Choose the exposure that reaches the pathology safely
- Do not start an approach description with the incision alone. Start with position, landmarks, interval, structures at risk, exposure target and closure.
- The same skin incision can be safe or dangerous depending on where the deep dissection goes.
- Approach choice follows the target: acetabulum, femur, femoral head, anterior ring, posterior ring or pelvic brim.
- Danger structures should be named before the incision: LFCN, femoral nerve, femoral vessels, obturator bundle, corona mortis, sciatic nerve and superior gluteal bundle.
- Good exposure is not the same as aggressive exposure. The safest approach gives enough access with the least avoidable soft-tissue and neurovascular harm.
- “Direct anterior hip uses the Smith-Petersen interval between sartorius and TFL; the LFCN is vulnerable near the ASIS.
- “Direct lateral and anterolateral hip approaches risk abductor dysfunction and superior gluteal nerve injury if the split is too proximal.
- “Posterior hip and Kocher-Langenbeck approaches require active sciatic nerve awareness and careful posterior repair when used for arthroplasty.
- “Modified Stoppa gives intrapelvic access to the pelvic brim, quadrilateral surface and medial acetabular displacement, but corona mortis and obturator structures must be controlled.
Surgical Approaches to the Hip and Pelvis
The best approach is the one that reaches the operative target safely in that patient. A familiar approach used for the wrong fracture, wrong implant problem or wrong soft-tissue situation becomes a liability.
Overview/Epidemiology
Hip and pelvic approaches are high-stakes because the region combines deep joints, major vessels, large nerves, powerful muscles and complex three-dimensional bony anatomy. The approach is not just a route to bone; it affects reduction quality, implant position, dislocation risk, abductor function, nerve injury, bleeding, infection risk and future revision options.
The common clinical settings are:
- primary and revision total hip arthroplasty
- femoral neck fracture arthroplasty
- acetabular fracture fixation
- pelvic ring fixation
- hip preservation surgery
- infection, tumour or complex reconstruction
- paediatric hip exposure for selected conditions
The same named approach may mean different things in different settings. A Kocher-Langenbeck exposure for the posterior acetabulum is related to posterior hip exposure but is not the same operation as a routine posterior arthroplasty approach. A Smith-Petersen exposure can be used for direct anterior THA, femoral head work and some hip preservation operations, but the deep releases and objectives differ.
Approach selection should start with the pathology: posterior wall, anterior column, quadrilateral surface, unstable pelvic ring, femoral head, acetabulum or femoral stem. Once the target is clear, the approach options become logical.
Anatomy/Biomechanics
The hip and pelvis are approached through a limited number of safe windows. The surgeon must know which structures are being protected and which structures are being deliberately released or repaired.

Hip arthroplasty approach anatomy
- Deep plane
- Sartorius and tensor fascia lata interval
- Key structures
- LFCN, ascending lateral femoral circumflex vessels, femoral nerve and vessels medially
- Practical consequence
- Low posterior instability risk but LFCN symptoms and femoral exposure challenges can occur
- Deep plane
- Watson-Jones interval between TFL and gluteus medius
- Key structures
- Superior gluteal nerve, abductors, femoral nerve medially
- Practical consequence
- Good anterior-lateral access; abductor handling affects gait
- Deep plane
- Split or detach anterior gluteus medius and vastus lateralis sleeve
- Key structures
- Superior gluteal nerve and abductor repair
- Practical consequence
- Stable exposure but Trendelenburg risk if abductor repair fails
- Deep plane
- Gluteus maximus split and short external rotator release
- Key structures
- Sciatic nerve, posterior capsule, short external rotators
- Practical consequence
- Excellent femoral and acetabular exposure; posterior repair improves stability
Acetabular and pelvic anatomy
The acetabulum is a ring-like structure with anterior column, posterior column, anterior wall, posterior wall and quadrilateral surface components. An approach must reach the surface that needs reduction and fixation.
Key danger structures:
- External iliac vessels: anterior approaches and pelvic brim work.
- Femoral nerve: lateral to femoral vessels and vulnerable in anterior windows.
- Corona mortis: vascular connection over the superior pubic ramus; it may bleed severely if missed.
- Obturator nerve and vessels: medial acetabular and quadrilateral surface work.
- Sciatic nerve: posterior acetabular exposure, posterior hip dislocation and posterior column manipulation.
- Superior gluteal bundle: exits above piriformis and can be injured with proximal posterior exposure or excessive abductor split.
Incisions, external-fixator pins and flap choices can make later definitive fixation or soft-tissue cover harder. The first approach should not compromise the reconstructive plan.
Internervous Plane
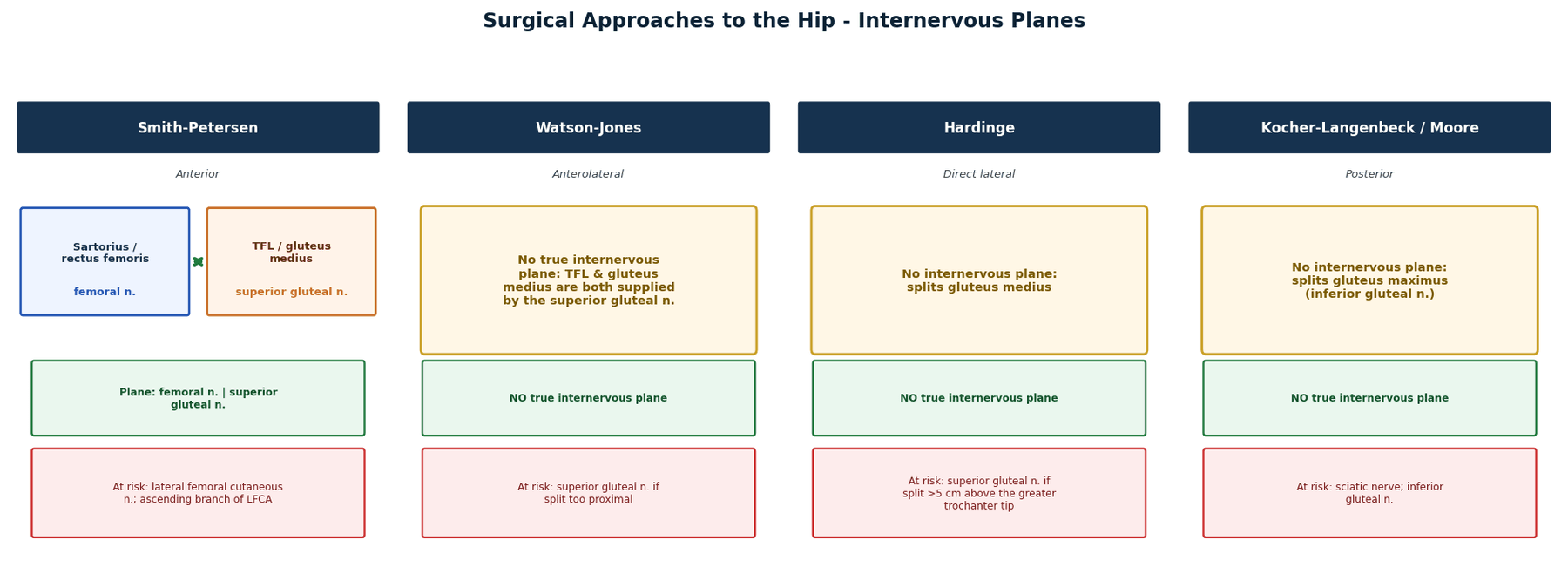
An internervous plane is safe because the muscles on either side are supplied by different nerves. Some hip and pelvic approaches are true internervous planes; others are muscle-splitting or tendon-release approaches that are safe only if the split, release and repair are controlled.
- Plane
- Sartorius/femoral nerve side and TFL/superior gluteal nerve side
- Why it matters
- A true interval, but LFCN and femoral exposure remain important risks
- Plane
- TFL and gluteus medius interval
- Why it matters
- Useful anterolateral access; avoid drifting into abductor injury
- Plane
- Transgluteal split or abductor sleeve
- Why it matters
- Not a pure internervous plane; abductor repair determines function
- Plane
- Gluteus maximus split and short rotator release
- Why it matters
- Muscle split/release approach; sciatic nerve and posterior repair are key
- Plane
- Between gluteus maximus and abductors with short rotator release
- Why it matters
- Posterior acetabular access; sciatic nerve and superior gluteal bundle define the safe limits
- Plane
- Extraperitoneal intrapelvic plane
- Why it matters
- Not an internervous limb plane; safety depends on bladder, corona mortis and obturator bundle protection
NERVEDanger Structures
Hook:Before the incision, name the structures that can change the operation.
Classification Systems
Classifications help define the target; they do not choose the approach alone.

- What it tells you
- Column and wall pattern
- Approach relevance
- Posterior wall and posterior column favour Kocher-Langenbeck; anterior column and quadrilateral displacement favour anterior or intrapelvic exposure
- What it tells you
- Fracture group and complexity
- Approach relevance
- Useful for communication and research; still requires CT-based reduction target planning
- What it tells you
- Mechanism and instability direction
- Approach relevance
- Helps anticipate anterior ring, posterior ring and vascular priorities
- What it tells you
- Rotational and vertical stability
- Approach relevance
- Unstable posterior ring injuries require posterior fixation strategy, not anterior plating alone
- What it tells you
- Revision THA bone defect pattern
- Approach relevance
- May require extensile exposure, augments, cages, cup-cage, custom implant or pelvic discontinuity strategy
Limitations
Classifications describe patterns, not the whole patient. Approach choice can change because of obesity, previous scars, open wounds, vascular injury, infection, surgeon experience, implant inventory, associated fractures and whether a second team is needed.
Clinical Assessment
Clinical assessment for an approach is not a generic history; it is a surgical access assessment.
Patient factors
- Body habitus and soft-tissue depth.
- Prior scars and previous approaches.
- Infection risk and skin quality.
- Vascular disease, anticoagulation and pelvic bleeding risk.
- Neurological baseline, especially sciatic, femoral and obturator function.
- Bone quality and osteoporosis.
- Ability to tolerate lateral, prone or supine positioning.
Injury or disease factors
- Open wound location and contamination.
- Hip dislocation direction and time to reduction.
- Femoral head damage, marginal impaction or intra-articular fragments.
- Acetabular column and wall involvement.
- Pelvic ring stability and haemodynamic state.
- Revision implants, cement, screws, plates, cages or pelvic discontinuity.
Examination points to document
- Distal pulses and limb perfusion.
- Femoral, sciatic, obturator and lateral femoral cutaneous nerve symptoms where relevant.
- Abductor function if planning lateral or revision hip surgery.
- Skin scars and planned incision conflicts.
- Compartment or soft-tissue swelling in trauma.
Investigations
Imaging determines the target and the safe corridor.
Plain radiographs
- AP pelvis for global alignment, hip joint status, pelvic ring asymmetry and implants.
- AP and lateral hip for arthroplasty planning, femoral morphology and component position.
- Judet oblique views for acetabular column and wall assessment when CT is not yet available.
- Inlet and outlet pelvis views for pelvic ring displacement and posterior ring assessment.
CT
CT is central for acetabular and pelvic ring surgery. It shows:
- anterior versus posterior column involvement
- posterior wall fragment size and marginal impaction
- quadrilateral surface displacement
- intra-articular fragments
- sacral fracture morphology
- safe iliosacral and transsacral screw corridors
- existing implant position or bone loss in revision surgery

CT angiography
Use when there is suspected arterial injury, expanding haematoma, pelvic bleeding concern, absent pulses, revision cup migration near vessels, tumour surgery or intrapelvic hardware migration.
MRI
MRI is not routine for fracture approach selection but can help in tumour, infection, osteonecrosis, soft-tissue abscess and hip preservation planning.
Differential of a Postoperative Neurological Deficit
A new deficit after a hip or pelvic approach is a clinical emergency of reasoning, not panic. Localise the lesion, decide if it is compressive and reversible, and act.
- Most likely cause
- Sciatic nerve (peroneal division) traction or compression
- Discriminators
- Knee flexion eases tension; check for haematoma; review intraoperative retraction
- Action
- Flex knee, extend hip, release tension; explore or decompress if compressive cause suspected
- Most likely cause
- Femoral nerve injury or compression
- Discriminators
- Loss of knee extension and patellar reflex; consider retractor on iliopsoas or haematoma
- Action
- Imaging for haematoma, decompress if compressive, document and counsel on recovery
- Most likely cause
- Lateral femoral cutaneous nerve neuropraxia
- Discriminators
- Purely sensory, no motor loss; very common and often self-limiting
- Action
- Reassure, document, expect improvement; persistent dysaesthesia may need referral
- Most likely cause
- Obturator nerve injury
- Discriminators
- Adductor weakness with medial thigh numbness
- Action
- Document, counsel; consider exploration only if a clear intraoperative cause is suspected
- Most likely cause
- Compressive haematoma or vascular injury
- Discriminators
- Tense swelling, falling haemoglobin, absent or changing pulses
- Action
- Urgent imaging or return to theatre, involve vascular surgery, do not wait
When a new deficit appears, exclude a treatable compressive cause - haematoma, tight closure, malpositioned retractor or a too-tight construct - before attributing the deficit to irreversible intraoperative nerve damage.
Management Algorithm
Approach selection is a sequence:
- Define the pathology and reduction target.
- Decide whether the patient needs damage-control, definitive fixation or staged reconstruction.
- Review imaging in axial, coronal, sagittal and three-dimensional terms.
- Identify danger structures and previous surgical planes.
- Choose the least harmful exposure that gives enough access.
- Plan fixation, implant removal, grafting, flap cover and closure before incision.
- Have an extensile or bailout plan.
Approach choice is mainly driven by surgeon experience, patient habitus, dislocation risk, femoral exposure, implant plan and ability to repair soft tissues. Anterior, lateral and posterior approaches can all produce good results when performed well.
When describing an approach, include what you will do if exposure is inadequate: extend the approach, change position, add a second window, use trochanteric osteotomy, call vascular or plastic surgery, or stage the operation.
Patient Positioning
Positioning is part of the approach. It determines access, fluoroscopy, reduction ability, anaesthetic safety and whether a second approach remains possible.
- Typical use
- Direct anterior hip, ilioinguinal, modified Stoppa, anterior pelvic ring, many percutaneous pelvic screws
- Checks before incision
- Image intensifier access, abdominal prep, traction options and vascular access
- Typical use
- Posterior THA, direct lateral THA, selected Kocher-Langenbeck exposure
- Checks before incision
- Pelvis must be stable; check pressure areas, sciatic nerve baseline and leg manipulation access
- Typical use
- Many posterior acetabular and posterior pelvic exposures
- Checks before incision
- Airway, abdomen free, pressure areas, fluoroscopy and ability to manage blood loss
- Typical use
- Combined anterior/posterior acetabular or pelvic reconstruction
- Checks before incision
- Plan draping, antibiotics, imaging, blood loss and sequence before starting
If a case may require vascular control, second approach, traction, external fixation, image intensifier access or conversion to arthroplasty, the starting position must allow that plan or make repositioning safe.
Approach Atlas
Direct anterior uses the anterior internervous plane between sartorius and tensor fascia lata. It is useful for supine arthroplasty and can reduce posterior instability risk, but femoral exposure can be demanding and LFCN symptoms are common.
Anterolateral uses the Watson-Jones interval and provides anterior-lateral hip access. It avoids posterior soft-tissue release but still demands abductor protection.
Direct lateral splits or detaches the anterior abductor sleeve. It is stable and extensile but can cause abductor weakness if the repair fails or the superior gluteal nerve is injured.
Posterior provides excellent femoral and acetabular access. The sciatic nerve, posterior capsule and short external rotators must be respected; posterior repair is part of modern stability strategy.
The ETO is repeatedly referenced above ("with ETO when needed", "trochanteric osteotomy") as the bailout for revision femoral exposure but is never described - and examiners expect you to be able to explain it:
- Indications: removal of a well-fixed cemented or cementless femoral stem, cement/distal cement-plug removal, access to a varus-remodelled or deformed proximal femur, and improved acetabular exposure in difficult revisions.
- Key technical principle - keep the fragment vascularised: the osteotomy is lateral-based, taking roughly the lateral one-third of the femoral circumference, and the bone fragment is kept in continuity with the vastus lateralis distally and the abductors (gluteus medius) proximally - this preserves its blood supply and the abductor lever arm. The length is tailored to the stem/cement to be removed (commonly around 12-14 cm), with the distal corner rounded to reduce stress-riser fracture.
- Repair/fixation: the trochanteric-abductor fragment is reduced and fixed back with cerclage cables/wires (often two or more), restoring abductor tension; union rates are high (typically reported around or above 90%) when the soft-tissue sleeve is preserved.
- Pitfalls: an under-vascularised or over-thin fragment risks non-union/migration; too short an osteotomy fails to relieve the implant; a square distal corner creates a fracture stress riser.
Exam point: the ETO is a lateral-based, vastus-and-abductor-pedicled osteotomy of about one-third the femoral circumference, used to remove well-fixed stems/cement and access femoral deformity, repaired with cables with a high union rate - it is the extensile bailout for the revision femur.
Surgical Technique
The surgical technique section describes approach principles. Individual operations still require detailed procedure-specific planning.
Confirm indication, imaging, side, implants, patient position and bailout plan. Mark ASIS, iliac crest, greater trochanter, femoral shaft, pubic symphysis and sacrum where relevant.
Plan image intensifier access before sterile prep. Prep widely enough for extension, traction, vascular control or a second approach if needed. Check neurovascular baseline before and after positioning.
Complications
- Where it occurs
- Direct anterior hip
- Prevention and recognition
- Respect interval near ASIS; counsel that numbness or dysaesthesia can occur
- Where it occurs
- Anterior hip and anterior acetabular approaches
- Prevention and recognition
- Know medial danger zone, use careful retractors and avoid blind instrumentation
- Where it occurs
- Posterior hip and posterior acetabulum
- Prevention and recognition
- Document baseline, avoid traction, protect during posterior column work
- Where it occurs
- Anterolateral and direct lateral hip
- Prevention and recognition
- Limit proximal split and repair abductors securely
- Where it occurs
- All THA approaches, pattern differs by approach
- Prevention and recognition
- Component position, soft-tissue repair, head size, offset and patient education
- Where it occurs
- Anterior pelvis and modified Stoppa
- Prevention and recognition
- Identify, clip or ligate; do not sweep blindly over superior pubic ramus
- Where it occurs
- Acetabular fracture surgery, extended approaches and head injury patients
- Prevention and recognition
- Minimise soft-tissue trauma and consider prophylaxis according to risk and local protocol
- Where it occurs
- Acetabular and pelvic ring fixation
- Prevention and recognition
- Use CT planning, adequate exposure, reduction aids and intraoperative imaging
The complication table lists heterotopic ossification (HO) but the examinable detail - grading, the approach-dependent risk gradient, and the actual prophylaxis options - is worth holding explicitly:
- Grading (Brooker): I = islands of bone in soft tissue; II = bone spurs from pelvis/proximal femur with at least one cm between opposing surfaces; III = spurs with less than one cm between surfaces; IV = apparent radiographic ankylosis. Higher grades correlate with functional loss.
- Risk is approach-dependent: HO is highest with the extended iliofemoral approach and with extensive abductor/gluteus stripping, intermediate with the Kocher-Langenbeck, and lowest with the ilioinguinal / anterior intrapelvic approaches (which spare the gluteal muscle mass). Head injury, male sex, delayed surgery and muscle debridement add risk.
- Prophylaxis (two equally-recognised options): (1) single-dose radiotherapy (commonly around 700-800 cGy) given within roughly 24-72 hours of surgery; or (2) indomethacin or another NSAID for several weeks postoperatively. Reserve prophylaxis for higher-risk approaches/patients - weigh NSAID effects on fracture/bone healing and the practicalities of perioperative radiotherapy.
Exam point: for acetabular/hip approaches say you would grade HO by Brooker, recognise the extended-iliofemoral/abductor-stripping approaches as highest-risk (intrapelvic lowest), and offer single-dose radiotherapy or an NSAID course as prophylaxis in selected high-risk cases.
Postoperative Care
Postoperative care depends on the operation, but approach-specific points matter.
Hip arthroplasty
- Check sciatic, femoral and peroneal nerve function.
- Check wound, haematoma and infection risk.
- Use approach-specific dislocation precautions where the surgeon considers them appropriate.
- Protect abductor repair after lateral approaches according to local protocol.
- Confirm component position and leg length on postoperative radiographs.
Acetabular and pelvic fixation
- Repeat neurological examination after surgery.
- Monitor haemoglobin, drains, wound swelling and pelvic bleeding risk.
- Use postoperative CT when reduction or screw placement needs confirmation.
- Weight-bearing depends on fracture stability, fixation quality and associated injuries.
- Monitor for DVT, heterotopic ossification, infection, nonunion and post-traumatic arthritis.
Outcomes/Prognosis
Outcomes depend more on pathology, surgical execution and patient factors than the name of the approach alone.
For THA, modern evidence suggests that direct anterior, lateral and posterior approaches can all achieve excellent outcomes when performed by experienced surgeons. Differences tend to involve early recovery patterns, dislocation direction, nerve symptoms, abductor morbidity, fracture risk and learning curve rather than a universal winner.
For acetabular fractures, reduction quality remains a major determinant of outcome. An approach that gives inadequate reduction access is worse than a larger approach chosen deliberately. Posterior wall comminution, marginal impaction, femoral head damage, delayed surgery, nerve injury and imperfect reduction worsen prognosis.
For pelvic ring injuries, outcome is influenced by haemodynamic injury, posterior ring reduction, neurological injury, associated trauma, chronic pain and rehabilitation access.
Guidelines, Registries & Global Practice
Hip and pelvic approach practice is shaped less by formal disease guidelines than by arthroplasty registries, trauma society principles and local resources. The unifying global principle is that the approach should reach the target safely in that patient and that complex acetabular and pelvic injuries belong in teams with the imaging, reduction tools and supporting specialties to manage them.
Global epidemiology
- Total hip arthroplasty is among the most common and most successful elective operations worldwide, with very high implant survival reported across major registries.
- The acetabular fracture population is ageing, with mean age rising from the late 30s toward the mid-40s and a growing proportion of anterior-column patterns and low-energy falls, according to PubMed-indexed contemporary reviews (Kelly et al., Injury 2020).
- Pelvic ring injuries follow a bimodal pattern: high-energy trauma in younger patients and fragility fractures of the pelvis in older patients, the latter rising with population ageing.
Side-by-side society positions
- Emphasis
- Evidence-based THA management and surgeon-individualised approach selection
- Practical signal
- No single THA approach is mandated; outcomes depend on execution and selection
- Emphasis
- Standards for high-energy pelvic and acetabular trauma and time-critical care pathways
- Practical signal
- Complex pelvic and acetabular injuries should be managed in or referred to specialist centres
- Emphasis
- Reduction-target-led approach selection and column-based acetabular principles
- Practical signal
- Choose the exposure that controls the displaced column or wall directly
- Emphasis
- Cross-national education and outcome benchmarking via registries
- Practical signal
- Audit approach-specific complications against registry comparators
Registry evidence
- AOANJRR (Australia), NJR (England, Wales, NI and IoM), AJRR (US), SHAR (Sweden), the Norwegian and New Zealand registries collectively report excellent long-term THA survivorship and allow approach, fixation and bearing comparisons at population scale.
- Registries are the appropriate denominator for approach-specific signals such as dislocation, periprosthetic fracture and early revision; single-surgeon series cannot replace them.
High- versus limited-resource practice variation
- In well-resourced settings, CT, three-dimensional planning, intraoperative navigation, cell salvage, interventional radiology and dedicated pelvic trauma teams are routinely available.
- In limited-resource settings, plain radiographs and Judet views, careful clinical reduction, external fixation and damage-control principles carry more weight, and early referral of complex acetabular or pelvic injuries to a capable centre is often the safest decision.
- The constant across all settings is sound anatomy, a reduction-target-led approach, control of danger structures and a defined bailout.
References
- 1Wang H, Liu JF, Wang F, et al.. "A comparison of the clinical efficacy of total hip arthroplasty via direct anterior approach and posterior approach: A meta-analysis". Medicine (Baltimore). 2024PubMed
- 2Liu R, Zhao Y, Yu Z, et al.. "Comparative efficacy of direct anterior approach versus conventional surgical approaches in total hip arthroplasty: a systematic review and meta-analysis of randomized clinical trials". Journal of Orthopaedic Surgery and Research. 2025PubMed
- 3White RE, Forness TJ, Allman JK, Junick DW. "Effect of posterior capsular repair on early dislocation in primary total hip replacement". Clinical Orthopaedics and Related Research. 2001PubMed
- 4Hernandez NM, Steele JR, Wu CJ, et al.. "A specific capsular repair technique lowered early dislocations in primary total hip arthroplasty through a posterior approach". Arthroplasty Today. 2020PubMed
- 5Dahm F, Aichmair A, Dominkus M, Hofstaetter JG. "Incidence of lateral femoral cutaneous nerve lesions after direct anterior approach primary total hip arthroplasty - a literature review". Orthopaedics & Traumatology, Surgery & Research. 2021PubMed
- 6Yang XT, Huang HF, Sun L, et al.. "Direct anterior approach versus posterolateral approach in total hip arthroplasty: a systematic review and meta-analysis of randomized controlled studies". Orthopaedic Surgery. 2020PubMed
- 7Srivastava A, Rajnish RK, Kumar P, Haq RU, Dhammi IK. "Ilioinguinal versus modified Stoppa approach for open reduction and internal fixation of displaced acetabular fractures: a systematic review and meta-analysis of 717 patients across ten studies". Archives of Orthopaedic and Trauma Surgery. 2022PubMed
- 8Shigemura T, Murata Y, Yamamoto Y, et al.. "Comparison between ilioinguinal approach and modified Stoppa approach for the treatment of acetabular fractures: an updated systematic review and meta-analysis". Orthopaedics & Traumatology, Surgery & Research. 2022PubMed
- 9Kelly J, Ladurner A, Rickman M. "Surgical management of acetabular fractures - a contemporary literature review". Injury. 2020PubMed
- 10Ganz R, Gill TJ, Gautier E, Ganz K, Krugel N, Berlemann U. "Surgical dislocation of the adult hip: a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis". Journal of Bone and Joint Surgery (British). 2001PubMed
- 11Ganz R, Klaue K, Vinh TS, Mast JW. "A new periacetabular osteotomy for the treatment of hip dysplasias. Technique and preliminary results". Clinical Orthopaedics and Related Research. 1988PubMed
- 12Sambhav K, Nayyar AK, Elhence A, Gupta R, Ghatak S. "Anatomical variations of corona mortis in the anterior intrapelvic approach: a cadaveric study". Mymensingh Medical Journal. 2022PubMed
Controversies & Areas of Uncertainty
These are the live debates an examiner uses to test judgement rather than recall. A safe answer acknowledges genuine equipoise and then states a defensible position.
- Arguments for
- Earlier pain relief, more cups in the Lewinnek zone, lower posterior instability risk
- Arguments against
- Higher intraoperative fracture and LFCN injury, longer operative time, real learning curve
- Pragmatic position
- No universal winner; choose the approach you perform safely and counsel approach-specific risks
- Arguments for
- Stoppa is faster, less blood loss, fewer complications and gives medial quadrilateral access
- Arguments against
- Ilioinguinal may give marginally better radiographic reduction and more lateral iliac access
- Pragmatic position
- Pattern-driven choice; many units now default to anterior intrapelvic with a lateral window when needed
- Arguments for
- Percutaneous iliosacral or transsacral screws are low-morbidity if reduction and corridors are adequate
- Arguments against
- Sacral dysmorphism narrows safe corridors; malreduction cannot be corrected through a screw
- Pragmatic position
- Reduce first; fix percutaneously only with a safe corridor, otherwise open or navigate
- Arguments for
- Avoids two operations, allows early weight-bearing, addresses poor bone and head damage
- Arguments against
- Technically demanding, fixation of columns still required, limited long-term data
- Pragmatic position
- Reserve for selected elderly patients with comminution, impaction or head injury in experienced hands
- Arguments for
- May improve screw accuracy and reduce neural breach in difficult corridors
- Arguments against
- Cost, availability, radiation and workflow time; fluoroscopy in expert hands remains reliable
- Pragmatic position
- Useful adjunct for dysmorphic sacra and transsacral screws, not a substitute for anatomy knowledge
At a Glance Table
- Likely target
- Femoral neck, acetabulum and proximal femur
- Common approach family
- Anterior, anterolateral, direct lateral or posterior
- Main danger
- Approach-specific nerve injury, instability or abductor dysfunction
- Likely target
- Implant, cement, bone loss, trochanter or acetabulum
- Common approach family
- Often posterior or extensile lateral, with ETO when needed
- Main danger
- Sciatic nerve, abductor mechanism, bone loss and instability
- Likely target
- Posterior wall, posterior column and marginal impaction
- Common approach family
- Kocher-Langenbeck
- Main danger
- Sciatic nerve and heterotopic ossification
- Likely target
- Pelvic brim and anterior column
- Common approach family
- Ilioinguinal, modified Stoppa or pararectus
- Main danger
- External iliac vessels, femoral nerve and corona mortis
- Likely target
- Intrapelvic medial wall
- Common approach family
- Modified Stoppa or pararectus
- Main danger
- Obturator bundle and corona mortis
- Likely target
- Anterior ring, posterior ring or sacroiliac complex
- Common approach family
- Anterior plating, percutaneous screws, posterior fixation or lumbopelvic fixation
- Main danger
- Bleeding, malreduction and neural injury
PILOTApproach Description
Hook:A safe approach is piloted before it is performed.
Clinical Scenarios
Practise clinical reasoning and management decisions out loud
“A young adult has a posterior hip dislocation reduced in emergency. CT shows a displaced posterior wall fracture with marginal impaction.”
“An older patient has an acetabular fracture with anterior column involvement, quadrilateral surface displacement and medial femoral head migration.”
“A patient asks which approach is best for primary total hip replacement.”
“A patient has an unstable pelvic ring injury with symphyseal diastasis and posterior sacroiliac disruption.”
Describe Any Approach
- Position and table setup.
- Landmarks and incision.
- Internervous or intermuscular interval.
- Structures at risk.
- Exposure target and bailout plan.
- Repair and closure.
Hip Arthroplasty
- Anterior: LFCN and femoral exposure.
- Lateral: superior gluteal nerve and abductor repair.
- Posterior: sciatic nerve and posterior repair.
- Revision: extensile exposure and implant-removal plan.
Acetabulum
- Posterior wall or column: Kocher-Langenbeck.
- Anterior column or wall: ilioinguinal or modified Stoppa.
- Quadrilateral surface: intrapelvic access.
- Complex patterns: combined or staged approach.
Do Not Miss
- Corona mortis in anterior pelvic surgery.
- Sciatic nerve in posterior acetabular exposure.
- Abductor repair after lateral hip exposure.
- Posterior ring instability in pelvic ring injury.
“A safe hip or pelvic approach is chosen by target pathology, planned from imaging, performed through a known interval and closed with repair of the structures that maintain function and stability.”
Evidence Base
Every card below is anchored to a verified PubMed-indexed source. Read the statistics carefully: they are exam-quotable because they come from the actual papers, not from approximations.
Direct anterior versus posterior THA - pooled cohort and RCT data
- 33 studies, 14,478 patients (4,911 direct anterior, 9,567 posterior).
- Direct anterior gave lower day 1 and day 2 pain scores and more cups within the Lewinnek safe zone (RR 1.13).
- Direct anterior carried higher intraoperative fracture (OR 2.18) and lateral femoral cutaneous nerve injury (RR 7.84).
- Dislocation rate, blood loss and heterotopic ossification did not differ significantly.
Direct anterior versus conventional approaches - randomized-trial synthesis
- 17 RCTs, 1,575 patients (4 Level I, 13 Level II).
- Direct anterior prolonged operative time by a mean of 14.5 minutes.
- Direct anterior reduced day 1 pain and improved 1-month Harris Hip Score (MD 3.41).
- Nerve injury risk was markedly higher with direct anterior (RR 7.37); fracture, dislocation, infection and thrombosis did not differ.