Excision Arthroplasty | Salvage Procedure | Definitive or Staging
Indications
Critical Must-Knows
- Primary indication: Periprosthetic joint infection (PJI) not suitable for DAIR
- Named after Gathorne Robert Girdlestone (1881-1950)
- Results in significant LLD (4-6cm) and functional limitation
- Can be definitive or interim (2-stage revision)
- Harris hip score improves with reimplantation
Clinical Pearls
- "Trendelenburg gait expected post-procedure
- "Hip abductors critical for stability of pseudarthrosis
- "Spacer preferred for interim if reimplantation planned
- "Higher success rate when combined with adequate antibiotics
Clinical Imaging
Imaging Gallery

Critical Girdlestone Exam Points
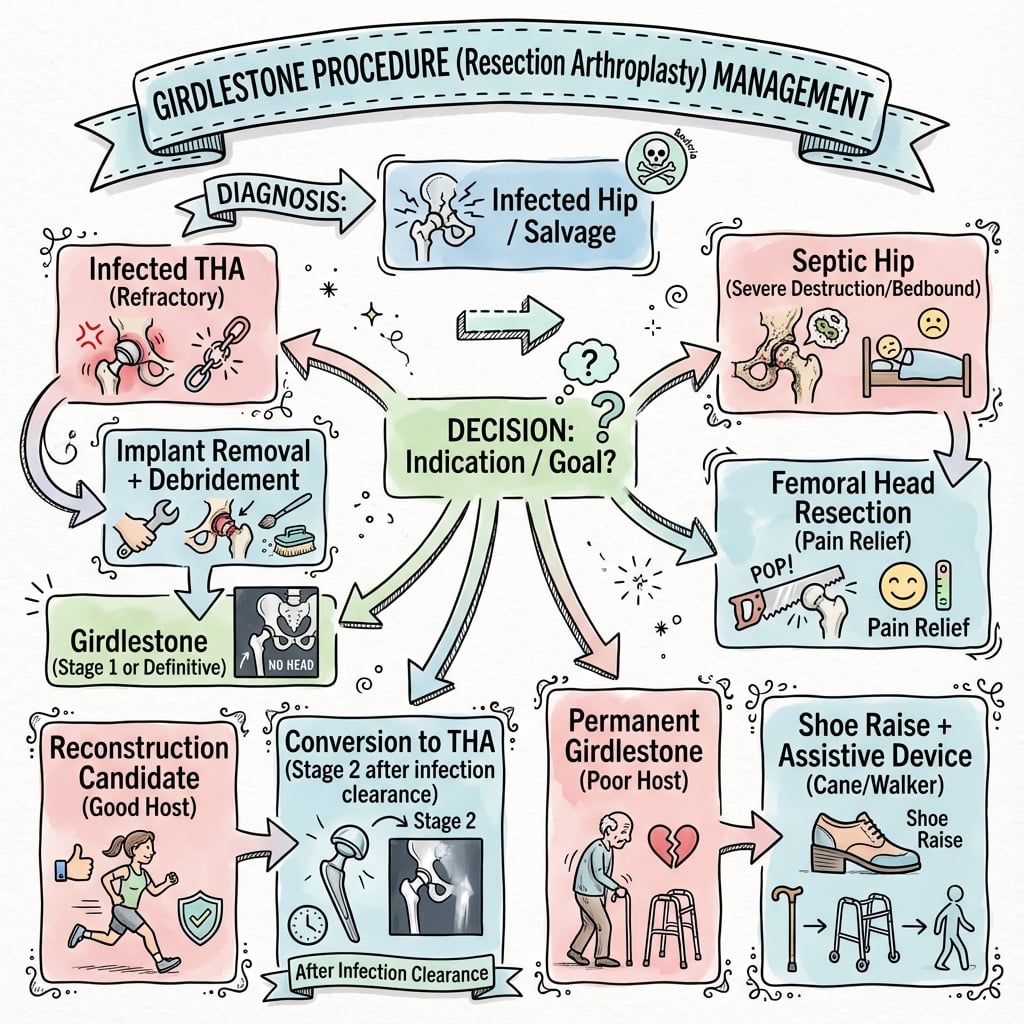
Core Indication
Periprosthetic joint infection where DAIR has failed or is contraindicated. Patient must be medically fit for surgery and able to tolerate prolonged antibiotics. Can be definitive (permanent) or interim (before reimplantation).
Functional Outcome
Significant disability expected: 4-6cm limb length discrepancy, Trendelenburg gait, need for walking aids. Pain relief usually achieved. 50-60% ambulatory with aids. Better than ongoing sepsis or repeated failed surgery.
Surgical Goal
Complete removal of infected prosthesis, cement, and devitalized tissue. Aggressive debridement is key to infection eradication. Preserve abductor mechanism when possible for pseudarthrosis stability.
Alternative Options
Antibiotic-loaded articulating spacer preferred for staging if reimplantation planned. Spacer maintains soft tissue tension and improves functional outcome during treatment. Static spacer or excision for definitive cases.
Quick Decision Guide
| Clinical Scenario | Fitness for Revision | Microorganism | Recommendation |
|---|---|---|---|
| Infected THA, medically fit | Yes | Sensitive, identifiable | 2-stage with spacer preferred |
| Infected THA, multiple surgeries | Limited | Resistant/fungal | Girdlestone (possibly definitive) |
| Failed 2-stage, ongoing infection | Exhausted options | Any | Definitive Girdlestone |
| Medical comorbidities prohibit revision | No | Any | Definitive Girdlestone + suppression |
RESCUEIndications for Girdlestone
| R | Resistant organism MDR pathogens or fungi |
| E | Exhausted surgical options Multiple failed revisions |
| S | Sepsis ongoing Persistent infection despite treatment |
| C | Comorbidities preclude revision Not medically fit |
| U | Unable to comply with antibiotic regimen Non-compliance risk |
| E | Extreme bone loss Insufficient acetabular/femoral stock |
| R | Resistant organism MDR pathogens or fungi | S | Sepsis ongoing Persistent infection despite treatment | U | Unable to comply with antibiotic regimen Non-compliance risk |
| E | Exhausted surgical options Multiple failed revisions | C | Comorbidities preclude revision Not medically fit | E | Extreme bone loss Insufficient acetabular/femoral stock |
Hook:When patient needs RESCUE from failed hip, consider Girdlestone!
RECLAIMKey Steps
| R | Remove prosthesis All components including cement |
| E | Excise infected tissue Aggressive debridement |
| C | Collect samples Multiple tissue samples for microbiology |
| L | Lavage thoroughly Copious irrigation (9L) |
| A | Abductors preserve Maintain hip stability |
| I | IV antibiotics Prolonged course (6-12 weeks) |
| M | Mobilize cautiously Protected weight bearing |
| R | Remove prosthesis All components including cement | L | Lavage thoroughly Copious irrigation (9L) | M | Mobilize cautiously Protected weight bearing |
| E | Excise infected tissue Aggressive debridement | A | Abductors preserve Maintain hip stability | ||
| C | Collect samples Multiple tissue samples for microbiology | I | IV antibiotics Prolonged course (6-12 weeks) |
Hook:RECLAIM the hip from infection!
SPACEGirdlestone vs Spacer
| S | Soft tissue tension Spacer maintains, Girdlestone loses |
| P | Planning for reimplantation Spacer if revision likely |
| A | Ambulatory status Better function with spacer |
| C | Cost consideration Spacer adds cost, Girdlestone simpler |
| E | Eradication goal Both effective if adequate debridement |
| S | Soft tissue tension Spacer maintains, Girdlestone loses | C | Cost consideration Spacer adds cost, Girdlestone simpler |
| P | Planning for reimplantation Spacer if revision likely | E | Eradication goal Both effective if adequate debridement |
| A | Ambulatory status Better function with spacer |
Hook:Use SPACE (spacer) if reimplantation planned!
Overview and Epidemiology
The Girdlestone procedure (excision arthroplasty) involves resection of the femoral head and neck without replacement. Originally described by Gathorne Robert Girdlestone for tuberculosis of the hip, it is now primarily used as a salvage procedure for periprosthetic joint infection (PJI) when other options have failed or are contraindicated.
Historical Context
G.R. Girdlestone (1881-1950) described excision arthroplasty in 1943 for tuberculosis of the hip. Pre-antibiotic era, it was the primary treatment for septic hip. Now reserved for salvage of infected arthroplasty or when patient is not a candidate for replacement.
Current Applications
- PJI: Failed DAIR or 2-stage
- Recurrent deep infection
- Not fit for revision surgery
- Resistant/difficult organisms
- Severe bone loss precluding reimplantation
Rare Indications
- Native hip septic arthritis (failed treatment)
- Tuberculosis (historical, rare now)
- Severe avascular necrosis (not suitable for THR)
- Certain malignancies (palliation)
Pathophysiology and Mechanisms
Key Anatomical Considerations
The abductor mechanism (gluteus medius/minimus inserting on greater trochanter) must be preserved for pseudarthrosis stability. Excessive bone resection results in proximal migration and worse function. The sciatic nerve is at risk and must be protected during posterior dissection.
Structures to Preserve vs Remove
| Structure | Preserve/Remove | Rationale |
|---|---|---|
| Greater trochanter (if viable) | PRESERVE | Abductor attachment crucial for stability |
| Femoral head/neck | REMOVE | Source of infection, resect to healthy bone |
| All implants and cement | REMOVE | Biofilm eradication requires complete removal |
| Abductor complex | PRESERVE | Trendelenburg gait worsens if lost |
| Hip capsule remnants | VARIABLE | May help contain pseudarthrosis |
Biomechanics of Pseudarthrosis
After Girdlestone, a fibrous pseudarthrosis develops. The proximal femur migrates superiorly until it articulates with the ischium/ilium. Abductor function determines stability - if preserved, patient may achieve limited ambulation. LLD of 4-6cm is typical.
Post-Resection Anatomy
- Proximal femoral stump
- Fibrous pseudarthrosis
- Proximal migration (4-6cm)
- Acetabulum becomes defunctioned
- Weight bearing through ischium
Functional Implications
- Positive Trendelenburg sign
- Marked limp
- Need for walking aids (cane or walker)
- Sitting tolerance usually preserved
- Severe restriction of activity
Classification Systems
Periprosthetic Joint Infection Classification
| Type | Timing | Typical Organism | Management |
|---|---|---|---|
| Acute postoperative | Less than 4 weeks post-op | S. aureus, gram-negatives | DAIR often successful |
| Late chronic | Greater than 4 weeks, less than 12 months | S. epidermidis, low virulence | DAIR may work, often 2-stage |
| Acute hematogenous | Any time, acute onset | S. aureus, streptococcus | DAIR if less than 3 weeks symptoms |
| Chronic (greater than 12 months) | Established infection | Any organism | 2-stage or Girdlestone |
DAIR vs Excision
DAIR success factors: Acute infection (less than 4 weeks), sensitive organism, well-fixed prosthesis, healthy host. Girdlestone indications: Failed DAIR, chronic infection, resistant organisms, poor host status.
Classification helps predict treatment success and guides surgical planning.
Clinical Assessment
History
- Presenting symptoms: Pain, swelling, sinus drainage
- Timeline: Acute vs chronic symptoms
- Previous surgeries: Number of revisions, organisms
- Antibiotic history: Previous treatments, allergies
- Comorbidities: Diabetes, immunosuppression
Physical Examination
- Wound inspection: Sinus tract, drainage, erythema
- Joint assessment: Warmth, effusion, ROM
- Neurovascular: Sciatic nerve function
- Limb length: Current discrepancy
- Gait: Ambulatory status
Clinical Indicators of PJI
| Finding | Significance | Action Required |
|---|---|---|
| Sinus tract communicating with prosthesis | Definitive for PJI | No further testing needed for diagnosis |
| Persistent wound drainage greater than 4 weeks | Highly suspicious | Aspiration and imaging |
| Pain with previously well-functioning joint | Suggestive | Full workup needed |
| Elevated inflammatory markers (CRP/ESR) | Supportive evidence | Correlate with clinical picture |
Sinus Tract = PJI
A sinus tract communicating with the prosthesis is pathognomonic for periprosthetic joint infection. No further diagnostic tests are required - proceed directly to treatment planning.
Investigations
Diagnostic Workup
Inflammatory markers: CRP (most sensitive), ESR. Serial values help monitor treatment response. WCC often normal in chronic infection.
Synovial fluid analysis: WCC (greater than 3000/μL), PMN% (greater than 80%), culture (hold 14 days). Alpha-defensin if available.
Radiographs: Component loosening, periosteal reaction. CT: Bone loss assessment, cement location. Nuclear medicine: If diagnosis uncertain.
MSIS Criteria for PJI Diagnosis
| Category | Criteria | Interpretation |
|---|---|---|
| Major (1 = positive) | Sinus tract OR 2+ cultures same organism | Definitive diagnosis |
| Minor (3+ = positive) | Elevated ESR/CRP | Supportive evidence |
| Minor | Elevated synovial WCC (greater than 3000) | Supportive evidence |
| Minor | Elevated synovial PMN% (greater than 80%) | Supportive evidence |
| Minor | Positive histology (greater than 5 PMN/HPF) | Supportive evidence |
| Minor | Positive single culture | Supportive evidence |
Culture Protocol
Extended culture (14 days) improves detection of slow-growing organisms like Propionibacterium acnes. Take samples BEFORE antibiotics. Minimum 5 tissue samples from different locations for optimal sensitivity.
Management Algorithm
Treatment Algorithm
Step 1: Confirm PJI Diagnosis
- Apply MSIS criteria
- Identify organism if possible
Step 2: Assess Patient Factors
- Medical fitness for surgery
- Bone stock quality
- Social support and compliance
- Functional expectations
Step 3: Treatment Selection
| Clinical Scenario | Recommended Treatment | Rationale |
|---|---|---|
| Acute PJI, fit patient, sensitive organism | DAIR first | High success rate, preserves function |
| Failed DAIR, fit patient, reconstructable | 2-stage with spacer | Good outcomes, aims for reimplantation |
| Failed 2-stage OR unfit for revision | Girdlestone (definitive) | Prioritizes infection control |
| Unfit for any surgery | Chronic suppression | Palliative approach |
Spacer vs No Spacer
Articulating spacer if reimplantation planned - maintains soft tissue tension, improves interim function. No spacer (Girdlestone) for definitive cases or when spacer stability is not achievable.
Multidisciplinary discussion with ID, microbiology, and patient is essential.
Indications and Contraindications
When to Consider Girdlestone
| Indication | Context | Type |
|---|---|---|
| Failed DAIR for PJI | Early infection, debridement insufficient | Staging or definitive |
| Failed 2-stage revision | Recurrent infection despite reimplantation | Definitive |
| Resistant/difficult organisms | Fungal, MDR bacteria | Definitive or long-term antibiotic |
| Medical comorbidities | High surgical risk, poor functional reserve | Definitive |
| Severe bone loss | Insufficient stock for reconstruction | Definitive |
| Non-compliant patient | Unable to complete antibiotic course | Definitive with suppression |
DAIR Failure Criteria
DAIR (Debridement, Antibiotics, Implant Retention) failure is an indication. Failure criteria include: persistent positive cultures, sinus tract persistence, ongoing clinical infection, or CRP/ESR non-normalization despite adequate course.
Patient selection is critical - discuss functional expectations thoroughly.
Preoperative Planning
Preoperative Workup
Confirm diagnosis: Aspiration with culture (extend hold time for slow-growing organisms), inflammatory markers (CRP, ESR), imaging (XR, CT for bone loss). Apply MSIS criteria for PJI diagnosis.
ID the pathogen: Determines antibiotic selection and duration. Consider resistant organisms, fungi, or mycobacteria in refractory cases. Liaise with microbiology/ID early.
Optimize patient: Nutrition (albumin greater than 3g/dL, total lymphocyte count), glycemic control (HbA1c under 8%), smoking cessation. Address cardiac, renal comorbidities.
Plan approach: Review previous incisions. Assess bone loss on imaging. Discuss with patient: realistic functional expectations, need for aids, LLD. Consider if spacer or definitive.
MSIS Criteria for PJI
Major criteria (1 = positive): Sinus communicating with prosthesis, OR same organism on 2 separate cultures. Minor criteria (3+ = positive): Elevated ESR/CRP, elevated synovial WCC, elevated synovial PMN%, positive histology, positive single culture. Be familiar with these criteria for diagnosis.
Laboratory Workup
- CRP and ESR: Baseline, follow response
- Synovial fluid: WCC, differential, culture
- Blood cultures: If systemic symptoms
- Albumin/prealbumin: Nutrition status
- HbA1c: Glycemic control
Imaging Workup
- XR: Component loosening, bone loss
- CT: Bone defects, cement location
- MRI: Soft tissue collection (rare)
- Nuclear medicine: If diagnosis uncertain
Surgical Technique
Setup and Approach
Positioning Steps
General or regional anesthesia. Prepare for potentially lengthy procedure. Adequate IV access and invasive monitoring if indicated. Administer antibiotics AFTER intraoperative cultures taken.
Lateral decubitus position is most common. Allows access to acetabulum and femur. Alternative: supine on fracture table if combined procedure. Secure pelvis with supports.
Standard prep and drape. Expose entire limb for length assessment. Mark previous incisions. Plan extensile approach if needed for cement removal.
Antibiotic Timing
Do not give antibiotics until intraoperative cultures taken. Collect minimum 5 tissue samples from different areas (synovium, capsule, bone-implant interface). Send for aerobic, anaerobic, and fungal cultures. Extended culture (14 days) for slow-growing organisms.
Prepare for extensile approach if cemented prosthesis with aggressive cement removal needed.
Complications
Potential Complications
| Complication | Incidence | Prevention/Management |
|---|---|---|
| Persistent infection | 10-30% | Adequate debridement, appropriate antibiotics, suppression if needed |
| Wound complications | 15-25% | Optimize nutrition, meticulous closure, manage dead space |
| Instability/dislocation | Common (inherent) | Expected outcome - brace/abduction pillow initially |
| Periprosthetic fracture (during removal) | 5-10% | Careful technique, prophylactic fixation if needed |
| Nerve injury (sciatic) | 1-3% | Careful dissection, identify and protect nerve |
| DVT/PE | Variable | Chemical and mechanical prophylaxis |
Persistent Infection
10-30% may have persistent infection despite adequate surgery. Risk factors: resistant organisms, inadequate debridement, retained cement/foreign material, immunocompromise. Options: repeat debridement, long-term suppression, or accept chronic wound.
Managing Persistent Infection
If infection persists: (1) Confirm adequate initial debridement, (2) Review antibiotic sensitivity and compliance, (3) Consider repeat surgery for retained material, (4) Long-term oral antibiotic suppression may control but not eradicate infection.
Postoperative Care
Postoperative Protocol
Ward care: Pain management, wound monitoring. Begin DVT prophylaxis. Drain management. Hip abduction pillow or brace for comfort. IV antibiotics continue (based on cultures).
Mobilization: Sit out of bed day 1-2. Protected weight bearing with frame/crutches. Physiotherapy - maintain muscle function. Wound inspection. Staple removal 2 weeks.
Ongoing care: Continue IV antibiotics (typically 6 weeks minimum). Transition to oral antibiotics if appropriate. Progressive mobilization. Address LLD with shoe raise.
Recovery phase: Complete antibiotic course. Monitor inflammatory markers (CRP should normalize). Consider reimplantation if staged procedure. Finalize walking aids, orthotics.
Antibiotic Duration
Minimum 6 weeks IV antibiotics followed by oral therapy. Duration depends on organism, response, and whether reimplantation planned. Consult infectious diseases for regimen. Monitor for drug toxicity (aminoglycosides - renal/ototoxicity, rifampicin - hepatic).
Mobilization Protocol
- WBAT with aids - walker or crutches
- Hip abduction strengthening
- Gait training for LLD
- Shoe raise 3-5cm for LLD
- Progress to single cane over months
Monitoring
- CRP weekly initially, then monthly
- Wound assessment at each visit
- Imaging if concern for retained material
- Monitor antibiotic side effects
- Assess function and pain
Outcomes and Prognosis
Outcomes Summary
| Outcome Measure | Girdlestone (Definitive) | 2-Stage with Reimplantation |
|---|---|---|
| Infection eradication | 70-80% | 75-85% |
| Harris Hip Score | 40-50 | 70-85 |
| Ambulatory status | 50-60% (with aids) | 85-95% |
| Patient satisfaction | Variable | Higher |
| Leg length discrepancy | 4-6cm | 1-2cm (correctable) |
Functional Expectations
Definitive Girdlestone = significant disability. Most patients need walking aids permanently, have marked limp (Trendelenburg), and 4-6cm LLD. Pain relief is usually achieved. Sitting tolerance preserved. Better than ongoing sepsis but substantially worse than successful reimplantation.
Good Outcomes
- Pain control achieved
- Infection eradicated
- Independent in ADLs
- Ambulatory with aids
- Satisfied with outcome given alternatives
Poor Outcomes
- Persistent infection
- Chronic wound/sinus
- Non-ambulatory
- Intractable pain
- Poor quality of life
Evidence Base
- Single-centre series of 88 patients (91 hips) with refractory PJI. Infection eradicated in 65/91 (71%). Mean limb shortening 5.7cm; mean walking distance 175m; mean Merle d'Aubigné-Postel score 9.3/18. Corticosteroid use (HR 6), preoperative fever (HR 4.1) and polymicrobial infection (HR 2.5) were independent predictors of failure. Infection-related mortality 7%.
- 28 hips in 26 patients treated by Girdlestone resection (mixed septic, tubercular, post-traumatic and CP indications). Pain relief in 84%; all patients required walking aids and all had a positive Trendelenburg sign. Mean limb shortening 3.8cm (range 1.5-6.5cm). Mean Harris Hip Score 64 (range 25-83); no excellent outcomes. 74% satisfied given alternatives.
- 25 knees treated with resection arthroplasty for recalcitrant PJI after a mean of 5 prior operations. 84% free of infection at mean 4-year follow-up; only 1 amputation. 45% community ambulators, 35% household, 20% transfer-only — all required bracing and assistive devices.
- Pragmatic multicentre RCT of 140 patients with hip PJI. No difference in WOMAC at 18 months between single- and two-stage revision; single-stage was better at 3 months, had fewer intraoperative complications (8% vs 27%) and was cost-effective. Markers of possible ongoing infection were similar (14% vs 11%).
- Original standardized MSIS definition of PJI. Major criteria: sinus tract communicating with prosthesis, OR same organism on 2 separate cultures. Minor criteria (4 of 6): elevated ESR/CRP, elevated synovial WCC, elevated synovial PMN%, positive histology, single positive culture, purulence.
- Evidence-based, externally validated scoring system. Major criteria (sinus tract or 2 positive cultures) remain diagnostic. Weighted minor criteria: serum CRP/D-dimer/ESR and synovial WCC, alpha-defensin, leukocyte esterase, PMN%, synovial CRP; aggregate score of 6 or more = infected. Sensitivity 97.7% vs 79.3% for the 2011 MSIS criteria.
- 489 joints across 24 studies. Candida albicans was the commonest organism (41.5%); 50.5% had concurrent bacterial coinfection. Recurrence by strategy: DAIR 81.4%, resection arthroplasty 53.1%, two-stage 47.7%. Mean systemic antifungal duration 12.8 weeks (fluconazole commonest); amphotericin B was the dominant cement additive.
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Failed 2-Stage Revision
"A 72-year-old diabetic man has had 2 previous revisions for infected THA over 5 years. He now presents with recurrent infection (MRSA), draining sinus, and HbA1c of 9.5%. He is a widower living alone with minimal family support."
Scenario 2: Staging for Reimplantation
"A 58-year-old otherwise healthy woman presents with infected THA (Staphylococcus epidermidis, susceptible) 2 years post primary. DAIR failed after 6 weeks. She is motivated for best functional outcome and wants to return to golf."
Scenario 3: Intraoperative Finding
"During first stage of 2-stage revision for PJI, you encounter severe acetabular bone loss with a cavitary defect and pelvic discontinuity. The femur has reasonable stock. What do you do?"
Scenario 4: Fungal PJI
"Culture from hip aspiration grows Candida albicans in a 65-year-old immunocompetent patient with painful THA. No previous surgery. What is your management?"
MCQ Practice Points
Primary Indication
Q: What is the most common indication for Girdlestone excision arthroplasty today? A: Periprosthetic joint infection (PJI) where DAIR has failed or is contraindicated, or as interim/definitive salvage for multiply recurrent infection. It was originally described for tuberculosis of the hip.
Expected Leg Length Discrepancy
Q: What leg length discrepancy is typically expected after Girdlestone procedure? A: 4-6cm shortening - The proximal femur migrates superiorly until it articulates with the pelvis at a pseudarthrosis. This results in significant shortening requiring shoe raise and walking aids.
Tissue Samples
Q: How many tissue samples should be obtained during revision for PJI? A: Minimum 5 tissue samples from different locations (membrane, capsule, acetabulum, femoral canal, collections). Take BEFORE antibiotics. Send for aerobic, anaerobic, and extended culture.
Spacer Benefit
Q: What is the main advantage of an articulating antibiotic spacer over Girdlestone as interim procedure? A: Maintains soft tissue tension - Preserves abductor length, improves interim function, and facilitates subsequent reimplantation by keeping soft tissues at appropriate tension and length.
MSIS Criteria
Q: What are the major criteria for PJI diagnosis according to MSIS? A: Two major criteria: (1) Sinus tract communicating with the prosthesis, OR (2) Same organism isolated on 2 or more separate tissue/fluid samples. Either one confirms PJI.
Guidelines, Registries & Global Practice
Hip PJI affects roughly 1-2% of primary and up to 4-5% of revision total hip replacements worldwide. As arthroplasty volumes rise, the absolute burden of PJI is growing, and resection arthroplasty persists as the salvage of last resort across all health systems.
Side-by-Side Guidance: PJI Diagnosis & Salvage
| Body | Diagnostic Framework | Position on Resection Arthroplasty |
|---|---|---|
| MSIS / ICM (international) | MSIS 2011 + 2018 validated weighted scoring; ICM consensus | Salvage for unreconstructable or multiply-failed PJI; spacer preferred if reimplantation feasible |
| AAOS (US) | Two-test screening (ESR + CRP), then aspiration; aligns with MSIS | Resection acceptable when host/limb cannot tolerate reconstruction |
| BOA / BOAST + NICE (UK) | Multidisciplinary PJI MDT; aspiration before empirical antibiotics | Single- or two-stage favoured (INFORM RCT); resection reserved for non-reconstructable hips |
| EBJIS / EFORT (Europe) | EBJIS definition (confirmed/likely/unlikely PJI) | Resection or definitive Girdlestone for refractory infection or unfit host |
Registry Evidence
- National registries (NJR England/Wales, AOANJRR, SHAR/Swedish, AJRR US, NZJR) track revision-for-infection rates
- Infection is a leading cause of early hip revision in all major registries
- Resection/excision is recorded but represents a small minority of revision outcomes
- Registry data confirm rising absolute PJI burden with increasing arthroplasty volume
High- vs Limited-Resource Practice
- High-resource: 2-stage with antibiotic spacer, OPAT, alpha-defensin/D-dimer, specialist PJI MDT
- Limited-resource: Girdlestone often used as definitive primary salvage (no spacer, limited microbiology)
- TB and chronic septic native hip still managed by primary excision in endemic regions
- Prolonged IV antibiotics may be replaced by early oral therapy (OVIVA-supported) where OPAT unavailable
Global Exam Focus
Examiners worldwide (FRCS, FRACS, EBOT, ABOS, DNB/MS) will expect: PJI diagnosis by MSIS/EBJIS criteria, the indication hierarchy (DAIR → single/two-stage → resection), surgical steps with the tissue-sampling protocol, antibiotic principles, and honest counselling of functional outcomes (shortening, Trendelenburg, aid-dependence).
Differential Diagnosis
A painful or failing hip arthroplasty is not always infected. Distinguishing PJI from aseptic causes is the pivotal decision before resection — an unnecessary Girdlestone for aseptic loosening is a catastrophic error.
Painful THA: PJI vs Mimics
| Diagnosis | Discriminating Features | Key Test | Why It Matters |
|---|---|---|---|
| Periprosthetic joint infection | Sinus, rest pain, raised CRP/ESR, early loosening | Aspiration (synovial WCC/PMN%, culture), MSIS score | Mandates debridement/resection, not simple revision |
| Aseptic loosening | Activity-related pain, normal inflammatory markers | Serial radiographs (lucency, migration), normal aspirate | Treated by revision, NOT resection |
| Adverse local tissue reaction (MoM/trunnionosis) | Metal bearing, pseudotumour, rising cobalt/chromium | Metal ions, MARS-MRI | Revision of bearing, not infection pathway |
| Periprosthetic fracture | Trauma, acute pain, deformity | Radiographs, Vancouver classification | Fixation/revision, not excision |
| Referred / extra-articular pain | Spinal stenosis, GTPS, hernia, vascular claudication | Targeted exam, imaging, diagnostic injection | Avoids unnecessary hip surgery |
| Instability / soft-tissue impingement | Mechanical clunk, recurrent subluxation | Component-position CT, dynamic exam | Component revision, not resection |
Do Not Resect an Aseptic Hip
Always exclude aseptic loosening, ALTR and extra-articular pain before committing to excision arthroplasty. A negative aspirate, normal CRP/ESR and no sinus point away from infection. Resection arthroplasty for a misdiagnosed aseptic hip needlessly inflicts permanent shortening and aid-dependence.
Controversies & Areas of Uncertainty
Definitive Girdlestone vs Reconstruction
With megaprostheses, cup-cage constructs and single-stage revision now feasible, the threshold for definitive excision keeps rising. Debate centres on whether borderline hosts are better served by a complex reconstruction attempt or by accepting a stable, infection-free pseudarthrosis.
Spacer vs No Spacer
Articulating spacers improve interim function and soft-tissue tension, but no high-level RCT proves superior infection eradication over a true Girdlestone. Spacer-related complications (dislocation, fracture, mechanical failure) are real, especially with major bone loss.
Single- vs Two-Stage
The INFORM RCT found no medium-term difference in patient-reported outcome between single- and two-stage hip revision, with single-stage offering faster recovery and lower cost. This narrows, but does not abolish, the role of staged management and resection.
Antibiotic Duration & Route
Traditional 6-week IV courses are challenged by trial evidence (e.g. OVIVA) supporting early oral switch for bone and joint infection. Optimal duration after resection, and the value of lifelong suppression, remain unresolved.
GIRDLESTONE PROCEDURE
Clinical summary
Core Concepts
- •Excision arthroplasty = SALVAGE for infected THA
- •Named after GR Girdlestone (TB of hip, 1943)
- •Can be DEFINITIVE or INTERIM (2-stage)
- •Spacer preferred if reimplantation planned
Indications (RESCUE)
- •Failed DAIR or 2-stage revision
- •Resistant/difficult organisms (MDR, fungal)
- •Medical comorbidities precluding revision
- •Severe bone loss preventing reconstruction
Surgical Pearls
- •5+ tissue samples BEFORE antibiotics
- •Remove ALL cement (biofilm reservoir)
- •Preserve ABDUCTORS (stability of pseudarthrosis)
- •Copious lavage (minimum 9L)
Outcomes
- •Infection eradication: 70-80%
- •LLD: 4-6cm (need shoe raise)
- •50-60% ambulatory with aids
- •Harris Hip Score ~40-50 (vs 70-85 with reimplantation)
Exam Pearls
- •MSIS criteria for PJI diagnosis
- •Minimum 6 weeks IV antibiotics
- •Trendelenburg gait expected
- •Better than ongoing sepsis