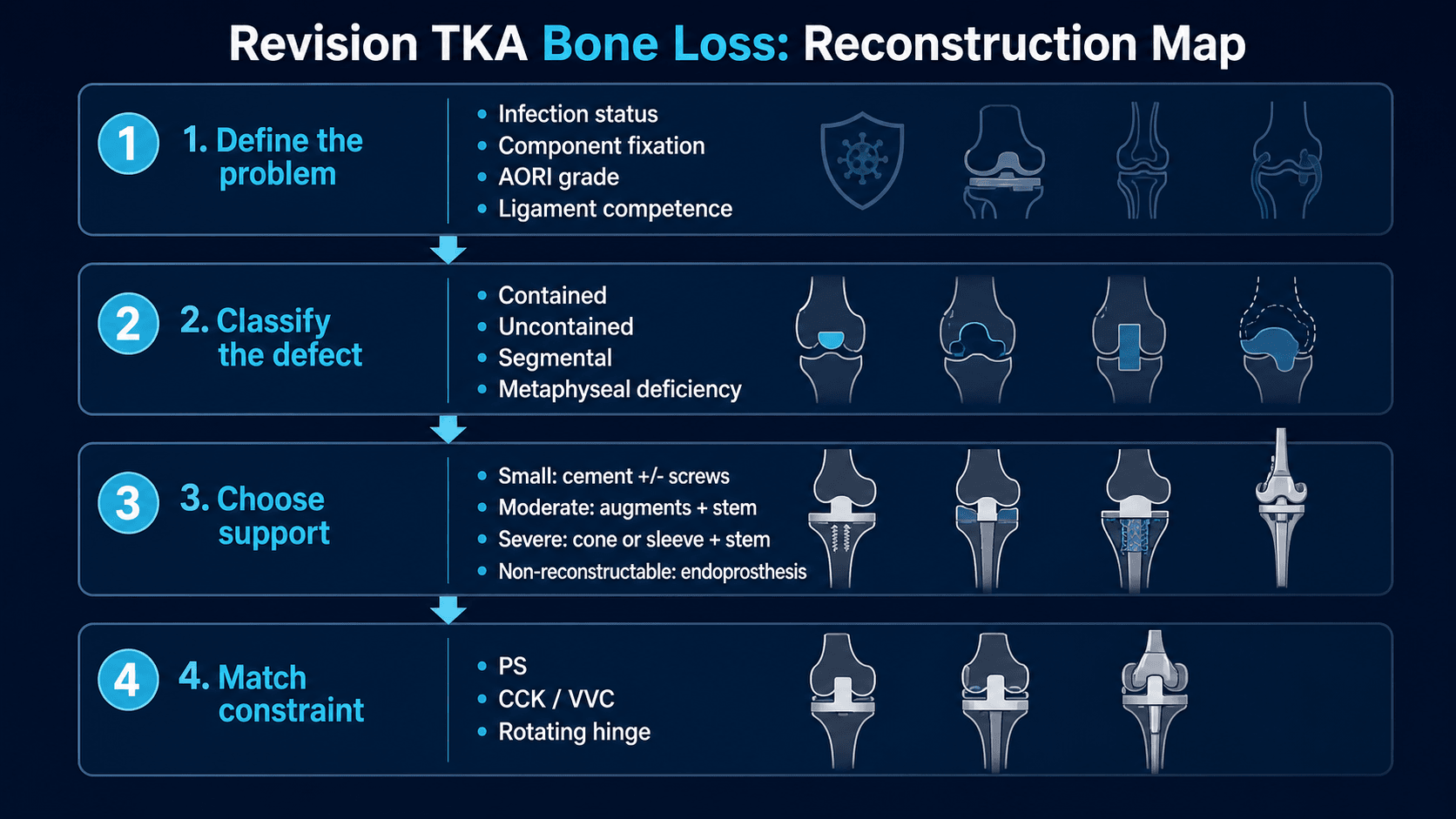
Map the defect | rebuild support | fix in zones | constrain only what remains unstable
- Bone loss is classified after implant removal. Pre-operative radiographs often underestimate the final defect.
- The reconstruction must restore a stable platform before constraint is chosen. Constraint cannot rescue poor fixation or unrecognised infection.
- Small contained defects can be filled. Larger uncontained defects need structural support rather than cement alone.
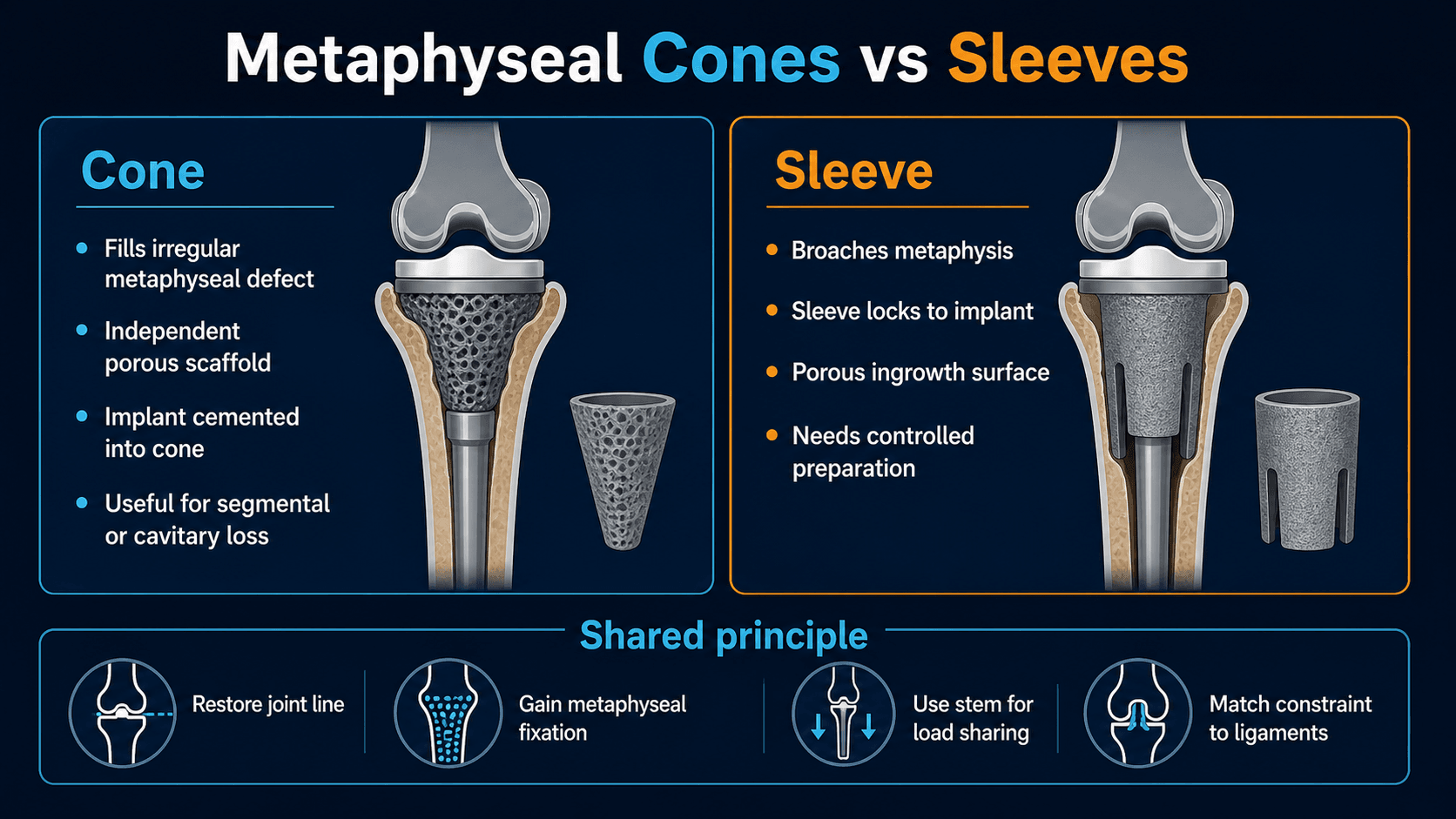
- Metaphyseal fixation is central in modern revision TKA. Cones and sleeves convert deficient metaphysis into a load-sharing support zone.
- Stem extensions are used for load sharing and alignment control. Cemented, cementless and hybrid fixation each have tradeoffs.
- “AORI is useful because it links defect severity to reconstruction choice; it is not just a naming system.
- “Use augments for peripheral segmental loss when the remaining platform can still support the component.
- “Use a cone when the defect is irregular and the implant needs an independent porous scaffold; use a sleeve when controlled broaching can obtain metaphyseal press-fit with an implant-linked sleeve.
- “Choose CCK or hinge based on residual ligament competence after bone loss and joint line have been reconstructed.
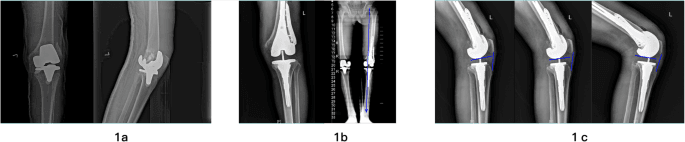
The true bone defect is often larger after components, cement, fibrous membrane and osteolytic debris are removed. The operation should be planned with backups, but the final reconstruction is decided after clean explantation, defect mapping and trial stability assessment.
- Reconstruction
- Cement with or without screws, morselised graft in selected contained defects, standard stemmed revision component if required.
- Constraint Implication
- PS or low constraint if ligaments and gaps are stable.
- Reconstruction
- Modular metal augment plus stem extension; restore joint line and platform.
- Constraint Implication
- PS or CCK depending collateral competence and gap balance.
- Reconstruction
- Porous metal cone or metaphyseal sleeve plus stem; build a stable metaphyseal support zone.
- Constraint Implication
- Often CCK; hinge if global ligament insufficiency remains.
- Reconstruction
- Rotating hinge, distal femoral replacement, proximal tibial replacement or tumour-style reconstruction in selected cases.
- Constraint Implication
- High constraint is part of the reconstruction, not a substitute for fixation.
- Reconstruction
- Culture strategy, debridement and infection pathway; one-stage or staged revision depends on organism, host, soft tissue and local practice.
- Constraint Implication
- Constraint is decided at reimplantation after defect and soft tissues are reassessed.
MAPBefore reconstruction | FILLDefect strategy | ZONESFixation target |
|---|---|---|
M Mechanism Loosening, infection, wear osteolysis, fracture, instability or previous revision. | F Fill contained loss Cement, screws or graft only when walls and support remain. | Z Zone 1 Epiphyseal platform: augments, cement and component surface. |
A AORI after explant Final grade is assigned after implant and cement removal. | I Increase support Augments for peripheral segmental loss. | O Zone 2 Metaphysis: cones, sleeves and porous ingrowth. |
P Platform Restore a stable tibial and femoral platform before judging constraint. | L Load share Stems and metaphyseal fixation reduce interface overload. | N Zone 3 Diaphysis: stem alignment and load sharing. |
L Link constraint Constraint follows residual ligament competence. | E Evaluate Check fixation, gaps, rotation and joint line during trialling. | |
S Stabilise Use the least constraint that controls the reconstructed knee. | ||
Map before rebuilding. | Fill small defects; support large defects. | Aim for stable fixation in multiple zones. |
Overview and Epidemiology
Revision TKA bone loss is the loss of femoral or tibial host bone that prevents a revision component from obtaining reliable support at the joint surface. It may be cavitary, segmental, contained, uncontained, metaphyseal, diaphyseal, traumatic, infective or iatrogenic.
The practical issue is simple: a revision knee fails if the surgeon restores an implant surface without restoring the bone platform underneath it. Bone loss affects fixation, joint line, offset, ligament tension, constraint choice, extensor mechanism mechanics and the risk of repeat loosening.
Common settings include:
- Aseptic loosening with progressive implant migration.
- Polyethylene wear with osteolysis.
- Periprosthetic joint infection with bone and soft-tissue compromise.
- Instability with asymmetric overload and component failure.
- Periprosthetic fracture or component extraction damage.
- Multiple previous revisions with combined bone and ligament deficiency.
The important question is not only “how big is the defect?” The important question is “where can this knee obtain durable fixation after the defect is reconstructed?” That is why modern revision planning uses AORI classification together with the zonal fixation concept.
Anatomy and Fixation Concepts
Revision TKA fixation can be understood in three zones. A durable construct usually uses more than one zone, especially when constraint is increased.
- Anatomy
- Joint-adjacent condyles, tibial plateau, remaining cortical rim and cancellous platform.
- Revision Reconstruction Role
- Component support, metal augments, cement fill, screws, graft and joint-line restoration.
- Anatomy
- Flared cancellous bone below the femoral condyles or tibial plateau.
- Revision Reconstruction Role
- Porous metal cone or sleeve fixation; major load-sharing zone for AORI 2B and 3 defects.
- Anatomy
- Femoral or tibial shaft engaged by the stem.
- Revision Reconstruction Role
- Alignment control, load sharing and bypass of metaphyseal deficiency.
Important mechanical principles:
- The epiphyseal platform sets joint line, flexion-extension gaps and component seating.
- The metaphysis provides broad load transfer; when deficient, cones and sleeves reconstruct this region.
- The diaphysis can guide alignment and reduce interface strain through stem extension.
- Higher constraint transmits higher forces to fixation interfaces, so fixation must be stronger when constraint increases.
- Offset stems, augments and sleeves may be needed to avoid forcing malposition just to make a stem fit the canal.
Pathophysiology
Bone loss develops through mechanical, biological and surgical mechanisms. The mechanism matters because it predicts the soft-tissue envelope and the reconstruction risk.
- Typical Defect
- Cavitary metaphyseal defects, sometimes with preserved cortical shell.
- Planning Consequence
- Assess containment. Graft or cement may work only if support remains; large cavitary loss often needs cone or sleeve.
- Typical Defect
- Progressive migration, uncontained tibial plateau or femoral condylar loss.
- Planning Consequence
- Plan augments, stems and metaphyseal support; look for joint-line change.
- Typical Defect
- Bone destruction, membrane, sinus risk, compromised soft tissue and poor biology.
- Planning Consequence
- Treat infection pathway first; reconstruction may be staged and more constrained.
- Typical Defect
- Eccentric overload, polyethylene wear, collateral stretching and segmental collapse.
- Planning Consequence
- Reconstruct bone and diagnose ligament competence before choosing CCK or hinge.
- Typical Defect
- Iatrogenic cortical perforation, condylar fracture or metaphyseal loss.
- Planning Consequence
- Use extraction tools carefully and have cones, sleeves, augments, stems and fracture fixation available.
- Typical Defect
- Bone loss plus disrupted cortical tube and possible implant loosening.
- Planning Consequence
- Combine fracture fixation principles with revision fixation; bypass defects and stress risers.
Classification
AORI is the common language for revision TKA bone defects. It is assigned separately for femur and tibia after implant removal, because cement, membrane, fibrous tissue and loose components can hide the true defect.
- Bone Loss
- Metaphyseal bone intact. Minor contained cancellous loss or small defects.
- Typical Reconstruction
- Cement, screws, morselised graft in selected contained defects, standard revision component or short stem if needed.
- Bone Loss
- Metaphyseal bone damaged in one femoral condyle or one tibial plateau.
- Typical Reconstruction
- Metal augment, cement and stem. Consider cone or sleeve if remaining metaphysis is weak.
- Bone Loss
- Metaphyseal bone damaged in both condyles or both tibial plateaus.
- Typical Reconstruction
- Cone or sleeve commonly required, plus stem and modular augments.
- Bone Loss
- Metaphyseal segment deficient or non-supportive, often with ligament compromise.
- Typical Reconstruction
- Cone or sleeve with stem if reconstructable; hinge or segmental replacement if bone and ligaments are not salvageable.
Clinical Presentation and Examination
Patients do not present saying they have AORI 2B bone loss. They present with a failed knee arthroplasty. Bone loss is suspected when symptoms, imaging or implant history suggest loosening, migration, osteolysis or major instability.
History
Ask for:
- Original arthroplasty indication, date, approach and implant type.
- Pain pattern: start-up pain suggests loosening; constant inflammatory pain raises concern for infection.
- Instability: giving way, coronal thrust, recurrent effusion, stairs difficulty or inability to trust the knee.
- Infection history: wound leakage, previous debridement, antibiotics, sinus, fevers, dental or systemic infection history.
- Previous revisions, retained hardware, stems, augments or cones/sleeves.
- Falls or fracture symptoms.
- Function, walking aids, stair ability and realistic goals.
- Medical risk: diabetes, obesity, renal disease, immunosuppression, smoking, anticoagulation, vascular disease.
Examination
Inspect:
- Gait, thrust, flexion contracture, recurvatum and walking aid dependence.
- Scars, sinus, skin quality, soft-tissue envelope and extensor mechanism.
- Limb alignment, joint-line height and patellar position.
Palpate and move:
- Effusion, warmth, tenderness, extensor lag and painful range.
- Varus-valgus opening at full extension, 30 degrees and 90 degrees.
- AP instability at 90 degrees.
- Rotational maltracking and patellar instability.
- Neurovascular status, especially peroneal nerve function and distal pulses.
A painful loose revision knee is infected until proven otherwise. Normal-looking skin and absence of fever do not exclude periprosthetic joint infection. Infection status must be settled before an aseptic bone-loss reconstruction is planned.
Differential Diagnosis of the Failing or Painful TKA
Bone loss is a consequence of a failure mode, never the diagnosis itself. The single most important step is identifying why the knee has failed, because the cause dictates whether reconstruction is even appropriate. A painful TKA with no identifiable failure mechanism is a relative contraindication to revision; revising for unexplained pain has poor outcomes.
- Discriminating Features
- Constant rest and night pain, early failure, effusion, raised inflammatory markers, prior wound problems or sinus.
- Key Test or Action
- ESR, CRP, D-dimer, synovial aspiration with cell count, differential, culture and alpha-defensin per MSIS/EBJIS criteria.
- Discriminating Features
- Start-up and weight-bearing pain, progressive radiolucency, migration or subsidence on serial films.
- Key Test or Action
- Serial weight-bearing radiographs; exclude infection before labelling aseptic.
- Discriminating Features
- Giving way, recurrent effusion, mid-flexion or coronal laxity, polyethylene wear.
- Key Test or Action
- Stress examination at 0, 30 and 90 degrees; assess gap balance and constraint level.
- Discriminating Features
- Late effusion, synovitis, expanding lucent lesions, often a well-fixed component.
- Key Test or Action
- Compare serial films for lytic progression; CT for osteolysis mapping.
- Discriminating Features
- Trauma history, acute pain, deformity, cortical break adjacent to component.
- Key Test or Action
- Full-length radiographs; CT if occult; assess implant fixation.
- Discriminating Features
- Extensor lag, inability to straight-leg raise, high or low patella, palpable defect.
- Key Test or Action
- Active extension test; lateral radiograph for patellar height; ultrasound or MARS imaging.
- Discriminating Features
- Anterior knee pain, stiffness, patellar maltracking, asymmetric wear.
- Key Test or Action
- CT rotational profile; assess component position and joint line.
- Discriminating Features
- Pain not matching examination, normal implant, radicular or hip features.
- Key Test or Action
- Examine hip and spine; vascular assessment; consider CRPS and neuroma.
If no failure mechanism is identified after a full infection and mechanical workup, do not revise. An undiagnosed painful TKA revised in hope rarely improves and may worsen. Identify the diagnosis first, then plan reconstruction.
Investigations
The investigation plan must answer four questions: is the knee infected, are the components loose or malpositioned, how much bone loss is present, and what implants/extraction tools are required?
- How To Order It
- Include the entire component and compare with prior films.
- What It Decides
- Radiolucency, migration, subsidence, osteolysis, patellar height, joint line and gross bone loss.
- How To Order It
- Hip-knee-ankle standing alignment view.
- What It Decides
- Mechanical axis, extra-articular deformity, stem planning and alignment correction.
- How To Order It
- Image the entire stem and canal.
- What It Decides
- Stem length, canal diameter, cortical defects, retained hardware and bypass planning.
- How To Order It
- Follow local periprosthetic joint infection pathway.
- What It Decides
- Aseptic reconstruction versus infection revision strategy.
- How To Order It
- Use when osteolysis, rotation, fracture, major bone loss or stem/canal planning is uncertain.
- What It Decides
- Defect extent, cortical shell, component rotation, occult fracture and underestimated tibial/femoral bone loss.
- How To Order It
- Obtain operation notes, labels and prior imaging.
- What It Decides
- Compatible extraction tools, cone/sleeve system, stem offset, augments and backup constraint.
Recent work on elective aseptic revision TKA confirms what revision surgeons see in theatre: major intra-operative defects can be underestimated pre-operatively. The theatre plan should include backup augments, cones, sleeves, stems and constraint even when the radiograph looks manageable.
Management
Management is a sequence, not a list of implants. The correct plan depends on infection status, host bone, defect shape, ligament competence, extensor mechanism, patient physiology and available implants.
Non-operative treatment is usually for patients who are medically unfit, have low functional demand, decline surgery or need temporary optimisation before revision. It is not definitive treatment for progressive loosening with major bone loss in a fit patient.
Options include:
- Activity modification and walking aids.
- Analgesia and management of inflammatory flares.
- Bracing for instability when surgery is not suitable.
- Infection suppression only when advised by the infection team and curative surgery is not appropriate.
- Optimisation of nutrition, glycaemic control, smoking cessation, anaemia, dental/skin sources and vascular status before surgery.
Failure signs include increasing pain, progressive migration, worsening instability, recurrent falls, fracture risk, sinus or systemic infection features.
Stems and Constraint
- Advantages
- Immediate fixation, useful in poor bone or wide canals, antibiotic cement option in selected cases.
- Tradeoffs
- Difficult extraction, stress transfer, cement removal burden at re-revision.
- Advantages
- Diaphyseal engagement, easier metaphyseal cement control, potential biological fixation.
- Tradeoffs
- Canal pain, end-of-stem stress, alignment dictated by canal unless offset stems are used.
- Advantages
- Cement at metaphyseal/component interface with press-fit diaphyseal stem.
- Tradeoffs
- Requires accurate canal preparation and compatible implant geometry.
- Advantages
- Allows component position to be independent of canal centre.
- Tradeoffs
- Adds complexity and requires careful trialling.
- Use When
- PCL absent but collaterals are competent and gaps are balanced.
- Do Not Use As
- A solution for collateral insufficiency.
- Use When
- Mild to moderate coronal laxity after reconstruction, collateral attenuation but not global deficiency.
- Do Not Use As
- A substitute for uncorrected malalignment or unsupported bone loss.
- Use When
- Global instability, severe collateral insufficiency, major AORI 3 defects, extensor/soft-tissue risk requiring high constraint.
- Do Not Use As
- A shortcut for poor exposure, poor platform reconstruction or uncertain infection.
- Use When
- Non-reconstructable distal femur or proximal tibia with major bone and ligament loss.
- Do Not Use As
- Routine treatment for reconstructable AORI 2B defects.
A high-yield revision-TKA concept the trial section names but does not explain: mid-flexion instability is laxity through the middle of the arc (roughly 30-60 degrees) in a knee that is stable in full extension and at 90 degrees. It is not simple flexion or extension gap imbalance - it is a collateral-isometry problem created by component position:
- The dominant cause is an elevated (proximalised) joint line - if the distal femoral joint line is raised (e.g. distal bone loss compensated by thick polyethylene rather than distal augments), the collateral ligaments are no longer isometric through the arc, becoming lax in mid-flexion.
- Femoral component downsizing/anteriorisation (loss of posterior offset / a small AP femur) similarly disturbs mid-arc collateral tension.
The critical exam point: mid-flexion instability is corrected by fixing the geometry - restore the joint line (distal femoral augments), restore femoral AP size and posterior offset (posterior augments), and correct component position - NOT by reflexively jumping up the constraint ladder. Adding a CCK or hinge over an elevated joint line masks the error and overloads fixation; constraint is for true collateral deficiency, not for a malpositioned reconstruction.
Exam point: laxity in mid-flexion with stability at 0 and 90 degrees = mid-flexion instability from joint-line elevation / femoral undersizing - restore the joint line and femoral geometry first; do not treat it as a reason to escalate constraint.
Surgical Technique
Position and setup
- Supine on a radiolucent table if intra-operative imaging may be needed.
- Tourniquet available; use depends on vascular status, surgeon preference and expected duration.
- Prepare the whole limb from groin to foot.
- Have extraction tools, flexible osteotomes, saws, burrs, cables, plates and stems available.
- Confirm availability of augments, cones, sleeves, CCK, hinge, segmental replacement and backup polyethylene sizes.
Exposure
- Use the previous midline incision where possible, respecting skin bridges.
- Develop full-thickness flaps only as much as necessary.
- Standard medial parapatellar arthrotomy is common.
- Extensile exposure options include quadriceps snip, V-Y turndown or tibial tubercle osteotomy.
- Choose extensile exposure early rather than avulsing the patellar tendon during forced eversion.
The patella is easy to ignore in a bone-loss revision but is a recurring exam and clinical pitfall:
- Patella baja / pseudo-patella baja: revision tends to elevate the joint line, which makes the patella sit relatively low (pseudo-baja) - causing impingement, reduced flexion and anterior pain. Restoring the joint line (as above) usually corrects pseudo-baja; true baja from a contracted/scarred tendon is harder and may need joint-line lowering or, rarely, tibial tubercle transfer.
- Assess patellar bone stock at revision and choose accordingly:
- Adequate stock - re-resurface with a new component.
- Thin/deficient stock - retain the bony shell unresurfaced (patelloplasty) rather than over-resect; a too-thin resurfaced patella risks fracture.
- Severe loss / non-reconstructable - options include a gull-wing osteotomy, a porous-metal (tantalum) patella with soft-tissue/mesh reconstruction, bone grafting, or patellectomy as a last resort (with its extensor-lag penalty).
- Always check patellar tracking and the extensor mechanism after reconstruction - maltracking signals component malrotation (correct the rotation, do not lateral-release your way out of a malrotated construct), and a deficient extensor mechanism may itself drive the constraint choice (hinge).
Exam point: in revision TKA, restore the joint line to fix pseudo-patella-baja, match patellar management to bone stock (re-resurface vs patelloplasty vs gull-wing/tantalum vs patellectomy), and read maltracking as malrotation - the patella is part of the reconstruction, not an afterthought.
Complications and Follow-Up
- Why It Happens
- Poor fixation, underestimated bone loss, excessive constraint load or failed ingrowth.
- Prevention or Management
- Multiple-zone fixation, correct stem/augment/cone/sleeve choice, serial radiographs.
- Why It Happens
- Long surgery, previous operations, dead space, host factors and compromised soft tissue.
- Prevention or Management
- Optimisation, cultures, meticulous debridement, antibiotic strategy and early recognition.
- Why It Happens
- Weak metaphysis, cone/sleeve preparation, stem broaching or component extraction.
- Prevention or Management
- Controlled preparation, prophylactic cables when needed, bypass and fixation.
- Why It Happens
- Wrong constraint, collateral insufficiency, joint-line error, malrotation or extensor mechanism failure.
- Prevention or Management
- Trial carefully; correct cause before increasing constraint.
- Why It Happens
- Diaphyseal engagement and load transfer.
- Prevention or Management
- Use appropriate stem length/diameter and counsel patients.
- Why It Happens
- Successful ingrowth makes later removal demanding.
- Prevention or Management
- Preserve host bone, use planned extraction technique and counsel about re-revision complexity.
- Why It Happens
- Multiple operations, patellar tendon avulsion, tubercle osteotomy problems or soft-tissue compromise.
- Prevention or Management
- Avoid forced exposure; repair and protect early.
- Why It Happens
- Difficult exposure, posterior cement, severe deformity correction or traction.
- Prevention or Management
- Document baseline, protect posterior structures and avoid blind posterior instrumentation.
Post-Operative Care
Post-operative instructions depend on fixation quality, soft-tissue repair and fracture risk.
- Typical Approach
- Often weight bearing as tolerated for stable cone/sleeve constructs; restrict if fracture, tenuous fixation, tubercle osteotomy or segmental reconstruction.
- Reason
- Protects biological fixation and soft-tissue repairs.
- Typical Approach
- Use selectively for extensor mechanism repair, ligament reconstruction or hinge/soft-tissue concern.
- Reason
- Controls early instability and protects repair.
- Typical Approach
- Peri-operative prophylaxis for aseptic cases; organism-specific plan for infection revision.
- Reason
- Infection risk is high in complex revision.
- Typical Approach
- Use local arthroplasty protocol with patient-specific risk adjustment.
- Reason
- Revision surgery has elevated thrombotic and bleeding risks.
- Typical Approach
- Early baseline AP/lateral, then serial films for migration, radiolucency, fracture, subsidence and loosening.
- Reason
- Cones, sleeves and stems need longitudinal assessment.
Guidelines, Registries and Global Practice
Revision TKA volume is rising worldwide. National registries consistently report that the leading reasons for revision are infection, aseptic loosening and instability, with bone loss as a frequent accompaniment rather than an isolated indication. There is no single global guideline that prescribes a specific bone-loss implant; instead, society guidance converges on a small number of principles: exclude infection first, restore a stable platform, fix in multiple zones and use the least constraint that achieves stability.
Global epidemiology
- Registry forecasting projects large increases in revision TKA over the coming decades, driven by an ageing population and expanding primary arthroplasty in younger patients.
- Across major registries, the dominant revision indications are periprosthetic joint infection, aseptic loosening, instability and polyethylene wear, all of which generate bone loss.
- AORI type 2 and 3 defects requiring metaphyseal reconstruction are concentrated in re-revision and infected cases.
- Position Relevant to Bone-Loss Revision
- Evidence-based and appropriate-use guidance on PJI diagnosis and the surgical management of the osteoarthritic and failed knee.
- Practical Emphasis
- Standardised infection workup before labelling a revision aseptic.
- Position Relevant to Bone-Loss Revision
- Revision knee replacement should be delivered through networked units with appropriate case-mix and infrastructure.
- Practical Emphasis
- Complex bone loss is best managed in revision networks with full implant inventory.
- Position Relevant to Bone-Loss Revision
- Zonal fixation and defect-led reconstruction teaching for revision TKA.
- Practical Emphasis
- Obtain fixation in at least two of three zones; bypass and protect compromised cortex.
- Position Relevant to Bone-Loss Revision
- Supports staged or single-stage protocols for infection and individualised constraint and fixation selection.
- Practical Emphasis
- Match infection pathway and constraint to host, organism and soft tissues.
- Position Relevant to Bone-Loss Revision
- Standardised definitions for periprosthetic joint infection used worldwide.
- Practical Emphasis
- Apply a recognised PJI definition before any aseptic bone-loss reconstruction.
Registry signals
- Arthroplasty registries (NJR, AJRR, AOANJRR, SHAR, Norwegian and NZJR) track revision burden and indications; they consistently identify infection and loosening as leading causes and document rising rates of complex constrained and stemmed revision constructs.
- Long-term single-institution cohorts complement registry data by reporting durable survivorship of porous metaphyseal cones, with infection rather than mechanical loosening as the main reason for late failure.
- Registries do not yet provide robust head-to-head cone-versus-sleeve survivorship; current comparative evidence is review and cohort level.
High-resource versus limited-resource practice
- High-Resource Setting
- Full range of cones, sleeves, modular augments, offset stems and hinges available on demand.
- Limited-Resource Setting
- Restricted inventory; reliance on cement, screws, bone graft and a limited stem range.
- High-Resource Setting
- Routine metal-artefact-reduction CT and long-leg alignment imaging.
- Limited-Resource Setting
- Plain radiographs predominate; advanced cross-sectional imaging less available.
- High-Resource Setting
- Synovial biomarkers, molecular testing and specialist microbiology.
- Limited-Resource Setting
- Aspiration, culture and inflammatory markers, sometimes without advanced assays.
- High-Resource Setting
- Dedicated revision networks and multidisciplinary infection teams.
- Limited-Resource Setting
- Revision performed in general units; referral networks may be limited.
Controversies and Areas of Uncertainty
Several questions remain genuinely unresolved and are common viva discussion points. The examiner is testing whether the candidate can reason about uncertainty rather than recite a single answer.
Both restore metaphyseal fixation with good short- to mid-term survivorship, but no high-quality randomised or registry head-to-head data establish superiority. Selection follows defect shape, implant system, host bone and surgeon familiarity rather than proven outcome difference.
Meta-analyses show comparable revision and loosening rates, with hybrid fixation showing a non-significant trend toward lower failure and cemented stems associated with more radiolucent lines. No method is universally superior; choice is individualised.
The optimal strategy for the infected knee with bone loss is debated. Single-stage revision is increasingly used in selected patients with a known sensitive organism and good soft tissues, but two-stage remains the default for complex or resistant infection.
Higher constraint increases interface stress and may threaten fixation. The principle is the least constraint that gives stability, but the threshold to escalate to a hinge after collateral loss is judgement-based, not formula-driven.
Porous metal cones and sleeves have largely displaced bulk structural allograft for most defects because allograft does not revascularise and carries union and resorption risk, but allograft retains a role in very large segmental loss in younger patients where bone stock restoration is valued.
The point at which reconstruction should be abandoned in favour of distal femoral or proximal tibial replacement is not precisely defined and depends on host bone, ligament competence, extensor mechanism and patient demand.
Clinical Scenarios
Practise clinical reasoning and management decisions out loud
“A 72-year-old patient has start-up pain, tibial component migration and a large medial tibial defect on radiographs.”
“During revision TKA the femoral component is removed and both condyles are deficient with poor metaphyseal support.”
“A previous revision knee has a well-fixed tibial sleeve but now requires re-revision for instability.”
“A patient presents with a chronically painful TKA, a discharging sinus and radiographic tibial osteolysis with metaphyseal bone loss.”
First principles
- Exclude infection.
- Map bone loss after explant.
- Rebuild the platform before choosing constraint.
AORI
- Type 1: small contained defects.
- Type 2A: one condyle or plateau deficient.
- Type 2B: both condyles or plateaus deficient.
- Type 3: major metaphyseal deficiency.
Reconstruction
- Small contained: cement, screws or selected graft.
- Segmental: metal augment.
- Severe metaphyseal: cone or sleeve plus stem.
- Non-reconstructable: hinge or endoprosthetic solution.
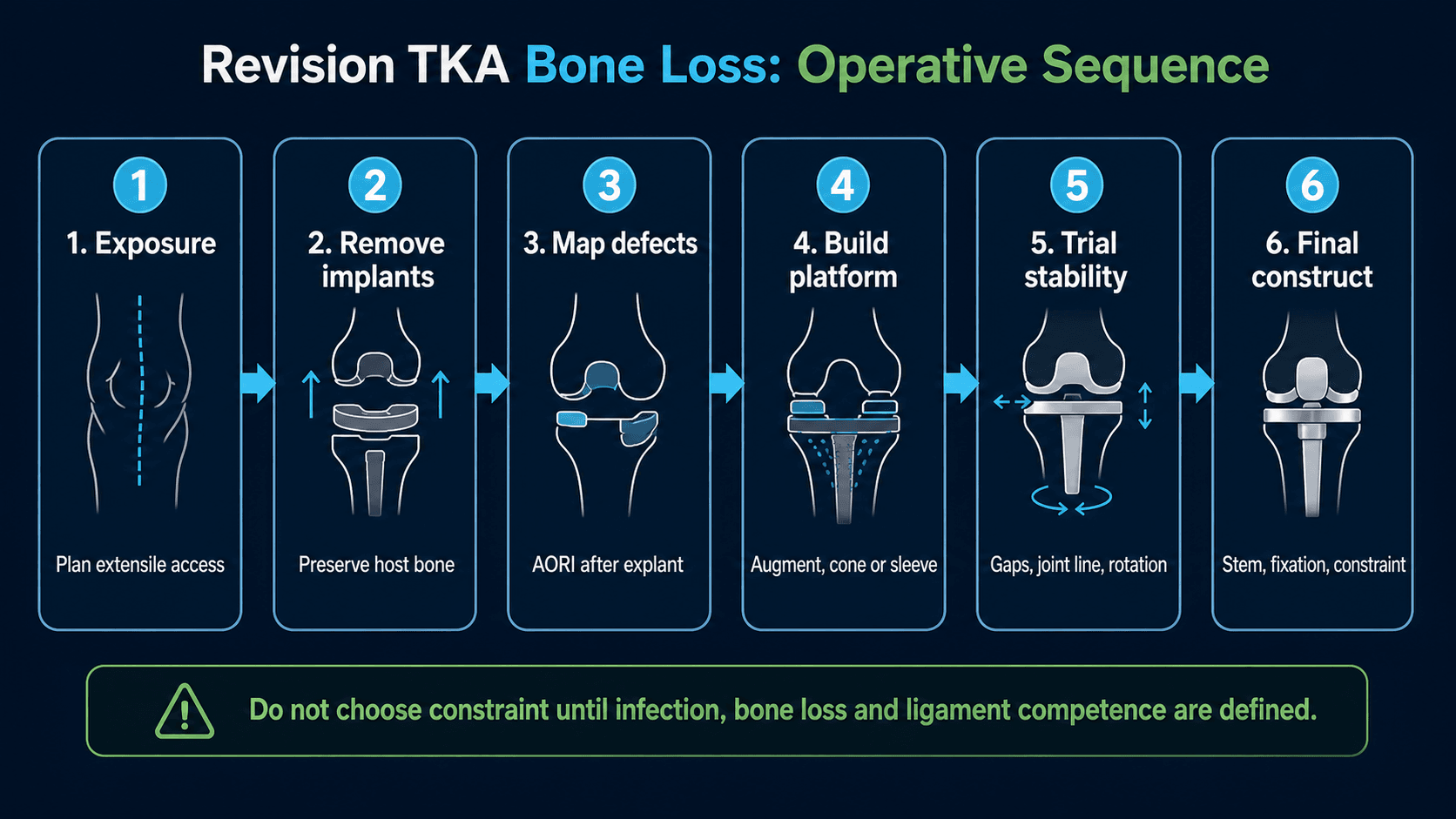
Operative sequence
- Expose safely.
- Remove implants preserving bone.
- Classify final defect.
- Build tibial and femoral support.
- Trial gaps, joint line, rotation and constraint.
- Fix final construct.
Common failures
- Underestimated bone loss.
- Missed infection.
- Cement-only reconstruction of uncontained loss.
- Overconstraint with weak fixation.
- Poor joint-line or posterior-offset restoration.
Evidence Base
AORI classification and reconstruction principles
- Foundational Anderson Orthopaedic Research Institute work defining defect classification and reconstruction alternatives.
- Select the least constraint required for stability to reduce stress at the implant-fixation interface.
- Severity of bone loss largely influences stem length; defects can be repaired with cement, augments or allograft when combined with stemmed components.
Metaphyseal bone loss review
- AORI is widely used because it helps link bone-loss severity with treatment choice.
- Small contained type 1 defects may be managed with cement, screws or morselised graft.
- Large uncontained type 2B and type 3 defects are commonly treated with structural support, cones or sleeves plus stems.
Mechanisms and treatment options
- Bone loss mechanisms include loosening, wear osteolysis, infection, fracture and extraction damage.
- Registry forecasting in this review projects a large rise in revision TKA volume over the coming decades.
- Modern options include cement, graft, augments, cones, sleeves and segmental reconstruction, individualised to defect type and patient factors.
Metaphyseal fixation indications and techniques
- Well-vascularised metaphyseal bone offers an additional fixation opportunity using cement, allograft, trabecular metal cones or porous-coated sleeves.
- Multiple series document good short-term survivorship with cones and sleeves.
- Persistent concerns include stress shielding and difficulty of removal; long-term data were lacking at the time of writing.