Diagnose the gap | correct the cause | use the least necessary constraint
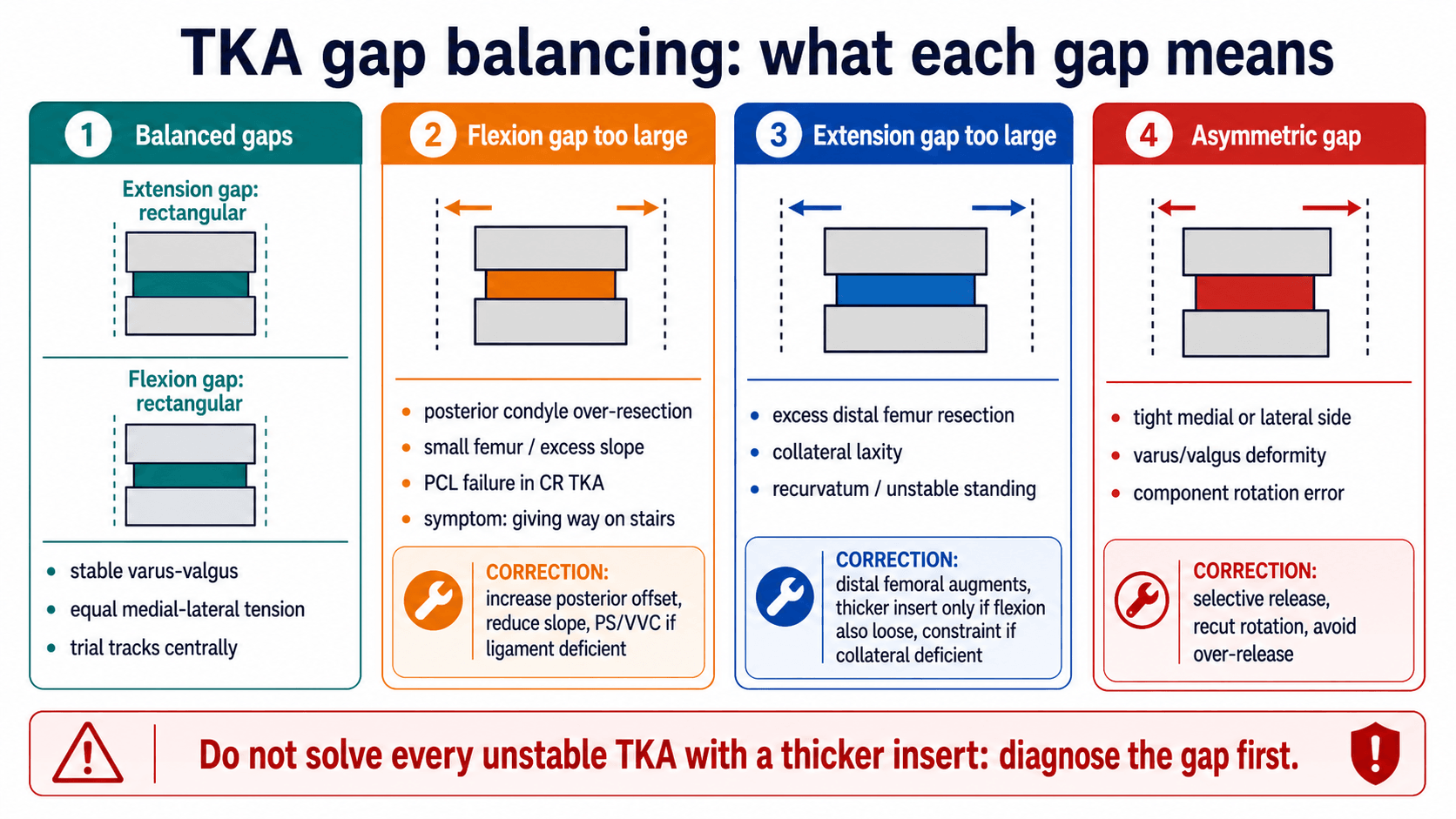
- A balanced TKA is not simply a thick insert. It is stable in extension, flexion and mid-flexion with a centred patella and no coronal thrust.
- Distal femoral resection changes extension gap. Posterior femoral condylar resection and posterior tibial slope mainly change flexion gap.
- Flexion instability often presents with stairs, chair-rise difficulty, recurrent effusions and vague anterior/periretinacular pain.
- Mid-flexion instability is a real but difficult diagnosis. It requires careful examination between full extension and 90° rather than a single endpoint test.
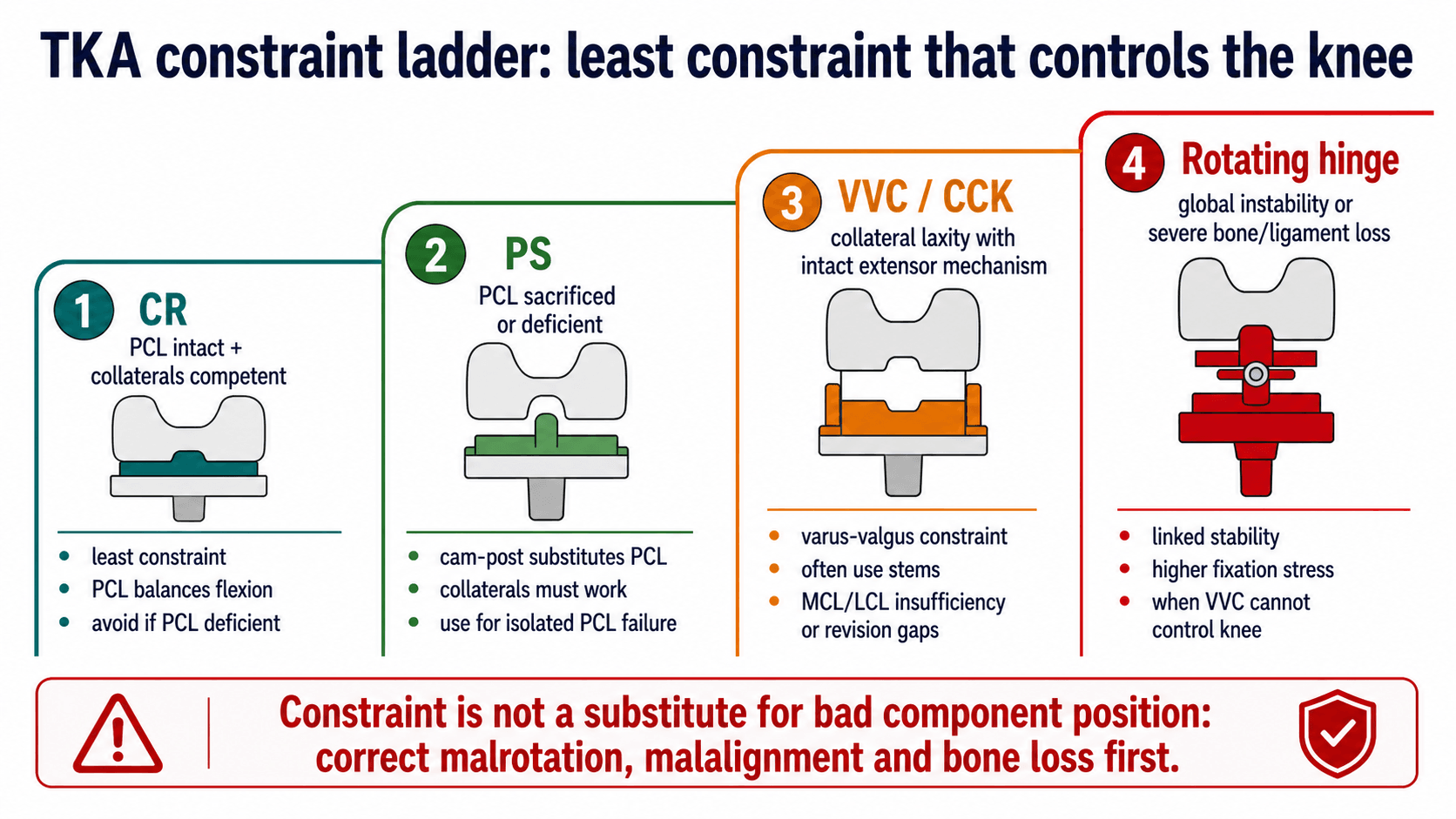
- Constraint treats residual instability after the cause is corrected. It does not compensate for malrotation, malalignment, infection or unrecognised bone loss.
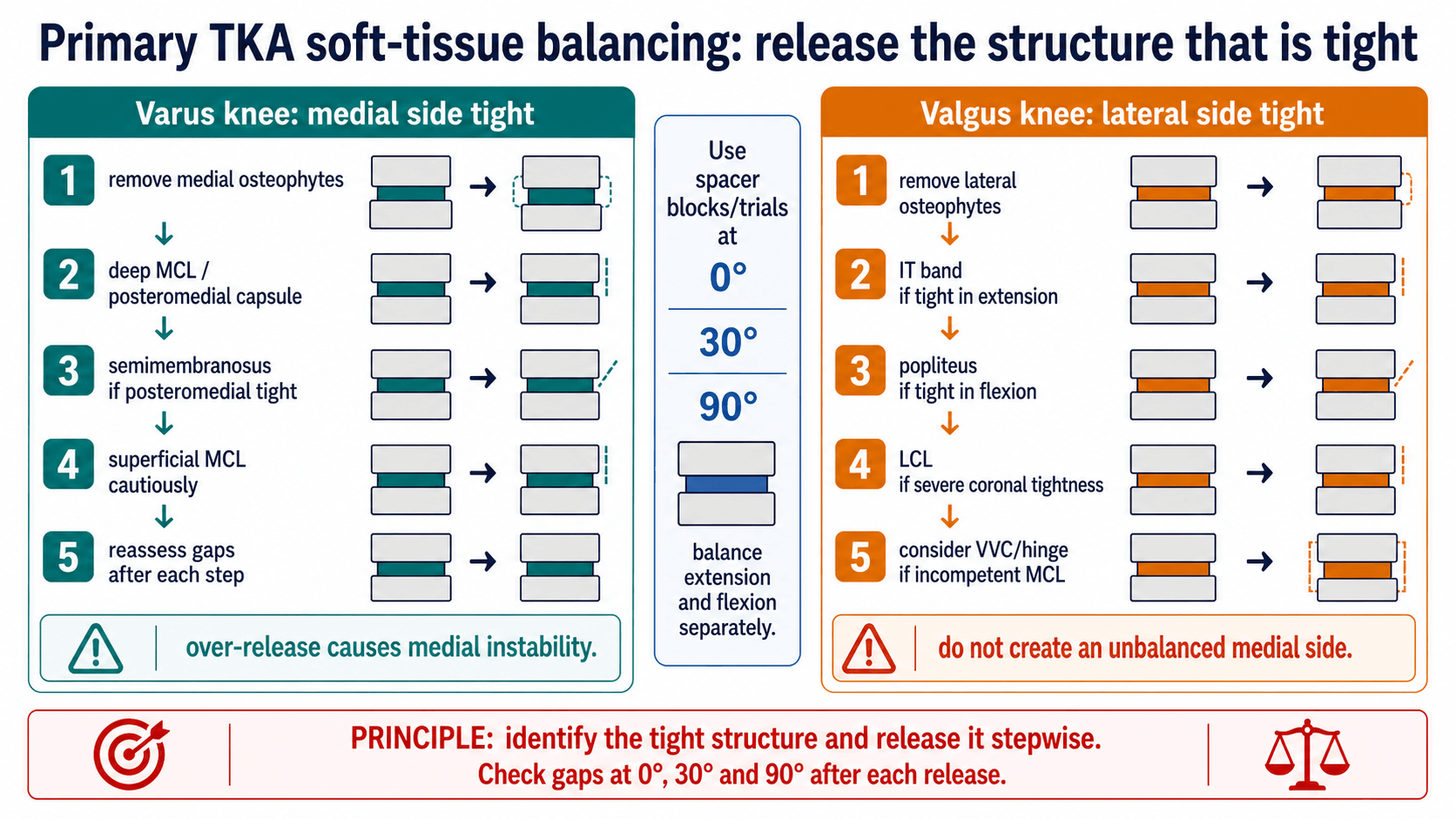
- “Varus-valgus stress must be tested at full extension, 30° and 90° because each position loads different stabilisers.
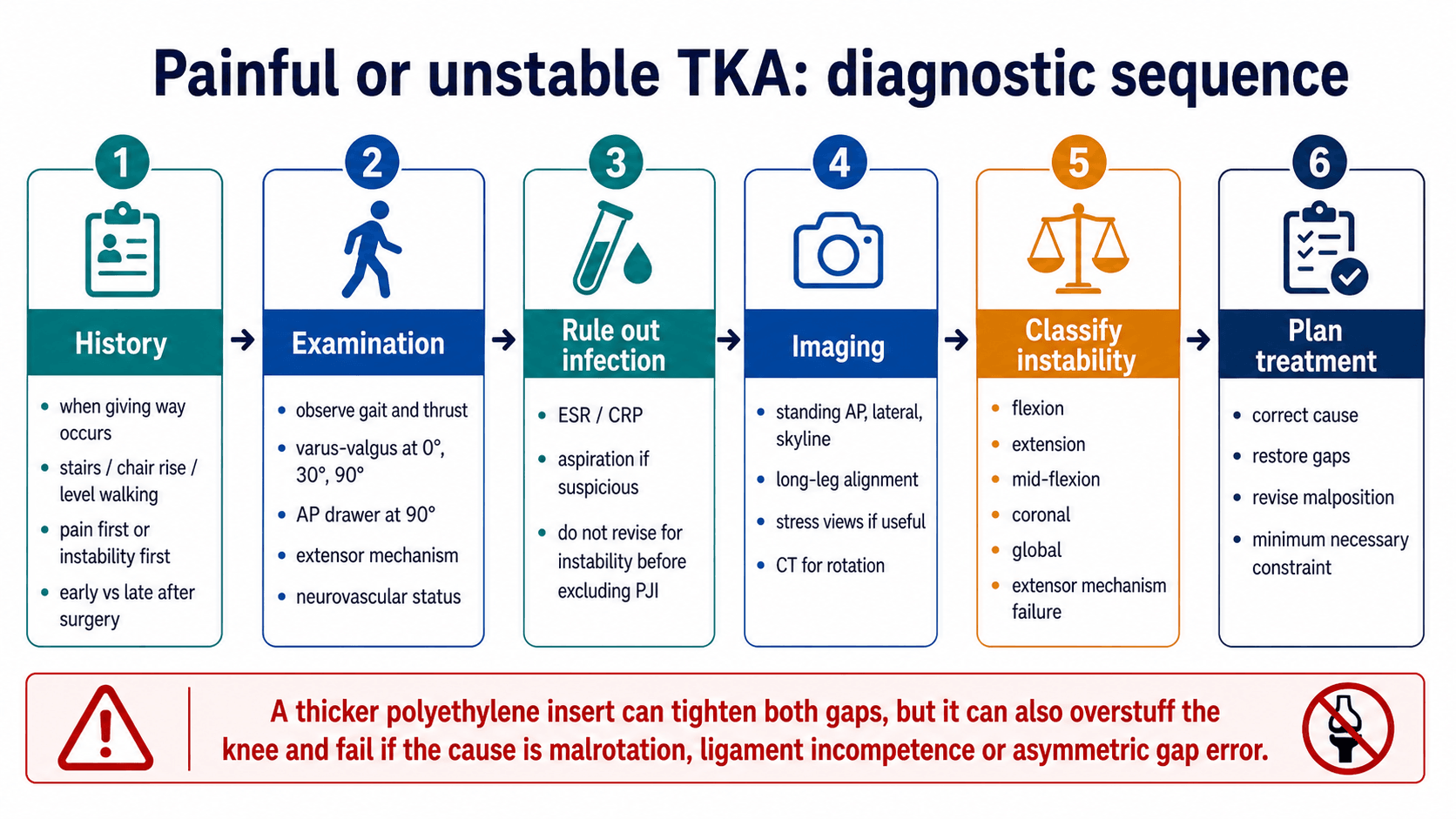
- “A thicker polyethylene insert tightens flexion and extension together; it cannot selectively fix a flexion gap problem without risking stiffness or overstuffing.
- “In a CR TKA, PCL incompetence is a classic cause of flexion instability; conversion to PS may be enough only if collaterals and component position are acceptable.
- “In revision, reconstruct the platform first: infection status, fixation, component position, bone loss, joint line, posterior offset and ligament competence.
The question is not “flexion instability equals PS” or “global instability equals hinge”. The surgeon must decide whether the cause is infection, component malposition, PCL failure, collateral incompetence, joint-line elevation, bone loss, posterior offset loss, tibial slope, extensor mechanism failure or true global laxity.
- Likely Problem
- Flexion gap too large.
- Correction Principle
- Increase posterior femoral offset, reduce excessive slope, correct PCL strategy, revise malrotation if present.
- Likely Problem
- Extension gap too large.
- Correction Principle
- Restore distal femoral joint line with distal augments; do not rely on thicker insert alone.
- Likely Problem
- Mid-flexion instability.
- Correction Principle
- Assess joint line, femoral component design/position, collateral isometry and coronal laxity.
- Likely Problem
- Collateral incompetence, asymmetric release, malalignment or bone loss.
- Correction Principle
- Correct alignment/bone loss and use VVC/CCK or hinge if soft tissues cannot stabilise the knee.
- Likely Problem
- Possible periprosthetic joint infection.
- Correction Principle
- Investigate infection before any instability revision.
D-P-SWhat changes gaps | PJIBefore revision | CPVHConstraint ladder |
|---|---|---|
D Distal femur Mainly changes extension gap. | P Pain pattern Pain may be infection, loosening, malrotation, instability or extensor failure. | C CR PCL and collaterals competent. |
P Posterior condyles Mainly changes flexion gap and posterior offset. | J Joint aspiration Use when infection suspicion persists after blood tests. | P PS PCL deficient but collaterals competent. |
S Slope More posterior tibial slope opens flexion gap, especially in CR knees. | I Implant position Do not revise instability without assessing component position. | V VVC/CCK Coronal laxity with usable extensor mechanism. |
H Hinge Global instability or severe bone/ligament loss. | ||
Distal, posterior, slope. | Painful loose TKA: infection first. | Constraint rises only when soft-tissue control falls. |
GAPSSafe Revision Sequence
Hook:GAPS keeps the revision plan cause-based rather than insert-based.
Overview and Definitions
TKA balancing means creating a knee that is stable through the full arc of motion without excessive constraint, stiffness or asymmetric soft-tissue tension. It is a bone, ligament, implant and alignment problem at the same time.
The key definitions are practical:
- Meaning
- Space and soft-tissue tension with the knee at full extension.
- Why It Matters
- Affected mainly by distal femoral resection, posterior capsule, collateral tension and osteophytes.
- Meaning
- Space and soft-tissue tension at 90° flexion.
- Why It Matters
- Affected mainly by posterior condylar resection, femoral sizing, posterior offset, tibial slope and PCL status.
- Meaning
- Medial and lateral compartments open evenly under tension.
- Why It Matters
- Needed for coronal stability and central tracking.
- Meaning
- One compartment remains tighter or looser than the other.
- Why It Matters
- Requires selective release, recut, component correction or constraint depending cause.
- Meaning
- Mechanical stability built into the implant.
- Why It Matters
- Useful when soft tissues cannot stabilise the knee, but it increases load transfer to fixation interfaces.
Surgically Relevant Anatomy
The knee is stabilised by bone cuts, implant geometry and soft tissues. A balanced TKA depends on respecting how each structure behaves in extension, flexion and mid-flexion.
- Main Role
- Primary medial restraint, especially against valgus stress.
- Operative Relevance
- Over-release in varus TKA causes medial instability and may force higher constraint.
- Main Role
- Medial tightness near the joint line.
- Operative Relevance
- Often released early after osteophyte removal in varus knees.
- Main Role
- Posterior stabiliser and flexion-gap restraint in CR TKA.
- Operative Relevance
- Incompetence creates flexion instability; excessive tension can limit flexion or lift off.
- Main Role
- Lateral stability, especially in valgus knees.
- Operative Relevance
- Release sequence depends on whether tightness is in extension, flexion or both.
- Main Role
- Lateral extension tightness.
- Operative Relevance
- Release if valgus knee is tight mainly in extension.
- Main Role
- Posterolateral flexion tightness.
- Operative Relevance
- Release cautiously if valgus knee is tight mainly in flexion.
- Main Role
- Block extension and distort gap assessment.
- Operative Relevance
- Remove osteophytes before judging true extension balance.
- Main Role
- Patellar tracking and active extension.
- Operative Relevance
- Extensor failure can mimic instability and changes reconstruction choices.
Pathophysiology
Instability occurs when the soft-tissue envelope and implant geometry no longer control the tibia under load. The mechanism is usually mechanical, but pain and swelling from infection or loosening can make the knee feel unstable; this is why infection and fixation are checked before revising gaps.
- What Happens Biomechanically
- Flexion gap opens because the femur is effectively undersized posteriorly.
- Clinical Pattern
- Giving way in flexion, stairs difficulty and AP drawer at 90°.
- What Happens Biomechanically
- Tibia rests in a posteriorly sloped platform, increasing flexion laxity.
- Clinical Pattern
- Flexion instability, especially in CR TKA with PCL insufficiency.
- What Happens Biomechanically
- Extension gap opens more than flexion gap.
- Clinical Pattern
- Recurvatum tendency or instability in stance.
- What Happens Biomechanically
- Flexion gap becomes asymmetric and patellofemoral tracking may fail.
- Clinical Pattern
- Pain, stiffness, patellar symptoms or asymmetric flexion instability.
- What Happens Biomechanically
- The knee cannot resist varus-valgus load despite acceptable bone cuts.
- Clinical Pattern
- Coronal opening at 0°, 30° or 90°; may require VVC/CCK or hinge.
- What Happens Biomechanically
- Collateral isometry and patellofemoral mechanics change through mid-flexion.
- Clinical Pattern
- Possible mid-flexion instability, stiffness or extensor symptoms.
Primary TKA Balancing
Before releases
Do not release soft tissue until the basics are correct:
- Confirm the tibial cut is not in unintended varus or valgus.
- Confirm distal femoral resection and femoral rotation are appropriate.
- Remove posterior, medial and lateral osteophytes.
- Clear meniscal remnants and loose bodies that tent the collateral ligaments.
- Test with spacer blocks or trials at extension, 30° and 90°.
- Correct obvious bone-cut error before sacrificing ligament.
Varus knee release sequence
- Action
- Remove medial tibial and femoral osteophytes.
- Decision Point
- If this corrects the gap, stop releasing.
- Action
- Release deep MCL and posteromedial capsule from proximal tibia.
- Decision Point
- Good first soft-tissue step for most fixed varus knees.
- Action
- Release semimembranosus if posteromedial tightness persists.
- Decision Point
- Useful when extension and posteromedial flexion remain tight.
- Action
- Pie-crust or cautiously lengthen superficial MCL if severe medial tightness remains.
- Decision Point
- Risk is medial instability; reassess repeatedly.
- Action
- Consider reduction osteotomy, sliding medial epicondyle osteotomy or constraint for severe fixed deformity.
- Decision Point
- Do this instead of uncontrolled MCL destruction.
Valgus knee release sequence
- Likely Structure
- IT band and posterolateral capsule.
- Surgical Response
- Release extension-side lateral structures first and reassess.
- Likely Structure
- Popliteus or LCL depending pattern.
- Surgical Response
- Release flexion-side structure cautiously; avoid creating lateral flexion laxity.
- Likely Structure
- LCL and broader posterolateral complex.
- Surgical Response
- Sequential release; high chance of needing increased constraint.
- Likely Structure
- Attenuated MCL in severe valgus.
- Surgical Response
- Do not rely on soft-tissue release alone; consider VVC/CCK or hinge.
Clinical Assessment of the Unstable TKA
History
Ask when the knee gives way. Flexion instability is classically worse with stairs, descending slopes, rising from a chair and activities that load the knee in flexion. Extension instability or recurvatum is more obvious during stance and level walking. Mid-flexion instability may feel vague: “not trusting the knee” between full extension and deep flexion.
Key history points:
- Timing after primary TKA: immediate, early, late or after trauma.
- Pain first or instability first.
- Recurrent effusions or swelling after activity.
- Stairs, chair rise, pivoting, level walking and downhill walking.
- Previous infection, wound issues, manipulation, stiffness or revision.
- Implant type if known: CR, PS, constrained condylar, rotating hinge.
- Neuromuscular disease, extensor mechanism symptoms or falls.
Examination technique
- How To Perform It
- Watch walking from front, side and back; look for varus/valgus thrust, recurvatum, limp and extensor lag.
- Positive Meaning
- Thrust suggests coronal instability or malalignment; recurvatum suggests extension instability or neuromuscular control problem.
- How To Perform It
- Patient supine, knee fully extended, stabilise femur and apply varus/valgus force at ankle.
- Positive Meaning
- Opening in extension suggests collateral incompetence, excessive extension gap or global instability.
- How To Perform It
- Unlock the knee slightly and repeat stress testing.
- Positive Meaning
- Isolates collateral behaviour better than full extension; useful for mid-flexion/coronal laxity.
- How To Perform It
- Knee flexed to 90°, foot supported, stress through the tibia.
- Positive Meaning
- Opening in flexion suggests flexion-gap asymmetry or collateral incompetence in flexion.
- How To Perform It
- Stabilise foot, flex knee to 90°, translate tibia anterior and posterior.
- Positive Meaning
- Excess AP translation suggests flexion instability, PCL failure in CR TKA or post-cam problems in PS TKA.
- How To Perform It
- Test coronal stability around 30° to 60° with the patient relaxed.
- Positive Meaning
- Instability here with stable endpoints supports mid-flexion instability.
- How To Perform It
- Assess active straight-leg raise, extensor lag, patellar tracking and apprehension.
- Positive Meaning
- Extensor failure or patellar instability can mimic giving way and changes reconstruction plan.
Differential diagnosis of the painful or "giving-way" TKA
The complaint of a knee that gives way is not specific. Several diagnoses present similarly and must be separated before any constraint or insert decision, because the wrong label leads to the wrong operation.
- Discriminating Features
- Objective laxity on stress at a defined flexion angle, recurrent effusions, pattern fits a specific gap.
- Key Test or Pitfall
- Stress at 0°, 30° and 90°; document the gap that opens.
- Discriminating Features
- Rest and night pain, raised CRP/ESR, effusion, sometimes warmth; instability may be a late effect of bone or soft-tissue destruction.
- Key Test or Pitfall
- ESR, CRP and aspiration with cell count, differential and culture before labelling as mechanical.
- Discriminating Features
- Start-up pain, progressive radiolucent lines, component migration or subsidence.
- Key Test or Pitfall
- Serial radiographs and comparison; loosening needs revision not insert exchange.
- Discriminating Features
- Buckling on stairs, extensor lag, quadriceps weakness, patellar maltracking; the knee gives way without true coronal laxity.
- Key Test or Pitfall
- Active straight-leg raise and extensor lag are easily missed if only collaterals are tested.
- Discriminating Features
- Anterior pain, apprehension, lateral tracking, clunk; often from component malrotation.
- Key Test or Pitfall
- Skyline view and CT rotation; do not treat as a tibiofemoral problem.
- Discriminating Features
- Pain, stiffness, patellar symptoms and asymmetric flexion gap rather than uniform laxity.
- Key Test or Pitfall
- CT rotational profile; soft-tissue release cannot fix a malrotated component.
- Discriminating Features
- Generalised giving way, falls, recurvatum, weakness out of proportion to mechanical findings.
- Key Test or Pitfall
- Neurological examination; bracing and rehabilitation rather than revision.
Investigations
What to request
- Standing AP, lateral and skyline radiographs of the knee.
- Full-length standing hip-to-ankle alignment radiograph.
- Comparison with prior radiographs to assess subsidence, loosening and joint-line change.
- Stress radiographs when clinical laxity needs documentation.
- CT rotational profile for suspected femoral or tibial component malrotation.
- ESR, CRP and aspiration when infection is possible.
- Consider bone scan or SPECT/CT selectively when loosening is unclear and infection has been addressed.
What to measure
- How To Assess
- Full-length standing film: femoral head centre to ankle centre through knee.
- Why It Changes Treatment
- Malalignment may drive coronal thrust and demands component or osteotomy-level correction.
- How To Assess
- AP knee and long-leg films.
- Why It Changes Treatment
- Varus tibial or valgus/varus femoral error can create asymmetric gaps.
- How To Assess
- True lateral radiograph.
- Why It Changes Treatment
- Excess slope increases flexion gap, especially in CR TKA.
- How To Assess
- Lateral radiograph and comparison to pre-op/early post-op if available.
- Why It Changes Treatment
- Loss of offset opens flexion gap and can cause flexion instability.
- How To Assess
- Compare with fibular head, adductor tubercle or prior films.
- Why It Changes Treatment
- Elevation can contribute to mid-flexion instability, patellar problems and extensor dysfunction.
- How To Assess
- CT using recognised femoral and tibial rotational references.
- Why It Changes Treatment
- Malrotation can cause flexion-gap asymmetry, patellar maltracking, stiffness and pain.
- How To Assess
- Radiolucent lines, migration, osteolysis, CT if needed.
- Why It Changes Treatment
- Loose or deficient components need revision reconstruction, not soft-tissue-only treatment.
Management Principles
- Treatment
- Physiotherapy for quadriceps/hip strength, gait retraining and proprioception.
- Limit
- Does not correct mechanical gap mismatch.
- Treatment
- Functional brace and activity modification.
- Limit
- Temporary or palliative option; monitor progression.
- Treatment
- Strengthening, swelling control and careful review.
- Limit
- Persistent recurrent effusion or objective drawer needs surgical planning.
- Treatment
- Do not start definitive instability treatment until infection pathway is complete.
- Limit
- Missed infection makes revision fail.
Isolated insert exchange is unsafe when instability is due to malrotation, malalignment, loose components, component undersizing, bone loss, PCL failure with a CR design, collateral incompetence, extensor mechanism failure or infection. It may be considered only when components are well-fixed, well-positioned, infection is excluded and both gaps can be corrected without overstuffing.
Genu recurvatum (hyperextension) is one of the three Cottino tibiofemoral instability patterns but its management is distinct and examinable:
- The mechanism: an extension gap that is too large / a distal femur over-resected (or a knee that hyperextends preoperatively) lets the knee fall into hyperextension; it is strongly associated with neuromuscular and connective-tissue conditions - classically poliomyelitis (where quadriceps weakness makes patients lock the knee in recurvatum to stand), and also rheumatoid/Charcot/Ehlers-Danlos knees.
- Intra-operative prevention (the counter-intuitive bit): to treat/prevent recurvatum you tighten the extension gap - under-resect (or build up/augment) the distal femur so the extension gap is relatively snug, and avoid excessive posterior tibial slope; this is the opposite of correcting a flexion contracture.
- The neuromuscular caveat: in a polio/quadriceps-deficient knee, a small degree of recurvatum may be functionally necessary for the patient to stand - over-correcting it can leave them unable to lock the knee; these patients often need a constrained/rotating-hinge implant or bracing rather than relying on soft-tissue balance.
- The pitfall: recurvatum tends to recur if the underlying muscle imbalance is not addressed - it is not simply a gap-cut problem.
Exam point: recurvatum is treated by tightening the extension gap (under-resect/augment the distal femur, limit slope), but in the polio/neuromuscular knee preserve the protective recurvatum or use a hinge - do not balance it like an ordinary extension-instability.
Complications and Failure Management
- Cause
- Posterior offset not restored, excessive slope persists, PCL failure not addressed.
- Prevention or Salvage
- Revise femur/tibia as needed; PS or VVC depending collateral competence.
- Cause
- Overstuffed knee, excessive insert thickness, joint-line error.
- Prevention or Salvage
- Correct gap cause rather than indiscriminate insert upsizing.
- Cause
- Collateral incompetence underestimated.
- Prevention or Salvage
- Increase to VVC/CCK or hinge; reconstruct bone loss and alignment.
- Cause
- High constraint without adequate fixation or bone support.
- Prevention or Salvage
- Use stems, augments, cones/sleeves and appropriate fixation strategy.
- Cause
- Pain and instability treated as mechanical only.
- Prevention or Salvage
- PJI workup before revision and cultures at surgery when indicated.
- Cause
- Exposure injury, chronic patellar maltracking or unrecognised extensor deficit.
- Prevention or Salvage
- Plan extensile exposure carefully; reconstruct extensor mechanism when needed.
Operative Technique
Revision for instability: PIPADRAW sequence
- What The Surgeon Does
- Supine, tourniquet available, previous incision planned, full limb accessible for alignment and stress testing.
- Pitfall
- Poor exposure makes component removal and gap assessment unreliable.
- What The Surgeon Does
- Have image intensifier if needed, extraction tools, augments, stems, cones/sleeves, PS, VVC/CCK and hinge options available.
- Pitfall
- Starting without the next constraint level can force a compromised reconstruction.
- What The Surgeon Does
- Antibiotics after cultures if infection concern, extensile exposure plan, aspiration/cultures as indicated.
- Pitfall
- Do not ignore infection because the referral says instability.
- What The Surgeon Does
- Use prior midline incision where safe; medial parapatellar arthrotomy is common; plan quadriceps snip or tibial tubercle osteotomy if exposure is difficult.
- Pitfall
- Avulsing the extensor mechanism changes the entire reconstruction.
- What The Surgeon Does
- Assess polyethylene wear, PCL status if CR, collateral integrity, extensor mechanism, component fixation and bone loss.
- Pitfall
- Do not remove well-fixed components before confirming why the knee is unstable.
- What The Surgeon Does
- Remove failed components when needed; rebuild tibial platform and femoral joint line; restore posterior offset and correct slope/rotation.
- Pitfall
- A thicker insert cannot correct a malpositioned femoral or tibial component.
- What The Surgeon Does
- Protect patellar tendon, MCL, LCL, popliteus, posterior capsule, popliteal vessels and peroneal nerve in valgus knees.
- Pitfall
- Peroneal nerve risk rises with valgus correction and flexion contracture correction.
- What The Surgeon Does
- Use stems for load sharing when constraint, bone loss or augments increase interface stress; use augments/cones/sleeves for bone defects.
- Pitfall
- Constraint without fixation support increases loosening risk.
- What The Surgeon Does
- Confirm tracking, stability at 0°, 30°, 60° and 90°, ROM, patella tracking and neurovascular status; brace if soft-tissue concern.
- Pitfall
- Failure to document the final stability arc leaves uncertainty after revision.
Guidelines, Registries & Global Practice
Global epidemiology
Instability is one of the leading mechanical causes of TKA revision worldwide, consistently appearing alongside infection and stiffness as a top reason for early revision and alongside infection, loosening and wear for late revision. As polyethylene quality improved, the relative share of wear-driven failure fell and technique-sensitive causes such as instability became proportionally more important. Valgus deformity accounts for roughly 10 percent of primary TKA, and these knees carry the greatest balancing and constraint challenge.
Society guidance, side by side
There is no single dedicated international guideline for "TKA instability"; practice is shaped by arthroplasty society consensus, registry data and revision-burden reporting rather than by a single algorithm.
- Emphasis Relevant to Balancing and Instability
- Evidence-based work on the painful TKA stresses systematic workup, mandatory infection exclusion (ESR, CRP, aspiration) before attributing symptoms to a mechanical cause.
- Emphasis Relevant to Balancing and Instability
- Revision activity concentrated in networked revision centres (the revision-network model), so complex instability and constraint decisions are increasingly made by specialist revision teams.
- Emphasis Relevant to Balancing and Instability
- Principles-based teaching: diagnose the loose gap, correct the cause (alignment, rotation, offset, bone loss) and use the least constraint that stabilises the reconstructed knee.
- Emphasis Relevant to Balancing and Instability
- Supports staged, cause-based revision and structured periprosthetic infection pathways before mechanical revision for instability.
Registry evidence
- Relevance to Instability and Constraint
- Tracks revision indications including instability and the use of constrained and hinged implants; informs implant and constraint selection by survivorship.
- Relevance to Instability and Constraint
- Reports revision causes and implant survivorship, with instability a recurring early-revision indication and higher-constraint designs monitored for survival.
- Relevance to Instability and Constraint
- Captures contemporary revision burden and the share attributable to instability and mechanical complications.
- Relevance to Instability and Constraint
- Long-standing survivorship data and revision-cause reporting that frame instability within total revision burden.
High- versus limited-resource practice
- Typical Reality
- Full revision implant ladder (augments, cones/sleeves, stems, VVC and hinge), CT rotation, navigation/robotics and specialist revision centres available.
- Implication
- Reconstruction can be matched precisely to the cause and to residual soft-tissue competence.
- Typical Reality
- Restricted constraint inventory, limited revision implants, less access to CT and cross-sectional imaging, fewer revision-trained surgeons.
- Implication
- Greater emphasis on correct primary balancing and alignment; instability is harder to salvage so prevention matters more.
- Typical Reality
- Infection exclusion before mechanical revision is universal and low-cost (clinical assessment, ESR, CRP, aspiration).
- Implication
- The single non-negotiable step is affordable everywhere and prevents failed revision.
Controversies and Areas of Uncertainty
Several balancing questions remain genuinely unresolved, and a strong exam answer acknowledges the uncertainty rather than overstating dogma.
- Current Position
- Mechanical alignment remains the default reference; kinematic and functional alignment aim to reproduce native soft-tissue tension.
- Why It Is Unsettled
- Registry-scale survivorship advantage for kinematic alignment is not yet proven; balance is achieved by different philosophies.
- Current Position
- Meta-analysis shows near-identical gaps, with only around 1 mm or 1 degree difference in rotation and joint line.
- Why It Is Unsettled
- Differences are small and probably clinically minor; most surgeons use a hybrid approach.
- Current Position
- There is no universally accepted laxity threshold (in millimetres or degrees) that defines pathological instability.
- Why It Is Unsettled
- Testing positions and grading systems are inconsistent, so the same knee can be labelled differently.
- Current Position
- Joint-line elevation, femoral undersizing and reduced femoral radius of curvature are proposed.
- Why It Is Unsettled
- Most evidence is computational and cadaveric; clinical studies conflict and several factors are inconclusive.
- Current Position
- Sensors, navigation and robotics improve the precision of gap and load balancing.
- Why It Is Unsettled
- Improved precision has not yet translated into proven long-term survivorship or function gains.
- Current Position
- Use the least constraint that controls the corrected knee.
- Why It Is Unsettled
- The exact point at which a surgeon should step from PS to VVC, or VVC to hinge, is judgement-based, not rule-based.
The mechanical-vs-kinematic-vs-functional alignment debate becomes concrete with the CPAK classification (Coronal Plane Alignment of the Knee, MacDessi 2021) - the modern framework for phenotyping the native knee before deciding how to balance it:
- Two variables: (1) the arithmetic HKA (aHKA = MPTA - LDFA) = the constitutional limb alignment (varus, neutral or valgus), and (2) the joint-line obliquity (JLO = MPTA + LDFA) = whether the joint line is apex-distal, neutral or apex-proximal.
- Nine types (a 3x3 grid): combining varus/neutral/valgus constitutional alignment with three joint-line-obliquity bands gives CPAK Types I-IX, with Type I (constitutional varus + apex-distal joint line) the commonest phenotype.
- Why it matters for balancing: it makes explicit that most knees are not natively neutral - a mechanically aligned TKA cuts every knee to neutral with a horizontal joint line (changing the soft-tissue envelope and requiring releases), whereas kinematic/functional alignment aims to reproduce the patient's pre-arthritic CPAK phenotype (constitutional alignment and joint-line obliquity), theoretically needing fewer releases and giving more "natural" balance.
- The unresolved question: which CPAK phenotypes are safe to restore versus which should be corrected toward neutral (e.g. how much residual varus or joint-line obliquity is acceptable) - this is the live controversy, with no proven long-term survivorship winner yet.
Exam point: CPAK = aHKA (alignment) x JLO (joint-line obliquity) giving nine phenotypes; it frames the alignment debate as "restore the native phenotype (kinematic/functional) vs cut to neutral (mechanical)" and explains why balancing strategy depends on the knee's constitutional shape.
Clinical Scenarios
Practise clinical reasoning and management decisions out loud
“A patient has recurrent effusions and giving way when descending stairs 18 months after a cruciate-retaining TKA. The knee is stable in extension but has increased anterior-posterior translation at 90°.”
“During primary TKA for a severe valgus knee, the extension gap remains laterally tight after bone cuts and osteophyte removal. The medial side is attenuated.”
“A patient is referred 3 years after a posterior-stabilised TKA with pain, swelling and a feeling that the knee is unreliable in the middle of the range. Stress testing is convincing for stability at full extension and at 90°, but the knee opens medially and laterally when tested at 30° to 45°. Inflammatory markers are normal.”
Examine
- Gait: thrust or recurvatum
- Varus-valgus at 0°, 30°, 90°
- AP drawer at 90°
- Mid-flexion stress
- Extensor mechanism
Image
- Standing AP/lateral/skyline
- Long-leg alignment
- Compare prior films
- CT for rotation
- ESR/CRP and aspirate if suspicious
Correct
- Flexion: posterior offset/slope/PCL
- Extension: distal femoral joint line
- Asymmetric: release or recut
- Global: constraint after reconstruction
- Never miss infection
“Diagnose which gap is wrong, correct the cause, then choose the least constraint that controls the knee.”
Evidence Signals
Gap balancing versus measured resection
- The goal of TKA is symmetric balanced flexion and extension gaps.
- Gap balancing aims to tension the collaterals and make the femoral component parallel to the tibial cut in flexion.
- The review argues gap balancing can produce more rectangular flexion gaps, while acknowledging controversy.
Gap balancing meta-analysis
- Eight observational comparison studies were pooled.
- Overall gap differences did not differ significantly between techniques (pooled mean difference -0.09 mm).
- Gap balancing produced greater femoral external rotation (0.77 degrees) and more joint-line elevation (1.17 mm), but differences were around 1 mm or 1 degree.
References
- Daines BK, Dennis DA. Gap balancing vs. measured resection technique in total knee arthroplasty. Clin Orthop Surg. 2014;6(1):1-8. doi:10.4055/cios.2014.6.1.1.
- Moon YW, Kim HJ, Ahn HS, Park CD, Lee DH. Comparison of soft tissue balancing, femoral component rotation, and joint line change between the gap balancing and measured resection techniques in primary total knee arthroplasty: a meta-analysis. Medicine. 2016;95(39):e5006. doi:10.1097/MD.0000000000005006.
- Siddiqi A, Smith T, McPhilemy JJ, Ranawat AS, Sculco PK, Chen AF. Soft-Tissue Balancing Technology for Total Knee Arthroplasty. JBJS Rev. 2020;8(1):e0050. doi:10.2106/JBJS.RVW.19.00050.
- Stambough JB, Edwards PK, Mannen EM, Barnes CL, Mears SC. Flexion Instability After Total Knee Arthroplasty. J Am Acad Orthop Surg. 2019;27(17):642-651. doi:10.5435/JAAOS-D-18-00347.
- Cottino U, Sculco PK, Sierra RJ, Abdel MP. Instability After Total Knee Arthroplasty. Orthop Clin North Am. 2016;47(2):311-316. doi:10.1016/j.ocl.2015.09.007.
- Chang MJ, Lim H, Lee NR, Moon YW. Diagnosis, causes and treatments of instability following total knee arthroplasty. Knee Surg Relat Res. 2014;26(2):61-67. doi:10.5792/ksrr.2014.26.2.61.
- Mehta N, Burnett RA, Kahlenberg CA, Miller R, Chalmers B, Cross MB. Mid-Flexion Instability After Total Knee Arthroplasty: Diagnosis, Implant Design, and Outcomes. Orthopedics. 2023;46(1):e13-e19. doi:10.3928/01477447-20220719-01.
- Vajapey SP, Pettit RJ, Li M, Chen AF, Spitzer AI, Glassman AH. Risk Factors for Mid-Flexion Instability After Total Knee Arthroplasty: A Systematic Review. J Arthroplasty. 2020;35(10):3046-3054. doi:10.1016/j.arth.2020.05.026.
- Rossi R, Cottino U, Bruzzone M, Dettoni F, Bonasia DE, Rosso F. Total knee arthroplasty in the varus knee: tips and tricks. Int Orthop. 2019;43(1):151-158. doi:10.1007/s00264-018-4116-3.
- Alesi D, Meena A, Fratini S, et al. Total knee arthroplasty in valgus knee deformity: is it still a challenge in 2021? Musculoskelet Surg. 2022;106(1):1-8. doi:10.1007/s12306-021-00695-x.
- Rezaei A, Moon J, Lichtig A, et al. Precision soft tissue balancing: grid-assisted pie-crusting in total knee arthroplasty. Front Surg. 2024;11:1331902. doi:10.3389/fsurg.2024.1331902.
- Le DH, Goodman SB, Maloney WJ, Huddleston JI. Current modes of failure in TKA: infection, instability, and stiffness predominate. Clin Orthop Relat Res. 2014;472(7):2197-2200. doi:10.1007/s11999-014-3540-y.