row (scaphoid, lunate, triquetrum) acts as an intercalated segment with no direct tendon insertions, moving passively in response to forces transmitted through the distal row. The distal row (trapezium, trapezoid, capitate, hamate) is rigidly interconnected and moves as a unit.
- The scaphoid is the critical mechanical link between the two rows. It bridges the proximal and distal carpal rows and prevents the lunate from extending into a DISI position. When the scapholunate ligament ruptures or the scaphoid fractures and does not unite, this mechanical link is lost and the lunate extends (DISI), the capitate migrates proximally, and the carpus collapses.
- In SLAC wrist, the pattern of degeneration follows the loss of scaphoid support. The scaphoid rotates into flexion and the increased contact pressures at the styloscaphoid and radioscaphoid joints cause progressive arthritis. The radiolunate joint is biomechanically spared because the lunate remains congruent within the lunate fossa even as it extends into DISI.
- The lunate fossa of the radius is a concave, spherical articulation that matches the proximal convexity of the lunate. This joint has a large contact area and low contact pressure, which explains why it is preserved in SLAC wrist until very late.
- After 4CF, the radiolunate joint becomes the sole remaining articulation between the forearm and the carpus. The fused capitate-lunate-hamate-triquetrum mass transmits loads through the lunate into the lunate fossa.
- Capitate: the largest carpal bone, centred in the distal row. Its proximal pole articulates with the lunate (the lunocapitate joint). After 4CF, the capitolunate interface must fuse for the procedure to succeed.
- Lunate: the keystone of the proximal row. Its proximal surface articulates with the radius (preserved) and its distal surface with the capitate (must fuse).
- Hamate: articulates with the triquetrum and the capitate. Inclusion in the fusion mass provides lateral stability and increases the surface area for fusion.
- Triquetrum: articulates with the lunate and hamate. Some surgeons exclude the triquetrum (three-corner fusion) but including it adds stability and does not significantly reduce motion.
- Flexion-extension arc is reduced to approximately 50-60% of normal (approximately 40-60 degrees total arc). This is because midcarpal motion is eliminated (the midcarpal joint is fused) and only radiolunate motion remains.
- Radioulnar deviation is reduced to approximately 50% of normal.
- Grip strength typically returns to approximately 65-80% of the contralateral side, which is often better than PRC in comparative studies.
- The fused carpal mass acts as a single block that pivots on the radiolunate joint, providing a stable but mobile wrist.
Internervous Plane and Surgical Interval
- Incision: longitudinal dorsal skin incision centred over Lister tubercle, extending approximately 6-8 cm from the distal radius to the midcarpal region.
- Interval: the approach is developed between the third (extensor pollicis longus) and fourth (extensor digitorum communis / extensor indicis proprius) dorsal compartments. The EPL is identified at its oblique course around Lister tubercle and retracted radially. The EDC/EIP tendons are retracted ulnarly.
- The posterior interosseous nerve (PIN) terminal branch is identified on the floor of the fourth compartment and sacrificed (neurectomy) to provide partial wrist denervation as part of the pain-relief strategy. A 1-2 cm segment is resected to prevent neuroma formation at the resection site.
- The dorsal wrist capsule is incised longitudinally, and the capsular flaps are elevated to expose the carpus from the distal radius to the midcarpal row.
- Lister tubercle - the key landmark on the dorsal radius, between the second and third compartments
- Extensor pollicis longus (EPL) - crosses obliquely in the third compartment; must be identified and protected
- Extensor digitorum communis (EDC) and extensor indicis proprius (EIP) - fourth compartment; retracted ulnarly
- Extensor carpi radialis brevis (ECRB) and longus (ECRL) - deep to the second compartment, radial side; may be retracted radially
- Dorsal radiocarpal ligament and dorsal intercarpal ligament - divided to access the carpus; some surgeons attempt repair at closure
- Posterior interosseous nerve - terminal branch on the floor of the fourth compartment; sacrificed for denervation
- Radial styloidectomy extension: the incision can be extended radially to allow access to the radial styloid for styloidectomy, performed to prevent radial impingement on the fused carpus during radial deviation.
- Some surgeons use a separate radial incision for the styloidectomy to avoid extensive dorsal dissection.
The posterior interosseous nerve terminal branch is routinely sacrificed during the dorsal approach for four-corner fusion. This provides a partial wrist denervation that contributes to pain relief. Examiners expect you to mention this as a standard step. A segment of approximately 1-2 cm is excised to prevent neuroma formation. The PIN motor branch to the extensor muscles branches proximally and is not at risk.
Patient Positioning and Setup
- Position: supine with the arm extended on a hand table. A padded tourniquet is applied to the upper arm. The arm is draped free to allow full wrist flexion, extension, and rotation.
- Anaesthesia: general or regional (brachial plexus block - axillary or supraclavicular). Regional anaesthesia provides excellent post-operative analgesia and allows early mobilisation of the fingers.
- Tourniquet: exsanguination and inflation to approximately 250 mmHg. The tourniquet should be released before closure to assess haemostasis, particularly around the dorsal radial artery branches.
- Fluoroscopy: essential. The image intensifier is positioned to obtain PA, lateral, and oblique views of the wrist. Intra-operative imaging confirms scaphoid excision completeness, correction of lunate alignment (reduction of DISI), hardware position, and adequacy of styloidectomy.
- Instrumentation: standard hand surgery tray, osteotomes, rongeurs, K-wires (0.045 and 0.062 inch), and the chosen fixation device (circular plate set, headless compression screws, or K-wires alone).
- Bone graft: autologous cancellous bone graft from the distal radius (via the same dorsal incision or a separate radial styloid window) or from the excised scaphoid (the healthy portions of the scaphoid provide excellent local autograft). Some surgeons use bone substitute or allograft.
Surgical Technique
The gold standard fixation method with the highest published union rates.
A longitudinal dorsal incision is made centred over Lister tubercle. The third and fourth extensor compartments are opened and the EPL and EDC tendons are retracted. The PIN terminal branch is identified and a 1-2 cm segment is excised. The dorsal capsule is incised longitudinally.
the scaphoid is identified and progressively excised using osteotomes, rongeurs, and a curette. Complete excision is essential - any remaining scaphoid fragments can cause persistent pain. The excised scaphoid bone is saved for local autograft. The scaphoid fossa of the radius is inspected to confirm it is free of significant arthritis.
approximately 3-5 mm of the radial styloid is resected using an oscillating saw or osteotome to prevent impingement on the fused carpus during radial deviation. Care is taken to protect the volar radiocarpal ligaments (particularly the radioscaphocapitate ligament) to maintain stability.
the lunate is reduced from its extended DISI position into a neutral or slight flexed position. This is critical - failure to reduce the lunate malalignment results in limited post-operative motion and dorsal impingement. The lunate is temporarily held reduced with a 0.045 inch K-wire into the radius.
the articular cartilage is denuded from the lunocapitate, lunotriquetral, capitohamate, and triquetrohamate joints using curettes, rongeurs, and a burr. Subchondral bone is perforated to promote bleeding and fusion. Cancellous autograft (from the excised scaphoid or distal radius) is packed into the fusion interfaces.
multiple 0.045-0.062 inch K-wires are inserted across the fusion mass - typically one from capitate to lunate, one from hamate to lunate, one from triquetrum to lunate, and one from capitate to hamate. Pins are cut flush or buried subcutaneously. The temporary lunate-reduction K-wire into the radius is retained for 4-6 weeks.
Fluoroscopic confirmation ensures complete scaphoid excision, adequate styloidectomy, neutral lunate alignment, and appropriate K-wire positions. The capsule is closed where possible and extensor retinaculum is repaired.
If the lunate is left in DISI (extended) position, the fused carpal mass will impinge dorsally on the radius during attempted wrist extension, severely limiting the functional arc. Always reduce the lunate to neutral alignment and stabilise it with a temporary K-wire into the radius before applying definitive fixation. Failure to correct DISI is a common technical error that produces a stiff, painful wrist despite a successful fusion.
Structures at Risk and Complications
Four-corner fusion has a significant complication profile. The overall complication rate ranges from approximately 10-30% in published series, with reoperation rates of approximately 10-20%.
- Nonunion - the most significant complication and the commonest reason for reoperation. Rates range from approximately 3% with K-wires to 15-30% with circular plates in some series. Risk factors include inadequate cartilage denudation, poor bone grafting, smoking, and insufficient fixation. Nonunion presents with persistent wrist pain and may require revision fusion or conversion to total wrist arthrodesis.
- Dorsal impingement - the fused carpal mass or prominent hardware impinges on the dorsal rim of the radius during wrist extension. This causes pain with terminal extension and is a common cause of persistent post-operative symptoms. Prevention includes adequate dorsal rim trimming, ensuring the lunate is reduced from DISI, and using low-profile fixation.
- Hardware complications - prominent dorsal hardware (especially circular plates) causes extensor tendon irritation, tenosynovitis, and rarely extensor tendon rupture. Hardware removal is required in approximately 10-30% of cases with circular plates. K-wires may back out or cause pin-tract infection.
- Radial styloid impingement - inadequate styloidectomy results in residual impingement between the radial styloid and the fused carpus during radial deviation. This presents as pain on radial deviation and may require revision styloidectomy.
- CRPS (complex regional pain syndrome) - reported in approximately 2-5% of cases. Early mobilisation of fingers, adequate analgesia, and early hand therapy are preventive.
- Infection - superficial wound infection in approximately 1-3%; deep infection requiring implant removal is rare.
- Residual stiffness - the expected motion after 4CF is approximately 40-60 degrees of flexion-extension (roughly 50-60% of normal). Patients who expect full motion will be disappointed. Pre-operative counselling is essential.
- Extensor tendon adhesion or rupture - dorsal dissection and hardware can cause adhesions limiting finger and wrist extension. EPL rupture has been reported with prominent hardware.
- Progressive radiolunate arthritis - although the radiolunate joint is preserved at surgery, it may degenerate over time (approximately 10-15% at long-term follow-up), eventually requiring conversion to total wrist arthrodesis.
- Superficial radial nerve neuroma - the dorsal approach puts the superficial radial nerve branches at risk; neuroma formation causes dorsal wrist and hand dysesthesia.
Examiners may ask about nonunion rates by fixation method. K-wires have the lowest nonunion rates (approximately 3-5%) but require prolonged immobilisation. Circular plates have the highest published nonunion rates (up to 15-30% in some series) due to the plate preventing compression across fusion surfaces. Headless compression screws show promising intermediate results (approximately 5-10%).
Guidelines, Registries and Global Practice
There is no single universal guideline for four-corner fusion; practice follows evidence-based principles of carpal arthritis staging and motion-preserving surgery. Several international hand surgery societies have published consensus statements and recommendations:
- ASSH (American Society for Surgery of the Hand): four-corner fusion and PRC are both recognised as motion-preserving options for SLAC/SNAC wrist stages I-II. The choice depends on the condition of the radiolunate and capitate head cartilage, patient demands, and surgeon experience.
- BSSH (British Society for Surgery of the Hand): guidelines support limited wrist arthrodesis as a motion-preserving alternative to total wrist fusion in appropriately selected patients with SLAC/SNAC arthritis. Patient counselling about expected motion and grip strength outcomes is emphasised.
- FESSH (Federation of European Societies for Surgery of the Hand): European practice generally favours four-corner fusion over PRC for patients with high functional demands, reflecting a preference for retaining the lunocapitate articulation. However, the evidence does not strongly favour one over the other.
- Large institutional series from the Mayo Clinic, Virginia Hand Center, and European centres confirm approximately 85-95% union rates with K-wire fixation and approximately 70-80% union rates with circular plates.
- Conversion to total wrist arthrodesis after failed 4CF is reported at approximately 10-15% at 10 years in most series, comparable to PRC conversion rates.
- Patient satisfaction scores are generally high (approximately 75-90% satisfied or very satisfied) in patients who achieve union.
- European hand surgeons have historically been more aggressive in performing limited wrist fusions compared with North American surgeons, who have tended toward PRC as the simpler first-line option for SLAC/SNAC wrist. This gap is narrowing as evidence accumulates.
- Japanese hand surgery literature has contributed significantly to understanding carpal kinematics after limited fusion, with several biomechanical studies from Japanese centres.
- In low- and middle-income settings, both PRC and K-wire four-corner fusion are valued as reliable, low-cost procedures that avoid the need for expensive implants.
- The trend away from circular plates toward K-wires or headless compression screws is now widespread in high-volume hand surgery centres globally, driven by the higher complication rates of dorsal plating.
- The choice between 4CF and PRC remains one of the most debated topics in hand surgery. Neither procedure has been shown to be clearly superior in high-quality randomised trials.
- PRC is simpler, faster, has a lower complication rate, and provides slightly better motion. 4CF may provide marginally better grip strength by retaining the native lunocapitate joint.
- Most surgeons now select based on: (1) radiolunate joint status (if arthritic, PRC or TWA), (2) capitate head cartilage (if arthritic, 4CF rather than PRC), (3) patient demands and expectations, and (4) surgeon experience and comfort with each technique.
Memory Aids
SLACSLAC Wrist Stages - SLAC Progresses PROXIMALLY
Hook:SLAC progresses from styloscaphoid (I) to radioscaphoid (II) to radiolunate (III) - 4CF works in I and II when the radiolunate is still healthy
FOURFour-Corner Fusion Indications - FOUR
Hook:4CF is for FOUR indications: Failed SL ligament, Os scaphoideum nonunion, Uninvolved radiolunate joint, Retained motion desired
PINCHComplications of Four-Corner Fusion - PINCH
Hook:After 4CF, watch for PINCH complications: Pseudarthrosis, Impingement, Nerve irritation, CRPS/stiffness, Hardware problems
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old right-hand-dominant mechanic presents with progressive right wrist pain and stiffness over 3 years. He recalls a fall on the outstretched hand approximately 10 years ago that was treated in a splint for 2 weeks. PA and lateral wrist radiographs show a dorsiflexed lunate (DISI), narrowing of the radioscaphoid joint with osteophytes, and a preserved radiolunate joint. The scaphoid appears shortened. Discuss your management.”
“A 45-year-old woman underwent scaphoid excision and four-corner fusion with a circular plate 14 months ago for SLAC II wrist. She reports persistent dorsal wrist pain, worse with extension, and has limited wrist extension to 20 degrees. Radiographs show a fused carpal mass with the circular plate prominent dorsally, and the lunate appears slightly extended. There is no lucency at the fusion interfaces. How would you manage her?”
One-liner
- Motion-preserving limited wrist arthrodesis for SLAC/SNAC arthritis: excise the scaphoid, fuse capitate-lunate-hamate-triquetrum, preserve the radiolunate joint
- Based on Watson and Ballet SLAC classification; appropriate for stages I and II with preserved radiolunate joint
SLAC staging
- Stage I: styloscaphoid arthritis (radial styloid-scaphoid)
- Stage II: entire radioscaphoid arthritis
- Stage III: radiolunate arthritis (contraindication for 4CF)
- Radiolunate preservation is the prerequisite for 4CF
Indications (FOUR)
- Failed scapholunate ligament (SLAC)
- Os scaphoideum nonunion (SNAC)
- Uninvolved radiolunate joint (mandatory)
- Retained motion desired by patient
Contraindications
- Radiolunate arthritis (SLAC III)
- Inflammatory arthritis (RA, psoriatic)
- Capitate head cartilage loss
- Active infection, severe osteoporosis
Fixation options
- K-wires: gold standard, lowest nonunion rate (3-5%), requires 6-8 weeks immobilisation
- Circular plate: higher nonunion rate (up to 15-30%), dorsal impingement risk
- Headless compression screws: emerging, low profile, promising early results
Surgical steps
- Dorsal approach between 3rd and 4th compartments
- PIN neurectomy (partial denervation)
- Complete scaphoid excision
- Radial styloidectomy (3-5 mm)
- Reduce lunate from DISI to neutral
- Denude four-corner joints, bone graft, fix
Complications (PINCH)
- Pseudarthrosis / nonunion (most significant)
- Impingement (dorsal, from plate or residual DISI)
- Nerve irritation (PIN branch, superficial radial)
- CRPS / stiffness
- Hardware problems (plate prominence, tendon irritation)
4CF vs PRC
- 4CF: better grip strength, retains lunocapitate joint, higher complication rate, more complex surgery
- PRC: simpler, faster recovery, better motion, lower complication rate, slightly less grip strength
- Choice: check radiolunate joint and capitate head cartilage; individualise based on patient demands
Outcomes
- Flexion-extension arc approximately 40-60 degrees (50-60% of normal)
- Grip strength approximately 65-80% of contralateral
- Union rate approximately 85-95% with K-wires
- Conversion to TWA approximately 10-15% at 10 years
- Patient satisfaction approximately 75-90% when union achieved
Evidence Base
- In a review of 4,000 wrist radiographs, Watson and Ballet identified 210 cases of degenerative wrist arthritis after excluding other arthritides. The most common pattern (57%) was arthritis between the scaphoid, lunate, and radius - the SLAC pattern; 27% occurred at the scaphoid-trapezium-trapezoid (STT) joint; a combination pattern was seen in 15%. Twenty operations were performed on 19 SLAC patients, with 18 of 19 reporting less pain postoperatively and none requiring pain medication. Flexion-extension and radial-ulnar deviation arcs improved considerably after surgery.
- In a retrospective comparison of 17 four-corner arthrodesis patients (mean 27-month follow-up) and 10 patients with 11 proximal row carpectomies (mean 37-month follow-up) for SLAC wrist, PRC achieved a greater total arc of motion (115 degrees = 64% of opposite wrist) than 4CF (95 degrees = 47% of opposite wrist). Grip strength was also better after PRC (94% of opposite wrist) than after 4CF (74%). Three of 17 4CF wrists failed and were converted to total wrist fusion, with two more awaiting arthrodesis; there were no failures in the PRC group.
- Retrospective comparison of 64 four-corner fusions over 5 years: 21 K-wires, 26 locking plates, and 17 retrograde headless compression screws. All three groups showed significant improvements in grip strength, pain at rest and with activity, wrist range of motion, and DASH scores. Overall complication and nonunion rates were low and not significantly different between groups. However, the headless compression screw group had significantly better postoperative pain with activity, dorsal flexion, and DASH scores than the K-wire group.
- A systematic review collated 52 articles examining outcomes for SLAC or SNAC wrists treated with PRC or 4CF. Both procedures improved pain and subjective outcomes in appropriately staged patients. PRC may provide better postoperative range of movement and lacks the 4CF-specific complications of nonunion, hardware problems, and dorsal impingement. However, the risk of subsequent osteoarthritis was significantly higher after PRC (although the majority were asymptomatic at the time of review). Grip strength, pain relief, and subjective outcomes were similar in both groups.
- Of 489 wrists that underwent 4CF for SLAC between 1982 and 2003 at the originators' institution, 15 wrists in 12 patients were available for 10-year minimum follow-up (mean 18 years). Mean flexion-extension arc was 68.6 degrees and radial-ulnar deviation arc 32.9 degrees. Mean QuickDASH was 7.8 (only 1 score above 16). 73% of radiographs showed minimal to moderate joint destruction and 27% severe. Patient satisfaction was high and functional impairment was low despite radiographic radiolunate changes in most patients.