Recognition and management of neurovascular complications following total knee arthroplasty including common peroneal nerve injury and vascular injuries
- Common peroneal nerve most vulnerable due to superficial course at fibular head
- Vascular injury rare but limb-threatening - requires emergency intervention
- Risk factors: valgus deformity, flexion contracture, RA, previous surgery
- Foot drop most common presentation - check ankle dorsiflexion immediately post-op
- Prevention: careful retraction, avoid excessive correction, knee flexion post-op
- “Viva scenario: Post-TKA foot drop - systematic approach to differentiation (peroneal nerve vs sciatic vs central cause) and management algorithm is essential. Know the anatomy of the popliteal fossa cold.
Critical Concepts for FRACS Examination:
-
Common peroneal nerve is the most commonly injured nerve in TKA - superficial location at fibular head makes it vulnerable to traction, compression, and direct injury
-
Vascular injury is rare (0.03-0.17%) but CATASTROPHIC - mortality up to 7%, amputation rate 10-42% if not recognized within 6-8 hours
-
Valgus correction greater than 10-15 degrees significantly increases nerve palsy risk due to lateral soft tissue stretching
-
Knee flexion post-operatively reduces tension on the peroneal nerve - splint in 30-45° flexion if nerve palsy develops
-
Cold, pulseless limb post-TKA is a surgical emergency - immediate vascular surgery consultation, do not delay for imaging if clinical signs clear
-
Most peroneal nerve palsies recover - 50-90% complete recovery, but may take 12-24 months
Epidemiology
Epidemiology of Neurovascular Injury
Nerve Injury
Common peroneal nerve palsy is the most frequent neurological complication following TKA, occurring in 0.3-1.3% of primary cases. [1,2] The incidence increases substantially in revision procedures and complex primary cases.
- Primary TKA
- 0.3-0.9%
- Revision TKA
- 2-3%
- High-Risk Cases
- Up to 9.5%
- Primary TKA
- 0.05-0.1%
- Revision TKA
- 0.1-0.3%
- High-Risk Cases
- Rare
- Primary TKA
- Very rare
- Revision TKA
- 0.1-0.2%
- High-Risk Cases
- Associated with hip pathology
- Primary TKA
- Very rare
- Revision TKA
- Case reports
- High-Risk Cases
- Often epidural-related
- Primary TKA
- 50-90%
- Revision TKA
- 40-70%
- High-Risk Cases
- Variable
Risk stratification by deformity:
- Valgus greater than 10°: 3.3% peroneal nerve palsy rate
- Valgus greater than 15°: 6-9.5% peroneal nerve palsy rate
- Flexion contracture greater than 20°: 4-5% nerve palsy rate [1,3]
Vascular Injury
Vascular complications are rare but carry significant morbidity and mortality:
- Overall incidence: 0.03-0.17% of TKA procedures [4,5]
- Popliteal artery injury most common vascular complication
- Delayed presentation (pseudoaneurysm, AVF) may occur weeks to months post-operatively
- Mortality rate: 5-7% when vascular injury occurs
- Amputation rate: 10-42% in delayed recognition [4]
Global and registry-level epidemiology, the side-by-side guideline comparison is consolidated in the dedicated Guidelines, Registries & Global Practice section below.
Anatomy
Critical Neurovascular Anatomy
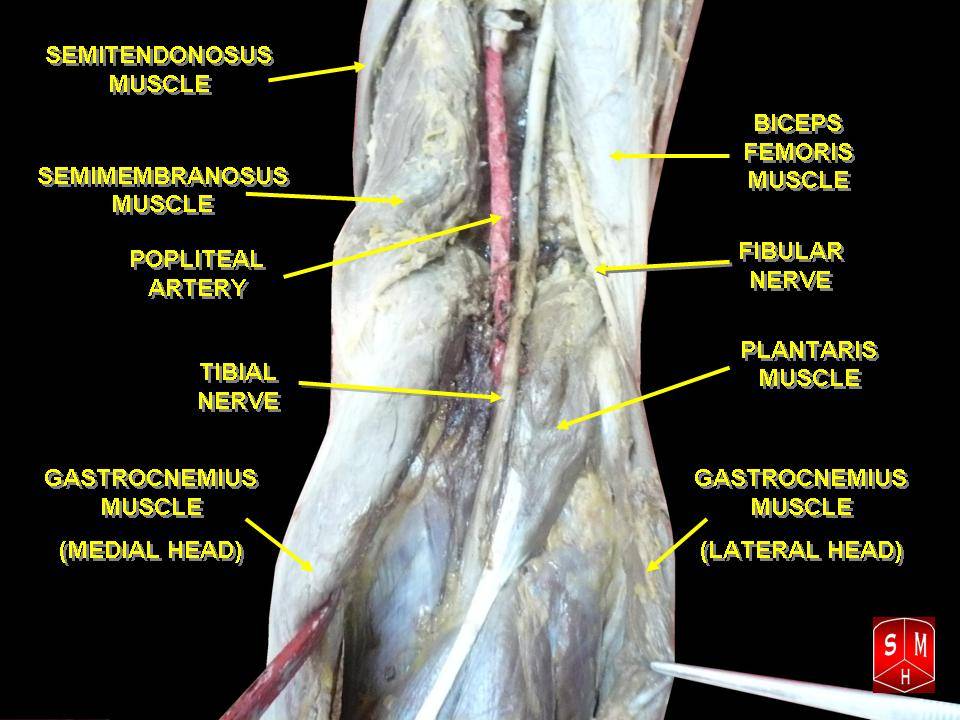
Understanding the anatomical relationships in the popliteal fossa and around the proximal fibula is essential for both prevention and management of neurovascular complications.
Popliteal Fossa Contents
- Tibial nerve - most posterior, crosses popliteal vessels from lateral to medial
- Popliteal vein - intermediate position
- Popliteal artery - deepest structure, closest to posterior capsule
- Popliteal artery lies approximately 5-10mm posterior to the posterior tibial cortex with knee in extension [6]
- Distance decreases with knee flexion beyond 90°
- Tethered by genicular branches - limited mobility
- Most vulnerable during posterior capsule release and tibial cutting
Common Peroneal Nerve Course
Course of common peroneal nerve:
- Originates from sciatic nerve at apex of popliteal fossa (variable level)
- Descends along medial border of biceps femoris tendon
- Wraps around fibular neck - superficial, vulnerable location
- Only 2-3mm of connective tissue between nerve and bone at fibular neck
- Divides into superficial and deep peroneal nerves
Why the peroneal nerve is vulnerable:
- Clinical Significance
- Limited excursion with limb lengthening
- Clinical Significance
- Prone to compression from positioning, retractors, dressings
- Clinical Significance
- Susceptible to traction injury with valgus correction
- Clinical Significance
- Watershed zone vulnerable to ischemia
- Clinical Significance
- Little protection from external compression
Proximal Tibiofibular Joint Anatomy
Clinical correlates:
- Lateral retractor placement must avoid fibular head
- Peroneal nerve can be directly visualized if in doubt
- Release of ITB and lateral structures places nerve at risk
- Proximal tibiofibular joint arthritis/osteophytes may alter anatomy
Vascular Anatomy Relevant to TKA
Popliteal artery branches in the knee region:
- Origin
- Popliteal, above joint
- Risk in TKA
- Medial release, posterior capsule
- Origin
- Popliteal, above joint
- Risk in TKA
- Lateral release
- Origin
- Posterior popliteal
- Risk in TKA
- Posterior cruciate ligament
- Origin
- Popliteal, below joint
- Risk in TKA
- Tibial preparation
- Origin
- Popliteal, below joint
- Risk in TKA
- Lateral tibial exposure
High-risk maneuvers for popliteal artery injury:
- Posterior capsule release (closest proximity)
- Posterior tibial osteophyte removal
- Oscillating saw during tibial cut (over-penetration)
- Anterior tibial retractor placement (impingement)
- Tibia extraction after cementation
Classification
Classification of Injury Type and Severity
Classifying neurovascular injury after TKA serves two purposes in the viva: it communicates severity/prognosis (which drives whether you observe, decompress, or repair) and it directs timing of intervention.
Seddon and Sunderland Nerve Injury Classification
The peroneal palsy that follows TKA is graded with the same framework used for any peripheral nerve injury. The grade is the single most important determinant of recovery potential.
- Conduction block from compression/ischaemia, axon and connective tissue intact
- No Wallerian degeneration; sensory often spared more than motor
- Recovery expected over days to weeks (up to ~12 weeks)
- Basis for most "traction/compression" palsies that recover with dressing release and knee flexion
- Axonal disruption with intact endoneurial tubes (Wallerian degeneration occurs distally)
- Recovery by axonal regrowth at roughly 1mm/day - months, often incomplete
- Detectable on EMG/NCS once degeneration is established (3-4 weeks)
- Complete transection or dense intraneural scar - no spontaneous recovery
- Rare in TKA; if recognised intra-operatively as transection, repair is indicated
- Distinguished from axonotmesis only by failure of recovery or operative findings
Vascular Injury Classification
- Lesion
- Thrombosis / intimal flap
- Mechanism in TKA
- Tourniquet on diseased vessel, traction, hyperextension kinking
- Typical Timing
- Intra-op to hours
- Lesion
- Laceration / transection
- Mechanism in TKA
- Saw over-penetration, posterior retractor, osteophyte removal
- Typical Timing
- Intra-op
- Lesion
- Transection with ischaemia + bleeding
- Mechanism in TKA
- Direct sharp injury to popliteal artery
- Typical Timing
- Intra-op
- Lesion
- Pseudoaneurysm
- Mechanism in TKA
- Partial wall injury, contained leak
- Typical Timing
- Days to weeks
- Lesion
- Arteriovenous fistula
- Mechanism in TKA
- Concurrent artery + vein injury
- Typical Timing
- Weeks to months
According to PubMed, in the Pennsylvania Hospital series (Calligaro et al.) acute arterial complications were grouped by mechanism (ischaemia, bleeding, ischaemia plus bleeding, pseudoaneurysm) and by timing - roughly half were recognised on the day of surgery and half over the first to fifth post-operative day, underscoring why delayed recognition drives morbidity.
Contributing Factors
Patient and Surgical Risk Factors
Pre-operative Risk Factors
- Greater than 10° valgus: 3-4× increased nerve palsy risk
- Greater than 15° valgus: 8-10× increased risk
- Lateral soft tissue contracture requires extensive release
- Correction "lengthens" the lateral structures including peroneal nerve
- Consider staged correction or constrained implants
- Greater than 20° fixed flexion: significantly elevated risk
- Posterior capsule release required - close to popliteal vessels
- Extension restoration elongates neurovascular structures
- Combined with valgus = highest risk scenario
- Lower nerve palsy risk than valgus
- Vascular injury risk similar
- Medial release does not tension peroneal nerve
Intra-operative Risk Factors
- Mechanism
- Direct compression of peroneal nerve
- Prevention Strategy
- Place retractor on proximal tibia, not fibula
- Mechanism
- Traction injury to peroneal nerve
- Prevention Strategy
- Staged correction, avoid greater than 10-15° correction
- Mechanism
- Direct injury to popliteal vessels
- Prevention Strategy
- Subperiosteal dissection, knee flexion, bent retractor
- Mechanism
- Laceration of posterior vessels
- Prevention Strategy
- Control depth, use oscillating saw with guard
- Mechanism
- Ischemic nerve injury
- Prevention Strategy
- Limit to less than 90-120 minutes, consider tourniquet-free
- Mechanism
- Compartment syndrome, compression
- Prevention Strategy
- Loose dressings, monitor post-operatively
- Mechanism
- Compression of neural structures
- Prevention Strategy
- Meticulous hemostasis, consider drain
Clinical Presentation
Recognition of Neurovascular Injury
Nerve Injury Presentation
- Foot drop - inability to dorsiflex ankle
- Weakness of toe extensors (EHL, EDL)
- Weakness of ankle eversion (peroneus longus and brevis)
- Foot slap during gait
- Steppage gait (high-stepping to clear foot)
- Numbness over dorsum of foot
- First web space sensation (deep peroneal territory)
- Lateral leg (superficial peroneal territory)
- May spare lateral foot (sural nerve)
- May be masked by regional anesthesia initially
- Typically recognized when block wears off (12-24 hours)
- MUST examine before discharge if outpatient
- Document ankle dorsiflexion power systematically
- Ankle dorsiflexion (L4-5) - grade 0-5
- Great toe extension (L5) - grade 0-5
- Ankle eversion (L5-S1) - grade 0-5
- Sensation first web space (deep peroneal)
- Sensation dorsum of foot (superficial peroneal)
Although the common peroneal nerve is the most important and most-tested motor nerve injury after TKA, the most frequently injured nerve of all is the infrapatellar branch of the saphenous nerve, which crosses the front of the knee from medial to lateral and is divided by the standard medial parapatellar (or midline) approach in a large proportion of TKAs. The result is an area of numbness on the antero-lateral side of the incision and, in a minority, a painful neuroma at the medial end of the scar with pain on kneeling and a positive Tinel sign. It is usually a benign, well-tolerated sensory deficit that recovers or is ignored, but it is a genuine source of patient dissatisfaction and litigation, so it belongs in the consent discussion ("a patch of numbness beside the scar is expected"). A symptomatic neuroma is managed with desensitisation first, then injection, and excision/proximal transposition for the refractory case. The exam point: distinguish this common benign sensory injury from the rare but serious peroneal motor palsy.
Vascular Injury Presentation
The "6 Ps" of Acute Limb Ischemia - MUST recognize immediately:
- Pain - severe, out of proportion, especially with passive stretch
- Pallor - white, waxy appearance of limb
- Pulselessness - absent pedal pulses (or new change from pre-op)
- Paresthesia - altered sensation, numbness
- Paralysis - motor weakness (late sign)
- Poikilothermia - cold limb, temperature difference
TIME IS CRITICAL - irreversible muscle necrosis begins at 6 hours of warm ischemia
Acute Arterial Injury:
- Clinical Features
- Acute hemorrhage, hypotension, hematoma
- Urgency
- Immediate surgery
- Clinical Features
- 6 Ps, cool limb, absent pulses
- Urgency
- Emergency - within 6 hours
- Clinical Features
- Delayed ischemia (hours), thrombus propagation
- Urgency
- Urgent - monitor closely
- Clinical Features
- Tense compartments, pain with passive stretch
- Urgency
- Emergent fasciotomies
Delayed Vascular Issues:
- Presentation
- Pulsatile mass, delayed bleeding, pain
- Timing
- Days to weeks
- Presentation
- Bruit, swelling, high-output failure
- Timing
- Weeks to months
- Presentation
- Calf swelling, pain, Homan's sign
- Timing
- Days to weeks
Differential Diagnosis of Post-TKA Foot Drop
- Clinical Features
- Ankle dorsiflexion weak, eversion weak, sensation dorsum foot
- Investigation
- Clinical, EMG at 3-4 weeks
- Clinical Features
- All below-knee motor/sensory loss
- Investigation
- Clinical, EMG, consider MRI spine/hip
- Clinical Features
- Back pain, bladder dysfunction, bilateral weakness
- Investigation
- Urgent MRI spine - neurosurgical emergency
- Clinical Features
- Back pain, dermatomal distribution, may have reflex changes
- Investigation
- MRI lumbar spine
- Clinical Features
- Upper motor neuron signs, other neurological findings
- Investigation
- CT/MRI brain
- Clinical Features
- Severe pain, tense compartments, late paralysis
- Investigation
- Clinical diagnosis, measure pressures if uncertain
Investigations
Imaging and Electrodiagnostics
Imaging in Neurovascular Injury:
- Indication
- Suspected vascular injury, pseudoaneurysm, DVT
- Findings
- Flow abnormalities, aneurysm, thrombus
- Indication
- Arterial injury, planning for intervention
- Findings
- Laceration, thrombosis, pseudoaneurysm
- Indication
- Nerve compression, hematoma localization
- Findings
- Hematoma, nerve edema, compression
- Indication
- Non-invasive vascular assessment
- Findings
- Arterial anatomy, occlusion
- Indication
- Diagnostic and therapeutic (embolization)
- Findings
- Gold standard for vascular injury
Nerve Conduction Studies / EMG:
- Not useful in acute setting (requires 2-3 weeks for Wallerian degeneration)
- Baseline at 3-4 weeks if no recovery
- Repeat at 3 months to assess recovery
- Useful to differentiate neurapraxia from axonotmesis
- Can localize level of lesion
Management Algorithm
Stepwise Management Approach
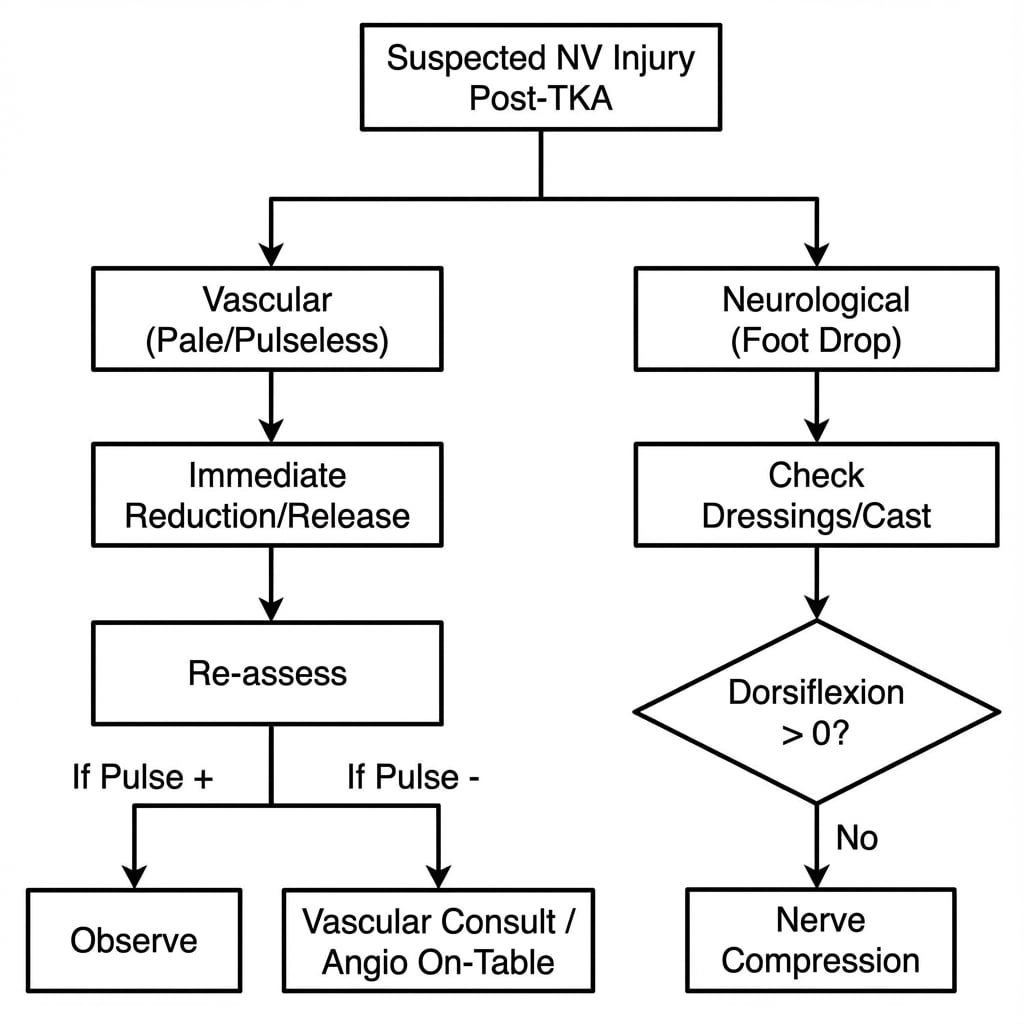
Acute Nerve Palsy Management
Step 1: Recognition and Documentation
- Document motor power (MRC grade 0-5)
- Document sensory examination
- Compare to pre-operative status if available
- Photograph any skin changes
Step 2: Remove Compressive Factors
- Loosen all dressings immediately
- Remove any circumferential bandages
- Release splint if present
- Ensure no external pressure on fibular head
Step 3: Positioning
- Flex knee to 30-45° to reduce nerve tension
- Avoid external rotation of leg
- Pad fibular head region
- Leg slightly elevated
Step 4: Rule Out Other Causes
- Epidural hematoma/abscess - check back pain, bladder, bilateral signs
- Compartment syndrome - check compartment tension
- Vascular injury - check pulses, perfusion
Step 5: Document and Communicate
- Inform patient and family
- Document in medical record
- Early referral to physiotherapy
- Consider early surgical exploration if concern for compressive hematoma
Acute Vascular Injury Management
VASCULAR EMERGENCY PROTOCOL:
- Recognize - cold, pulseless, painful limb
- Call for help - immediate vascular surgery consultation
- Position - limb at heart level (not elevated)
- Heparinize - systemic heparin if not contraindicated
- Image - CTA if stable, direct to OR if unstable
- Time - irreversible ischemia begins at 6 hours - do NOT delay
Do NOT wait for imaging if clinical diagnosis is clear - proceed to operating room
Management by Injury Type:
- Immediate Action
- Direct pressure, call vascular
- Definitive Treatment
- Primary repair or vein graft
- Immediate Action
- Heparinize, urgent vascular consult
- Definitive Treatment
- Thrombectomy ± bypass
- Immediate Action
- Emergency fasciotomies
- Definitive Treatment
- All 4 compartments, leave open
- Immediate Action
- Monitor if small, intervention if expanding
- Definitive Treatment
- Endovascular or open repair
- Immediate Action
- Usually not urgent
- Definitive Treatment
- Elective surgical or endovascular repair
Fasciotomy Technique:
- All 4 compartments must be released
- Single lateral incision can access anterior, lateral, and superficial posterior
- Separate posteromedial incision for deep posterior
- Leave wounds open - delayed primary closure or skin grafting
Surgical Technique
Operative Management Technique
Most peroneal palsies are managed non-operatively. Surgery is reserved for (1) intra-operative recognition of nerve transection, (2) a compressive haematoma, (3) failure to recover by 3-6 months (decompression/neurolysis), (4) established permanent foot drop (tendon transfer), and (5) any vascular injury.
no clinical or electrical recovery by ~3 months, or a documented compressive lesion.
- Supine or lateral; tourniquet optional and used judiciously
- Lazy-S or curvilinear incision over the fibular neck, behind the biceps femoris tendon
- Identify common peroneal nerve posterior to biceps femoris, trace distally around the fibular neck
- Release the fibrous arch/origin of peroneus longus (the classic constriction point)
- External neurolysis of epineurial fibrosis; decompress superficial and deep branches
- Intraneural neurolysis only if a discrete fascicular constriction is found
- Preserve the nerve's vascular supply; avoid devascularising mobilisation
Mont and colleagues found 30/31 patients (97%) improved and discontinued the AFO after decompression versus 3/9 (33%) managed non-operatively, supporting decompression when non-operative measures fail.
operating too early (most Sunderland I-II recover spontaneously); missing a more proximal sciatic lesion; iatrogenic injury during dissection at the fibular neck.
Complications
Complications of the Injury and its Treatment
Neurovascular injury after TKA is itself a complication, but it generates its own cascade of secondary complications that the examiner expects you to anticipate, recognise, and manage.
- Approximate Frequency / Context
- ~10-50% of palsies fail to fully recover (varies widely by series)
- Prevention
- Avoid over-correction of valgus; protect nerve; release dressings early
- Recognition & Management
- AFO; tendon transfer after ~12 months if no recovery
- Approximate Frequency / Context
- After prolonged ischaemia/reperfusion or bleeding
- Prevention
- Limit tourniquet time; meticulous haemostasis; high index of suspicion
- Recognition & Management
- Pain on passive stretch, tense compartments; emergency 4-compartment fasciotomy
- Approximate Frequency / Context
- 10-42% with delayed recognition of vascular injury
- Prevention
- Recognise ischaemia early; do not delay for imaging when clear
- Recognition & Management
- Urgent revascularisation within the ischaemic window
- Approximate Frequency / Context
- Following late revascularisation
- Prevention
- Timely revascularisation; consider fasciotomy
- Recognition & Management
- Monitor CK, renal function, potassium; fluids, renal support
- Approximate Frequency / Context
- Delayed (days to months)
- Prevention
- Careful posterior dissection; recognise partial wall injury
- Recognition & Management
- Duplex/CTA; endovascular or open repair
- Approximate Frequency / Context
- After significant nerve injury
- Prevention
- Early mobilisation, analgesia, nerve care
- Recognition & Management
- Multidisciplinary pain management
- Approximate Frequency / Context
- ~5-7% historically with vascular injury (lower in modern series)
- Prevention
- Early recognition, haemodynamic resuscitation
- Recognition & Management
- Resuscitation, haemorrhage control, ITU support
The dominant theme examiners probe is that delayed recognition - not the injury itself - is the driver of catastrophic outcome and of litigation. A documented pre-operative neurovascular status and a documented timely post-operative re-examination are your protection both clinically and medicolegally.
Postoperative Care
Post-operative and Rehabilitation Care
After a Peroneal Nerve Palsy
- Positioning: maintain knee flexion (30-45 degrees) initially to offload the nerve; pad the fibular head; avoid external rotation of the limb.
- Orthotics: fit an ankle-foot orthosis early to allow safe mobilisation and prevent equinus contracture.
- Physiotherapy: passive ankle range of motion to prevent contracture, strengthening of any preserved muscles, gait re-education with the AFO.
- Surveillance: serial documented neurological examinations (weekly initially); baseline EMG/NCS at 3-4 weeks; repeat at ~3 months to judge reinnervation and prognosis.
- Counselling: honest discussion that recovery, when it occurs, typically spans 12-24 months and may be incomplete.
After a Vascular Repair
- Joint care with the vascular team: monitor distal pulses, Doppler signals, capillary refill and compartment status hourly initially.
- Vigilance for compartment syndrome after reperfusion; low threshold for fasciotomy.
- Anticoagulation/antiplatelet regimen as directed by vascular surgery.
- Monitor for reperfusion injury (CK, renal function, electrolytes).
- Delayed primary closure or split-skin grafting of fasciotomy wounds.
Rehabilitation Milestones
- Nerve Injury Focus
- Dressing release, knee flexion, document exam
- Vascular Injury Focus
- Perfusion monitoring, fasciotomy if needed
- Nerve Injury Focus
- AFO, physiotherapy, baseline EMG at 3-4 weeks
- Vascular Injury Focus
- Wound care, anticoagulation, graft surveillance
- Nerve Injury Focus
- Repeat EMG; assess reinnervation
- Vascular Injury Focus
- Duplex surveillance of repair/graft
- Nerve Injury Focus
- Decide on neurolysis if no recovery
- Vascular Injury Focus
- Manage claudication, late stenosis
- Nerve Injury Focus
- Tendon transfer for permanent deficit
- Vascular Injury Focus
- Long-term vascular follow-up
Outcomes
Prognosis and Recovery
Peroneal Nerve Palsy Outcomes
Recovery Rates:
- Complete recovery: 50-90% (literature varies widely)
- Partial recovery: 10-30%
- No recovery: 5-20%
- Mean recovery time: 12-18 months
- Maximum recovery typically by 2-3 years
- Better Prognosis
- Delayed onset (dressings)
- Worse Prognosis
- Immediate post-operative
- Better Prognosis
- Partial palsy
- Worse Prognosis
- Complete palsy
- Better Prognosis
- Evidence of reinnervation
- Worse Prognosis
- No motor unit recruitment
- Better Prognosis
- Traction/compression
- Worse Prognosis
- Direct transection
- Better Prognosis
- No diabetes or neuropathy
- Worse Prognosis
- Diabetic neuropathy present
- Better Prognosis
- Early dressing release, AFO
- Worse Prognosis
- Delayed recognition
Functional Outcomes:
- Most patients with complete recovery have normal function
- Patients with AFO-dependent foot drop can still ambulate
- Patient satisfaction lower than uncomplicated TKA
- Consider revision or tendon transfer for permanent deficit
Vascular Injury Outcomes
Outcomes by Recognition Timing:
- Limb Salvage Rate
- 90-95%
- Amputation Rate
- 5-10%
- Limb Salvage Rate
- 70-80%
- Amputation Rate
- 20-30%
- Limb Salvage Rate
- 40-60%
- Amputation Rate
- 40-60%
Long-term Outcomes:
- Patients with limb salvage may have claudication
- Repeat intervention may be required
- Chronic pain and disability common
- Litigation risk significant
Medicolegal Considerations
- Neurovascular injury is a recognized complication of TKA
- Documentation of consent discussion essential
- Pre-operative neurological status should be documented
- Post-operative examination must be timely and documented
- Delayed recognition is the most common source of litigation
Prevention Strategies
Surgical Techniques to Minimize Risk
Pre-operative Planning
- Document pre-operative neurological status (ankle dorsiflexion, sensation)
- Assess peripheral pulses and ABI if vascular disease suspected
- Consider vascular surgery consultation for calcified vessels/prior vascular surgery
- Review previous surgical records for anatomical variations
- Inform patient of increased risk if risk factors present
- Templating to predict required correction
- Consider constrained implants for severe deformity (reduce soft tissue release)
- Plan for staged correction if greater than 15° valgus
- Have vascular surgery backup if high-risk case
Intra-operative Prevention
- Lateral retractor on proximal tibia, NOT fibular head
- If placing lateral retractor, do so with knee flexed
- Consider visualizing peroneal nerve in high-risk cases
- Gentle, intermittent retraction - avoid prolonged pressure
- Limit valgus correction to 10-15° in single stage
- For severe valgus, consider constrained implant to reduce release
- Staged correction for extreme deformity
- Accept slight under-correction rather than nerve palsy
- Wider cuff (10cm minimum) distributes pressure
- Lower inflation pressure (limb occlusion pressure + 100mmHg)
- Limit duration when possible
- Consider tourniquet-free TKA in high-risk patients
- Avoid excessive tension on closure
- Loose, well-padded dressings
- Splint in slight flexion (20-30°) in high-risk cases
- Avoid circumferential tight bandages
In the highest-risk knee — a severe fixed valgus deformity with a flexion contracture that needs extensive lateral release and significant lengthening of the lateral side — some surgeons perform a prophylactic decompression of the common peroneal nerve at the time of TKA, releasing it at the fibular neck (the constricting peroneus-longus arch) so the corrected, lengthened nerve is not tethered. The rationale is to pre-empt the traction palsy rather than treat it afterwards, and it is an adjunct to the standard preventive measures (staged or limited correction, constrained implants, avoiding excessive single-stage valgus correction, splinting in flexion). It remains debated and selective — the evidence is limited and it adds operative time and a second wound — so it is not routine, but it is a legitimate, examinable option for the extreme valgus / flexion-contracture knee. The exam point: know it exists and when it might be considered, while recognising the mainstay is still correction strategy and postoperative knee-flexion positioning.
Post-operative Monitoring
- Document pulses and ankle dorsiflexion in recovery
- Repeat examination when regional block wears off
- Monitor for compartment syndrome (especially if tourniquet used)
- Low threshold for dressing loosening if concerns
- Splint knee in 30-45° flexion for 48-72 hours
- Serial neurological examinations
- Early physiotherapy input
- Consider routine Doppler assessment if vascular concern
Guidelines, Registries & Global Practice
Global Epidemiology, Guidelines and Registry Evidence
Global Burden and Practice Variation
Total knee arthroplasty is among the highest-volume elective orthopaedic procedures worldwide, with over a million performed annually in the United States alone and rising volumes across Europe, the United Kingdom, Australia and Asia. Because neurovascular injury is rare, single-centre series under-represent it; the most reliable incidence figures come from large institutional cohorts and prospectively collected datasets. According to PubMed, the verified pooled picture is consistent across geographies: peroneal palsy in roughly 0.3-1.3% of primary TKA (higher with valgus deformity and revision), and arterial injury in roughly 0.03-0.17%.
Practice variation centres on three modifiable areas: tourniquet use (duration and whether used at all), deformity correction strategy (single-stage versus staged, constrained implants), and pre-operative vascular screening of patients with peripheral arterial disease. Tourniquet-free and limited-tourniquet TKA has gained traction in Europe and Australasia partly to reduce ischaemic nerve risk, whereas tourniquet use remains common in North America.
Guidance Comparison
- Relevant Position / Guidance
- No dedicated neurovascular-injury guideline; the AAOS surgical management of osteoarthritis of the knee CPG informs patient selection and shared decision-making, and emphasises documented informed consent for recognised complications
- Evidence Level / Status
- Consensus/CPG-based
- Relevant Position / Guidance
- Covers patient selection, optimisation and information-giving for primary hip/knee replacement; complications such as nerve and vascular injury fall under the consent and shared-decision recommendations rather than a specific algorithm
- Evidence Level / Status
- Guideline (GRADE-informed)
- Relevant Position / Guidance
- Best-practice principles for knee arthroplasty stress pre-operative neurovascular documentation, vascular assessment in PVD, and prompt escalation of suspected ischaemia; align with general vascular-emergency standards
- Evidence Level / Status
- Professional consensus
- Relevant Position / Guidance
- Educational principles emphasise protecting the popliteal vessels (retractor medial to PCL, avoid hyperextension) and the peroneal nerve during lateral release, mirroring the Ninomiya anatomical findings
- Evidence Level / Status
- Expert/educational consensus
- Relevant Position / Guidance
- Promotes registry-based outcome monitoring and risk-factor awareness (valgus deformity, flexion contracture, RA, PVD); supports tourniquet stewardship
- Evidence Level / Status
- Consensus/registry-informed
- Relevant Position / Guidance
- Acute limb ischaemia pathways apply directly: urgent revascularisation within the ischaemic window, heparinisation, and consideration of endovascular first-line at experienced centres
- Evidence Level / Status
- Guideline
Registry Evidence
- What it captures
- Implant survival, revision rates, indications - not specific neurovascular complications
- Relevance to this topic
- Confirms procedural volume and revision burden (a higher-risk group for nerve injury); complication-specific data require linked datasets
- What it captures
- Outcomes and revision; complication coding limited
- Relevance to this topic
- Large denominators contextualise rarity of vascular injury; mortality and revision tracked
- What it captures
- Long-running outcome and revision data
- Relevance to this topic
- Benchmark for outcomes; reinforces that neurovascular injury is rare relative to aseptic loosening/infection
- What it captures
- Prospectively collected systemic and local complications
- Relevance to this topic
- The primary source of the verified incidence figures used throughout this topic
- Neurovascular complication rates remain consistent across international registries and institutional series; high-volume centres with fellowship-trained surgeons report lower overall complication rates.
MCQ Practice Points
High-Yield MCQ and Exam Points
Q: A patient develops foot drop after TKA. Which muscle action is the most sensitive bedside test of common peroneal nerve function? A: Ankle dorsiflexion (tibialis anterior). Loss of dorsiflexion is the hallmark; eversion (peroneus longus/brevis) and great-toe extension are also affected.
Q: Where is the popliteal artery in relation to the joint line during TKA, and where should a posterior retractor sit? A: It is a lateral structure at the joint line (Ninomiya); the retractor should be placed medial to the tibial plateau midline, and inserted no more than 1cm, avoiding placement lateral to the PCL.
Q: When should nerve conduction studies/EMG be performed after a post-TKA peroneal palsy? A: At 3-4 weeks for a baseline (Wallerian degeneration is not detectable acutely), repeated at ~3 months for prognosis. Ordering EMG on day 1 is a classic wrong answer.
Q: What is the single most important prognostic factor for recovery of a post-TKA peroneal palsy? A: Whether the palsy is incomplete (partial) versus complete at onset - partial palsies are far more likely to recover fully (Asp/Rand).
Discriminating facts examiners test:
- The popliteal artery is a lateral structure at the joint line; a posterior retractor placed lateral to the PCL or inserted more than 1cm endangers it (Ninomiya). Place retractors medial to the tibial plateau midline.
- Hyperextension tents and kinks the popliteal artery - dangerous during patellar preparation, especially in atherosclerotic vessels.
- Recovery is best when the palsy is incomplete (partial) at onset and when there is delayed onset attributable to dressings (Asp/Rand; Idusuyi/Morrey).
- Tourniquet time over 120 minutes carries a 7.7% neurological complication rate (Horlocker); flexion contracture over 20 degrees gives OR 3.9.
- Operative decompression after failed non-operative treatment improved 97% of patients versus 33% (Mont).
- Indirect (traction/thrombotic) injury is the commonest vascular mechanism in TKA, in contrast to direct injury in THA (Parvizi/Pulido).
At a Glance
At a Glance: Quick Decision Summary
- Rapid Answer
- Common peroneal nerve (superficial at fibular neck)
- Rapid Answer
- Foot drop - check ankle dorsiflexion before discharge
- Rapid Answer
- Fixed valgus + flexion contracture (lateral release lengthens nerve)
- Rapid Answer
- Remove all dressings, flex knee 30-45 degrees, exclude emergencies
- Rapid Answer
- 3-4 weeks (Wallerian degeneration not detectable acutely)
- Rapid Answer
- Most recover; complete recovery in roughly half to two-thirds, over 12-24 months
- Rapid Answer
- 0.03-0.17% of TKA - rare but limb- and life-threatening
- Rapid Answer
- Approximately 6 hours of warm ischaemia - do NOT wait for imaging if clear
- Rapid Answer
- Immediate vascular surgery referral; CTA if stable, theatre if unstable
VASCULAR
Hook:The word VASCULAR itself flags that these are the at-risk knees
PPPPPP6 Ps
Hook:The same six Ps used in compartment syndrome and acute arterial occlusion teaching
DROPDROP-FOOT
Hook:A foot DROP that you treat by acting on every letter of FOOT
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You are asked to see a 68-year-old woman on the ward day 1 after a left TKA for severe valgus osteoarthritis. The nurses are concerned because she cannot lift her left foot off the bed. How do you approach this patient?”
“Two hours after a primary TKA, the recovery nurse reports the foot is cold, mottled and the patient has severe calf pain. The dorsalis pedis and posterior tibial pulses are absent. Walk me through your management.”
“A patient has a complete peroneal nerve palsy after TKA for valgus deformity. There is no clinical or electrical recovery at 4 months. The patient asks what can be done. How do you counsel and manage them?”
Incidence
- Peroneal nerve palsy: 0.3-1.3% primary TKA
- Valgus greater than 15°: 6-9.5% peroneal palsy rate
- Vascular injury: 0.03-0.17%
- Amputation rate with delayed vascular recognition: 10-42%
Risk Factors (VASCULAR mnemonic)
- Valgus greater than 10-15° correction
- Atherosclerosis / PVD
- Stiff knee / flexion contracture greater than 20°
- Calcified vessels
- Underlying RA
- Limb lengthening (excessive correction)
- Anatomical variants / previous surgery
- Revision surgery
Anatomy
- Peroneal nerve wraps around fibular neck - only 2-3mm protection
- Popliteal artery 5-10mm from posterior tibial cortex
- Nerve fixed at sciatic notch and fibular tunnel - limited excursion
- Vulnerable to traction with valgus correction
Clinical Features
- Foot drop = ankle dorsiflexion weakness (L4-5)
- Cannot extend toes or evert ankle
- Sensory loss: dorsum of foot, first web space
- Vascular: 6 Ps - Pain, Pallor, Pulseless, Paresthesia, Paralysis, Poikilothermia
Prevention
- Retractor on tibia not fibular head
- Limit valgus correction to 10-15° single stage
- Flexed knee during posterior work
- Loose dressings, slight knee flexion post-op
- Tourniquet: wider cuff, lower pressure, limited duration
Management - Nerve
- Immediate: loosen dressings, flex knee 30-45°
- AFO for ambulation
- EMG at 3-4 weeks baseline
- 50-90% complete recovery over 12-24 months
- Posterior tibial tendon transfer if no recovery at 12 months
Management - Vascular Emergency
- Immediate vascular surgery consultation
- Heparinize if not contraindicated
- CTA if stable, direct to OR if unstable
- Irreversible ischemia at 6 hours - do NOT delay
- Fasciotomies for compartment syndrome - all 4 compartments
Viva Answers
- Systematic exam: motor, sensory, vascular, compartments
- Exclude emergencies: compartment syndrome, vascular injury, epidural pathology
- Immediate: loosen dressings, flex knee, document, counsel
- EMG too early acutely - need 3-4 weeks for Wallerian degeneration
- Prognosis: 70-90% recover, 12-24 months timeline
Evidence Base
Landmark Evidence
The following evidence is drawn from PubMed-indexed primary literature. Each card has been verified against its PubMed record.
Nerve Injury After Primary TKA - Incidence and Recovery (Columbia Series)
- 19 neurological complications among 1,476 primary TKAs (1970-1998) - overall incidence 1.3%
- A larger-than-expected proportion of rheumatoid knees sustained neurological injury
- In this series valgus deformity, flexion contracture, epidural analgesia and prolonged tourniquet were not statistically associated with palsy - illustrating genuine controversy over risk factors
- All patients showed at least partial recovery with conservative treatment, most recovering completely
Peroneal Nerve Palsy After TKA - Predisposing and Prognostic Factors (Mayo Clinic)
- 32 peroneal palsies among 10,361 TKAs (1979-1992)
- Preoperative valgus deformity (p less than 0.0001), epidural analgesia for postoperative pain (p less than 0.03) and previous lumbar laminectomy (p less than 0.04) were significantly associated with palsy
- High frequency of DELAYED presentation - postulated to relate to impaired proprioception/sensation under epidural analgesia and unprotected limb positioning
- Double-crush phenomenon proposed for patients with prior laminectomy or asymptomatic neuropathy
Peroneal Palsy After TKA - Prognosis for Recovery (Mayo Clinic)
- 26 peroneal palsies after 8,998 TKAs (1972-1985); 18 complete and 8 incomplete
- At mean 5.1 years, recovery was complete in 13 and partial in 12 (only one had no recovery)
- Complete recovery was significantly more likely when the initial palsy was incomplete (partial)
- Patients with partial palsy and with complete recovery had significantly higher knee scores - severity at onset is the key prognostic factor
Popliteal Artery Location and Risk During TKA (Cadaveric + MRI Anatomy)
- Intra-operative arteriograms and 50 transverse MRI scans defined the popliteal artery as a LATERAL structure at the joint line
- A posterior retractor placed the artery at risk when positioned lateral to the PCL or inserted more than 1cm into soft tissue
- Hyperextension produced dramatic tenting/kinking of the artery; both hyperflexion and hyperextension are dangerous, especially in atherosclerotic vessels
- Recommendation: place posterior retractors MEDIAL to the tibial plateau midline and avoid extremes of flexion/extension
Tourniquet Time and Neurological Complications After TKA
- 1,166 knee replacements with tourniquet time over 120 min; 129 nerve palsies in 90 patients (overall 7.7%)
- Risk rose with longer tourniquet time (OR 2.8 per 30-min increase) and preoperative flexion contracture over 20 degrees (OR 3.9); younger age also associated
- Complete recovery in 76/85 (89%) peroneal and 44/44 (100%) tibial palsies
- A reperfusion (deflation) interval only modestly reduced risk - total tourniquet time is the dominant driver
Operative Decompression for Peroneal Nerve Palsy
- 31 patients undergoing decompression after at least 2 months of non-operative management
- Epineurial fibrosis and fibrous bands constricting the nerve at the fibular head and proximal peroneus longus origin were found intra-operatively
- 30/31 (97%) improved and discontinued the AFO versus only 3/9 (33%) managed non-operatively (p less than 0.01)
- Supports operative decompression when non-operative measures fail to improve within ~2 months
References
References
According to PubMed, the following references were verified against their PubMed records (PMID and DOI shown where available).
-
Schinsky MF, Macaulay W, Parks ML, Kiernan H, Nercessian OA. Nerve injury after primary total knee arthroplasty. J Arthroplasty. 2001;16(8):1048-1054. PMID: 11740762. DOI
-
Idusuyi OB, Morrey BF. Peroneal nerve palsy after total knee arthroplasty. Assessment of predisposing and prognostic factors. J Bone Joint Surg Am. 1996;78(2):177-184. PMID: 8609107. DOI
-
Nercessian OA, Ugwonali OF, Park S. Peroneal nerve palsy after total knee arthroplasty. J Arthroplasty. 2005;20(8):1068-1073. PMID: 16376265. DOI
-
Calligaro KD, Dougherty MJ, Ryan S, Booth RE. Acute arterial complications associated with total hip and knee arthroplasty. J Vasc Surg. 2003;38(6):1170-1177. PMID: 14681604. DOI
-
Rand JA. Vascular complications of total knee arthroplasty. Report of three cases. J Arthroplasty. 1987;2(2):89-93. PMID: 3612144. DOI
-
Ninomiya JT, Dean JC, Goldberg VM. Injury to the popliteal artery and its anatomic location in total knee arthroplasty. J Arthroplasty. 1999;14(7):803-809. PMID: 10537254. DOI
-
Asp JP, Rand JA. Peroneal nerve palsy after total knee arthroplasty. Clin Orthop Relat Res. 1990;(261):233-237. PMID: 2245551.
-
Rose HA, Hood RW, Otis JC, Ranawat CS, Insall JN. Peroneal nerve palsy following total knee arthroplasty. A review of The Hospital for Special Surgery experience. J Bone Joint Surg Am. 1982;64(3):347-351. PMID: 7061551.
-
Horlocker TT, Hebl JR, Gali B, Jankowski CJ, Burkle CM, Berry DJ, et al. Anesthetic, patient, and surgical risk factors for neurologic complications after prolonged total tourniquet time during total knee arthroplasty. Anesth Analg. 2006;102(3):950-955. PMID: 16492857. DOI
-
Mont MA, Dellon AL, Chen F, Hungerford MW, Krackow KA, Hungerford DS. The operative treatment of peroneal nerve palsy. J Bone Joint Surg Am. 1996;78(6):863-869. PMID: 8666604.
-
Parvizi J, Pulido L, Slenker N, Macgibeny M, Purtill JJ, Rothman RH. Vascular injuries after total joint arthroplasty. J Arthroplasty. 2008;23(8):1115-1121. PMID: 18676115. DOI
-
Pulido L, Parvizi J, Macgibeny M, Sharkey PF, Purtill JJ, Rothman RH, Hozack WJ. In hospital complications after total joint arthroplasty. J Arthroplasty. 2008;23(6 Suppl 1):139-145. PMID: 18722311. DOI
-
Troutman DA, Dougherty MJ, Spivack AI, Calligaro KD. Updated strategies to treat acute arterial complications associated with total knee and hip arthroplasty. J Vasc Surg. 2013;58(4):1037-1042. PMID: 23747133. DOI
Note on sources: a previously cited reference (attributed to Abularrage et al., "Arterial injury during primary total joint arthroplasty: a 13-year review", J Vasc Surg 2013) could not be located in PubMed during verification and has been removed; the same epidemiological points are covered by the verified Calligaro/Troutman series above.