Complex Reconstruction | Bone Loss Management | Registry Data Critical
- Aseptic loosening is the most common indication for revision THA (60-70%)
- Paprosky classification guides acetabular reconstruction strategy
- Component removal must preserve bone stock - avoid excessive reaming
- Infection must be ruled out - ESR, CRP, aspiration with culture in all cases
- AOANJRR data: Cemented stems have lower revision rate than uncemented in revision setting
- “Type IIIB acetabular defects require structural support (cage, triflange, or reconstruction ring)
- “Extended trochanteric osteotomy (ETO) provides excellent femoral stem exposure with low complication rate
- “Re-revision risk increases with each subsequent surgery - counsel patients accordingly
- “Australian registry shows higher failure rates for cementless acetabular components in revision
Aseptic loosening most common. Must exclude infection with CRP, ESR, aspiration. Recognize periprosthetic fracture, instability, liner wear, and osteolysis patterns.
Paprosky classification drives treatment. Type I-II use hemispherical cups. Type IIIA needs augments. Type IIIB requires structural support with cage or custom implant.
Preserve bone stock at all costs. Use extended trochanteric osteotomy for well-fixed stems. Avoid aggressive reaming of acetabulum. Plan extraction before incision.
Restore hip center and offset. Achieve biologic fixation when possible. Use modular components. Address leg length discrepancy. Consider constrained liners for instability.
- Defect Type
- Paprosky I-II acetabular, Cortical type femoral
- Treatment Strategy
- Standard hemispherical cup, cementless stem
- Key Pearl
- Prepare for one size larger cup
- Defect Type
- Paprosky IIIA acetabular
- Treatment Strategy
- Jumbo cup with superior augment or bone graft
- Key Pearl
- Superior dome augment restores hip center
- Defect Type
- Paprosky IIIB acetabular
- Treatment Strategy
- Cup-cage construct or custom triflange
- Key Pearl
- Requires pelvic discontinuity assessment
- Defect Type
- Paprosky III femoral
- Treatment Strategy
- Extended trochanteric osteotomy + long stem
- Key Pearl
- ETO allows controlled extraction with bone preservation
PREPAREDPreoperative Planning for Revision THA
Hook:Be PREPARED for revision THA - planning prevents poor performance in complex bone loss scenarios!
Overview and Epidemiology
Revision THA is one of the most technically demanding procedures in adult reconstruction. With increasing primary THA volumes and aging populations, revision burden is projected to increase by 137% by 2030. Australian registry data (AOANJRR) shows 18% cumulative revision rate at 15 years for primary THA, with aseptic loosening remaining the leading indication. Re-revision rates are significantly higher at 35% at 10 years, emphasizing the importance of getting the first revision right.
- Age: Mean 65-70 years at revision (younger than primary)
- Gender: Slightly more common in males
- Time to revision: Median 10-12 years from primary
- Registry trend: Increasing revision volume despite improving implant survival
- Complication rate: 2-3x higher than primary THA
- Operative time: 2-4 hours (vs 1-1.5 hours for primary)
- Blood loss: Average 600-800ml (higher with bone loss)
- Hospital stay: 5-7 days vs 2-3 days for primary
Indications for Revision THA
Aseptic Loosening (60-70% of Revisions)
- Radiographic Signs
- Radiolucent lines over 2mm, cup migration, screw breakage
- Clinical Presentation
- Groin pain with activity, start-up pain
- Threshold for Revision
- Symptomatic loosening with function limitation
- Radiographic Signs
- Subsidence over 5mm, progressive radiolucency, cement mantle fracture
- Clinical Presentation
- Thigh pain with weight-bearing, limp
- Threshold for Revision
- Painful subsidence or osteolysis threatening bone stock
- Radiographic Signs
- Dual loosening with osteolysis
- Clinical Presentation
- Severe hip pain, reduced function
- Threshold for Revision
- Symptomatic with deteriorating bone stock
Key Investigation: Rule out infection with CRP, ESR, hip aspiration if inflammatory markers elevated.
FAILSAFEIndications for Revision THA
Hook:FAILSAFE captures all revision THA indications - aseptic loosening leads, but infection must be excluded in every case!
Anatomy and Biomechanics
Hip Anatomy Relevant to Revision THA
- Anterior column: Iliopubic - supports anterior rim and dome
- Posterior column: Ilioischial - supports posterior wall and dome
- Quadrilateral surface: Medial wall between columns
- Teardrop: Radiographic landmark for medial wall integrity
- Kohler's line: Assess medial cup migration
- Metaphysis: Proximal fit region for standard stems
- Diaphysis: Distal fixation zone for revision stems
- Isthmus: Narrowest point, critical for canal-filling stems
- Cortical thickness: Determines perforation risk during revision
- Canal geometry: Champagne-flute vs stovepipe shapes
Biomechanical Principles in Revision
Anatomic hip center should be restored whenever possible:
- Superior migration increases joint reaction forces by 30-50%
- Increases abductor moment arm demands
- Leads to Trendelenburg gait and instability
- AAOS guideline: Restore center within 2cm of anatomic position
Accepting superior center trades short-term stability for long-term abductor insufficiency.
- Implication for Revision
- Bone loss reduces load-bearing area
- Technical Solution
- Maximize host bone contact, use augments to restore rim support
- Implication for Revision
- Metaphyseal deficiency prevents proximal fixation
- Technical Solution
- Bypass defect, achieve distal diaphyseal fixation over 4cm
- Implication for Revision
- Insufficient offset causes impingement and instability
- Technical Solution
- Use modular stems, adjust neck length, plan templating
- Implication for Revision
- Excessive lengthening causes nerve injury
- Technical Solution
- Limit to under 4cm, accept slight shortness if needed
Classification Systems
Paprosky Acetabular Defect Classification
- Bone Loss Pattern
- Minimal bone loss, intact hemisphere
- Rim Integrity
- Rim intact, supportive
- Treatment
- Standard hemispherical uncemented cup
- Bone Loss Pattern
- Superior or medial bone loss, distorted hemisphere
- Rim Integrity
- Rim partially supportive
- Treatment
- Hemispherical cup with medial graft or superior augment
- Bone Loss Pattern
- Superior migration under 3cm, teardrop intact
- Rim Integrity
- Rim supportive
- Treatment
- Hemispherical cup, possibly oversized (jumbo)
- Bone Loss Pattern
- Medial wall deficiency, migration into pelvis
- Rim Integrity
- Rim intact
- Treatment
- Hemispherical cup with medial augment or mesh
- Bone Loss Pattern
- Superior migration under 3cm, teardrop obscured
- Rim Integrity
- Rim partially supportive (over 50%)
- Treatment
- Jumbo cup with superior augment or graft, cages if needed
- Bone Loss Pattern
- Superior migration over 3cm, medial wall deficient
- Rim Integrity
- Rim minimally supportive (under 50%)
- Treatment
- Cup-cage construct, custom triflange, reconstruction ring
Key differentiator: Amount of supportive rim available. Type IIIA has over 50% host bone contact potential with jumbo cup. Type IIIB has under 50% contact, necessitating structural support. Migration over 3cm superior and medial wall deficiency = IIIB.
PAPROSKYPAPROSKY Acetabular Defect Classification
Hook:PAPROSKY guides acetabular reconstruction from simple cups (Type I) to complex cages (Type IIIB) based on rim integrity and migration!
Clinical Assessment
- Pain characteristics: Groin (acetabular), thigh (femoral), start-up vs activity
- Functional limitation: Walking distance, stairs, ADLs
- Previous surgeries: Number, approaches, complications, implant types
- Infection symptoms: Prolonged wound drainage, fevers, systemic illness
- Instability: Number of dislocations, mechanism, closed reduction success
- Gait: Trendelenburg (abductor insufficiency), antalgic, limb length
- Scars: Previous incisions, quality, sinuses
- Range of motion: Terminal flexion pain (loosening), restricted arc
- Abductor strength: Assess gluteus medius integrity
- Leg length discrepancy: Measure from ASIS to medial malleolus
- Neurovascular: Baseline documentation (femoral pulse, sciatic function)
Any of these warrant aspiration before revision:
- Wound drainage persisting over 6 weeks from primary surgery
- Recurrent atraumatic dislocations (infection destabilizes soft tissues)
- Early failure (under 5 years) without mechanical explanation
- Constitutional symptoms (fevers, night sweats, weight loss)
- Elevated inflammatory markers (CRP over 10, ESR over 30)
Missing occult infection and proceeding with aseptic revision leads to catastrophic outcomes.
Differential Diagnosis of the Painful Total Hip Arthroplasty
- Pain Pattern
- Rest and night pain, constant, early failure
- Key Discriminator
- Raised CRP/ESR, sinus, wound issues
- Confirmatory Test
- Aspiration: cell count, culture, alpha-defensin
- Pain Pattern
- Start-up pain; groin (cup) or thigh (stem)
- Key Discriminator
- Progressive radiolucency, migration, subsidence
- Confirmatory Test
- Serial radiographs; normal inflammatory markers
- Pain Pattern
- Episodic giving-way, mechanical
- Key Discriminator
- Documented dislocation, component malposition
- Confirmatory Test
- Radiographs of cup version/inclination, exam
- Pain Pattern
- Deep ache, swelling, clunk
- Key Discriminator
- Metal-on-metal or modular taper bearing
- Confirmatory Test
- Serum cobalt/chromium, MARS MRI for pseudotumour
- Pain Pattern
- Acute pain after fall, inability to weight-bear
- Key Discriminator
- Trauma history, deformity
- Confirmatory Test
- Radiographs (Vancouver classification)
- Pain Pattern
- Variable, may not relate to hip activity
- Key Discriminator
- Normal hip imaging, positive spine or peripheral signs
- Confirmatory Test
- Diagnostic intra-articular local anaesthetic, spine imaging
Periprosthetic joint infection is the single most important diagnosis to exclude in any painful THA before attributing symptoms to a mechanical cause. Proceeding with an aseptic revision in an unrecognised infected joint is a catastrophic error.
Functional Assessment Tools
Outcome Measures
100-point scale: pain (44), function (47), ROM (5), deformity (4). Score under 70 = poor, 70-79 = fair, 80-89 = good, 90-100 = excellent.
Western Ontario and McMaster Universities Osteoarthritis Index. 24 items covering pain, stiffness, function. Sensitive to change in revision.
12-item patient questionnaire. Score 0-48 (48 = best). Quick, validated for revision populations.
The Decision to Revise: Never Operate Without a Diagnosis
The differential table lists extrinsic and referred causes of a painful THA (spine, vascular, hernia, greater trochanteric pain syndrome) and points to a diagnostic intra-articular local anaesthetic, and the topic stresses excluding infection — but the single governing principle is never stated outright: revision should be offered only when a specific, correctable diagnosis has been established that matches the symptoms. Revising a painful THA for "unexplained pain," without a defined mechanical or infective cause, gives poor and unpredictable results and may leave the patient worse.
The systematic work-up of the painful THA, in order:
- Exclude infection first — CRP and ESR, then aspiration (cell count, differential, culture ± alpha-defensin) if raised or if there is any clinical suspicion. This is non-negotiable and underpins everything else (an unrecognised infected joint revised as "aseptic" is catastrophic).
- Exclude extrinsic / referred sources the differential lists — lumbar spine (radiculopathy/stenosis causing groin or thigh pain), vascular claudication, inguinal/femoral hernia, and greater trochanteric pain syndrome / abductor pathology — because none of these is cured by revising the hip.
- Confirm an intra-articular source — a diagnostic intra-articular local-anaesthetic injection that relieves the pain supports a true intra-articular cause; failure to relieve points away from the prosthetic hip.
- Define the specific failure mode — aseptic loosening, instability, adverse local tissue reaction / taper corrosion (serum cobalt-chromium, MARS MRI), periprosthetic fracture, or wear/osteolysis — with the imaging and tests above.
Only then operate, with the procedure matched to the diagnosis. If a thorough work-up yields no correctable diagnosis, do not revise — continue investigation, optimise non-operative measures, and observe.
Before recommending revision, you must have a specific, correctable diagnosis that explains the pain: exclude infection (CRP/ESR, aspiration), exclude referred causes (spine, vascular, hernia, GTPS), confirm an intra-articular source (diagnostic local-anaesthetic injection), and define the failure mode. Operating on unexplained pain is a classic trap with poor outcomes — no diagnosis means no revision.
Investigations
Imaging Protocol
Radiographic Workup
AP pelvis and lateral hip. Assess Paprosky classification, measure migration, evaluate bone loss. Full-length femur (AP) including knee to assess femoral canal and plan stem length.
45-degree obturator and iliac obliques. Assess posterior and anterior column integrity. Essential for detecting pelvic discontinuity. Iliac oblique shows anterior column, obturator shows posterior column.
3D reconstruction of pelvis and femur. Measure precise bone loss volumes. Plan custom implants (triflange). Gold standard for pelvic discontinuity detection. Essential for preoperative planning in Paprosky IIIB.
Metal artifact reduction sequences (MARS) for pseudotumor in metal-on-metal bearings. Assess soft tissue (abductor tears). Not routinely needed for standard aseptic loosening.
Laboratory Investigations
- Normal Value
- Under 10 mg/L
- Interpretation
- Elevated in infection but also loosening, metallosis
- Action
- If over 10: Aspiration recommended
- Normal Value
- Under 30 mm/hr
- Interpretation
- Less specific than CRP, elevated in many conditions
- Action
- If over 30: Aspiration recommended
- Normal Value
- WBC under 3000, PMN under 80%
- Interpretation
- Gold standard for infection diagnosis pre-revision
- Action
- Send cell count, culture, consider alpha-defensin
- Normal Value
- Negative
- Interpretation
- Biomarker with high sensitivity/specificity for PJI
- Action
- Adjunct when CRP/ESR equivocal, not first-line
MSIS Criteria for PJI Diagnosis: Two positive cultures OR one of: sinus tract, elevated synovial WBC (over 3000), elevated synovial PMN (over 80%), positive alpha-defensin, or positive histology.
Templating and Preoperative Planning
- Measure superior migration: Distance from teardrop to cup dome
- Assess medial wall: Kohler's line, teardrop integrity
- Classify defect: Paprosky I-IIIB based on rim integrity
- Plan implant: Hemispherical vs jumbo vs cage vs triflange
- Estimate size: Usually 2-4mm larger than primary cup
- Stem removal strategy: ETO if well-fixed, extraction if loose
- Canal diameter: Measure at isthmus and 4cm distal to stem
- Select stem type: Standard, extensively coated, modular tapered
- Plan length: Bypass defects by 2x diameter, minimum 4cm contact
- Restore offset: Template leg length and femoral offset

Management Algorithm

Decision Pathway by Paprosky Classification
Acetabular Reconstruction Strategy
Bone loss: Minimal, rim intact, hemisphere preserved. Treatment: Standard hemispherical uncemented cup. Ream to bleeding bone, under-ream 1-2mm for press-fit. Supplemental screws optional. Expected outcome: 85-90% survival at 10 years.
Bone loss: Superior or medial deficiency, distorted hemisphere, rim partially supportive. Treatment: Hemispherical cup (may be oversized) with medial bone graft (Type IIA) or superior support (Type IIB). Screws for supplemental fixation. Expected outcome: 80-85% survival at 10 years.
Bone loss: Superior migration under 3cm, teardrop obscured, over 50% rim supportive. Treatment: Jumbo cup (62-66mm) with superior metal augments or structural allograft. Multiple screws. Restore anatomic hip center. Expected outcome: 75-85% survival at 10 years.
Bone loss: Superior migration over 3cm, medial wall deficient, under 50% rim supportive. Treatment: Cup-cage construct (uncemented cup + Burch-Schneider cage) OR custom triflange (3D-planned flanges to ilium/ischium/pubis). If pelvic discontinuity: Column plating first. Expected outcome: 70-80% survival at 10 years.
Key Decision Point: Host bone contact potential determines implant selection. Over 50% contact = hemispherical cup achievable. Under 50% = structural support needed.
Surgical Technique
Surgical Approach Selection
- Advantages
- Extensile, excellent visualization, can extend distally
- Disadvantages
- Abductor detachment risk if extends too superior
- Best Use
- Most revision cases, especially femoral-sided work
- Advantages
- Gluteus medius preserved, lower dislocation if primary was AL
- Disadvantages
- Limited distal extension, abductor damage possible
- Best Use
- Acetabular-only revisions, preserve abductors
- Advantages
- Stable construct, good acetabular exposure
- Disadvantages
- Abductor disruption, Trendelenburg risk
- Best Use
- Isolated acetabular revisions with stable stem
- Advantages
- Avoids additional scars, preserves blood supply
- Disadvantages
- May not be optimal for revision exposure
- Best Use
- Default unless primary approach precludes adequate exposure
Key Principle: Extensile exposure is critical. Do not hesitate to extend incision distally for femoral access or proximally for acetabular exposure. Poor visualization leads to complications.
Complications
- Incidence
- 10-15% (vs 2-5% primary)
- Risk Factors
- Abductor insufficiency, malposition, bone loss limiting constraint
- Management
- Closed reduction, abduction brace. If recurrent: component revision to correct position or constrained liner
- Incidence
- 2-10% (higher with bone loss)
- Risk Factors
- Previous infection, wound issues, comorbidities, operative time over 3 hours
- Management
- Acute (under 3 weeks): Debridement, liner exchange, antibiotics. Chronic: Two-stage revision with spacer
- Incidence
- 5-15% at 10 years (higher for cementless cups in revision)
- Risk Factors
- Inadequate fixation, bone quality poor, infection
- Management
- Re-revision with increased bone loss. AOANJRR shows cemented cups have lower revision rate in revision setting
- Incidence
- 3-5%
- Risk Factors
- Osteoporosis, cortical perforation, ETO, forceful impaction
- Management
- Intraoperative: Cable fixation, extend stem. Postoperative: ORIF if stem stable, revision if loose
- Incidence
- 1-3% (sciatic most common)
- Risk Factors
- Leg lengthening over 4cm, posterior approach, retractor placement
- Management
- Most are neurapraxia - observation for 6-12 months. EMG at 6 weeks if no recovery. Surgical exploration rarely indicated
- Incidence
- 5-7%
- Risk Factors
- Inadequate fixation, patient noncompliance, infection
- Management
- If asymptomatic: Observation. If symptomatic: Revision cable fixation, bone grafting, protected weight-bearing
Key strategies:
- Exclude infection preoperatively - CRP, ESR, aspiration if any suspicion
- Avoid leg lengthening over 4cm - increases sciatic nerve stretch injury risk exponentially
- Plan component removal - ETO for well-fixed stems prevents perforation
- Restore hip center - superior migration increases dislocation and abductor insufficiency
- Obtain stable initial fixation - inadequate fixation leads to early loosening
Postoperative Care and Rehabilitation
Immediate Postoperative Period (Days 0-7)
DVT prophylaxis: Chemical (LMWH or rivaroxaban) + mechanical (sequential compression). Continue for 35 days. Pain management: Multimodal analgesia - paracetamol, NSAIDs if no contraindication, opioids as needed. Drain removal: When output under 30ml per 8 hours, typically 24-48 hours.
Weight-bearing status: Depends on fixation and bone quality.
- Standard revision (good fixation): Touch weight-bearing to partial weight-bearing
- Structural graft or cage: Touch weight-bearing for 6-12 weeks
- ETO: Partial weight-bearing for 6-12 weeks until union Mobilize with physiotherapy: Walker or crutches. Hip precautions if posterior approach.
Wound check: Monitor for drainage, erythema, dehiscence. Functional goals: Independent transfers, toilet, short distances with walking aid. Discharge criteria: Pain controlled, mobilizing safely, home supports arranged.
Hip Precautions (Posterior Approach): Avoid flexion over 90 degrees, adduction past midline, internal rotation for 6 weeks. Reduces dislocation risk from 15% to under 5%.
Outcomes and Prognosis
- Implant Strategy
- Hemispherical uncemented cup
- Survival at 10 Years
- 85-90%
- Notes
- Outcomes approach primary THA if good bone stock
- Implant Strategy
- Jumbo cup + augments
- Survival at 10 Years
- 75-85%
- Notes
- Augments provide better longevity than structural graft alone
- Implant Strategy
- Cup-cage or triflange
- Survival at 10 Years
- 70-80%
- Notes
- Custom triflange showing promising results in severe defects
- Implant Strategy
- Proximally coated stem
- Survival at 10 Years
- 90-95%
- Notes
- Excellent outcomes with modern cementless stems
- Implant Strategy
- Modular tapered long stem
- Survival at 10 Years
- 85-90%
- Notes
- Bypassing defect with distal fixation highly successful
Prognostic Factors
- Aseptic indication (no infection)
- Minimal bone loss (Paprosky I-II)
- Good bone quality (healthy host)
- First revision (not re-revision)
- Younger patient with good bone stock
- Previous infection (even if eradicated)
- Severe bone loss (Paprosky IIIB, IV)
- Multiple prior revisions (re-revision)
- Medical comorbidities (uncontrolled diabetes, immunosuppression)
- Abductor deficiency (increases instability)
AOANJRR findings:
- Cemented acetabular components have lower revision rate than cementless in revision setting (contrary to primary THA)
- Re-revision rate 35% at 10 years highlights difficulty of revision surgery
- Infection accounts for higher proportion of re-revisions (20%) compared to primary revisions (10%)
- Modular femoral stems have higher revision rate than monoblock stems in revision setting
These registry findings should guide implant selection and patient counseling.
Cemented vs Cementless Fixation in the Revision Setting
The registry observation that "cemented acetabular components have a lower revision rate than cementless in the revision setting" — the reverse of primary THA — is quoted throughout this topic, but the reason and its important caveat are never developed.
Why fixation behaves differently in revision. The revision bed is sclerotic, relatively avascular, often deficient and previously instrumented, so reliable biological ingrowth (on which cementless fixation depends) is harder to achieve than in healthy primary bone. That mechanistic disadvantage is why older registry signals (AOANJRR) favoured cemented cups in revision. Equally, cementing into a smooth, sclerotic old canal/socket gives poor cement interdigitation, so primary-style cement fixation is also less reliable — the fundamental problem in revision is the host bone, not the fixation mode per se.
The major caveat — highly-porous metals. Modern highly-porous cementless cups and augments (trabecular metal / tantalum) achieve ingrowth even in deficient bone and have substantially narrowed (or reversed) the historical cemented advantage; much of the old "cemented is better in revision" registry signal reflects earlier, less-porous cementless designs. So treat it as a registry generalisation, not an absolute law.
Practical fixation strategy (match fixation to bone):
- Acetabulum: a highly-porous cementless hemispherical cup when there is ≥50% host-bone contact and a stable press-fit is achievable; when structural support is needed (cup-cage / reconstruction ring) a polyethylene liner is cemented into the cage; a cemented cup alone into deficient sclerotic bone loosens early and is reserved for low-demand elderly patients or cementing into a cage.
- Femur: revision is dominated by cementless extensively porous-coated or modular fluted tapered stems achieving distal diaphyseal fixation; cemented femoral revision retains a defined role — notably impaction bone grafting into a contained canal (the Exeter/UK–Netherlands tradition, routed to the bone-loss reconstruction topic) and the elderly poor-bone patient — but not primary-style cementing into a bare sclerotic canal.
Registries (AOANJRR) historically show cemented cups outperform cementless in revision — the opposite of primary THA — because the deficient, sclerotic, avascular revision bed makes biological ingrowth unreliable. But highly-porous metals (trabecular metal/tantalum) have largely closed that gap. Match fixation to bone: highly-porous cementless where host bone supports ingrowth (≥50% contact), and structural support (cage with a cemented liner) or cement-into-contained-graft where it does not.
Guidelines, Registries & Global Practice
Global Epidemiology and Failure Modes
- Finding
- US total hip revisions projected to grow 137% between 2005 and 2030; demand to double by 2026
- Source
- Kurtz, JBJS Am 2007 (PMID 17403800)
- Finding
- Instability/dislocation 22.5%, mechanical loosening 19.7%, infection 14.8% (51,345 revisions)
- Source
- Bozic, JBJS Am 2009 (PMID 19122087)
- Finding
- Approximately 18% cumulative percent revision at 15 years after primary THA; re-revision risk much higher
- Source
- AOANJRR Annual Report
- Finding
- Single-dose prophylaxis as effective as multiple doses for PJI prevention
- Source
- Tan, JBJS Am 2019 (PMID 30845037)
Guideline and Registry Positions (Side-by-Side)
- Region
- USA
- Key Position
- Rule out infection before assuming aseptic failure; restore hip centre; classify bone loss to guide reconstruction
- Evidence Basis
- Clinical practice guidance / consensus
- Region
- Global
- Key Position
- Standardised PJI definition and workup (serum CRP/ESR, aspiration with cell count and culture, biomarkers); two-stage exchange for chronic PJI
- Evidence Basis
- Delphi consensus, multinational
- Region
- United Kingdom
- Key Position
- Revision arthroplasty concentrated in higher-volume units/networks; structured infection pathways and MDT decision-making
- Evidence Basis
- Guidance and best-practice standards
- Region
- Europe / Australia / USA
- Key Position
- Mandatory implant and outcome capture; survival benchmarking informs implant selection in revision
- Evidence Basis
- Observational registry data
Reconstruction philosophy varies by region: trabecular-metal/cup-cage constructs and custom triflanges are favoured in North America and Australasia, whereas impaction bone grafting (Exeter/Sloof-Ling technique) has a strong tradition in the UK and the Netherlands for contained defects. Across all systems the constants are the same: exclude infection, classify bone loss (Paprosky), restore the hip centre, and obtain stable fixation that bypasses the defect.
Hospital Systems Considerations
Revision THA Pathway in Australian Public Hospitals
Symptomatic loosening typically triaged as Category 2 (target treatment within 90 days). Severe pain or bone loss threatening viability may warrant Category 1 (urgent, within 30 days).
Mandatory: CRP, ESR, radiographs (AP pelvis, lateral hip, full femur), hip aspiration if inflammatory markers elevated. CT scan if complex bone loss. Cardiac and anesthesia clearance.
Length of stay: Average 5-7 days vs 2-3 for primary. Blood cross-match 2-4 units. DVT prophylaxis 35 days. Physiotherapy daily. Occupational therapy for home modifications.
Supports: Arrange home modifications, community physiotherapy, walking aids. Follow-up at 6 weeks, 3 months, 12 months, then annually. Registry reporting.
Key documentation requirements:
- Informed consent must include: Higher complication rates than primary (dislocation 10-15%, infection 5-10%, nerve injury 1-3%), re-revision risk 35% at 10 years, prolonged recovery 6-12 months, leg length discrepancy possibility
- Preoperative infection workup: Document CRP, ESR results. If aspiration performed, document indication and results. Failure to exclude infection before aseptic revision is major litigation risk
- Component selection rationale: Document why specific implant chosen (e.g., "Paprosky IIIA defect - jumbo cup with superior augment selected to restore hip center")
- Intraoperative complications: If perforation, fracture, or nerve injury occurs, document immediately and inform patient postoperatively
Common litigation issues:
- Unrecognized infection revised as aseptic (catastrophic outcome)
- Sciatic nerve injury from excessive leg lengthening (document leg length measured intraoperatively)
- Recurrent dislocation (document component position optimization and abductor repair)
- Early re-revision (document bone quality and fixation achieved)
Comprehensive documentation and realistic patient expectations are essential medicolegal protection.
MCQ Practice Points
Q: A 65-year-old patient has acetabular component loosening with superior migration of 3.5cm and medial wall deficiency. What Paprosky classification is this? A: Paprosky Type IIIB. Type IIIB is defined by superior migration over 3cm and typically includes medial wall deficiency. This differs from Type IIIA which has migration under 3cm. Type IIIB requires structural support (cage or triflange) whereas Type IIIA can often be managed with jumbo cup and augments.
Q: What is the minimum length an Extended Trochanteric Osteotomy should extend distal to the tip of a well-fixed femoral stem? A: The ETO should extend at least to the tip of the stem, and preferably 1-2cm beyond to allow adequate access for stem extraction. The total length is typically 10-15cm. The new revision stem must bypass the osteotomy by at least 2x the stem diameter distally to prevent stress concentration.
Q: According to AOANJRR data, what is the approximate re-revision rate at 10 years after first revision THA? A: 35% at 10 years. This highlights that revision THA has significantly worse outcomes than primary THA (18% revision rate at 15 years). Re-revision risk increases with each subsequent surgery, emphasizing importance of getting the first revision right and counseling patients appropriately.
Q: What is the most common nerve injured during revision THA and what is the primary risk factor? A: Sciatic nerve is most commonly injured (1-3% incidence). Primary risk factor is leg lengthening over 4cm, which causes traction injury to the nerve. Risk increases exponentially with lengthening beyond 4cm. Other risk factors include posterior approach and prolonged retractor placement.
Q: What is the threshold for host bone contact with a hemispherical cup below which structural support (cage) is typically required? A: Under 50% host bone contact typically requires structural support with a cage, reconstruction ring, or custom triflange. This corresponds to Paprosky Type IIIB defects. Over 50-70% contact (Type IIIA) can usually be managed with jumbo cup and augments alone.
Q: According to AOANJRR, do cemented or cementless acetabular components have better survival in the revision THA setting? A: Cemented acetabular components have lower revision rates than cementless in the revision setting according to AOANJRR data. This is contrary to primary THA where cementless cups perform better. The finding suggests biological fixation is more difficult to achieve in deficient bone, and cement may provide more reliable initial stability.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman presents with progressive groin pain 12 years after primary THA. Radiographs show superior migration of the acetabular component by 2.5cm, with obscured teardrop. The femoral stem is well-fixed. CRP is 8, ESR is 25. How would you assess and manage this patient?”
“You are planning revision THA for a 72-year-old man with aseptic loosening of the acetabular component. The femoral stem is well-fixed and extensively porous-coated. Walk me through your approach to femoral component removal and reconstruction.”
“Intraoperatively during revision THA, after removing a loose acetabular component, you discover severe superior and medial bone loss with independent motion between anterior and posterior columns. How do you proceed?”
Key Classifications
- Paprosky Acetabular: Type I (intact rim), Type II (distorted, superior/medial loss), Type IIIA (migration under 3cm, over 50% rim), Type IIIB (migration over 3cm, under 50% rim)
- Paprosky Femoral: Type I (minimal loss), Type II (metaphyseal loss, diaphysis intact), Type IIIA (diaphysis over 4cm intact), Type IIIB (diaphysis damaged), Type IV (extensive loss)
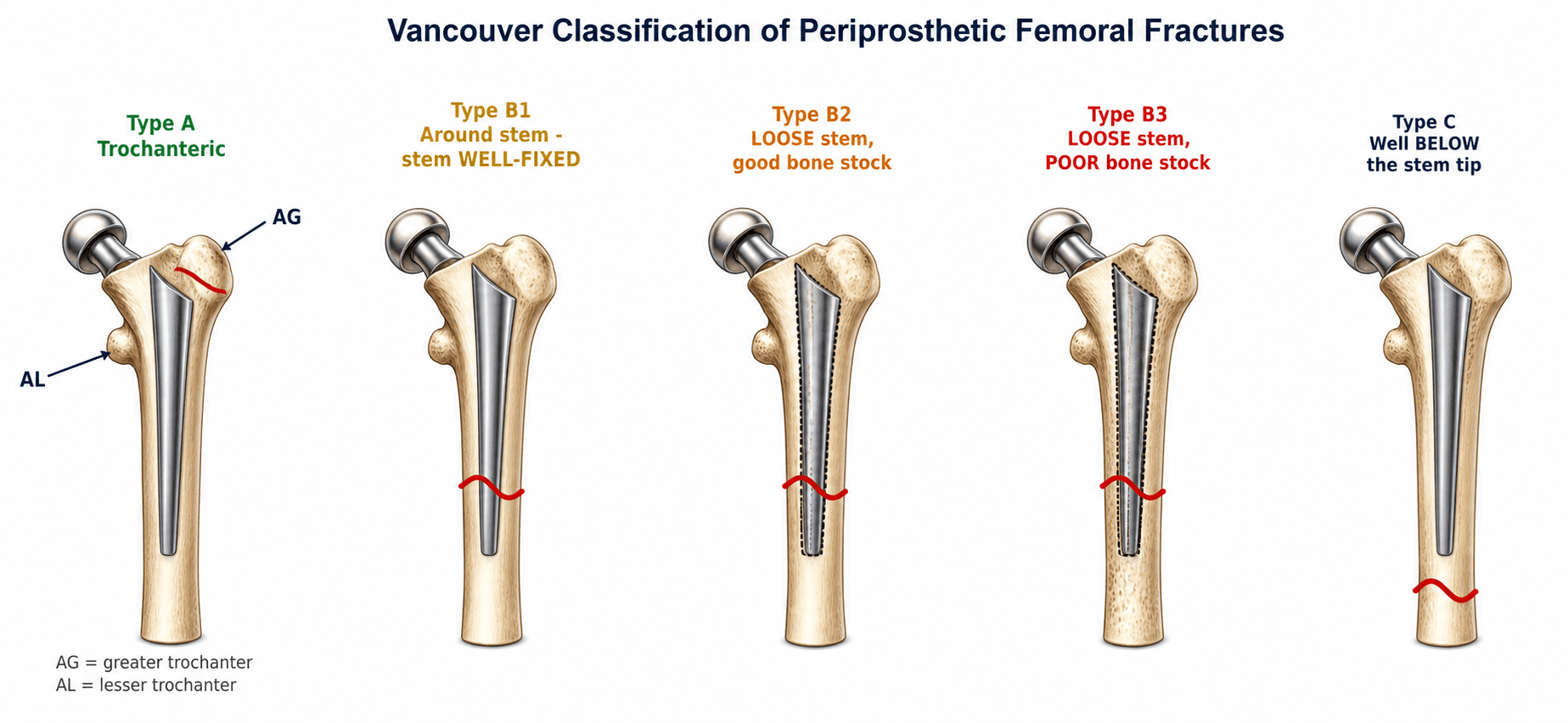
- Vancouver Fracture: A (trochanteric, stem stable), B1 (around stem, stable), B2 (around stem, loose), B3 (loose with poor bone), C (distal to stem)
- Pelvic discontinuity = independent column motion, requires plating + cage/triflange
Surgical Approach
- Type I-II acetabular: Hemispherical uncemented cup, ream to bleeding bone, under-ream 1-2mm
- Type IIIA acetabular: Jumbo cup (over 62mm) + superior augments or structural graft, restore hip center
- Type IIIB acetabular: Cup-cage construct or custom triflange, requires structural support
- ETO for well-fixed femoral stem: 10-15cm distal to tip, anterior 1/3, posterior hinge, minimum 3 cables, bypass 2x diameter
Critical Steps
- ALWAYS exclude infection: CRP/ESR, aspiration if elevated or suspicious
- Plan component removal before incision: ETO for well-fixed stems prevents perforation
- Restore anatomic hip center: Superior migration leads to abductor insufficiency
- Achieve stable initial fixation: Inadequate fixation = early loosening
- Minimum 4cm diaphyseal contact for femoral stems, bypass defects by 2x diameter
Surgical Pearls
- Jumbo cups need over 50% host bone contact for success without cage
- Metal augments have lower resorption than structural allograft
- ETO union rate over 90% with cable fixation, nonunion risk 5-7%
- Constrained liners for recurrent instability have 5-8% failure at 5 years
- Leg lengthening over 4cm increases sciatic nerve injury risk exponentially
Complications
- Dislocation 10-15% (vs 2-5% primary) - malposition, abductor insufficiency
- Infection 2-10% (higher with bone loss, operative time over 3 hours)
- Nerve injury 1-3% (sciatic from lengthening over 4cm)
- Re-revision 35% at 10 years (counsel patients about high failure rate)
- ETO nonunion 5-7% (protected weight-bearing 6-12 weeks)
Evidence Base and Key Trials
Epidemiology and Projected Burden of Revision THA
- US Nationwide Inpatient Sample of 51,345 revision THAs: most common causes were instability/dislocation 22.5%, mechanical loosening 19.7% and infection 14.8%
- All-component revision was the most frequent procedure type (41.1%)
- Companion projection study (Kurtz, JBJS Am 2007, PMID 17403800, DOI 10.2106/JBJS.F.00222) forecasts US total hip revisions to grow 137% between 2005 and 2030
- Demand for hip revision projected to double by 2026
- Provides the quantitative basis for workforce and resource planning
Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR)
- Approximately 18% cumulative percent revision at 15 years for primary conventional THA
- Re-revision rates after a first revision are substantially higher than after primary THA
- Loosening/lysis and dislocation are leading recorded reasons for revision
- Cemented and hybrid fixation perform well in many revision and older-patient subgroups
- Mandatory near-complete national capture of arthroplasty procedures
Paprosky Acetabular Defect Classification (Landmark)
- Original description of the acetabular defect classification (Types 1 to 3A/3B) on 147 cemented cups revised to cementless press-fit components
- Mean follow-up 5.7 years; classification based on degree of superior, medial and rim bone loss
- Only 6 of 147 components (4.0%) were unstable, all Type 3B, confirming structural support is required for the most severe defects
- Adequate remaining host bone is essential for ingrowth of hemispherical components
- Defined the framework still used to plan acetabular reconstruction strategy
Extended Trochanteric Osteotomy in Aseptic Revision THA: Systematic Review
- Systematic review of 19 studies including 1,478 extended trochanteric osteotomies
- Mean overall union rate 93.1% (1,377 of 1,478 cases)
- Radiographic femoral stem subsidence greater than 5mm in 7.1%
- Union and subsidence rates similar between periprosthetic fracture and non-fracture revisions
- Trochanteric plate with cables recommended as first-choice fixation
Extra-large Uncemented Hemispherical (Jumbo) Cups for Revision THA
- 89 extra-large uncemented hemispherical cups (66mm or larger in men, 62mm or larger in women) for acetabular revision with bone loss
- Survivorship 93% at 8 years with removal for any reason as the endpoint; 98% with aseptic loosening as the endpoint
- Mean modified Harris hip score improved from 56 to 83 points (mean follow-up 7.2 years)
- All four sockets that loosened had combined cavitary and segmental bone loss
- Dislocation was the most frequent complication (11 of 89 hips)
Custom Triflange Acetabular Component for Pelvic Discontinuity
- 28 patients (30 hips) with failed THA and pelvic discontinuity treated with a CT-based custom porous-coated triflange prosthesis
- 20 hips followed for a mean of 10 years; no component was revised
- Definite healing of the discontinuity (bridging callus) in 18 of 20 hips, with no broken screws or implant migration
- Mean Harris hip score improved from 41 to 80 points
- Five patients had one or more postoperative dislocations
Perioperative Antibiotic Prophylaxis in Total Joint Arthroplasty
- Retrospective study of 20,682 primary total joint arthroplasties comparing single-dose versus multiple-dose antibiotic prophylaxis
- PJI rate 0.60% with a single dose versus 0.88% with multiple doses
- No significant difference on univariate, multivariate or propensity-matched analysis
- No additional benefit of multiple doses even in patients at high preoperative PJI risk
- Supports that prophylactic antibiotics after skin closure may not be required for primary TJA
Treatment of Acetabular Defects with Pelvic Discontinuity (Paprosky/Sporer)
- Defines the treatment algorithm for pelvic discontinuity based on healing potential and biologic ingrowth potential
- If the discontinuity can heal: treat in compression with a posterior column plate plus structural allograft or trabecular metal acting as an internal plate
- If healing potential is absent: bridge and treat in distraction with a cage, trabecular metal with augmentation, or a custom triflange
- Prompt intraoperative recognition of discontinuity is essential for success
- Established the distraction/cup-cage concept widely used today