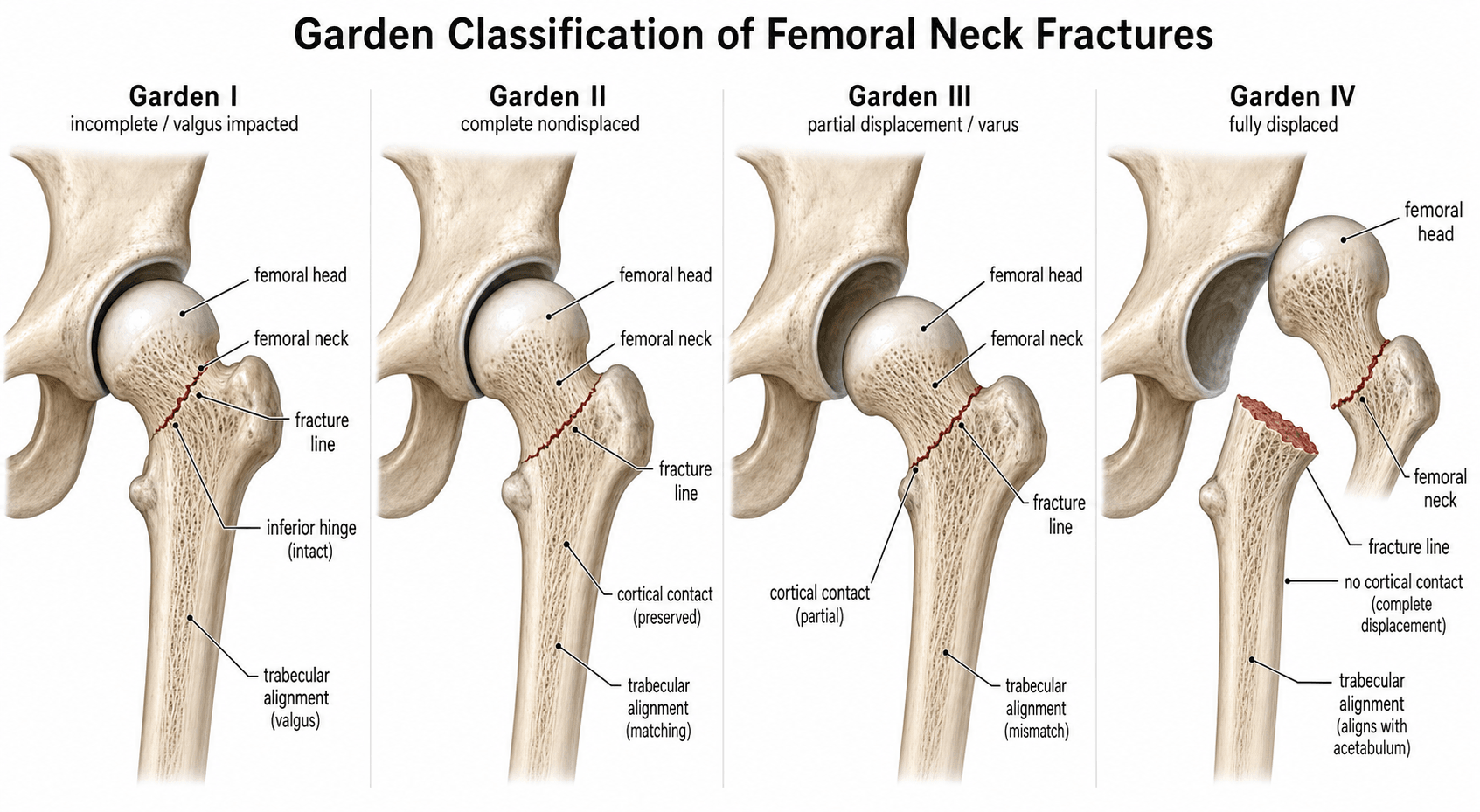
Garden Classification of Femoral Neck Fractures
The Garden system is the standard language for intracapsular neck of femur fractures, but inter-observer reliability is only moderate for the four-type version. In practice and in most exam answers, fractures are dichotomised into undisplaced (Garden I-II) versus displaced (Garden III-IV) because this binary split drives treatment and has better reproducibility. Always state both the full Garden type and the clinical dichotomy when describing a fracture.
The Garden Classification System

The Garden classification is based on the appearance of the femoral head and neck on the anteroposterior radiograph. It describes the position of the capital fragment relative to the acetabulum and the degree of cortical continuity.
- Description
- Valgus-impacted or incomplete
- Key Radiographic Signs
- Head tilted into valgus on neck; trabeculae still aligned or slightly impacted; cortical break incomplete
- Displacement Status
- Undisplaced
- Description
- Complete but undisplaced
- Key Radiographic Signs
- Full fracture line visible across neck; head and neck remain aligned; no varus or valgus tilt
- Displacement Status
- Undisplaced
- Description
- Partially displaced
- Key Radiographic Signs
- Head tilted into varus; partial cortical contact remains; fracture line oblique
- Displacement Status
- Displaced
- Description
- Fully displaced
- Key Radiographic Signs
- No cortical contact; head free in acetabulum or rotated; shaft displaced proximally and externally rotated
- Displacement Status
- Displaced
Incomplete • Complete • Partial • FreeGarden I to IV progression
Hook:Incomplete → Complete → Partial → Free: the higher the Garden number, the greater the displacement and the higher the risk of losing the femoral-head blood supply.
The critical distinction is between undisplaced (I-II) and displaced (III-IV). Undisplaced fractures preserve the retinacular blood supply far better; once displacement occurs the superior retinacular vessels are at risk and avascular necrosis becomes a real threat.
The reason an intracapsular fracture threatens the head is the femoral-head blood supply, which examiners expect you to describe:
- The dominant supply is the deep branch of the medial femoral circumflex artery (MFCA), which gives rise to the lateral epiphyseal / retinacular vessels — chiefly the posterosuperior retinacular vessels (in the retinacula of Weitbrecht) that ascend the femoral neck beneath the synovium to enter the head.
- The lateral femoral circumflex artery supplies the anterior/inferior neck and head (lesser contribution), and the artery of the ligamentum teres (from the obturator/MFCA) supplies only a small medial epiphyseal area — minor and variable in adults, so it cannot save a head deprived of its retinacular supply.
- A displaced intracapsular fracture tears the ascending retinacular vessels, and the intracapsular haematoma raises intracapsular pressure (tamponade) further compromising perfusion — the dual mechanism behind the AVN risk rising from roughly 10% (undisplaced) to 20-30% (displaced), and the rationale some cite for urgent reduction (± capsular decompression) in the young.
Garden Types and Management Implications
Management decisions are driven by patient age, comorbidities, fracture displacement and the viability of the femoral head.
- Patient Group
- Any age
- Preferred Treatment
- Internal fixation — cannulated screws or sliding hip screw
- Key Considerations
- Preserve the head; low AVN risk; allow early mobilisation
- Patient Group
- Young, fit (under about 60-65 years)
- Preferred Treatment
- Urgent closed or open reduction and internal fixation
- Key Considerations
- Aim for prompt anatomical reduction; higher AVN risk; preserve the native head
- Patient Group
- Older, frail (over about 75-80 years)
- Preferred Treatment
- Cemented hemiarthroplasty or total hip arthroplasty
- Key Considerations
- Avoid prolonged surgery; allow immediate full weight-bearing; lower re-operation rate than fixation

In a young patient with a displaced Garden III or IV fracture, treat it as a surgical priority: obtain a prompt, ANATOMICAL reduction (closed or open), compress the fracture, and protect the reduction with a sliding hip screw or cannulated screws in an inverted-triangle configuration. Quality of reduction is the factor most clearly linked to outcome; while early surgery is widely recommended, the evidence that each hour of delay independently raises avascular necrosis is debated, so do not accept a poor reduction simply to operate faster.
Undisplaced fix • Displaced young reduce • Displaced old replaceTreatment by displacement
Hook:Undisplaced → fix; Displaced young → reduce + fix; Displaced old → replace.
"Arthroplasty in the elderly" needs the contemporary detail examiners now expect:
- Hemiarthroplasty vs total hip arthroplasty: reserve THA for the more active, independent, cognitively intact older patient (e.g. mobilises with no more than a stick, not cognitively impaired, medically fit — the NICE criteria) and especially with acetabular cartilage wear/arthritis — THA gives better function but higher dislocation; hemiarthroplasty suits the less mobile/frailer patient. The HEALTH trial found no significant difference in secondary hip procedures between THA and hemiarthroplasty at 2 years, with modestly better function favouring THA.
- Cemented over uncemented stems: a cemented stem is preferred (NICE) because uncemented stems carry a higher periprosthetic-fracture rate in the osteoporotic elderly (balance against the rare bone-cement implantation syndrome).
- Fixation construct (when fixing): the FAITH trial found no overall reoperation difference between a sliding hip screw and multiple cancellous screws, but the SHS was favoured in current smokers, basicervical fractures and displaced fractures.
- The undisplaced caveat: even a "Garden I-II" fracture in the elderly with marked posterior tilt (over ~20° on the lateral) has a high fixation-failure rate and may be better served by arthroplasty — displacement on the AP is not the whole story.
Limitations and Reliability
- The four-type Garden system has only moderate inter-observer reliability; many surgeons cannot consistently distinguish Type II from Type III on plain radiographs.
- The binary split into undisplaced versus displaced is far more reproducible and is what most guidelines and registries actually use for outcome reporting.
- Garden does not account for posterior comminution, which is visible on the lateral radiograph and increases the risk of fixation failure.
- The classification is purely radiographic and does not incorporate patient factors such as bone quality, comorbidities or time to presentation.
- Modern CT and MRI can detect occult Garden I fractures and assess femoral head perfusion, but the Garden label itself remains a plain-film tool.
- Garden is a displacement system; the Pauwels classification is its companion. Pauwels grades the fracture by the angle of the fracture line to the horizontal (I under 30°, II 30–50°, III over 50°), which estimates the shear across the fracture: the more vertical the line (Pauwels III), the greater the shear and the higher the risk of non-union and fixation failure. Pauwels is most useful in the young patient with a vertical fracture, where it guides the choice of a more shear-resistant construct (e.g. a fixed-angle device or the addition of a buttress); Garden and Pauwels are quoted together for these injuries.
- AO/OTA classifications exist but, on reliability testing, are no better than Garden (and the 2018 revision performed worse), so Garden remains the everyday language despite its limitations.
Exam Viva
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman falls at home and sustains a left femoral neck fracture. The anteroposterior radiograph shows a complete fracture line with the head tilted into slight varus and partial cortical contact. What is the Garden classification and how would you manage her?”
“A 52-year-old man is brought in after a high-energy road-traffic collision. He has a displaced femoral neck fracture that you classify as Garden IV. Outline your operative plan and the key discussion points for consent.”
The four Garden types
- Type I: valgus-impacted or incomplete — head tilted into valgus, trabeculae aligned
- Type II: complete but undisplaced — full fracture line visible, head and neck aligned
- Type III: partially displaced — varus tilt, some cortical contact remains
- Type IV: fully displaced — no cortical contact, head free or rotated
Clinical dichotomy that actually matters
- Undisplaced (Garden I-II): fix with screws or sliding hip screw in almost all patients
- Displaced (Garden III-IV): young patient — urgent reduction and fixation; older patient — arthroplasty
- Displacement increases AVN risk from under 10 percent to 20-30 percent
- Always obtain and review the lateral radiograph for posterior comminution
Key exam points and pitfalls
- Reliability is moderate for four types; excellent for the binary undisplaced versus displaced split
- Garden does not replace clinical judgement — bone quality, comorbidities and time since injury all matter
- In young patients with displaced fractures, document the time of injury and aim for theatre within 6-12 hours
- Posterior comminution on the lateral view predicts loss of reduction even if the anteroposterior view looks acceptable
Evidence Base
All four citations were verified against PubMed and they tell one coherent story. Three independent reliability studies (Thomsen 1996, Cai 2022, Cazzato 2022) consistently show the four-type Garden system is only moderately reproducible (full agreement on ~15% of cases; kappa ~0.39–0.49), with Stage II vs III the weak point — but the undisplaced-vs-displaced dichotomy is highly reliable (kappa ~0.68–0.90). Cai goes further, suggesting truly incomplete (Garden I) fractures may not exist in osteoporotic bone (all "Garden I" were complete at surgery). The treatment limb rests on the Parker/Gurusamy Cochrane review: for displaced fractures, internal fixation has less operative trauma but a markedly higher re-operation rate than arthroplasty — the evidence behind replacing (not fixing) the displaced fracture in the elderly. Net: classify with the binary split, and let age/physiology and the Cochrane evidence drive fix-versus-replace.
Observer variation in the radiographic classification of fractures of the neck of the femur using Garden's system
- Six observers classified 96 femoral-neck fractures; all six agreed on only 14 (15%)
- Poor agreement for the full four-type system (kappa 0.39), becoming acceptable when reduced to undisplaced (I-II) versus displaced (III-IV) (kappa 0.68)
- Distinguishing Stage II from Stage III remained problematic
Internal fixation versus arthroplasty for intracapsular proximal femoral fractures in adults
- Meta-analysis of 17 randomised trials (2694 participants) comparing internal fixation with arthroplasty for intracapsular hip fractures
- Internal fixation had less operative trauma (shorter surgery, less blood loss/transfusion, lower deep infection) but a significantly higher re-operation rate
- Arthroplasty had a lower re-operation rate; limited data suggested a cemented arthroplasty gave less pain and better function than fixation
Does Garden type I incomplete femoral neck fracture really exist in older adults? To evaluate the stability and consistency of Garden classification.
- Garden classification shows only moderate inter-observer reliability even among experienced surgeons
- Many apparent Garden I fractures are complete on CT, questioning the existence of truly incomplete fractures in osteoporotic bone
- Simplifying to undisplaced versus displaced improves both reliability and clinical utility
Femoral neck fracture: the reliability of radiologic classifications.
- Six surgeons classified 150 femoral-neck fractures using Garden, 2018 AO/OTA and simplified AO/OTA systems
- Garden had only fair-to-moderate interobserver reliability (kappa 0.28-0.73, mean 0.49); the 2018 AO/OTA was worse (mean 0.30) and the simplified AO/OTA similar to Garden (mean 0.48)
- No classification was superior, and greater surgeon experience did not improve reliability