Frykman Classification of Distal Radius Fractures
- Confusing the two joints. Radiocarpal involvement = types III–IV; DRUJ (sigmoid notch) involvement = types V–VI; both = VII–VIII. The DRUJ-only pair (V/VI) is the most-forgotten.
- Forgetting the odd/even rule. Odd = no ulnar styloid; even = styloid present — each odd/even pair is otherwise identical.
- Quoting Frykman as if it guided treatment. It is descriptive, not prognostic, with the worst inter-observer reliability of the common systems (kappa ~0.26) — name it, then add AO/OTA (23-A/B/C) and Fernandez for operative planning.
- Letting the label override the numbers. Displacement, comminution, radial height/inclination, volar tilt and articular step-off (keep under 2 mm) drive management far more than the Frykman type.
- Dismissing the ulnar styloid. An ulnar styloid BASE fracture can disrupt the TFCC foveal insertion and destabilise the DRUJ — assess stability (piano-key/press test, stress views); a tip fracture rarely matters.
The Frykman classification system
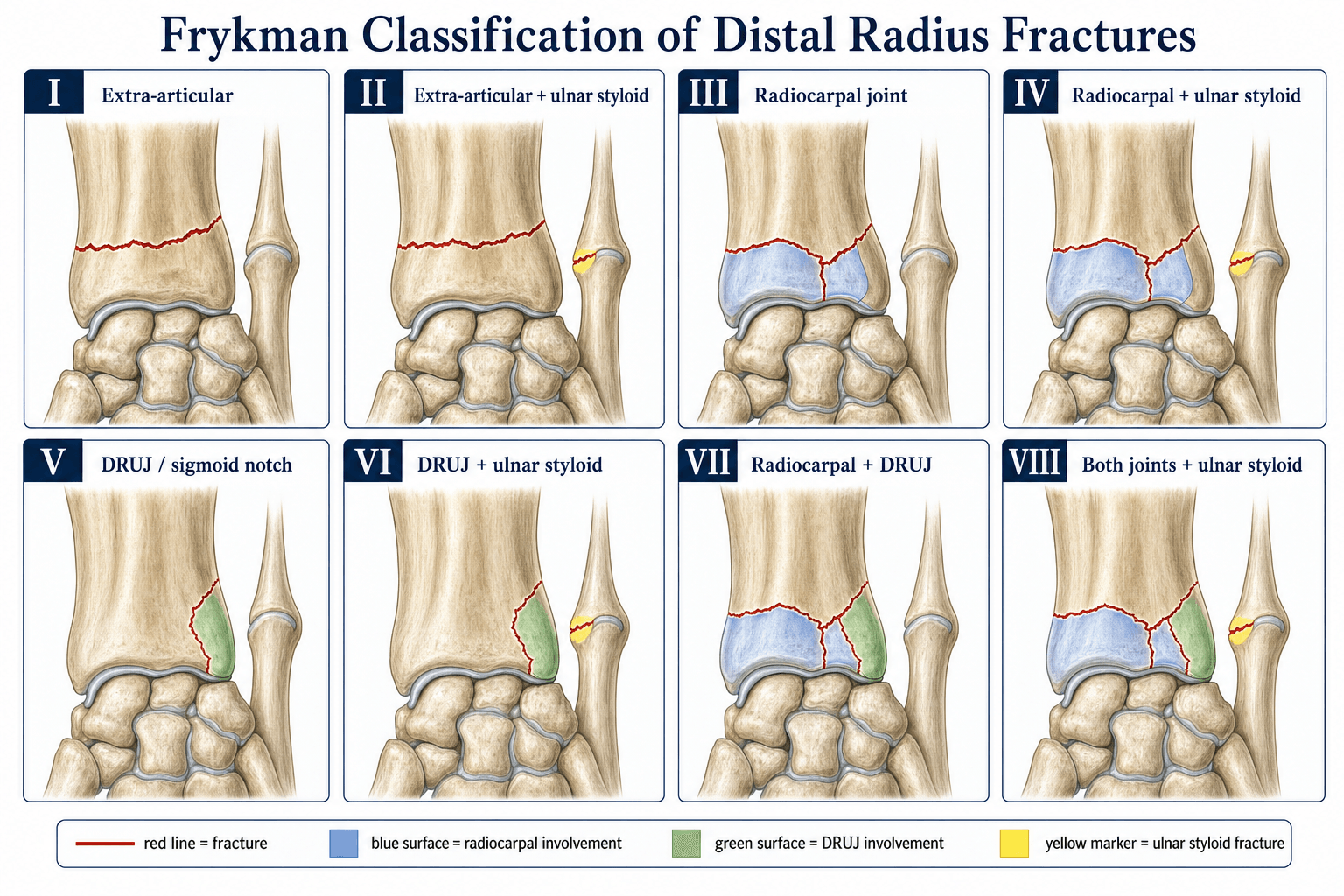

The Frykman classification (1967) divides distal radius fractures into eight types based on two binary questions (radiocarpal joint involvement and DRUJ involvement) and one additional feature (ulnar styloid fracture).

- Radiocarpal joint
- No
- DRUJ
- No
- Ulnar styloid fracture
- No
- Description
- Extra-articular, no ulnar styloid fracture
- Radiocarpal joint
- No
- DRUJ
- No
- Ulnar styloid fracture
- Yes
- Description
- Extra-articular with ulnar styloid fracture
- Radiocarpal joint
- Yes
- DRUJ
- No
- Ulnar styloid fracture
- No
- Description
- Intra-articular into the radiocarpal joint only
- Radiocarpal joint
- Yes
- DRUJ
- No
- Ulnar styloid fracture
- Yes
- Description
- Radiocarpal with ulnar styloid fracture
- Radiocarpal joint
- No
- DRUJ
- Yes
- Ulnar styloid fracture
- No
- Description
- Intra-articular into the DRUJ only
- Radiocarpal joint
- No
- DRUJ
- Yes
- Ulnar styloid fracture
- Yes
- Description
- DRUJ with ulnar styloid fracture
- Radiocarpal joint
- Yes
- DRUJ
- Yes
- Ulnar styloid fracture
- No
- Description
- Intra-articular into both joints
- Radiocarpal joint
- Yes
- DRUJ
- Yes
- Ulnar styloid fracture
- Yes
- Description
- Both joints with ulnar styloid fracture
Odd none, Even extraOdd–even rule for the ulnar styloid
Hook:The ulnar styloid is the toggle between each odd/even pair — odd = none, even = extra (styloid).
Extra → Radio → Ulnar → BothAscending joint involvement
Hook:Joint involvement climbs across the pairs: none, radiocarpal, DRUJ, both.
Types V and VI involve the DRUJ but spare the radiocarpal joint — a fracture running into the sigmoid notch without crossing the dorsal or volar rim into the radiocarpal surface. They are uncommon in practice but examiners love them, precisely because the DRUJ-only pattern is easy to forget.
Frykman is purely descriptive; the examiner pairs it with the classic eponyms, which capture the displacement direction Frykman ignores:
- Colles: an extra-articular distal radius fracture with dorsal angulation/displacement (the "dinner-fork" deformity) — the FOOSH fracture of the osteoporotic elderly, often dorsally comminuted.
- Smith (reverse Colles): volar angulation/displacement (the "garden-spade" deformity), from a fall onto the flexed wrist / dorsum of the hand — inherently unstable.
- Barton: an intra-articular fracture-dislocation/subluxation through the dorsal or volar rim, the carpus displacing with the rim fragment (volar Barton is commoner) — needs a buttress plate.
- Chauffeur's (Hutchinson): an intra-articular radial-styloid avulsion (via the radioscaphocapitate/radial collateral ligaments) — look for an associated scapholunate / perilunate injury.
- Die-punch: depression of the lunate facet (the lunate driven into the articular surface).
Relationship to other classification systems
- Basis
- Intra-articular involvement + ulnar styloid
- Strengths
- Simple; exam-friendly
- Weaknesses
- No displacement, comminution, or mechanism; fair reliability
- Basis
- Extra-articular / partial articular / complete articular (23-A/B/C) + subgroups
- Strengths
- Detailed; better reliability (especially the 3 main types)
- Weaknesses
- Complex; many subgroups
- Basis
- Mechanism (bending, shear, compression, avulsion, combined)
- Strengths
- Links mechanism to treatment; clinically relevant
- Weaknesses
- Requires understanding of force vectors
- Basis
- Extra- vs intra-articular, stable vs unstable
- Strengths
- Practical; guides operative decision
- Weaknesses
- Oversimplifies articular patterns
When asked to classify a distal radius fracture, give the Frykman type if you can, then immediately offer the AO/OTA and Fernandez classifications — this shows breadth and that you understand the limitations of any single system.
Ulnar styloid fracture & DRUJ instability
The presence of an ulnar styloid fracture (even-numbered Frykman types) raises the question of DRUJ instability:
- The TFCC inserts on the fovea at the base of the ulnar styloid — a fracture through or proximal to the foveal base can disrupt this insertion and destabilise the DRUJ.
- Tip (distal) ulnar styloid fractures usually spare the TFCC foveal insertion and rarely cause clinically significant DRUJ instability.
- Assess DRUJ stability clinically (piano-key / press test) and, if uncertain, with stress fluoroscopy or MRI.
- Managing an unstable DRUJ with a distal radius fracture may need ulnar styloid fixation, TFCC repair, or DRUJ pinning in addition to radial fixation.
Do not dismiss an ulnar styloid fracture as incidental. In the context of a distal radius fracture, an ulnar styloid base fracture with DRUJ instability — if unrecognised and untreated — can cause chronic ulnar-sided wrist pain, reduced grip strength, and forearm rotation deficits.
Clinical application & limitations
- Frykman does not account for displacement direction. A volar Barton-type and a dorsal Colles-type can both be type III if the radiocarpal joint is involved, yet differ substantially in management and prognosis.
- Comminution and metaphyseal fragmentation are ignored. A highly comminuted extra-articular fracture (Frykman I) may be harder to manage than a minimally displaced radiocarpal fracture (Frykman III).
- Inter-observer reliability is only fair-to-moderate. Reliability studies (Andersen et al., Belloti et al., Ploegmakers et al.) place Frykman in the fair range and below the AO/OTA system, especially on inter-observer testing.
- Prognostic value is limited. Frykman type alone does not reliably predict functional outcome, post-traumatic arthritis, or the need for fixation; higher types correlate only loosely with higher-energy injury.
- It remains a useful communication shorthand and an exam staple, but most trauma surgeons use AO/OTA (23-A/B/C) or Fernandez for operative decisions.
The classification label matters far less than the measurements — know the normal values and how the acceptability thresholds derive from them:
- Radial inclination (PA): normal ~22° (about 21 to 25°).
- Radial height/length (PA): normal ~11 to 12 mm (radial styloid tip to the ulnar corner of the distal radius).
- Volar (palmar) tilt (lateral): normal ~11° (about 10 to 12°).
- Ulnar variance: normal ~neutral (within about ±2 mm).
- Acceptable reduction / operative triggers (the parameters this topic cites): dorsal angulation more than ~10° (loss of volar tilt past neutral), radial shortening more than ~3 mm, radial inclination loss past ~5°, and an intra-articular step-off of 2 mm or more — these, not the Frykman type, drive the decision to fix.
Guidelines, registries & global practice
- AAOS distal radius CPG: does not mandate any single classification; emphasises that radiographic parameters (dorsal angulation over 10°, radial shortening over 3 mm, articular step-off over 2 mm) should guide operative management regardless of classification label.
- AO Foundation: the AO classification (23-A/B/C) is preferred in AO teaching and the AO Surgery Reference; Frykman is acknowledged historically but not used in AO treatment algorithms.
- BSSH / BOA (UK): UK trauma units use AO/OTA; Frykman appears in FRCS exam preparation but is not referenced in BOAST distal radius guidance.
- Fernandez classification: widely used in European and South American centres for its mechanism-based link between injury pattern and surgical strategy.
- Epidemiology: distal radius fractures are the commonest adult fracture, with a bimodal distribution (young high-energy males, older osteoporotic females); the operative proportion of displaced fractures has risen with volar locking-plate adoption. (Distal radius fractures are not tracked in arthroplasty registries.)
Viva practice
Exam viva
Practise clinical reasoning and management decisions out loud
“A 58-year-old woman falls on an outstretched hand. Radiographs show a dorsally displaced, comminuted fracture of the distal radius with a fracture line entering the radiocarpal joint and a fracture of the ulnar styloid base. Classify this fracture.”
“A 42-year-old man sustains a high-energy fall. Radiographs show a severely comminuted distal radius fracture with involvement of both the radiocarpal joint and the sigmoid notch (DRUJ), with an ulnar styloid fracture. How do you classify and manage this fracture?”
Exam cheat sheet
2-by-4The eight types in one frame
Hook:Four pairs (extra, radiocarpal, DRUJ, both); the even member of each pair adds the ulnar styloid fracture.
- Eight types from radiocarpal ± DRUJ ± ulnar styloid; odd = no styloid, even = styloid; involvement climbs none → radiocarpal → DRUJ → both.
- Types V/VI = DRUJ only (radiocarpal spared) — the easily-forgotten pair.
- Frykman is descriptive, not prognostic, with only fair reliability — supplement with AO/OTA and Fernandez.
- Articular step-off (under 2 mm), radial height, inclination and volar tilt matter more than the classification label.
- An ulnar styloid BASE fracture flags possible TFCC disruption/DRUJ instability — assess it (piano-key test, stress views).
The eight types (memorise the pattern)
- I extra-articular, no styloid — II extra-articular, with styloid
- III radiocarpal only, no styloid — IV radiocarpal only, with styloid
- V DRUJ only, no styloid — VI DRUJ only, with styloid
- VII both joints, no styloid — VIII both joints, with styloid
Odd–even rule
- Odd = no ulnar styloid fracture (I, III, V, VII)
- Even = ulnar styloid fracture present (II, IV, VI, VIII)
- Joint involvement escalates: none → radiocarpal → DRUJ → both
Key exam talking points
- Frykman is descriptive, not prognostic — only fair inter-observer reliability
- Supplement with AO/OTA (23-A/B/C) and Fernandez (mechanism) for operative planning
- Ulnar styloid base fracture = possible TFCC disruption and DRUJ instability — assess it
- Articular reduction quality (step-off under 2 mm) matters more than the classification label
Evidence Base
Fracture of the distal radius including sequelae — shoulder-hand-finger syndrome, disturbance in the distal radio-ulnar joint and impairment of nerve function. A clinical and experimental study
- Introduced the eight-type classification based on radiocarpal and DRUJ involvement and the presence of an ulnar styloid fracture.
- Associated DRUJ disturbance and ulnar-sided injury with worse sequelae of distal radius fractures.
- Established the ascending pattern of joint involvement (extra-articular → radiocarpal → DRUJ → both) still taught today.
According to PubMed, the eight-type system comes from Frykman 1967 (DOI); the fair-to-moderate, AO-inferior reliability from Andersen et al. 1996 (DOI), Belloti et al. 2008 (DOI; Frykman inter-observer kappa 0.26) and Ploegmakers et al. 2007 (DOI); and the ulnar-styloid/DRUJ-instability link from May et al. 2002 (DOI). The AO/OTA and Fernandez systems and the radiographic acceptability parameters are standard distal-radius teaching.