Tissue freezes, then thawing drives the real damage; the final injury level may take weeks to declare
- Frostbite is a freeze-thaw injury: ice crystals damage tissue on freezing, but the inflammation and microvascular thrombosis after thawing cause much of the final loss.
- Do not rewarm in the field if there is any chance the part will refreeze. A refreeze-thaw cycle is far more damaging than staying frozen during transfer.
- Definitive hospital rewarming is rapid immersion in warm water at 37 to 39 degrees Celsius with analgesia, because thawing is very painful.
- Initial appearance does not predict the final injury. The depth and tissue loss declare themselves over days to weeks.
- For severe deep frostbite presenting early, tissue plasminogen activator (thrombolysis) or the prostacyclin analogue iloprost can dramatically reduce amputation.
- Surgery is usually delayed: wait for clear demarcation before amputation, unless there is wet gangrene, spreading infection or sepsis.
- “Frostbite mantra: freeze, thaw, then watch. The most important early decisions are when to rewarm and whether the patient is a candidate for thrombolysis or iloprost.
- “The classic surgical aphorism is 'frostbite in January, amputate in July' — let the tissue demarcate rather than debriding early.
- “Hypothermia takes priority over the frozen part: resuscitate and rewarm the core before focusing on the digits.
- “Blisters reaching the tip suggest superficial injury; haemorrhagic blisters that stop proximally suggest deep injury and worse prognosis.
Frostbite (Cold Injury)
Frostbite is a freeze-thaw injury and the appearance early on under-predicts tissue loss. Treat hypothermia first, never rewarm if refreezing is possible, use rapid warm-water rewarming in hospital, and identify early the severe deep injuries that may benefit from thrombolysis or iloprost. Amputation is almost always delayed until demarcation is clear.
- Low Concern
- Definitive rewarming guaranteed before any refreezing
- High Concern
- Part may refreeze during transfer
- Management Effect
- Keep frozen and evacuate rather than thaw then refreeze
- Low Concern
- Normothermic, stable patient
- High Concern
- Hypothermia or systemic instability
- Management Effect
- Resuscitate and core-rewarm before focusing on the part
- Low Concern
- Clear blisters reaching the tip, soft tissue after thaw
- High Concern
- Haemorrhagic blisters stopping proximally or hard insensate tissue
- Management Effect
- Deep injury triggers imaging and salvage-drug assessment
- Low Concern
- Presenting within the salvage window (hours)
- High Concern
- Delayed presentation beyond 24 to 48 hours
- Management Effect
- Early window allows thrombolysis or iloprost
- Low Concern
- Dry, demarcated, uninfected gangrene
- High Concern
- Wet gangrene, spreading infection or sepsis
- Management Effect
- Dry demarcation waits; wet or infected forces early surgery
FREEZEField | THAWHospital | WAITSurgery |
|---|---|---|
F Find and remove from cold Shelter the patient and remove wet, constrictive clothing and jewellery. | T Temperature-controlled bath Rapid immersion at 37 to 39 degrees Celsius until the part is soft and red. | W Watch for demarcation Allow weeks for the boundary between dead and viable tissue to form. |
R Refreeze risk Do not thaw the part if it might refreeze before reaching definitive care. | H Hurts a lot Give strong analgesia; thawing is extremely painful. | A Amputate late Frostbite in January, amputate in July: early debridement removes salvageable tissue. |
E Examine the core Treat hypothermia first; a cold heart and brain outrank cold fingers. | A Anti-thrombotic window Consider thrombolysis or iloprost for severe deep injury presenting early. | I Intervene early only if Wet gangrene, spreading infection or sepsis force earlier surgery. |
E Elevate and protect Pad the part, avoid rubbing or dry heat, and prevent further trauma. | W Wound and tetanus care Aloe vera, ibuprofen, blister care, elevation and tetanus cover. | T Therapy and rehab Hand or foot therapy, oedema control and cold-sensitivity counselling. |
Z Zero rubbing Never rub with snow; mechanical trauma worsens ice-crystal injury. | ||
E Evacuate Plan rapid transfer so definitive rewarming can be done safely. | ||
What you do in the cold matters most. | Thaw fast, treat the pain. | Let the line declare itself. |

Overview and Epidemiology
Frostbite is the freezing of tissue that occurs when the local temperature drops low enough for ice crystals to form. It most often affects the exposed peripheries: fingers, toes, ears, nose and cheeks. For the orthopaedic and hand surgeon, the digits matter most, because deep frostbite of the fingers and toes is the injury that leads to amputation.
Frostbite was historically a military problem, but it is now increasingly a civilian injury. The people affected today include mountaineers and high-altitude climbers, outdoor and homeless populations, people intoxicated with alcohol or drugs in cold weather, those with psychiatric illness, and patients with peripheral vascular disease or diabetes who have reduced cold sensation and perfusion.
The single most important concept to state early is that frostbite is a freeze-thaw injury. The damage from freezing is only part of the story; a large share of the final tissue loss is driven by the inflammation and microvascular thrombosis that follow rewarming. This shapes everything: when to thaw, whether to give clot-busting or vessel-opening drugs, and when to operate.
Pathophysiology and Anatomy
Frostbite injury happens in overlapping phases:
- Prefreeze (cooling): the tissue cools, vessels constrict, sensation is lost and the skin becomes pale and numb before any ice forms.
- Freeze-thaw: ice crystals form, first outside the cells and then within them at lower temperatures. Crystals damage cell membranes, draw water out of cells and concentrate electrolytes, injuring the tissue directly.
- Vascular stasis: vessels alternately constrict and dilate, and plasma leaks out, causing sludging and stasis in the small vessels.
- Late progressive ischaemia: after thawing, reperfusion releases inflammatory mediators (prostaglandins, thromboxane and free radicals), platelets aggregate and microvascular thrombosis spreads. This progressive thrombosis is the key target of thrombolysis and iloprost.
The digit is vulnerable because it has a high surface-area-to-volume ratio, end-arterial blood supply and little insulating soft tissue. Once the small digital vessels thrombose, the distal pulp and nail bed lose perfusion and progress to dry gangrene over days to weeks.
Reperfusion after rewarming triggers an inflammatory cascade with thromboxane and prostaglandins, platelet aggregation and progressive microvascular thrombosis. This is why early appearance under-predicts loss and why anti-thrombotic and vasodilator drugs can salvage tissue.
A freeze-thaw-refreeze cycle multiplies ice-crystal and vascular injury. If there is any risk the part will refreeze during transfer, it is safer to keep it frozen until definitive rewarming can be guaranteed.

Frostbite (freezing injury) and non-freezing cold injury such as trench foot are different conditions. Trench foot follows prolonged cold and wet exposure above freezing, the tissue does not freeze, and aggressive rapid rewarming is not the treatment. Misclassifying one as the other leads to the wrong management.
Classification and Severity
Before the established injury, the mildest end of the cold-injury spectrum is frostnip — superficial cooling with pallor and numbness but no ice-crystal formation and no tissue loss, fully reversible on rewarming. It causes no permanent damage but is an important warning sign that true (freezing) frostbite may follow if exposure continues.
Two complementary frameworks are then used for established frostbite. A simple depth-based scheme (like burns) is intuitive at the bedside, while a four-grade severity scheme — the Cauchy classification — based on the appearance of the part after rapid rewarming (day 0) plus an early bone scan (around day 2) predicts outcome and the level of likely tissue loss.
- Tissue Involved
- Epidermis only
- Appearance
- Numb central white or yellow plaque with surrounding redness and swelling; no blisters
- Typical Outcome
- Heals fully; may have skin peeling and cold sensitivity
- Tissue Involved
- Epidermis and dermis
- Appearance
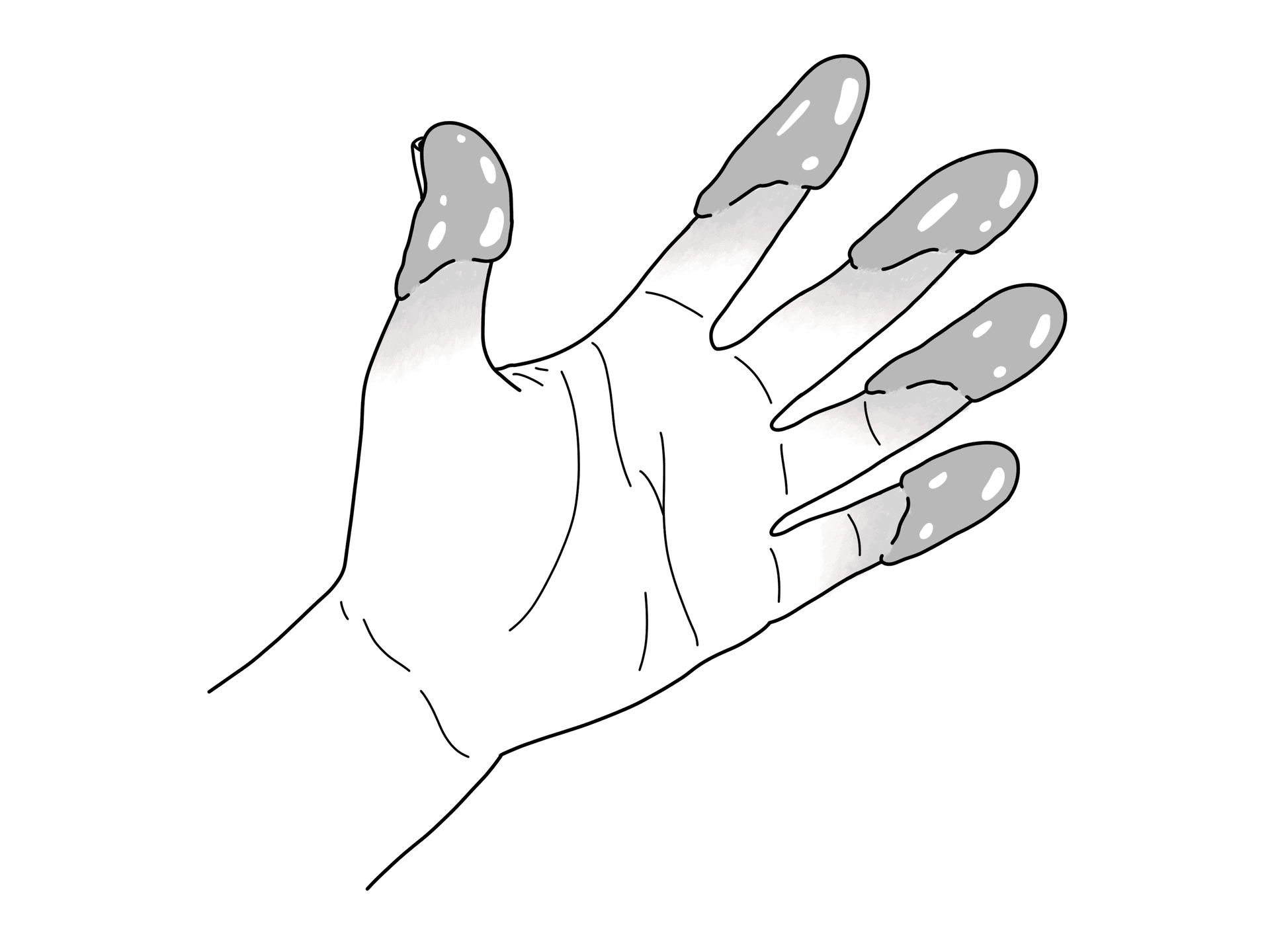
- Clear or milky fluid-filled blisters reaching the fingertip, with redness and swelling
- Typical Outcome
- Usually heals; risk of long-term cold sensitivity and nail change
- Tissue Involved
- Full-thickness skin and subcutaneous tissue
- Appearance
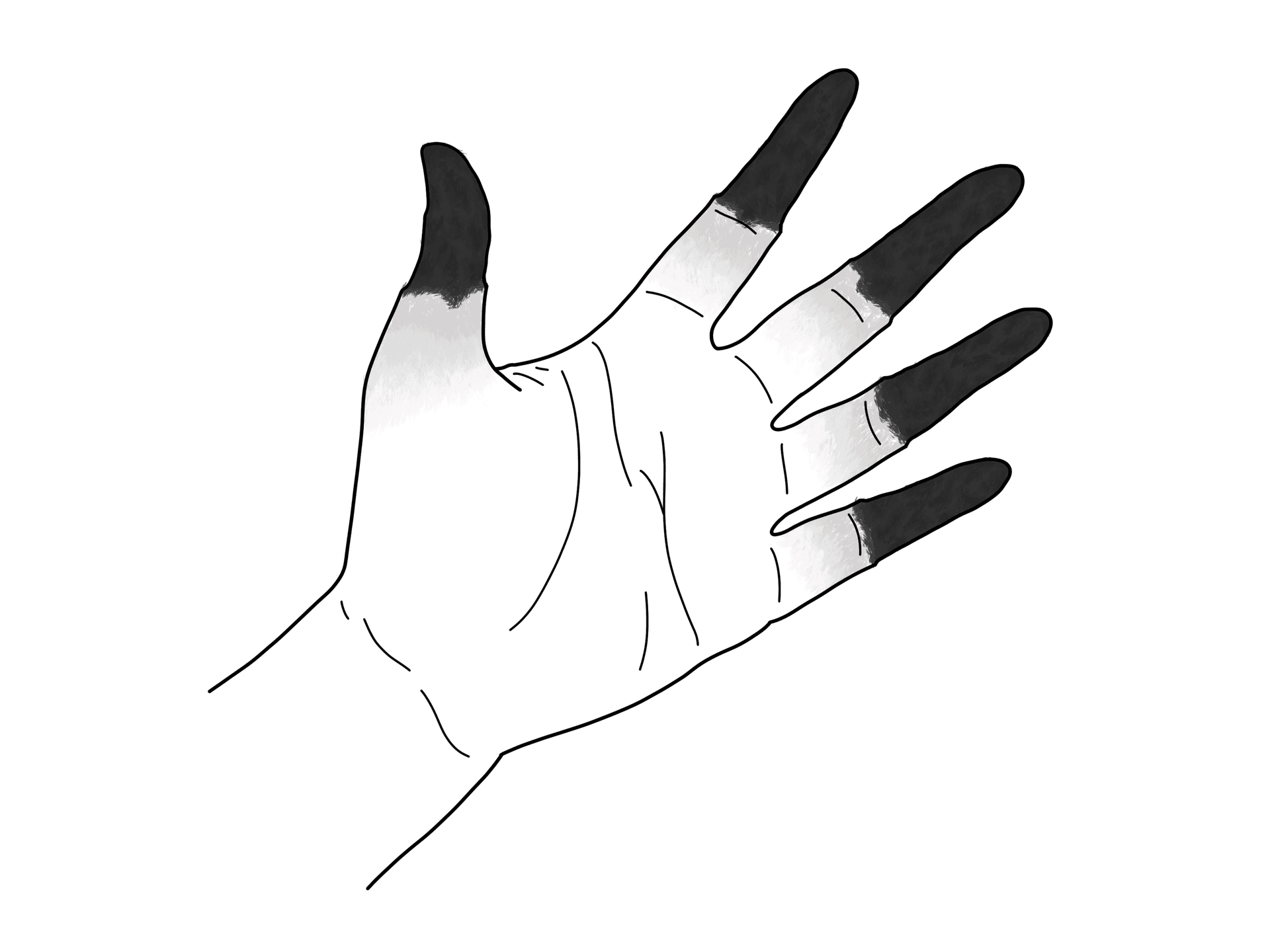
- Haemorrhagic (blood-filled) blisters that stop short of the tip; deeper tissue injury
- Typical Outcome
- Tissue loss likely; some loss of skin or pulp
- Tissue Involved
- Muscle, tendon and bone
- Appearance
- Hard, woody, mottled or blue-grey tissue; little or no blistering; deep insensate part
- Typical Outcome
- High amputation risk; deep structural loss
Clear blisters that extend to the fingertip suggest superficial injury and a better prognosis. Haemorrhagic blisters that stop proximally, or an absence of blisters with hard insensate tissue, suggest deep injury and a worse prognosis.
Clinical Assessment
The history should capture the cold exposure and the salvage window, because timing changes treatment.
Ask:
- How cold was it, for how long, and was there wind chill, altitude or water immersion?
- When did the part freeze, and has it already been thawed or refrozen?
- Has any field rewarming been attempted, and was there a risk of refreezing afterwards?
- Time since injury: is the patient still within the window for thrombolysis or iloprost?
- Was there hypothermia, intoxication, trauma or entrapment?
- Patient factors: smoking, diabetes, peripheral vascular disease, prior frostbite and tetanus status.
Examination is done before and after rewarming and then repeated:
- Before rewarming: the part is often white or waxy, hard and numb; do not predict outcome from this.
- After rewarming: assess colour return, capillary refill, sensation, and the type and extent of blisters.
- Look: the level of any colour change, blistering, mottling and the proximal boundary of injury.
- Feel: whether tissue is soft and pliable (better) or remains hard and woody (worse).
- Systemic: core temperature, conscious level and signs of hypothermia or sepsis.
A hypothermic patient must be resuscitated and core-rewarmed before attention turns to the frozen digits. Treating the fingers while ignoring a dangerously low core temperature is unsafe.
Investigations and Imaging
Most frostbite is a clinical diagnosis. Imaging matters in severe deep injury, where it predicts tissue loss and guides salvage and surgical planning.
- Plain radiographs: initially normal; later may show soft-tissue loss, osteolysis, bony resorption and, in long-standing or childhood cases, growth plate damage.
- Technetium bone scan (triple-phase): the key prognostic test in deep frostbite. Absent uptake in a digit predicts non-viable tissue and likely amputation, while preserved uptake predicts salvage. Repeating the scan after a few days helps define the eventual level.
- Angiography or MR angiography: can demonstrate small-vessel thrombosis and is used when thrombolysis is being considered, both to confirm occlusion and to monitor response.
- SPECT or SPECT-CT: can refine the bone scan and help plan the amputation level.
In deep frostbite, a technetium bone scan performed in the first days shows which tissue has lost perfusion. Absent uptake predicts loss and informs both the decision to attempt salvage and, later, the amputation level. Plain X-rays are normal early and unhelpful for prognosis.

Differential Diagnosis
The frozen, then red and blistered, then blackened digit can be confused with other causes of a cold, discoloured or necrotic extremity. The discriminating feature is usually the clear history of freezing cold exposure.
- Overlapping Feature
- Cold, numb, later blistered or blackened digits
- Discriminating Feature
- Clear sub-freezing exposure; freeze-thaw history; tip-to-proximal injury pattern
- Why It Matters
- Needs rewarming protocol and possible thrombolysis or iloprost
- Overlapping Feature
- Cold, swollen, painful feet after cold exposure
- Discriminating Feature
- Above-freezing cold and wet, no tissue freezing
- Why It Matters
- Gradual rewarming; rapid immersion is wrong
- Overlapping Feature
- Cold, pale, painful, pulseless extremity
- Discriminating Feature
- Embolic or thrombotic vascular history without freezing exposure
- Why It Matters
- Needs urgent revascularisation, not rewarming
- Overlapping Feature
- Cold-triggered colour change and discomfort
- Discriminating Feature
- Episodic or milder, no actual tissue freezing or gangrene
- Why It Matters
- Conservative management and warmth, not amputation
- Overlapping Feature
- Blackened, malodorous tissue, systemic upset
- Discriminating Feature
- Spreading infection, sepsis and rapid progression
- Why It Matters
- Forces early surgery rather than waiting for demarcation
Management Algorithm
Pre-hospital priorities:
- Move the patient to shelter and remove wet, constrictive clothing and any rings or jewellery.
- Treat hypothermia and any major trauma first.
- Protect the part: pad it, avoid rubbing, and do not apply dry heat such as a fire or exhaust pipe (the part is numb and burns easily).
- Do not rewarm the part if there is any chance it will refreeze before reaching care. Walking on already-thawed frostbitten feet also risks further damage.
- If safe rewarming is not possible, keep the part frozen and evacuate.
Definitive Treatment and Salvage Options
The treatment is staged: protect and rewarm correctly, then identify the severe deep injuries that can be salvaged with thrombolysis or iloprost, then wait for demarcation before surgery.
- Mechanism / Purpose
- Reverse freezing quickly to limit ice-crystal injury
- Timing
- On arrival, once refreeze risk is removed
- Key Caveat
- Very painful; give analgesia; avoid dry heat
- Mechanism / Purpose
- Block prostaglandin and thromboxane pathways
- Timing
- Started after rewarming
- Key Caveat
- Adjuncts; not a substitute for salvage drugs in deep injury
- Mechanism / Purpose
- Dissolve microvascular thrombosis to restore perfusion
- Timing
- Best within about 24 hours of injury
- Key Caveat
- Bleeding risk; contraindicated after recent trauma, surgery or bleeding
- Mechanism / Purpose
- Vasodilate and reduce platelet aggregation
- Timing
- Best within about 48 hours; can be later than tPA
- Key Caveat
- No major bleeding risk, so usable when tPA is contraindicated
- Mechanism / Purpose
- Increase oxygen delivery to marginal tissue
- Timing
- Adjunct, often combined with iloprost
- Key Caveat
- Evidence limited to small studies; not stand-alone
- Mechanism / Purpose
- Remove demarcated non-viable tissue
- Timing
- After demarcation (weeks), unless infection forces earlier
- Key Caveat
- Early debridement sacrifices salvageable tissue
Both reduce amputation in severe deep frostbite. Thrombolysis (tPA) dissolves clot but carries bleeding risk and has a tight early window. Iloprost is a vasodilating prostacyclin analogue with no major bleeding risk, a slightly longer window, and is the better choice when the patient has bleeding risk or recent trauma.
Surgical Technique
Surgery in frostbite is mostly about timing and tissue preservation rather than a single procedure. The aim is to remove demarcated dead tissue at the latest safe point while keeping every millimetre of viable length.
Core surgical principles:
- Default to delayed surgery; let demarcation declare the true level before committing to amputation.
- Use clinical demarcation plus imaging (bone scan, and SPECT-CT where available) to plan the level.
- Preserve maximal viable length and functional units, especially the thumb and the great toe.
- Optimise the patient first: stop smoking, correct nutrition and manage comorbidities that impair healing.
Complications
Complications arise from both the acute injury and the long aftermath of cold injury.
- Mechanism
- Progressive microvascular thrombosis and necrosis
- Prevention or Response
- Correct rewarming, early thrombolysis or iloprost, delayed surgery
- Mechanism
- Secondary infection of necrotic tissue
- Prevention or Response
- Wound care, tetanus cover, antibiotics and earlier surgery if it spreads
- Mechanism
- Freeze-thaw-refreeze cycle
- Prevention or Response
- Never rewarm if the part might refreeze before definitive care
- Mechanism
- Nerve and vascular injury
- Prevention or Response
- Counsel on cold avoidance; manage neuropathic pain
- Mechanism
- Autonomic and sensory nerve damage
- Prevention or Response
- Long-term symptom management and reassurance
- Mechanism
- Cartilage and periarticular injury
- Prevention or Response
- Hand or foot therapy; later joint care
- Mechanism
- Freezing injury to the physis
- Prevention or Response
- Recognise risk; long-term orthopaedic follow-up for deformity
Rehabilitation and Outcomes
Recovery from significant frostbite is long, and rehabilitation begins as soon as the tissue is stable.
Priorities:
- elevate to control oedema and protect blisters and wounds
- begin gentle hand or foot therapy to preserve motion once safe
- manage neuropathic pain and cold sensitivity, which are very common
- support smoking cessation, because nicotine worsens vasoconstriction
- counsel on lifelong cold protection, as previously frostbitten parts are more vulnerable
Outcomes and Prognosis
Outcome depends on the depth and grade of injury, the time to correct rewarming, whether the part refroze, the salvage window for thrombolysis or iloprost, and patient factors such as smoking and vascular disease. Many patients keep long-term cold sensitivity, altered sensation and pain even when the digits are saved.
Prognostic factors to state clearly:
- depth and severity grade (more proximal injury means greater loss)
- time to correct rapid rewarming and whether refreezing occurred
- whether the patient reached the salvage window for thrombolysis or iloprost
- bone-scan perfusion in the first days
- smoking, diabetes and peripheral vascular disease
- presence of infection or wet gangrene
With early modern salvage treatment, contemporary series report substantially lower amputation rates than the historical literature, but severe deep injury still carries a real risk of tissue loss.
Guidelines, Registries & Global Practice
Frostbite is globally consistent in its biology but varies in who is affected and what salvage treatment is available. It affects mountaineers and outdoor workers everywhere, but in many settings the largest burden is among homeless, intoxicated and socially vulnerable people. Because it is uncommon there is no large dedicated registry, and authors have repeatedly called for an international frostbite register to pool data; current evidence comes from guidelines, single-centre series and pooled reviews across many countries.
- Emphasis
- Graded evidence-based prevention and treatment pathway
- Practical Point
- Rapid warm-water rewarming, no refreezing, tPA or iloprost for severe early injury, delayed surgery
- Emphasis
- Field decisions, remote consultation and salvage protocols
- Practical Point
- Treat hypothermia first, recognise the early salvage window, use telemedicine for remote cases
- Emphasis
- Iloprost and hyperbaric oxygen for severe frostbite
- Practical Point
- Iloprost is widely used in Europe; hyperbaric oxygen used as an adjunct in selected centres
- Emphasis
- Demarcation-guided delayed amputation
- Practical Point
- Frostbite in January, amputate in July; preserve viable length
High- versus limited-resource practice variation. In well-resourced centres the standard includes rapid controlled rewarming, bone scanning, interventional radiology for thrombolysis, iloprost, hyperbaric oxygen and structured rehabilitation. In limited-resource or remote settings the priorities are correct field care, avoidance of refreezing, prompt evacuation and demarcation-guided surgery, since the advanced salvage drugs and imaging may be unavailable. The most transferable lessons everywhere are to treat hypothermia first, never rewarm if refreezing is possible, rewarm rapidly and correctly when safe, and delay amputation until demarcation.
Documentation that carries value anywhere: the exposure conditions and duration, time of freezing and any thawing or refreezing, time to definitive rewarming, depth and grade of injury, salvage treatment given and its timing, imaging findings, and the rehabilitation and cold-protection plan. Drug choice, thrombolysis protocols and hyperbaric referral should follow local emergency, vascular and interventional-radiology pathways.
Controversies and Areas of Uncertainty
Frostbite is uncommon, so much of the evidence is from small series and there is no single large randomised trial. Several questions remain genuinely open.
Intra-arterial and intravenous thrombolysis both salvage tissue, but the optimal route, dose and the precise time limit are not settled, and tPA carries real bleeding risk that must be weighed in each patient.
Iloprost reduces amputation with no major bleeding risk, but availability, licensing and familiarity vary widely between countries, which affects whether it can be used in practice.
Hyperbaric oxygen appears beneficial as an adjunct to iloprost in small studies, but the evidence is limited and it is not a stand-alone treatment or universally available.
The principle of delaying amputation until demarcation is well established, but the exact timing is judgement-based and must be balanced against the risk of infection in necrotic tissue.
MCQ Practice Points
Q: When should a frostbitten part NOT be rewarmed in the field? A: When there is any risk it will refreeze before definitive care, because a freeze-thaw-refreeze cycle is far more damaging than remaining frozen.
Q: What is the definitive rewarming method? A: Rapid immersion in water at 37 to 39 degrees Celsius with strong analgesia; avoid dry heat and avoid refreezing.
Q: Which patient with bleeding risk and severe early frostbite is best suited to iloprost rather than tPA? A: Iloprost vasodilates and reduces platelet aggregation without major bleeding risk, so it is preferred when thrombolysis is contraindicated.
Q: When should amputation be performed in dry, demarcated frostbite? A: Delayed, after clear demarcation, unless wet gangrene, infection or sepsis force earlier surgery.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A climber descends with hard, white, numb fingers after a night exposed at altitude. He is several hours from definitive care and the temperature is still well below freezing.”
“A homeless man presents 8 hours after cold exposure with both feet hard, insensate and dusky, with early haemorrhagic blisters on several toes after rewarming.”
“Six weeks after frostbite, a patient has dry, blackened, clearly demarcated necrosis of two toes. The surrounding tissue is healthy and there are no signs of infection.”
Recognise
- Freezing cold exposure with white, waxy, hard, numb peripheries.
- Frostbite is a freeze-thaw injury; early appearance under-predicts loss.
- Distinguish from non-freezing cold injury (trench foot).
Field
- Treat hypothermia and major trauma first.
- Do not rewarm if refreezing is possible; avoid rubbing and dry heat.
- Protect the part and evacuate for controlled rewarming.
Hospital
- Rapid rewarming in water at 37 to 39 degrees Celsius with analgesia.
- Ibuprofen, aloe vera, elevation, blister care and tetanus cover.
- Bone scan or angiography to assess perfusion in deep injury.
Salvage
- tPA within about 24 hours to dissolve microvascular thrombosis.
- Iloprost within about 48 hours; preferred if bleeding risk.
- Hyperbaric oxygen as an adjunct in selected centres.
Surgery and Warn
- Delay amputation until demarcation; preserve viable length.
- Operate early only for wet gangrene, infection or sepsis.
- Counsel on cold sensitivity, pain, stiffness and growth-plate risk in children.
Evidence Base
Wilderness Medical Society Clinical Practice Guidelines for Frostbite: 2024 Update
- Recommends rapid rewarming in water at 37 to 39 degrees Celsius and avoidance of any rewarming when refreezing is possible.
- Supports thrombolysis (tPA) and iloprost to reduce amputation in severe deep frostbite presenting early, with ibuprofen and aloe vera as adjuncts.
- Endorses delayed surgery guided by demarcation and imaging rather than early debridement.
A clinical review of the management of frostbite
- Final tissue loss reflects temperature, exposure duration, wind chill, altitude and systemic hypothermia.
- Describes field and hospital management and remote specialist consultation for injuries in austere settings.
- Highlights intravascular thrombolysis and intravenous vasodilators as developments that can reduce loss.