Map bone | classify defect | restore fixation | prepare backups
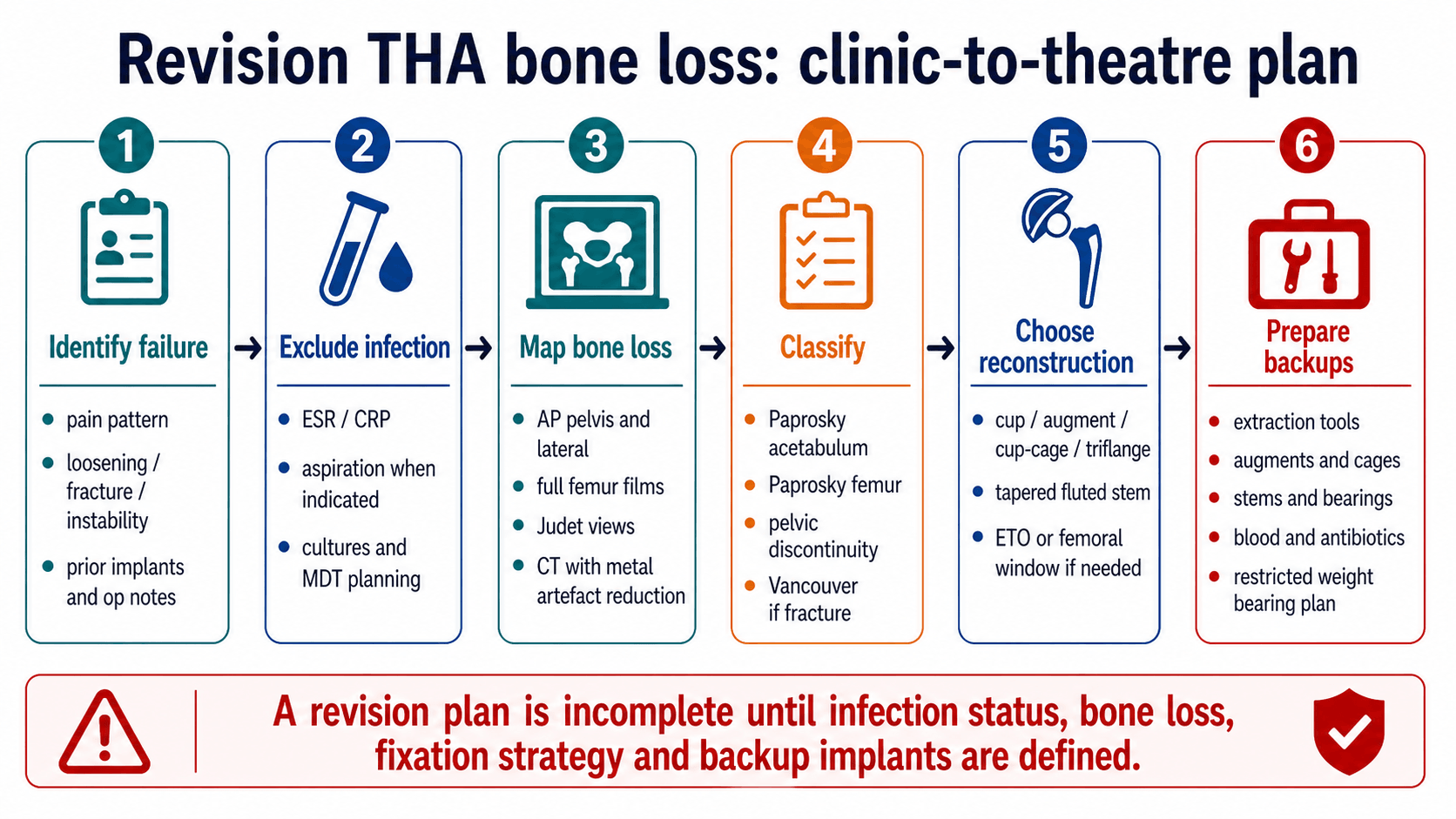
- Revision THA starts by defining failure and excluding infection. Bone loss reconstruction fails if the infection diagnosis is missed.
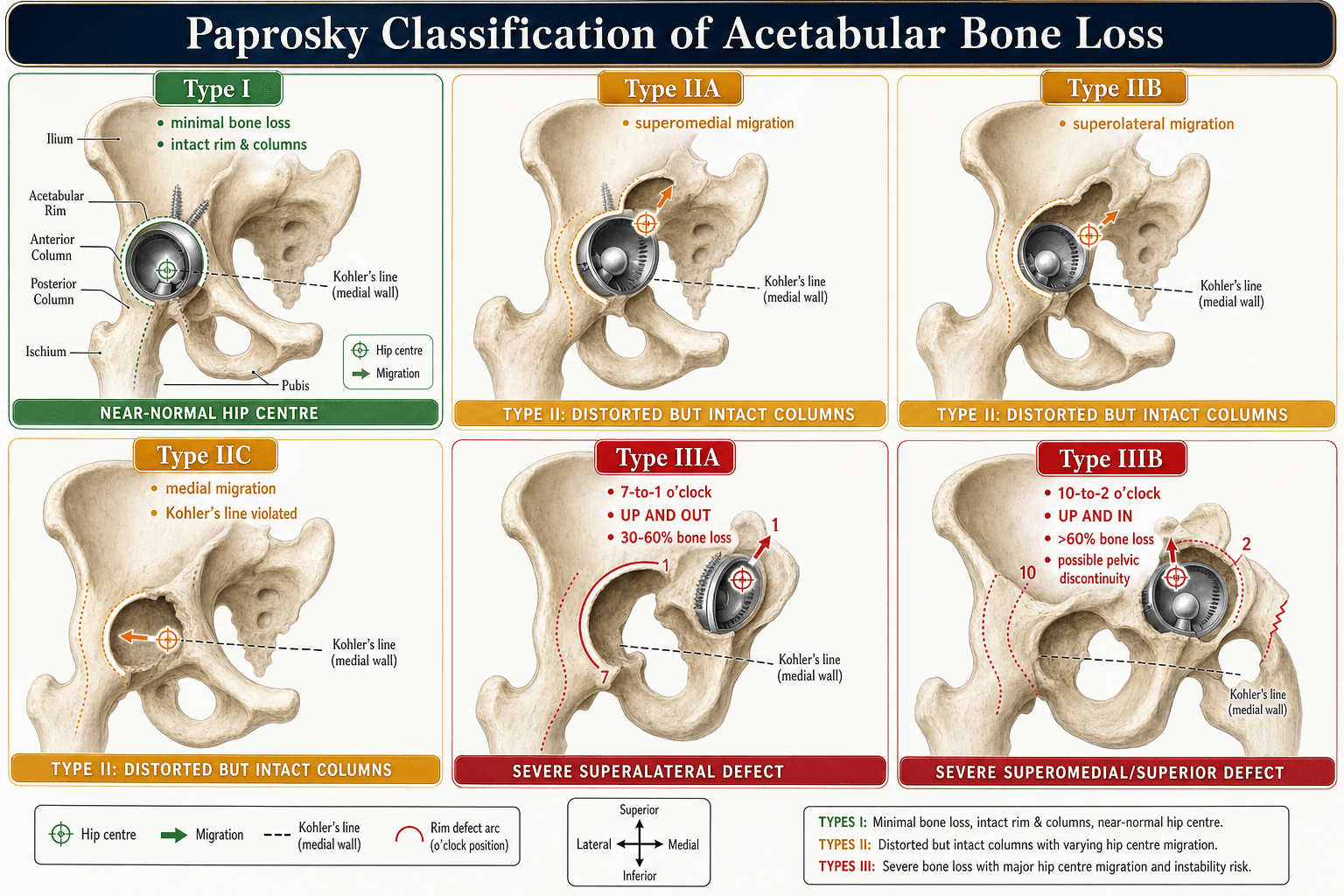
- Paprosky acetabular classification is useful because it estimates rim and column support. It is not just a memorised table.
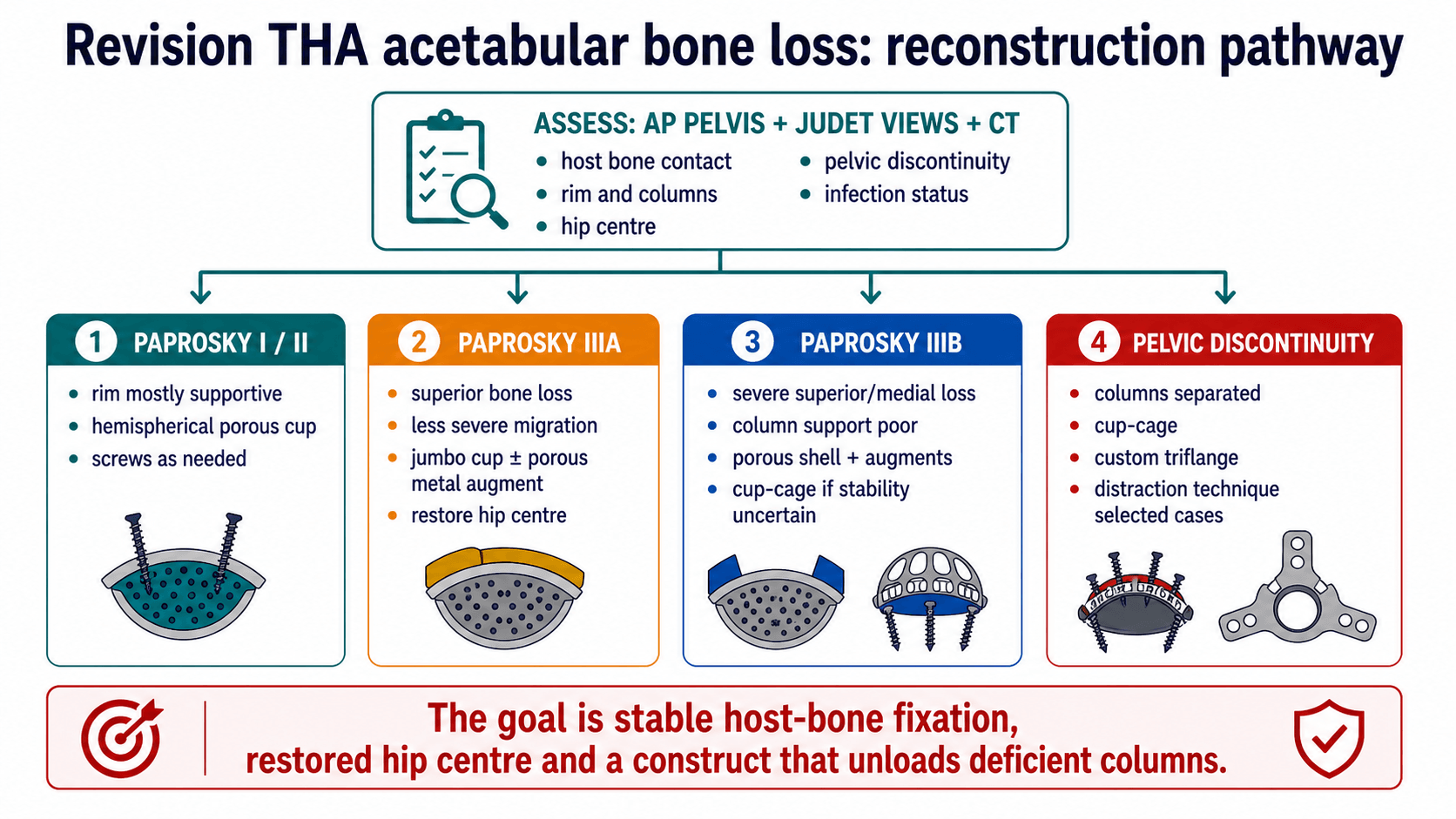
- Pelvic discontinuity means the superior ilium and inferior ischiopubic segment are separated. Standard hemispherical fixation is often insufficient.
- Femoral revision succeeds by obtaining stable fixation beyond the defect. Diaphyseal/isthmus support matters more than proximal appearance alone.
- A revision plan is incomplete without backup implants. Extraction tools, augments, cages, stems, bearings and weight-bearing plan must be decided before theatre.
- “Order AP pelvis, lateral hip, full femur films, Judet views and CT with metal artefact reduction when acetabular columns are uncertain.
- “Use Paprosky to decide if a cup can grip host bone, whether augments are required, and whether the construct must span or unitise the pelvis.
- “A custom triflange can be powerful for severe defects but has high complication and dislocation risk; counsel accordingly.
- “ETO is a controlled exposure tool for well-fixed stems or cement, not a failure of technique.
The AP pelvis gives the first impression. It does not reliably define posterior column support, pelvic discontinuity, femoral isthmus fixation, version, occult fracture or infection. The operation should not start until the surgeon has mapped the bone and planned extraction plus reconstruction.
MAPPre-op workup | HOSTAcetabulum | STEMFemur |
|---|---|---|
M Mechanism of failure Loosening, infection, fracture, instability, wear or adverse local tissue reaction. | H Host contact Porous shell needs enough supportive host bone. | S Support at isthmus Diaphyseal support enables tapered fluted fixation. |
A Anatomy of bone loss Columns, rim, medial wall, isthmus, cortical tube and fracture lines. | O Offset and hip centre Reconstruction must restore biomechanics. | T Trochanteric osteotomy ETO preserves bone during difficult extraction. |
P Plan extraction and backups Removal tools, ETO, augments, cages, stems and weight-bearing restrictions. | S Structural support Augments, cup-cage or triflange when columns are deficient. | E Endoprosthesis Consider when host femur cannot support a revision stem. |
T Test discontinuity CT/Judet views and intra-operative stability determine strategy. | M Measure length/version Restore leg length, offset and version, not just fixation. | |
Map before cutting. | Host bone decides fixation. | Fix beyond the defect. |
BACKUPTheatre Readiness
Hook:Revision THA without BACKUP is not planned surgery.
Overview and Definitions
Revision THA bone loss is a reconstruction problem, not simply a component exchange. The surgeon must identify why the arthroplasty failed, whether infection is present, how much host bone remains, and which construct can achieve durable fixation.
The practical definitions are:
- Meaning
- Bone loss surrounded by a rim or cortical shell.
- Treatment Implication
- May be filled with morselised graft or cement/augment depending size and fixation.
- Meaning
- A rim, wall or column segment is missing.
- Treatment Implication
- Needs structural support: augment, cage, structural graft or custom component.
- Meaning
- Superior ilium separated from inferior ischiopubic segment through the acetabulum.
- Treatment Implication
- Construct must stabilise or unitise the pelvis; standard cup fixation is often inadequate.
- Meaning
- Proximal femur cannot support the stem.
- Treatment Implication
- Shift fixation distally with a tapered fluted stem if diaphysis allows.
- Meaning
- No reliable proximal or diaphyseal host fixation.
- Treatment Implication
- Consider proximal femoral replacement or allograft-prosthetic composite in selected cases.
Pathophysiology
Bone loss in revision THA usually develops from osteolysis, loosening, stress shielding, infection, periprosthetic fracture, adverse local tissue reaction or repeated previous surgery. Each mechanism leaves a different reconstruction problem.
- Typical Bone Problem
- Cavitary acetabular or proximal femoral defects, sometimes with intact rim.
- Planning Consequence
- Assess whether fixation remains possible with shell/stem exchange and grafting.
- Typical Bone Problem
- Progressive migration, rim deficiency, femoral cortical thinning or pedestal formation.
- Planning Consequence
- Plan extraction and reconstruction; classify both sides.
- Typical Bone Problem
- Bone destruction plus compromised soft tissues.
- Planning Consequence
- Treat infection pathway first; reconstruction may need staged strategy.
- Typical Bone Problem
- Femoral cortical tube disrupted; implant may be loose.
- Planning Consequence
- Use Vancouver plus Paprosky femoral planning; fixation must bypass fracture and deficient bone.
- Typical Bone Problem
- Combined acetabular/femoral deficiency, abductor damage and instability risk.
- Planning Consequence
- Expect higher constraint, complex exposure and restricted rehabilitation.
- Typical Bone Problem
- Columns no longer form a continuous ring.
- Planning Consequence
- Cup-cage, triflange or distraction technique rather than simple hemispherical cup.
Clinical Presentation and Assessment
History and examination
Ask what failed and what has already been done. Important history includes original diagnosis, approach, implant type, fixation method, bearing surface, prior infection, wound issues, instability episodes, fractures, metal-on-metal exposure, antibiotics, anticoagulation, neurological symptoms and functional goals.
Examination must document:
- Gait, Trendelenburg sign, abductor function and walking aids.
- Limb length, fixed deformity, flexion contracture and rotational profile.
- Scar position and soft-tissue envelope.
- Neurovascular status, especially sciatic/peroneal symptoms.
- Pain with rotation, trochanteric pain and signs of loosening or instability.
- Spine and pelvic obliquity when leg length or instability is part of the problem.
First-line imaging and tests
- How To Order It
- Standing or standardised AP pelvis plus lateral of affected hip.
- What It Answers
- Migration, hip centre, loosening, osteolysis, offset, leg length and component position.
- How To Order It
- Include hip to knee with entire implant and distal femur.
- What It Answers
- Stem length, cement, cortical defects, distal hardware and bypass planning.
- How To Order It
- Oblique pelvic views when columns/discontinuity are uncertain.
- What It Answers
- Anterior and posterior column support.
- How To Order It
- Pelvis and/or femur depending defect.
- What It Answers
- Column integrity, discontinuity, version, bone stock, osteolysis and occult fracture.
- How To Order It
- Screen for infection; aspirate when markers, symptoms or history are suspicious.
- What It Answers
- Defines whether revision is aseptic or infection pathway.
- How To Order It
- Obtain stickers, op notes and bearing/taper details.
- What It Answers
- Determines extraction tools, compatibility and backup components.
Investigations
The investigation plan must answer four questions before theatre: is the joint infected, is the acetabular column support intact, where can the femur obtain fixation, and what implant/extraction equipment is required.
- Decision It Supports
- Aseptic revision versus infection pathway, culture strategy and staging.
- Unsafe Shortcut
- Calling a loose implant aseptic without infection workup.
- Decision It Supports
- Migration, hip centre, offset, leg length, loosening and gross osteolysis.
- Unsafe Shortcut
- Using AP pelvis alone to choose augments or cages.
- Decision It Supports
- Stem length, cement mantle, cortical tube, distal hardware, fracture and bypass length.
- Unsafe Shortcut
- Planning femoral revision without seeing the whole stem.
- Decision It Supports
- Anterior and posterior column integrity when discontinuity is possible.
- Unsafe Shortcut
- Missing posterior column deficiency.
- Decision It Supports
- Column support, discontinuity, component version, osteolysis, cortical defects and occult fracture.
- Unsafe Shortcut
- Assuming a cup can grip host bone without cross-sectional mapping.
Bone-Loss Mapping
- Bone-Loss Pattern
- Minimal bone loss; hemispherical shape and rim supportive.
- Reconstruction Meaning
- Porous hemispherical cup usually sufficient.
- Bone-Loss Pattern
- Distorted hemisphere with superior, lateral or medial bone loss.
- Reconstruction Meaning
- Cup with screws, graft or limited augment depending host contact.
- Bone-Loss Pattern
- Severe superior bone loss but some column/rim support remains.
- Reconstruction Meaning
- Jumbo cup, porous shell and augments; restore hip centre if possible.
- Bone-Loss Pattern
- Severe superior/medial migration with poor column support; discontinuity risk.
- Reconstruction Meaning
- Cup-cage, custom triflange, distraction or complex augment strategy.
The viva trap is to treat all pelvic discontinuity the same. Management diverges on whether the discontinuity is acute or chronic:
- Acute discontinuity: an intra-operative or recent fracture through reasonable host bone (e.g. during cup extraction or reaming), with healthy bleeding bone surfaces. Like any fracture in good bone it can heal, so it is treated as a fracture - posterior column plating and/or compression across the discontinuity with a hemispherical shell - aiming for primary bony union.
- Chronic discontinuity: a long-standing separation in osteolytic, sclerotic, often atrophic bone with no healing potential. Compression and plating alone fail because the bone will not unite, so the construct must bridge or distract the deficient columns rather than rely on healing - cup-cage, custom triflange, or acetabular distraction (which uses the elastic recoil of the distracted hemipelvis to load a porous shell plus augments).
Recognising which you face - from chronicity, bone quality and intra-operative bleeding - dictates whether you compress-and-heal or bridge-and-distract.
Management
Management is selected by fixation biology and mechanical stability. The surgeon should not choose an implant because it is familiar; the implant must solve the defect pattern.
- Preferred Direction
- Porous hemispherical shell with screws; graft contained defects as required.
- Why
- Enough host bone exists for initial stability and ingrowth.
- Preferred Direction
- Jumbo cup or porous shell plus modular augment.
- Why
- Augment converts an unsupported segment into a stable platform.
- Preferred Direction
- Plan cup-cage, custom triflange or distraction rather than shell alone.
- Why
- The construct must bridge or unitise deficient columns.
- Preferred Direction
- Consider impaction grafting when stable containment and surgeon experience allow.
- Why
- May restore bone stock but fails if initial stability is poor.
Acetabular Reconstruction
- Best Use
- Paprosky I/II and selected IIIA with enough host bone contact.
- Limitations and Pitfalls
- Fails if rim/columns cannot support initial stability.
- Best Use
- Superior bone loss where large shell restores contact.
- Limitations and Pitfalls
- Can raise hip centre or over-ream if used indiscriminately.
- Best Use
- Segmental superior, posterior or medial defects with shell contact possible.
- Limitations and Pitfalls
- Augment must support shell and be mechanically stable; cement only at augment-shell interface when used.
- Best Use
- Severe bone loss or discontinuity when a shell alone may not be stable.
- Limitations and Pitfalls
- Cage protects shell while ingrowth occurs; risk of dislocation, infection and cage fatigue remains.
- Best Use
- Massive defects, pelvic discontinuity, failed cages or unusual anatomy.
- Limitations and Pitfalls
- Requires CT-based manufacture, longer lead time and counselling about high complication risk.
- Best Use
- Selected chronic pelvic discontinuity with porous shell and augments.
- Limitations and Pitfalls
- Technique-sensitive; requires careful patient and defect selection.
- Best Use
- Contained or reconstructable defects, especially where bone-stock restoration matters.
- Limitations and Pitfalls
- Use caution in severe uncontained defects or when primary stability is weak.
Know where the cup-cage came from. The Burch-Schneider antiprotrusio cage is a metal cage with a superior iliac flange (screwed to the ilium) and an inferior flange that hooks into the ischium, spanning a severe defect or discontinuity to offload it. Its weakness is biological: a cage is a purely mechanical bridge with no bone-ingrowth surface, so it relies entirely on screw fixation and tends to loosen or fatigue-fracture over time, especially in a chronic discontinuity that never heals.
The cup-cage construct is the modern evolution that solves this: a highly porous (ingrowth-capable) hemispherical shell is first secured to host bone, then a cage is placed over it spanning ilium to ischium. The cage protects the porous shell from load while the shell osseointegrates - so once ingrowth occurs the construct is biologically fixed, not merely screw-dependent. This is why the cup-cage has largely superseded the standalone antiprotrusio cage for severe defects and chronic discontinuity, with custom triflanges and distraction occupying the most extreme end of the spectrum.
Femoral Reconstruction
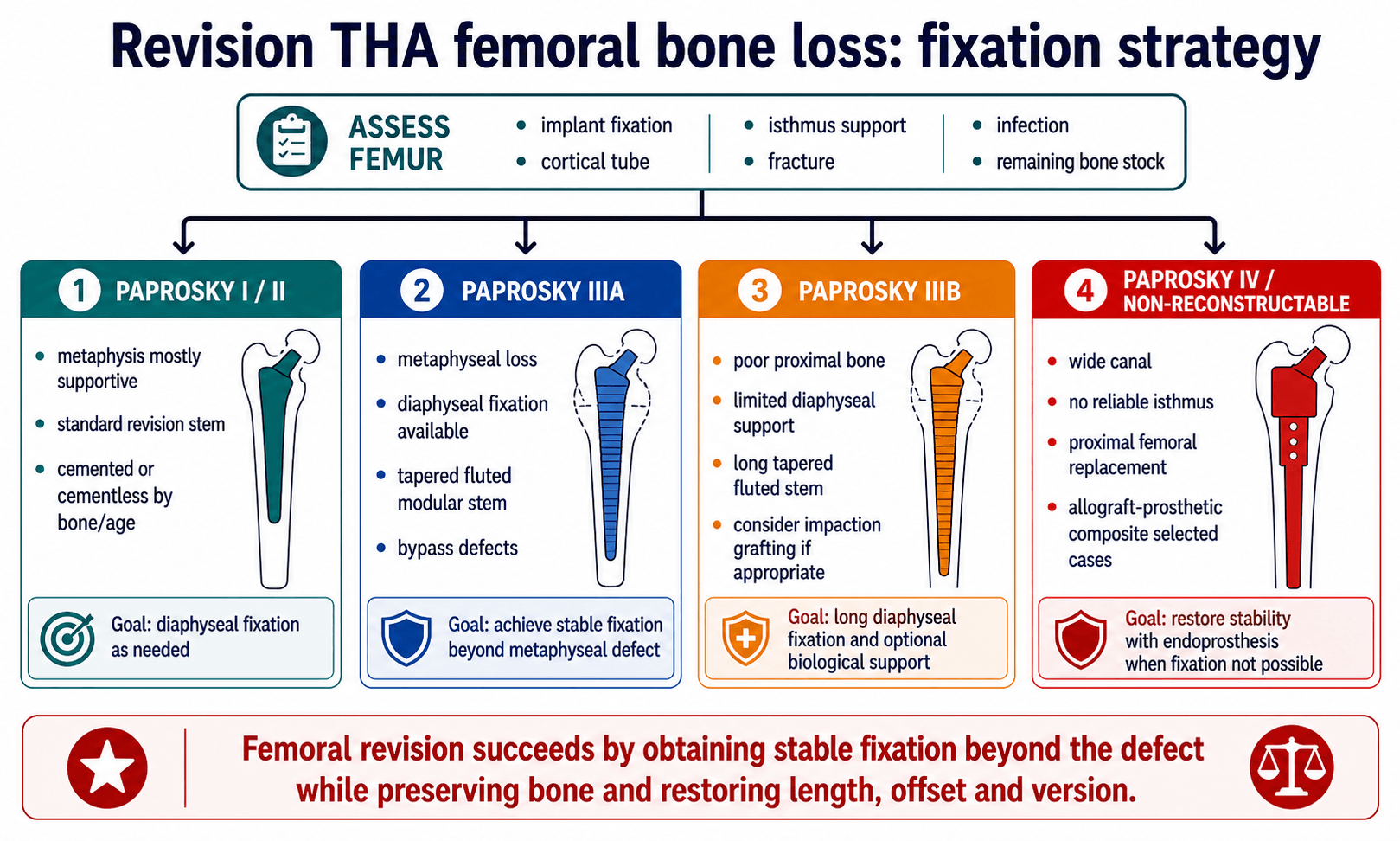
Bypass the defect, obtain axial and rotational stability, restore length/offset/version, and avoid creating a fracture during extraction.
Paprosky IV, severe Vancouver B3 fractures, tumour-like bone loss or failed multiple revisions may require proximal femoral replacement or allograft-prosthetic composite.
- When To Choose
- Older patient, poor bone, intact cement mantle strategy or selected low-demand cases.
- Key Technical Point
- Cement technique and version control are critical.
- When To Choose
- Paprosky IIIA/selected IIIB with diaphyseal fixation available.
- Key Technical Point
- Achieve axial/rotational stability beyond defect and restore version with modularity.
- When To Choose
- Selected femora with adequate diaphyseal engagement.
- Key Technical Point
- Mismatch, thigh pain and stress shielding must be considered.
- When To Choose
- Younger patient or contained femoral deficiency where bone stock restoration is realistic.
- Key Technical Point
- Technique-sensitive; needs intact cortical tube and stable cemented stem construct.
- When To Choose
- Non-reconstructable proximal femur, massive bone loss, severe B3 fracture or salvage setting.
- Key Technical Point
- Higher dislocation/infection risk; restore abductors and soft-tissue tension where possible.
Complications and Failure Management
- Why It Happens
- Abductor deficiency, altered hip centre, constrained reconstruction, soft-tissue damage.
- Prevention or Management
- Restore offset/length/version, choose bearing strategy, consider dual mobility or constrained liner in selected cases.
- Why It Happens
- Long surgery, multiple revisions, dead space and compromised host.
- Prevention or Management
- Optimise, culture, debride, antibiotic plan and staged reconstruction when indicated.
- Why It Happens
- Poor host fixation, inadequate column support, failed ingrowth or overloaded cage.
- Prevention or Management
- Use appropriate host bone fixation, augments, cage/triflange and protected rehabilitation.
- Why It Happens
- Limb lengthening, traction, scar dissection or screw/cage placement.
- Prevention or Management
- Document pre-op status, limit acute lengthening, protect sciatic nerve and use safe screw corridors.
- Why It Happens
- Extraction, weak cortex, stress risers or inadequate bypass.
- Prevention or Management
- ETO, cables/struts, long stems and bypass defects.
- Why It Happens
- Poor biology, inadequate fixation or excessive stripping.
- Prevention or Management
- Preserve attachments, cable fixation, protected weight bearing and revision fixation if symptomatic failure.
Operative Technique
Revision THA bone loss operation: PIPADRAW sequence
- What The Surgeon Does
- Usually lateral decubitus for posterior/lateral revision; ensure full femur access and ability to extend incision.
- Pitfall
- Positioning that prevents distal femoral exposure makes ETO or fracture control harder.
- What The Surgeon Does
- Have AP pelvis/full femur templates, extraction systems, burrs, cables, augments, cages, stems, bearings and backup constraint.
- Pitfall
- Starting without backup implants converts a planned reconstruction into improvisation.
- What The Surgeon Does
- Antibiotics/cultures per infection plan, blood availability, cell salvage if used, previous incision strategy.
- Pitfall
- Giving antibiotics before cultures may compromise microbiology if infection is suspected.
- What The Surgeon Does
- Use prior approach where safe; extensile posterior, lateral or anterolateral exposure by implant, scar and surgeon familiarity.
- Pitfall
- Poor soft-tissue handling increases instability and wound complications.
- What The Surgeon Does
- Identify abductors, sciatic nerve risk zone, pseudocapsule, implants, cables/screws and osteolytic membrane.
- Pitfall
- Aggressive membrane removal can damage remaining host bone.
- What The Surgeon Does
- Remove liner/head first; assess fixation; use curved blades/extraction tools for cup; use ETO for difficult stem/cement removal when appropriate.
- Pitfall
- Uncontrolled extraction causes iatrogenic fracture and worsens bone loss.
- What The Surgeon Does
- Rebuild acetabulum to host bone/columns and femur to reliable fixation zone; restore hip centre, offset, length and version.
- Pitfall
- Stable-looking components can still be biomechanically wrong if hip centre or version is poor.
- What The Surgeon Does
- Sciatic nerve, superior gluteal neurovascular bundle, femoral vessels medially, abductors, greater trochanter and peroneal nerve stretch.
- Pitfall
- Lengthening and scar dissection increase nerve risk.
- What The Surgeon Does
- Weight bearing by construct, bone loss, ETO fixation and fracture risk; dislocation precautions and abductor rehabilitation.
- Pitfall
- Allowing full weight bearing after tenuous fixation can fail the reconstruction.
Extended trochanteric osteotomy
Use ETO when a well-fixed stem, long cement mantle, distal ingrowth, cement restrictor, femoral deformity or high fracture risk makes direct extraction unsafe. The aim is controlled access while preserving the vascularised osteotomy fragment.
Key steps:
- Plan osteotomy length from implant/cement extent; commonly about 12 to 16 cm from the greater trochanter in described techniques.
- Preserve vastus lateralis and abductor attachments to maintain biology.
- Round osteotomy corners with burr to reduce stress risers.
- Open the osteotomy in a controlled fashion, remove stem/cement, reconstruct the canal, then close with cables or wires.
- Protect against trochanteric migration, nonunion, fracture and abductor dysfunction.
Guidelines, Registries and Global Practice
Revision burden is rising worldwide as the primary THA population grows and ages. National joint registries are the best source of global epidemiology because they capture whole populations rather than single-centre series.
- Signal
- Across major registries (AOANJRR, NJR, AJRR, SHAR) aseptic loosening, dislocation and infection are consistently the leading reasons for revision THA.
- Planning Relevance
- These mechanisms generate most acetabular and femoral bone loss; anticipate them in workup.
- Signal
- Registries report a steady absolute rise in revision procedures as the primary arthroplasty cohort expands and survives longer.
- Planning Relevance
- Demand for augments, cup-cages, triflanges and tapered fluted stems is increasing globally.
- Signal
- Registry data show re-revision risk is higher than first-time revision, particularly after instability and infection.
- Planning Relevance
- Counsel patients that complex bone-loss reconstruction is not always a single definitive operation.
- Signal
- Outcome literature and registry-linked series show a shift away from cemented reconstruction toward highly porous shells and modular porous augments.
- Planning Relevance
- Mirror contemporary practice; cemented sockets are now selective.
- Emphasis Relevant to Bone Loss
- Systematic infection workup before revision (serology then aspiration) and structured pre-operative planning.
- Practical Takeaway
- Exclude periprosthetic joint infection before any aseptic bone-loss reconstruction.
- Emphasis Relevant to Bone Loss
- Complex revision and pelvic discontinuity concentrated in higher-volume revision units with multidisciplinary input.
- Practical Takeaway
- Refer massive bone loss and discontinuity to experienced revision teams.
- Emphasis Relevant to Bone Loss
- Mechanical principles: bypass the defect, obtain stable fixation in host bone and protect biology during exposure.
- Practical Takeaway
- Fixation strategy is defined by where reliable host bone remains.
- Emphasis Relevant to Bone Loss
- Standardised classification (Paprosky), infection exclusion and registry-informed implant selection.
- Practical Takeaway
- Use a shared classification language and registry-supported implants.
- Well-Resourced Setting
- CT with metal artefact reduction and Judet views routinely available.
- Limited-Resource Setting
- May rely on plain films and Judet views; CT access can be limited, raising the value of careful radiographic assessment.
- Well-Resourced Setting
- Full range of porous augments, cup-cages, custom triflanges and modular tapered stems.
- Limited-Resource Setting
- Custom and modular options may be unavailable; structural allograft, cages and standard revision implants are used more.
- Well-Resourced Setting
- CT-based manufacture feasible with adequate lead time.
- Limited-Resource Setting
- Manufacturing lead time, cost and supply chain often make custom triflange impractical.
- Well-Resourced Setting
- Registry capture and structured surveillance.
- Limited-Resource Setting
- Surveillance may be opportunistic; emphasise durable, forgiving constructs.
Controversies and Areas of Uncertainty
Both manage severe defects and discontinuity. Off-the-shelf cup-cage avoids manufacturing lead time and cost, while custom triflange is matched to unique anatomy. High-quality comparative data are limited and choice remains largely surgeon- and resource-dependent.
Distraction with a porous shell and augments is a newer technique for chronic pelvic discontinuity that aims to use elastic recoil for stability. Evidence is mostly single-centre cohorts; its place relative to cup-cage and triflange is still being defined.
Dual mobility reduces dislocation while preserving motion, but late intraprosthetic dissociation is a concern. Constrained liners can salvage severe abductor deficiency but transmit higher loads to fixation. The threshold between them is not standardised.
Modular fluted tapered stems aid version and length control but introduce a modular junction at risk of corrosion or fracture. Whether modular or monoblock stems are preferable in a given defect remains debated.
Clinical Scenarios
Practise clinical reasoning and management decisions out loud
“A patient presents with a painful loose acetabular component. AP pelvis shows superior migration and medial wall deficiency. CT suggests poor posterior column support but no clear acute infection.”
“A well-fixed cementless femoral stem must be removed during revision THA. The proximal femur is thin and there is concern that extraction will fracture the femur.”
“Intra-operatively, during a revision THA for a loose cup, you find motion between the superior and inferior hemipelvis when you stress the acetabulum. CT had shown medial migration and a broken Kohler line.”
Workup
- History, op notes and implant details
- ESR/CRP ± aspiration
- AP pelvis, lateral and full femur
- Judet views for columns
- CT for discontinuity/version/bone stock
Acetabulum
- Paprosky I/II: porous shell
- IIIA: shell plus augment/jumbo cup
- IIIB: poor columns, plan backup
- Discontinuity: cup-cage/triflange/distraction
- Restore hip centre and host fixation
Femur
- Classify Paprosky femur
- Plan extraction and ETO
- Fix beyond deficient bone
- Restore length, offset and version
- Prepare fracture and salvage options
“Exclude infection, map bone loss, classify acetabulum and femur, then choose a construct that obtains stable fixation.”
Evidence Signals
Acetabular bone-loss update
- Paprosky remains the most commonly used acetabular bone-loss classification.
- Careful radiological assessment can diagnose bone-loss pattern and chronic pelvic discontinuity before surgery.
- Contemporary practice increasingly uses highly porous shells with modular porous metal augments.
Acetabular reconstruction review
- Pre-operative evaluation includes history, examination, infection workup and detailed radiographic planning.
- Paprosky classification is based on column integrity and guides treatment strategy.
- Uncemented biological fixation techniques are preferred in many contemporary reconstructions.
References
- Sanghavi SA, Paprosky WG, Sheth NP. Evaluation and Management of Acetabular Bone Loss in Revision Total Hip Arthroplasty: A 10-year Update. J Am Acad Orthop Surg. 2024;32(10):e466-e475. doi:10.5435/JAAOS-D-23-00645.
- Fryhofer GW, Ramesh S, Sheth NP. Acetabular reconstruction in revision total hip arthroplasty. J Clin Orthop Trauma. 2020;11(1):22-28. doi:10.1016/j.jcot.2019.11.004.
- Hasenauer MD, Paprosky WG, Sheth NP. Treatment options for chronic pelvic discontinuity. J Clin Orthop Trauma. 2018;9(1):58-62. doi:10.1016/j.jcot.2017.09.009.
- Abdel MP, Trousdale RT, Berry DJ. Pelvic Discontinuity Associated With Total Hip Arthroplasty: Evaluation and Management. J Am Acad Orthop Surg. 2017;25(5):330-338. doi:10.5435/JAAOS-D-15-00260.
- Taunton MJ, Fehring TK, Edwards P, Bernasek T, Holt GE, Christie MJ. Pelvic discontinuity treated with custom triflange component: a reliable option. Clin Orthop Relat Res. 2012;470(2):428-434. doi:10.1007/s11999-011-2126-1.
- De Martino I, Strigelli V, Cacciola G, et al. Survivorship and Clinical Outcomes of Custom Triflange Acetabular Components in Revision Total Hip Arthroplasty: A Systematic Review. J Arthroplasty. 2019;34(10):2511-2518. doi:10.1016/j.arth.2019.05.032.
- Sershon RA, McDonald JF 3rd, Nagda S, Hamilton WG, Engh CA Jr. Custom Triflange Cups: 20-Year Experience. J Arthroplasty. 2021;36(9):3264-3268. doi:10.1016/j.arth.2021.05.005.
- Brown JM, Mistry JB, Cherian JJ, et al. Femoral Component Revision of Total Hip Arthroplasty. Orthopedics. 2016;39(6):e1129-e1139. doi:10.3928/01477447-20160819-06.
- Wyles CC, Hannon CP, Viste A, et al. Extended Trochanteric Osteotomy in Revision Total Hip Arthroplasty. JBJS Essent Surg Tech. 2023;13(3):e21.00003. doi:10.2106/JBJS.ST.21.00003.
- Jones SA. Impaction Grafting Made Easy. J Arthroplasty. 2017;32(9S):S54-S58. doi:10.1016/j.arth.2017.02.045.
- Lee JM, Kim TH. Acetabular Cup Revision Arthroplasty Using Morselized Impaction Allograft. Hip Pelvis. 2018;30(2):65-77. doi:10.5371/hp.2018.30.2.65.
- Fink B, Ahmadian A, Sax FH, Schuster P. Revision total hip arthroplasty using a modular fluted, tapered revision femoral component and interlocking screws in Vancouver B3 periprosthetic fractures with insufficient bone at the isthmus. Bone Joint J. 2024;106-B(4):344-351. doi:10.1302/0301-620X.106B4.BJJ-2023-0899.R1.
- Wyles CC, Hannon CP, Viste A, Perry KI, Trousdale RT, Berry DJ, Abdel MP. Extended Trochanteric Osteotomy in Revision Total Hip Arthroplasty. JBJS Essent Surg Tech. 2023;13(3):e21.00003. doi:10.2106/JBJS.ST.21.00003.