Fracture | Instability | Clunk Syndrome | Aseptic Loosening
- Patellar complications are the most common cause of TKA reoperation (historically up to 50%)
- Extensor mechanism integrity is the key determinant of management for fractures
- Patellar clunk syndrome presents as a painful 'clunk' at 30-45 degrees of flexion (extension from flexion)
- Malrotation of femoral/tibial components is a major cause of patellar instability
- Avascular necrosis risk is increased by lateral retinacular release (sacrifices superior lateral genicular artery)
- “Look for component malrotation on axial CT (Berger Protocol)
- “Patellar clunk is treated with arthroscopic debridement of the fibrous nodule
- “Goldberg classification drives treatment: Is the extensor mechanism working? Is the implant loose?
- “Avoid ORIF for patellar fractures in TKA if possible - high non-union rate (poor bone stock)
Must assess active straight leg raise. Inability implies Type III/IV fracture or tendon rupture requiring surgery.
Internal rotation of femoral or tibial component is a classic cause of instability and anterior knee pain.
Superior Lateral Genicular Artery. At risk during lateral release. Damage leads to patellar AVN and fracture.
Fibrous nodule at superior pole. Clunks at 30-45° flexion. Differentiate from crepitus or instability.
- Diagnosis
- Patellar Clunk Syndrome
- Treatment
- Arthroscopic Debridement
- Key Pearl
- Resect fibrous nodule
- Diagnosis
- Goldberg Type I
- Treatment
- Non-operative (Brace)
- Key Pearl
- Watch for displacement
- Diagnosis
- Goldberg Type II
- Treatment
- Revision Arthroplasty
- Key Pearl
- Remove loose button/cement
- Diagnosis
- Goldberg Type III
- Treatment
- Surgical Repair/ORIF
- Key Pearl
- High failure rate
- Diagnosis
- Patellar Instability
- Treatment
- Revision of Malrotated Component
- Key Pearl
- Soft tissue release fails if malrotated
MALROTATIONCauses of Patellar Instability
Hook:MALROTATION involves Malposition, Alignment, Lateralization - Remember internal rotation is the enemy!
SAVERisks of Lateral Release
Hook:SAVE the Superior Lateral Genicular Artery to prevent AVN and fracture!
Overview and Epidemiology
Historically, patellar complications were responsible for up to 50% of TKA failures. Modern implant designs (smoother trochlea, better instrumentation) have significantly reduced this, but it remains a leading cause of reoperation.
- Vascular: Lateral release (AVN)
- Technical: Over-resection (less than 12mm), excessive thermal necrosis
- Patient: Osteoporosis, high activity, male gender
- Component: Internal rotation (Femur/Tibia), Medialization of femoral component
- Soft Tissue: Tight lateral retinaculum, loose MCL (valgus)
Anatomy and Biomechanics
The patella is supplied primarily by the genicular anastomosis. The Superior Lateral Genicular Artery and Inferior Lateral Genicular Artery are most critical. A wide lateral retinacular release sacrifices the Superior Lateral Genicular Artery, significantly increasing the risk of patellar AVN and subsequent fragmentation/fracture.
- Effect on Patella
- Increases Q-angle
- Surgical Pearl
- Avoid internal rotation! Use Whiteside's line/TEA
- Effect on Patella
- Lateralizes Tubercle
- Surgical Pearl
- Align to medial 1/3 tibial tubercle
- Effect on Patella
- Increases Q-angle
- Surgical Pearl
- Lateralize femoral component to improve tracking
- Effect on Patella
- Increases shear force
- Surgical Pearl
- Measure pre-op thickness and reproduce it
Overstuffing and Patellar Composite Thickness
Overstuffing appears in the instability mnemonic and the biomechanics table ("measure pre-op thickness and reproduce it"), so it is worth defining the patellofemoral overstuffing mechanism it refers to.
- The patellar composite. After resurfacing, the patellar composite = residual patellar bone + the button; the aim is to reproduce the native patellar thickness (measured with a caliper before cutting). Native adult patellar thickness is roughly 22-25 mm, and about 12-15 mm of residual bone should be preserved to avoid fracture and osteonecrosis.
- Over-resection (residual bone under about 12 mm) weakens the patella and predisposes to fracture and AVN — compounded if the superior lateral genicular supply is also lost.
- Overstuffing (a composite thicker than native, or an oversized/proud anterior femoral flange) increases patellofemoral contact pressure and the extensor lever-arm demand, causing reduced flexion, anterior knee pain and higher shear that in turn drives maltracking, instability and component wear.
- Practical rule. Measure the patella before resection and resurface to reproduce native thickness; avoid an oversized or anteriorly-translated femoral component. Both errors are patellofemoral: too thin risks the bone, too thick risks the joint.
Q: Why does patellar resurfacing aim to reproduce the native composite thickness? A: The composite (residual bone + button) should match the pre-resection thickness. Over-resection (residual bone under ~12 mm) predisposes to fracture/AVN; overstuffing (too-thick composite or a proud anterior femoral flange) raises patellofemoral pressure and causes reduced flexion, anterior knee pain and maltracking. Measure before you cut.
Classification Systems
Goldberg Classification
The standard classification for periprosthetic patellar fractures. The grid below is the treatment-oriented framework (extensor-mechanism integrity by implant stability) commonly used in exams; the original Goldberg (1988) paper actually classified fractures by location and involvement (Types I, II, IIIA, IIIB and lateral fracture-dislocation), but both converge on the principle that an intact mechanism with a stable implant does best.
- Mechanism Intact?
- YES
- Implant Stable?
- YES
- Treatment
- Non-operative (Imm. Range of Motion)
- Mechanism Intact?
- YES
- Implant Stable?
- NO
- Treatment
- Revision (Excise loose button/cement)
- Mechanism Intact?
- NO (Disrupted)
- Implant Stable?
- YES
- Treatment
- Surgery (Repair/ORIF + liner exchange)
- Mechanism Intact?
- NO (Disrupted)
- Implant Stable?
- NO
- Treatment
- Surgery (Resection/Patellectomy/Allograft)
For Type II (Loose implant, Intact mechanism), if the bone stock is poor, it is often better to remove the loose button and leave the patella unresurfaced (patelloplasty) rather than attempting to recement a new button onto a shell of bone.
MILSGoldberg Classification (Fractures)
Hook:MILS helps decide if surgery is needed - Mechanism and Implant stability are key.
Patellar Crepitus vs Clunk: The Fibrosynovial Spectrum
The exam warning tells you to differentiate patellar clunk from crepitus — the two sit on one spectrum of peripatellar fibrosynovial hyperplasia in posterior-stabilised (PS) knees, and the distinction matters for treatment.
- Same origin, different severity. Both arise from fibrous/synovial tissue at the quadriceps-patella junction interacting with the intercondylar box of a PS femoral component. Crepitus is a palpable or audible grating through the mid-flexion arc from softer peripatellar fibrosynovial hyperplasia; clunk is a discrete, often painful catch as a mature fibrous nodule snaps out of the box during terminal extension (around 30-45 degrees).
- Shared risk factors. PS designs, smaller/thinner patellar components, patella infera, a less accommodating trochlear box, and certain implant designs; the anterosuperior patella-quadriceps junction is the culprit zone.
- Treatment ladder. Crepitus is usually milder and often settles with observation and physiotherapy; clunk (a mechanical block) typically needs arthroscopic debridement of the nodule (the gold standard), which is also effective for refractory crepitus.
- The viva discriminator. Both preserve range of motion (unlike arthrofibrosis, which is stiffness). Crepitus = grating, often incidental; clunk = a painful, reproducible catch on extension. Naming both shows you understand the spectrum.
Q: How do patellar crepitus and patellar clunk differ, and how are they treated? A: Both come from peripatellar fibrosynovial tissue engaging the box of a PS femoral component. Crepitus is milder grating through mid-flexion (often observation/physio); clunk is a discrete painful catch from a mature nodule in terminal extension, treated by arthroscopic debridement. Both keep good ROM — that separates them from arthrofibrosis.
Clinical Assessment
- Instability: "Knee gives way", "Patella jumps out"
- Clunk: Painful catch/clunk at 30-45 degrees flexion
- Fracture: Acute pain, inability to straight leg raise
- Pain: Anterior knee pain, worse with stairs/rising
- Observation: Q-angle, Valgus alignment
- Palpation: Fibrous nodule (Clunk), Tenderness
- Dynamic: Patellar tracking (J-sign), Active SLR (Mechanism integrity)
- Implant: Assess for gross loosening/instability
In any painful TKA, infection must be ruled out first. Aseptic loosening and patellar complications can mimic infection. Obtain ESR/CRP and aspirate if elevated.
Investigations
Imaging Protocol
- AP/Lateral: Fracture, implant position, bone stock
- Skyline (Merchant): Critical for assessment of patellar tilt, subluxation, and fracture profile
- Indication: Instability or Anterior Knee Pain
- Assess: Rotational alignment of femoral and tibial components
- Femur: PCA (Posterior Condylar Axis) vs TEA (Transepicondylar Axis)
- Tibia: Geometric center vs Tubercle
- Indication: Pain with normal X-rays/CT
- Finding: Increased uptake ('hot') patella may suggest stress fracture or loosening
The Berger Protocol typically combines femoral and tibial rotation.
- Internal Rotation of Femoral Comp + Internal Rotation of Tibial Comp = Severe Patellar Instability. Even minor internal rotation of both can summate to cause significant tracking issues.


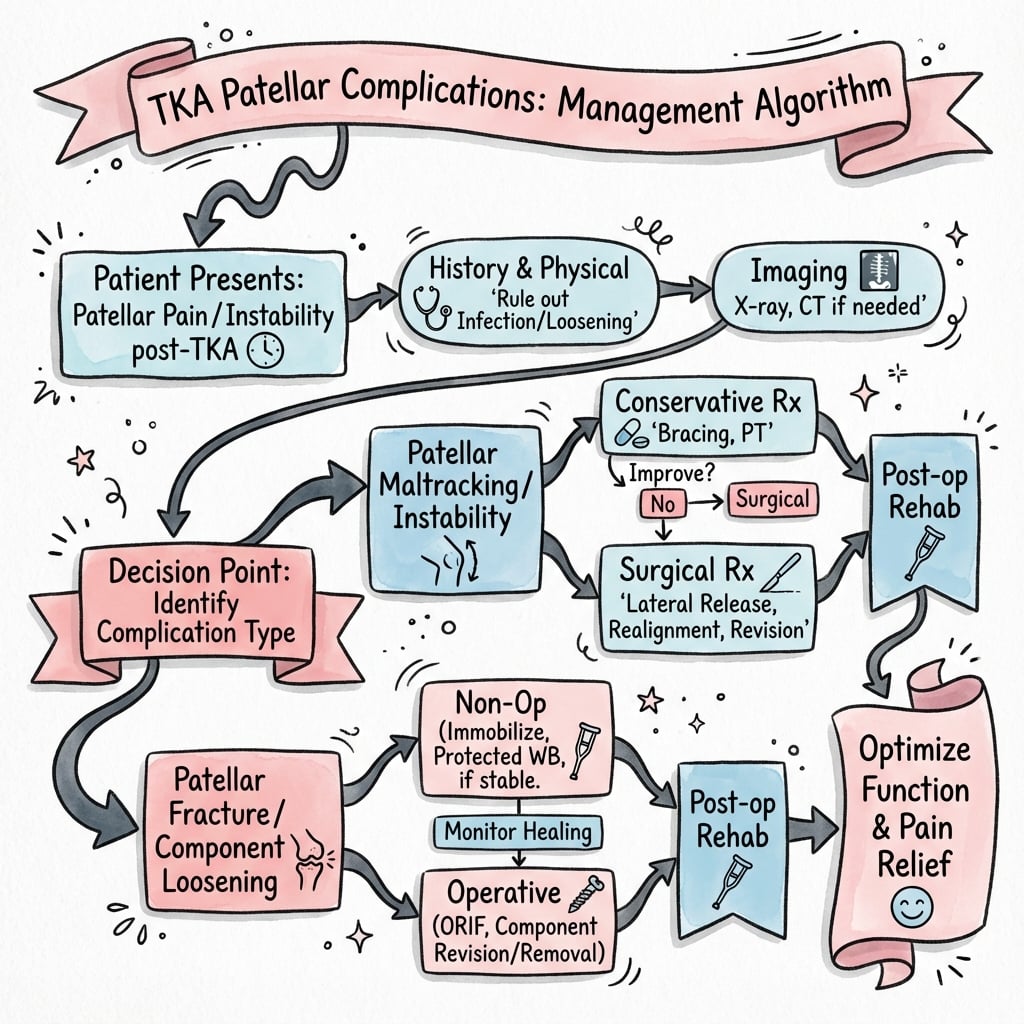
Management Algorithm
Management of Patellar Fracture
Based on Goldberg Classification.
Principles:
- Preserve extensor mechanism (Priority #1)
- Preserve bone stock
- Avoid surgery if mechanism is intact (Type I)
Treatment Steps
- Cylinder cast/brace in extension for comfort
- Allow weight bearing as tolerated
- Start immediate ROM (if stable) to prevent stiffness
- Extensor mechanism is intact but button is loose.
- Surgery: Remove loose button.
- Decision: Recement (if good bone greater than 12mm) vs Resection Arthroplasty (Patelloplasty).
- Extensor disrupted, Button stable.
- Surgery: Repair extensor mechanism + ORIF (Tension band).
- Outcome: Poor. High failure rate. Consider allograft if repair poor.
- Disrupted + Loose.
- Surgery: Remove button + Reconstruct mechanism (Allograft/Mesh).
- Typically requires removal of loose bodies and major reconstruction.
Management decisions depend on patient factors and fracture stability.

Surgical Technique
Revision for Patellar Instability (Malrotation)
Surgical Steps
- Medial parapatellar approach (standard).
- Extensive synovectomy.
- Inspect patellar tracking before dislocating/everting.
- Use epicondylar axis (TEA) and Whiteside's line.
- Confirm internal rotation of femoral component.
- Remove femoral component carefully (preserve bone).
- Osteotomes/Gigli saw if cemented.
- External Rotation: Set femoral component in 3 degrees external rotation relative to posterior condyles (or parallel to TEA).
- Lateralization: Use an offset stem or shift component laterally to improve tracking.
- "No Thumbs" test: Patella should track centrally without thumb pressure throughout ROM.
Complications
- Risk
- High in Type III/IV
- Management
- Allograft/Mesh Reconstruction
- Prevention
- Avoid aggressive ROM
- Risk
- Lateral Release
- Management
- Observation over Patellectomy
- Prevention
- Preserve Sup Lat Genicular Artery
- Risk
- Common (Poor bone)
- Management
- Accept if painless/stable
- Prevention
- Optimized fixation
- Risk
- Malrotation not addressed
- Management
- Revision TKA
- Prevention
- Correct component rotation
Postoperative Care
Rehabilitation Protocol
- Fracture/Repair: Hinged knee brace locked in extension.
- Weight Bearing: WBAT with brace locked in extension.
- Revision TKA: Often WBAT, start ROM immediately if stable.
- Fracture: Start passive ROM limited to 0-30 degrees (if repair strong).
- Clunk Resection: Immediate full ROM allowed.
- X-rays: Check at 2 weeks and 6 weeks for alignment/displacement.
- Unlock brace for walking (if SLR control good).
- Progressive flexion as tolerated.
- Strengthening (quadriceps) starts late (3 months) for fractures.
- Full functional activity.
- Monitor for late loosening or recurrence of instability.
Strict adherence to range of motion limits is required for extensor repairs.
Outcomes and Prognosis
- High Complication Rate: Surgical repair fails in 20-30% of cases.
- Non-union: Common (30-50%) but often painless if Type I.
- Best Outcome: Type I treated non-operatively (96% success).
- Excellent: Arthroscopic debridement has greater than 95% success rate.
- Recurrence: Rare if sufficient nodule resected.
- Revision: Success depends on identifying cause.
- Malrotation: Revising components has 80-90% success.
- Soft Tissue Only: Lateral release alone has high failure if malrotation missed.
- Poor Prognosis: Primary repair has high failure rate.
- Reconstruction: Allograft/Mesh often required.
- Salvage: Arthrodesis may be end stage.

Guidelines, Registries & Global Practice
Periprosthetic patellar fracture is uncommon (around 0.7% of TKAs; Ortiguera & Berry), but patellofemoral problems collectively remain a leading reason for reoperation. Risk rises with resurfacing, lateral release, over-resection (composite under 12 mm), and component malrotation. Reported rates vary widely with implant design and whether the patella was resurfaced.
- Patellar Resurfacing
- Selective or routine (surgeon-dependent)
- Key Recommendation
- No single mandate; tailor to design, anatomy, anterior knee pain risk
- Patellar Resurfacing
- Either acceptable
- Key Recommendation
- Decision should be informed and design-specific; rule out infection before revision
- Patellar Resurfacing
- N/A (fracture focus)
- Key Recommendation
- Manage periprosthetic patellar fracture by extensor integrity + implant fixation
- Patellar Resurfacing
- Selective
- Key Recommendation
- Optimise component rotation; avoid routine lateral release
- Patellar Resurfacing
- Lower reoperation when resurfaced
- Key Recommendation
- Resurfacing associated with reduced secondary patellar surgery
- Joint registries (NJR UK, AJRR US, AOANJRR Australia, NZJR) consistently show lower rates of secondary patellar surgery when the patella is resurfaced.
- Level I meta-analysis (Chen 2021) concurs: reduced reoperation and noise, no difference in anterior knee pain.
- Rule out PJI first: aspiration plus ESR/CRP before any revision for "pain" or "instability" - a universal standard.
- High-resource: extensor allograft and synthetic mesh available; rotational CT readily obtained.
- Limited-resource: allograft scarce, so autograft/mesh and tertiary referral are emphasised; reliance on skyline radiographs where CT access is limited.
MCQ Practice Points
Q: Which arterial structure is most at risk during a lateral retinacular release in TKA? A: Superior Lateral Genicular Artery (SLGA) - The SLGA runs in the lateral retinaculum. A wide lateral release can transect this vessel, compromising patellar blood supply and increasing the risk of avascular necrosis and fracture.
Q: A patient with a well-fixed TKA sustains a patellar fracture after a fall. She is able to perform a straight leg raise. The implant appears stable on X-ray. What is the Goldberg classification and appropriate management? A: Type I - Non-operative - This is a Goldberg Type I fracture (Intact extensor mechanism + Stable implant). The active straight leg raise confirms mechanism integrity. Treatment is non-operative (immobilizer/brace) as surgical intervention has a high complication rate.
Q: What is the most likely cause of late-presenting patellar instability after TKA? A: Component Malrotation - While all can cause issues, component malrotation (especially internal rotation of the femoral or tibial component) is a leading cause of mechanical patellar instability. Polyethylene wear can cause late instability but malrotation is the primary mechanical driver.
Q: Why is primary repair of a chronic patellar tendon rupture in TKA contraindicated? A: High Failure Rate - Primary repair of chronic disruptions (especially in revision scenarios) has an excessively high failure rate. Management requires reconstruction using either an extensor mechanism allograft or synthetic mesh (e.g., Marlex), rather than simple suture repair.
Q: How does excessive joint line elevation affect the patella? A: Pseudo-Patella Baja - elevating the joint line (e.g., with thick poly or distal femoral augments) causes "pseudo-patella baja". The patella tendon length is normal, but the patella impinges on the tibial post or poly during flexion, reducing ROM and causing anterior pain.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old female, 1 year post-op PS-TKA. Doing well but complains of a painful 'catch' or 'clunk' when she stands up from a chair. No pain at rest. ROM 0-120.”
“A 75-year-old male, 5 years post-TK. Falls onto knee. Pain, swelling. X-ray shows a transverse fracture of the patella. The button appears well-fixed.”
“A patient presents with anterior knee pain and feelings of instability 2 years post-TKA. She feels the kneecap 'jumps'. On exam, she has a positive J-sign and lateral apprehension.”
Key Classifications
- Goldberg I: Intact mech, Stable implant → Non-op
- Goldberg II: Intact mech, Loose implant → Revision/Patelloplasty
- Goldberg III: Disrupted mech, Stable implant → Repair + Fixation
- Goldberg IV: Disrupted mech, Loose implant → Salvage/Reconstruct
Patellar Clunk
- Fibrous nodule at superior pole
- Catches in intercondylar box (PS knees)
- Clunk at 30-45° extension
- Rx: Arthroscopic debridement
Instability Causes
- Internal Rotation of Femoral Comp
- Internal Rotation of Tibial Comp
- Valgus alignment
- Tight lateral retinaculum
- Medialized femoral component
Management Pearls
- Avoid surgery for Type I fractures (high complication rate)
- CT scan critical for instability (assess rotation)
- Lateral release endangers Superior Lateral Genicular Artery
- Berger Protocol: Combined internal rotation predicts instability
Blood Supply
- Genicular anastomosis
- Superior Lateral Genicular Artery (Most important)
- Inferior Lateral Genicular Artery
- Avoid deep lateral dissection
Evidence
- Ortiguera & Berry: nonop for intact mechanism/stable implant; surgery has high complications
- Berger: combined internal rotation predicts patellar complication severity (CT)
- Hozack: defined patellar clunk syndrome (PS designs)
- Chen 2021 / registries: resurfacing lowers reoperation rate
- Scott: lateral release compromises SLGA, risks AVN/stress fracture
Evidence Base
Goldberg Classification of Periprosthetic Patellar Fracture
- The original 1988 paper analysed 36 patellar fractures in 35 condylar TKAs (mean 4.5-year follow-up)
- Classified by fracture location and involvement of the extensor mechanism and implant/cement composite (Types I, II, IIIA, IIIB and lateral fracture-dislocation)
- Fractures sparing the implant/cement and quadriceps (Type I) and nondisplaced inferior-pole fractures (Type IIIB) did well non-operatively; operatively treated disrupted/dislocated types had more failures
- This underpins the widely-taught treatment framework used here: intact mechanism plus stable implant has the best prognosis; disrupted-mechanism or loose-implant fractures the worst
The Patellar Clunk Syndrome
- Original description in three patients after posterior-stabilised TKA
- Painful 'catch' or 'clunk' on knee extension
- Prominent fibrous nodule at junction of proximal patellar pole and quadriceps tendon
- Surgical removal of the nodule resolved symptoms
Periprosthetic Patellar Fracture: Classification & Outcomes
- 85 fractures (77 patients) after 12,464 TKAs - overall prevalence 0.68%
- Significantly more common in men (1.01%) than women (0.40%)
- Type I (intact mechanism + stable implant, n=38): nonoperative treatment with only one late failure
- Operative treatment (disrupted mechanism or loose component) had high complication and reoperation rates
Malrotation Causing Patellofemoral Complications
- 30 patients with patellofemoral complications vs 20 well-functioning controls
- Complication group had excessive combined (femoral + tibial) internal rotation; controls were in external rotation
- Combined internal rotation 1-4 deg: lateral tracking/tilt; 3-8 deg: subluxation; 7-17 deg: dislocation or late prosthesis failure
- Transepicondylar axis and tibial tubercle are reproducible CT landmarks
Lateral Release, Patellar AVN & Stress Fracture
- Patellar stress fracture incidence 0.7% in rheumatoid vs 3.5% in osteoarthritic knees
- Osteonecrosis occurred in at least three cases where lateral release had sacrificed the superior lateral genicular artery
- Vessel should be preserved to protect patellar and lateral skin flap blood supply
- Preserving peripheral cortex and bone stock reduces fracture risk
Patellar Resurfacing vs Non-resurfacing: Meta-analysis
- 32 randomized trials, 6887 knees
- Resurfacing significantly reduced reoperation (overall and at 5+ years) and noise
- Higher Knee Society and function scores with resurfacing
- No significant difference in anterior knee pain, ROM or patient satisfaction