Benign Tendon Sheath Lesion | Most Common Hand Tumor | Same Disease as PVNS
GCTTS Classification
Critical Must-Knows
- GCTTS is the extra-articular form of TGCT - same pathology as PVNS, different location
- Second most common hand tumor after ganglion cyst (accounts for 10% of hand masses)
- CSF1-COL6A3 fusion drives pathogenesis - same molecular driver as PVNS
- Recurrence 10-20% due to incomplete excision or diffuse infiltrative type
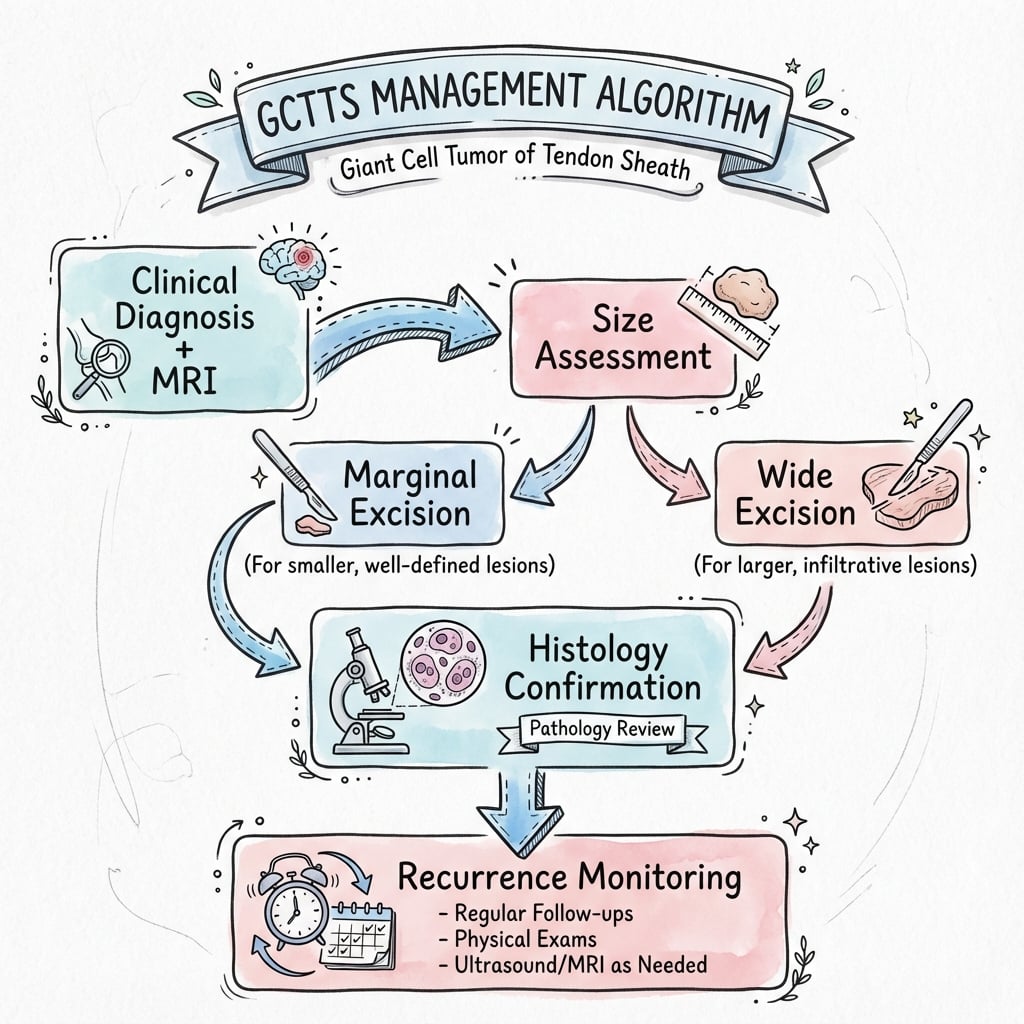
- Treatment: Complete marginal excision with intact capsule - avoid fragmentation
Clinical Pearls
- "GCTTS equals PVNS extra-articularly - same histology (hemosiderin, giant cells)
- "Classic location: Volar aspect of digits (index and middle finger most common)
- "MRI shows low signal on T1 and T2 (hemosiderin) - same as PVNS blooming
- "Key to prevent recurrence: Excise with intact capsule, inspect for satellite lesions
Clinical Imaging
Imaging Gallery

Critical GCTTS Exam Points
Relationship to PVNS
GCTTS equals TGCT extra-articularly. Intra-articular location equals PVNS. Extra-articular (tendon sheath) equals GCTTS. Same pathological process (CSF1-driven), different anatomical location.
Location Pattern
Volar digits (index, middle finger). Over 50% occur in hand, most on volar aspect of digits. Attaches to flexor tendon sheath. Rarely involves extensor side.
Surgical Principle
Excise with intact capsule. Fragmentation or incomplete excision increases recurrence from 10% to over 30%. Inspect for satellite lesions. Protect digital neurovascular bundles.
Recurrence Risk
10-20% recurrence overall. Diffuse type recurs more (30-40%) than localized. Recurrence peaks at 1-2 years. Re-excision is treatment for recurrence.
Quick Decision Guide - GCTTS Management
| Presentation | Type | Treatment | Key Pearl |
|---|---|---|---|
| Painless nodule, volar digit, slow-growing, no trauma | Localized GCTTS | Marginal excision with intact capsule | Recurrence 10-15% if complete excision |
| Infiltrative mass, wraps around structures, bone erosion | Diffuse GCTTS | Wide excision with margins | Higher recurrence (30-40%) - need wide margins |
| Recurrent mass after previous excision | Recurrent GCTTS | Re-excision + search for satellite lesions | Inspect prior surgical field for incomplete excision |
GIANTGCTTS Pathological Features
| G | Giant cells (multinucleated) Histological hallmark - reactive, not neoplastic |
| I | Iron (hemosiderin) Pigment deposition causes dark color grossly |
| A | Attached to tendon sheath Arises from tendon sheath, not tendon itself |
| N | Nodular mass Well-circumscribed lobulated appearance |
| T | Tan-yellow color Gross pathology - tan to yellow-brown (xanthoma cells) |
| G | Giant cells (multinucleated) Histological hallmark - reactive, not neoplastic | N | Nodular mass Well-circumscribed lobulated appearance |
| I | Iron (hemosiderin) Pigment deposition causes dark color grossly | T | Tan-yellow color Gross pathology - tan to yellow-brown (xanthoma cells) |
| A | Attached to tendon sheath Arises from tendon sheath, not tendon itself |
Hook:GIANT cells + iron = the pathology of GCTTS, a GIANT among hand tumors!
HANDGCTTS Clinical Features
| H | Hand location (75%) Volar aspect of index and middle fingers most common |
| A | Asymptomatic (painless) Slow-growing painless mass, incidental finding |
| N | Neurovascular proximity Close to digital nerves and vessels - protect during excision |
| D | Discrete nodule Well-defined lobulated mass on tendon sheath |
| H | Hand location (75%) Volar aspect of index and middle fingers most common | N | Neurovascular proximity Close to digital nerves and vessels - protect during excision |
| A | Asymptomatic (painless) Slow-growing painless mass, incidental finding | D | Discrete nodule Well-defined lobulated mass on tendon sheath |
Hook:GCTTS loves the HAND - remember the key clinical features!
RECURRecurrence Risk Factors
| R | Residual disease Incomplete excision leaves microscopic tumor |
| E | Extensive (diffuse) type Infiltrative growth pattern wraps around structures |
| C | Capsule rupture Fragmentation during surgery seeds recurrence |
| U | Under-excision Not removing satellite lesions |
| R | Revision surgery Recurrent lesions harder to excise completely |
| R | Residual disease Incomplete excision leaves microscopic tumor | U | Under-excision Not removing satellite lesions |
| E | Extensive (diffuse) type Infiltrative growth pattern wraps around structures | R | Revision surgery Recurrent lesions harder to excise completely |
| C | Capsule rupture Fragmentation during surgery seeds recurrence |
Hook:Prevent RECURRENCE by complete excision with intact capsule!
Overview and Epidemiology
Why GCTTS Matters Clinically
Giant cell tumor of tendon sheath (GCTTS) is the second most common hand tumor after ganglion cyst, accounting for approximately 10% of all hand masses. It is the extra-articular manifestation of tenosynovial giant cell tumor (TGCT) - the same pathological process as PVNS, but arising from tendon sheath rather than joint synovium. Despite being benign, GCTTS causes functional impairment due to mass effect and can erode adjacent bone. Recurrence occurs in 10-20% of cases, primarily due to incomplete excision.
Demographics
- Age: Peak incidence 30-50 years (adults)
- Gender: Female predominance 2:1
- Location: Hand and wrist 75%, foot 20%, other 5%
- Laterality: No dominant hand preference
Clinical Impact
- Functional impairment: Mass effect limits finger motion
- Bone erosion: Pressure erosion of phalanx (20-30% of cases)
- Recurrence: 10-20% overall (higher for diffuse type)
- Neurovascular risk: Close proximity to digital neurovascular bundles
The classic patient is a middle-aged woman with a painless slow-growing nodule on the volar aspect of a digit.
Pathophysiology and Molecular Biology
GCTTS is Not a True Neoplasm - It's a Reactive Proliferation
Despite the name "tumor", GCTTS is a clonal proliferative disorder driven by CSF1-COL6A3 fusion (same as PVNS). Mononuclear stromal cells express CSF1, which recruits inflammatory cells (macrophages, giant cells) via CSF1R. The giant cells are reactive (not neoplastic) - the neoplastic component is the mononuclear stromal cells.
| Feature | Mechanism | Clinical Consequence |
|---|---|---|
| CSF1-COL6A3 fusion | Chromosomal translocation drives CSF1 overexpression | Clonal proliferation of stromal cells |
| CSF1R activation | Macrophages recruited by CSF1 via CSF1R binding | Inflammatory infiltrate creates mass |
| Hemosiderin deposition | Recurrent microhemorrhage into lesion | MRI low signal (blooming), gross dark color |
| Pressure erosion | Mass compresses adjacent bone | Cortical scalloping or erosion of phalanx |
Histopathology
- Multinucleated giant cells: Hallmark (but reactive)
- Mononuclear stromal cells: Neoplastic component (CSF1 expressing)
- Hemosiderin-laden macrophages: From microhemorrhage
- Xanthoma (foam) cells: Lipid-laden macrophages (yellow color)
- Capsule: Usually well-encapsulated (localized type)
Differential Histology
- vs PVNS: Same histology, different location (joint vs tendon sheath)
- vs Ganglion: No giant cells, mucinous cyst contents
- vs Fibroma: No giant cells or hemosiderin
- vs Giant cell tumor of bone: Different location, more aggressive
The key pathological distinction is localized (well-encapsulated) versus diffuse (infiltrative) types.
Classification and Clinical Forms
Localized GCTTS (90% of cases)
Clinical Features:
- Well-circumscribed lobulated nodule
- Arises from tendon sheath (usually flexor)
- Firm, rubbery, mobile mass
- Painless (unless compressing nerve)
- Slow growth over months to years
Imaging:
- MRI: Low signal T1 and T2, well-defined margins
- May show blooming on GRE sequences (hemosiderin)
- No soft tissue invasion
Treatment:
- Marginal excision with intact capsule
- Low recurrence (10-15%) if complete excision
Localized GCTTS has excellent prognosis with complete excision.
Localized vs Diffuse - Treatment and Prognosis Distinction
The critical exam point: Localized GCTTS (90% of cases) has well-defined margins and low recurrence (10-15%) with marginal excision. Diffuse GCTTS (10% of cases) has infiltrative growth, is difficult to excise completely, and recurs in 30-40% despite wide margins. This distinction guides surgical approach and patient counseling.
Clinical Presentation and Assessment
History
- Mass: Painless slow-growing nodule (months to years)
- Location: Volar digit (index and middle finger most common)
- Symptoms: Usually asymptomatic, mass effect only
- Pain: Rare unless nerve compression or joint involvement
- Trauma: No history of trauma (helps differentiate from other lesions)
Examination
- Inspection: Visible lobulated mass, skin intact
- Palpation: Firm, rubbery, well-defined, mobile on tendon sheath
- Range of motion: May be limited by mass effect
- Neurovascular: Usually intact (but mass may compress nerve)
- Transillumination: Negative (solid, not cystic like ganglion)
GCTTS vs Ganglion Cyst - Key Clinical Distinction
Key differentiating features: Ganglion cyst transilluminates (fluid-filled), is softer/fluctuant, and often arises from joint or tendon sheath near joint. GCTTS does NOT transilluminate (solid), is firm/rubbery, and can occur anywhere along tendon sheath. Both are common hand masses - clinical exam and MRI differentiate.
Location Distribution:
- Hand (75%): Index and middle fingers most common, volar aspect
- Wrist (5%): Flexor or extensor tendon sheaths
- Foot (20%): Toes and plantar aspect
- Other (under 5%): Ankle, knee (rare)
The classic presentation is painless volar digit mass that does not transilluminate.
Imaging and Diagnosis
Diagnostic Imaging Protocol
Initial assessment: Rule out bone lesion (giant cell tumor of bone), assess for pressure erosion.
Key findings:
- Usually normal (soft tissue mass)
- Cortical scalloping or erosion of adjacent phalanx (20-30%)
- No matrix calcification (unlike chondroma)
- Preserved joint space
Diagnostic MRI features: Low signal on T1 and T2 weighted sequences due to hemosiderin. Blooming artifact on GRE sequences (same as PVNS).
Sensitivity: Over 90% for GCTTS diagnosis when low signal present.
Key findings:
- Well-defined margins (localized) or infiltrative (diffuse)
- Low signal T1 and T2 (hemosiderin)
- Blooming on GRE sequences
- Relationship to neurovascular structures (surgical planning)
Appearance: Solid hypoechoic mass attached to tendon sheath
Role: Differentiate from ganglion (cystic), assess vascularity
Limitation: Cannot assess bone erosion or deep extent
Indications: Atypical imaging, need to exclude malignancy
Approach: Excisional biopsy (preferred for small lesions) or incisional biopsy for large masses
Histology confirms: Giant cells, hemosiderin, mononuclear stromal cells
MRI Low Signal - Characteristic Finding
Q: What is the characteristic MRI appearance of GCTTS? A: Low signal on both T1 and T2 weighted sequences - caused by hemosiderin (iron) deposition. Blooming artifact on gradient echo (GRE) sequences is also characteristic (same as PVNS). This low signal helps differentiate GCTTS from other hand masses like ganglion (high signal T2) or fibroma (intermediate signal).
Differential Diagnosis
GCTTS Differential Diagnosis
| Condition | Key Distinguishing Features | Imaging Differences |
|---|---|---|
| Ganglion cyst | Most common hand mass, cystic, transilluminates, fluctuant | High signal T2, fluid on US, near joint |
| Fibroma of tendon sheath | Firm solid mass, no hemosiderin, benign | Intermediate signal T1/T2, no blooming |
| Glomus tumor | Subungual location, exquisitely tender, pulsatile pain | High signal T2, intense enhancement, nail bed |
| Epithelioid sarcoma | MALIGNANT, painless mass, ulceration, young adults | Heterogeneous signal, invasion, lymph nodes |
| Giant cell tumor of bone | Bone origin (not soft tissue), aggressive lytic lesion | Lytic bone lesion, cortical breakthrough |
The critical distinction is benign (GCTTS, ganglion, fibroma) versus malignant (epithelioid sarcoma) - biopsy if any concern for malignancy.
Management Algorithm
Localized GCTTS Management
Goal: Complete marginal excision with intact capsule to minimize recurrence.
Treatment Steps
Imaging review: MRI to assess extent, relationship to neurovascular structures
Consent: Recurrence risk (10-15%), neurovascular injury risk, stiffness
Anesthesia: Local with sedation or regional block (Bier block, axillary block)
Approach: Volar or dorsal incision based on mass location
Technique:
- Identify and protect digital neurovascular bundles (Bruner incision for volar)
- Dissect capsule from surrounding structures
- Excise with intact capsule (avoid fragmentation)
- Inspect for satellite lesions
- Check for bone erosion (curettage if present)
Closure: Skin only (no drain needed), splint for comfort
- Early range of motion (3-5 days) to prevent stiffness
- Hand therapy for rehabilitation
- Splint for comfort (not mandatory)
- Return to work at 2-4 weeks
Protocol: Clinical exam at 6 and 12 months
Recurrence: Usually within 2 years if occurs
Re-excision: Treatment for recurrence
Localized GCTTS has excellent prognosis with complete excision.
Complete Excision with Intact Capsule - Key to Prevent Recurrence
The single most important technical factor to prevent recurrence is excision with intact capsule without tumor fragmentation. Rupture of the capsule or piecemeal excision seeds the surgical field with tumor cells and increases recurrence from 10-15% to over 30%. Inspect for satellite lesions (small nodules near main mass) which also contribute to recurrence.
Surgical Technique - Volar Digit Excision
Patient Positioning and Setup
Setup Checklist
Supine with arm on hand table.
- Tourniquet on upper arm
- Hand supinated on sterile hand table
- Magnification (loupes or microscope) for neurovascular protection
- Local with sedation (small lesions)
- Regional block (Bier block, axillary) for larger lesions
- General anesthesia rarely needed
- Tourniquet (exsanguinate with Esmarch)
- Loupes or microscope
- Fine instruments for neurovascular dissection
Standard hand surgery positioning.
Complications of GCTTS and Treatment
| Complication | Incidence/Risk Factors | Prevention/Management |
|---|---|---|
| Recurrence (most common) | 10-20% overall (higher for diffuse type, incomplete excision) | Complete excision with intact capsule, remove satellites |
| Digital nerve injury | Nerve adherent to tumor capsule, iatrogenic during dissection | Magnification, meticulous technique, identify nerves early |
| Digital artery injury | Vessel adherent to capsule, risk during excision | Identify vessels, protect with vessel loops, bipolar cautery |
| Stiffness | Prolonged immobilization, adhesions | Early range of motion (3-5 days), hand therapy |
| Wound infection | Low risk (under 2%), contamination | Sterile technique, perioperative antibiotics if indicated |
Neurovascular Injury - Key Surgical Risk
Digital neurovascular bundles are immediately adjacent to GCTTS on volar digits. The tumor capsule may be adherent to nerve or artery. Use magnification (loupes or microscope), identify neurovascular structures early, and dissect meticulously. Nerve injury causes permanent numbness. Artery injury requires repair or risks digit ischemia.
The major complication is recurrence, driven by incomplete excision or diffuse type.
Postoperative Care and Rehabilitation
Postoperative Rehabilitation Protocol
- Bulky dressing and volar splint
- Elevation to reduce swelling
- Pain control (oral analgesics)
- Remove splint at day 3-5
- Early active ROM to prevent stiffness
- Continue elevation between exercises
- Light activities of daily living (no lifting)
- Remove sutures at 10-14 days
- Progressive strengthening exercises
- Hand therapy for scar massage, edema control
- Return to unrestricted activities at 4-6 weeks
- Clinical exam at 6 and 12 months
- MRI if recurrence suspected (palpable mass)
- Most recurrences occur within 2 years
Early range of motion is critical to prevent finger stiffness after hand surgery.
Recurrence and Outcomes
| Factor | Recurrence Risk | Management Strategy |
|---|---|---|
| Localized type, complete excision | 10-15% | Standard marginal excision, clinical surveillance |
| Incomplete excision or capsule rupture | over 30% | Re-excision if recurrence detected early |
| Diffuse type | 30-40% | Wide excision, consider adjuvant if unresectable recurrence |
Management of Recurrent GCTTS
First recurrence: Re-excision with wider margins, search for satellite lesions that were missed during initial surgery. Multiple recurrences: Consider adjuvant radiation (20 Gy) for unresectable disease, or CSF1R inhibitor (pexidartinib off-label) for extensive recurrent disease. Most recurrences occur within 2 years - long surveillance important.
Overall outcomes are excellent with low complication rates and high function restoration if excision is complete.
Controversies and Areas of Uncertainty
Role of Adjuvant Radiotherapy
Low-dose external beam radiotherapy is proposed for diffuse or repeatedly recurrent disease, but evidence is limited to small series. Benefit must be weighed against radiation morbidity in the hand (skin, joint stiffness, theoretical late malignancy). Most authors reserve it for unresectable recurrence rather than primary use.
Timing and Place of Pexidartinib
ENLIVEN proved efficacy in advanced TGCT, but the trial was dominated by large-joint diffuse disease, hepatotoxicity is significant, and there is no EMA approval. Its role in digital GCTTS is off-label and confined to recurrent disease not amenable to surgery.
How Wide is 'Wide Enough'?
Positive margins are the strongest predictor of recurrence, yet aggressive margins in the digit threaten nerves, vessels and tendons. The optimal balance between oncological clearance and functional preservation for diffuse digital disease remains undefined.
Value of Routine Postoperative MRI
Surveillance is usually clinical, with MRI reserved for suspected recurrence. Whether routine imaging detects recurrence earlier and improves outcomes (versus added cost and false positives) is unsettled.
The recurring theme is that GCTTS is biologically benign but locally tenacious - the controversies all centre on how aggressively to treat a non-lethal disease without harming hand function.
Evidence Base and Key Studies
CSF1 Translocation Defines GCTTS/PVNS (Landmark)
- Translocations involving chromosome 1p13 present in the majority of TGCT and PVNS cases
- CSF1 is the gene at the 1p13 breakpoint, fused to COL6A3 (2q35) in some cases
- Translocation present in only a MINORITY of intratumoral cells, driving CSF1 overexpression
- Most cells express CSF1R but not CSF1 - a 'tumour-landscaping' effect recruits non-neoplastic cells into the mass
CSF1 Overexpression Across PVNS/TGCT Spectrum
- 60 TGCT/PVNS patients studied by in situ hybridisation and immunohistochemistry
- CSF1 translocation plus high CSF1 RNA in 61% (35/57); high CSF1 expression WITHOUT translocation in 39% (22/57)
- CSF1 overexpression present in all TGCT/PVNS cases regardless of translocation status
- Supports targeting the CSF1/CSF1R axis therapeutically
Radiologic-Pathologic Correlation of PVNS/GCTTS
- GCTTS (tendon-sheath form) is the most common form of the disease, roughly 3:1 over intra-articular PVNS
- Tendon-sheath disease occurs most often in the hand and foot
- Prominent low T2 signal and 'blooming' artefact on gradient-echo from hemosiderin are nearly pathognomonic
- MRI is optimal for defining lesion extent to guide complete resection
GCTTS Can Mimic Intrinsic Bone Lesions
- Within 200 consecutive osseous (pseudo)tumours of the hand, 6 were caused by a neighbouring GCTTS eroding bone
- Lesions showed well-defined cortical defects or scalloping; one was slightly expansile and osteolytic
- Dense collagen and hemosiderin-laden macrophages explain high CT attenuation and low T2 signal
- Marked gadolinium enhancement from proliferative capillaries
Surgical Management of TGCT: Systematic Review
- Systematic review of 25 studies (from 434 screened) on surgical, adjuvant and systemic treatment of TGCT
- Diffuse TGCT carries high risk of recurrence, progression and disability
- Surgery remains standard; high recurrence and surgical risk motivate novel systemic options
- Systemic CSF1R-directed therapy is valuable within a multidisciplinary approach for advanced disease
Risk Factors for Margin Positivity and Recurrence (Hand)
- 44 patients with localised hand TGCT treated surgically (2009-2023); 68% female, mean age 47.5y
- Most common site: index (second) finger, 31.8%; positive margins in 20.5%
- Recurrence in 9.1% overall, but 44.4% among patients with positive margins
- Bone invasion, IP-joint proximity, neurovascular involvement and Al-Qattan type 2 independently predicted positive margins and recurrence
Hand GCTTS: 11-Year Series with Functional Outcomes
- 36 patients (23 female), mean age 38.8y, mean tumour diameter 2.6 cm
- Classified by Al-Qattan system; recurrence in 4 patients (11.1%) at mean 21-month follow-up
- Mean QuickDASH 6.3; 86% rated their outcome satisfactory
- No recurrent case had received postoperative radiotherapy
Pexidartinib for Advanced TGCT (ENLIVEN Phase 3)
- Randomised phase 3 trial, 120 patients with symptomatic advanced TGCT not amenable to surgery
- Overall response at week 25 (RECIST): 39% (24/61) with pexidartinib vs 0% placebo (p less than 0.0001)
- Serious adverse events in 13% of pexidartinib patients vs 2% placebo
- Mixed/cholestatic hepatotoxicity led to early enrolment closure - an identified risk
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Painless Volar Digit Mass
"A 42-year-old woman presents with a 2-year history of a painless mass on the volar aspect of her index finger. On examination, you feel a firm, well-defined, non-tender nodule attached to the flexor tendon sheath. The mass does not transilluminate. MRI shows a lobulated mass with low signal on T1 and T2. What is your diagnosis and management?"
Scenario 2: Surgical Technique for GCTTS Excision
"You have decided to proceed with excision of a localized GCTTS on the volar aspect of the index finger. Walk me through your surgical approach and key technical points."
Scenario 3: Recurrent GCTTS Management
"A 38-year-old woman had excision of GCTTS from her middle finger 18 months ago. She now presents with a recurrent mass at the same site. MRI shows an infiltrative mass wrapping around the flexor tendon and adherent to digital nerve. How do you manage this?"
MCQ Practice Points
Epidemiology Question
Q: What is the most common location for GCTTS? A: Volar aspect of the digits (hand and wrist 75% of cases), specifically index and middle fingers most common. Foot accounts for 20% of cases. GCTTS is the second most common hand tumor after ganglion cyst (10% of hand masses).
Pathogenesis Question
Q: What is the relationship between GCTTS and PVNS? A: GCTTS equals PVNS (same disease, different location). Both are tenosynovial giant cell tumor (TGCT) driven by CSF1-COL6A3 fusion. PVNS is intra-articular (joint synovium), GCTTS is extra-articular (tendon sheath). Same histology (hemosiderin, giant cells) and molecular pathogenesis (CSF1 overexpression).
Imaging Question
Q: What is the characteristic MRI appearance of GCTTS? A: Low signal on both T1 and T2 weighted sequences due to hemosiderin (iron) deposition. Blooming artifact on gradient echo (GRE) sequences is also characteristic (same as PVNS). This distinguishes GCTTS from ganglion (high T2 signal) and other soft tissue masses.
Treatment Question
Q: What is the key surgical principle to minimize GCTTS recurrence? A: Complete marginal excision with intact capsule - avoid tumor fragmentation or spillage. Fragmentation increases recurrence from 10-15% to over 30%. Also critical to search for and remove satellite lesions (small nodules near main tumor) which contribute to recurrence.
Recurrence Question
Q: What is the recurrence rate for localized vs diffuse GCTTS? A: Localized GCTTS: 10-15% recurrence with complete excision (well-encapsulated, easier to excise completely). Diffuse GCTTS: 30-40% recurrence despite wide excision (infiltrative growth, difficult to achieve negative margins). Time to recurrence: median 1-2 years.
Guidelines, Registries & Global Practice
Global Epidemiology Snapshot
GCTTS is the most common form of tenosynovial giant cell tumour worldwide - roughly a 3:1 ratio over intra-articular PVNS (Murphey, Radiographics 2008). It is the second most common hand mass after the ganglion cyst, predominates in the hand and foot, peaks at 30-50 years, and shows consistent female predominance across international series (64-68% female in recent hand cohorts). The localized nodular form accounts for ~90% of digital cases; the diffuse type is rarer but disproportionately drives recurrence.
Side-by-Side Guidance and Evidence Sources
| Body / Source | Position on GCTTS / TGCT | Practical Implication |
|---|---|---|
| WHO Classification of Soft Tissue Tumours | Localized and diffuse TGCT classed as benign; rare malignant TGCT recognised | Malignant transformation is exceptional - biopsy any atypical/rapidly growing lesion |
| AAOS / orthopaedic oncology (US) consensus reviews | Marginal excision for localized; multidisciplinary care plus consider systemic therapy for diffuse/advanced | Site and type drive aggressiveness of surgery and need for adjuvants |
| EORTC / ESMO sarcoma guidance (Europe) | Surgery is standard; CSF1R inhibition (pexidartinib) for symptomatic advanced disease not amenable to surgery | Reserve systemic therapy for unresectable/morbid diffuse disease |
| FDA (2019) / EMA regulatory status | Pexidartinib FDA-approved for symptomatic TGCT not amenable to surgery (REMS for hepatotoxicity); EMA approval not granted | Access to systemic therapy varies by region - surgery remains the global default |
Registry & Evidence Notes
- No dedicated implant registry (GCTTS is a soft-tissue excision, not arthroplasty)
- Evidence base is retrospective series and systematic reviews, plus one phase 3 RCT (ENLIVEN) for advanced TGCT
- Recurrence reporting is heterogeneous: ~10-15% localized, ~30-40% diffuse across pooled series
- Histology is the diagnostic gold standard in every setting
High- vs Limited-Resource Practice
- High-resource: MRI mapping, microsurgical excision, pexidartinib for refractory diffuse disease, radiosynoviorthesis for joint disease
- Limited-resource: Diagnosis often clinical plus ultrasound or radiograph; marginal excision under loupe magnification with tourniquet
- Outcomes for localized digital GCTTS are excellent globally with complete excision
- Systemic CSF1R inhibitors are costly and not universally available
Consent and Documentation (Globally Applicable)
Key points to document for GCTTS surgery:
- Recurrence risk: 10-20% overall, higher (30-40%) for diffuse type
- Neurovascular injury: digital nerve or artery injury risk (permanent numbness or digit ischaemia)
- Stiffness: risk if prolonged immobilisation - early ROM mitigates this
- Incomplete excision: residual/satellite disease drives recurrence
- Functional impact: typically 2-4 weeks off manual work plus hand therapy
GCTTS is a common hand tumour managed routinely by hand and orthopaedic surgeons worldwide, with excellent outcomes after complete excision of localized disease.
GIANT CELL TUMOR OF TENDON SHEATH (GCTTS)
Clinical summary
Key Pathology
- •GCTTS equals TGCT extra-articularly (same as PVNS, different location)
- •CSF1-COL6A3 fusion drives CSF1 overexpression and macrophage recruitment
- •Histology: Multinucleated giant cells, hemosiderin-laden macrophages, mononuclear stromal cells, xanthoma cells
- •Gross: Tan-yellow lobulated mass attached to tendon sheath
Epidemiology
- •Second most common hand tumor (after ganglion) - 10% of hand masses
- •Peak age 30-50 years, female 2:1
- •Location: Hand/wrist 75% (volar digits - index/middle finger), foot 20%
- •Localized type 90%, diffuse type 10%
Imaging
- •MRI low signal T1 and T2 = hemosiderin (same as PVNS)
- •Blooming artifact on GRE sequences
- •Well-defined margins (localized) or infiltrative (diffuse)
- •XR: Bone erosion in 20-30% (pressure erosion, not invasion)
Treatment
- •Localized: Marginal excision with intact capsule (10-15% recurrence)
- •Diffuse: Wide excision with margins (30-40% recurrence)
- •Key principle: Intact capsule (fragmentation increases recurrence 3-fold)
- •Remove satellite lesions, early ROM to prevent stiffness
Surgical Pearls
- •Bruner incision for volar access, protect digital neurovascular bundles
- •Magnification (loupes/microscope) critical for nerve/vessel protection
- •Excise en bloc with intact capsule - avoid tumor spillage
- •Search for satellites, curettage bone erosions if present