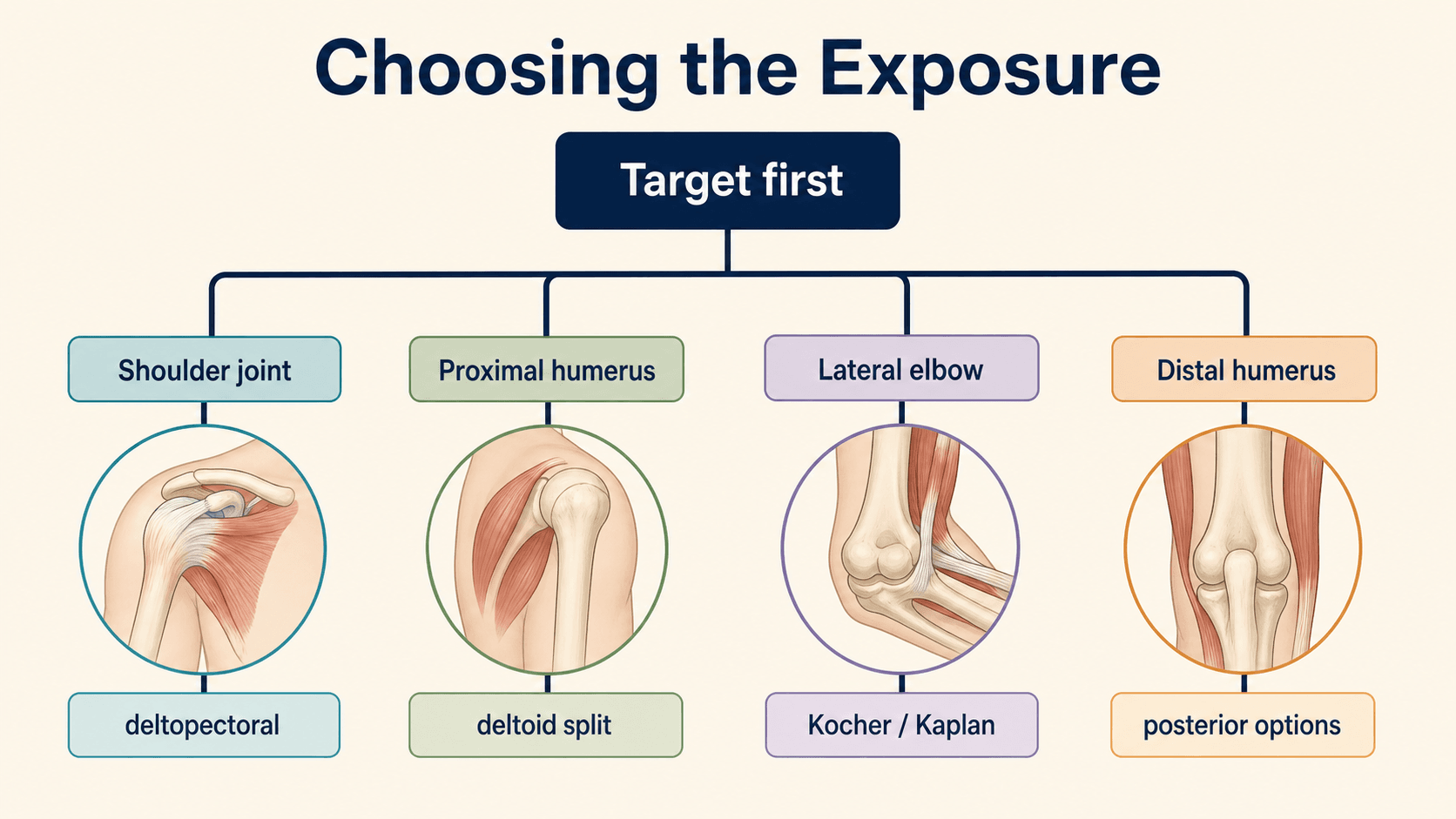
Choose the exposure that reaches the pathology while protecting function
- Do not describe an approach as a skin incision only. A safe answer includes position, landmarks, interval, danger structures, exposure target and repair.
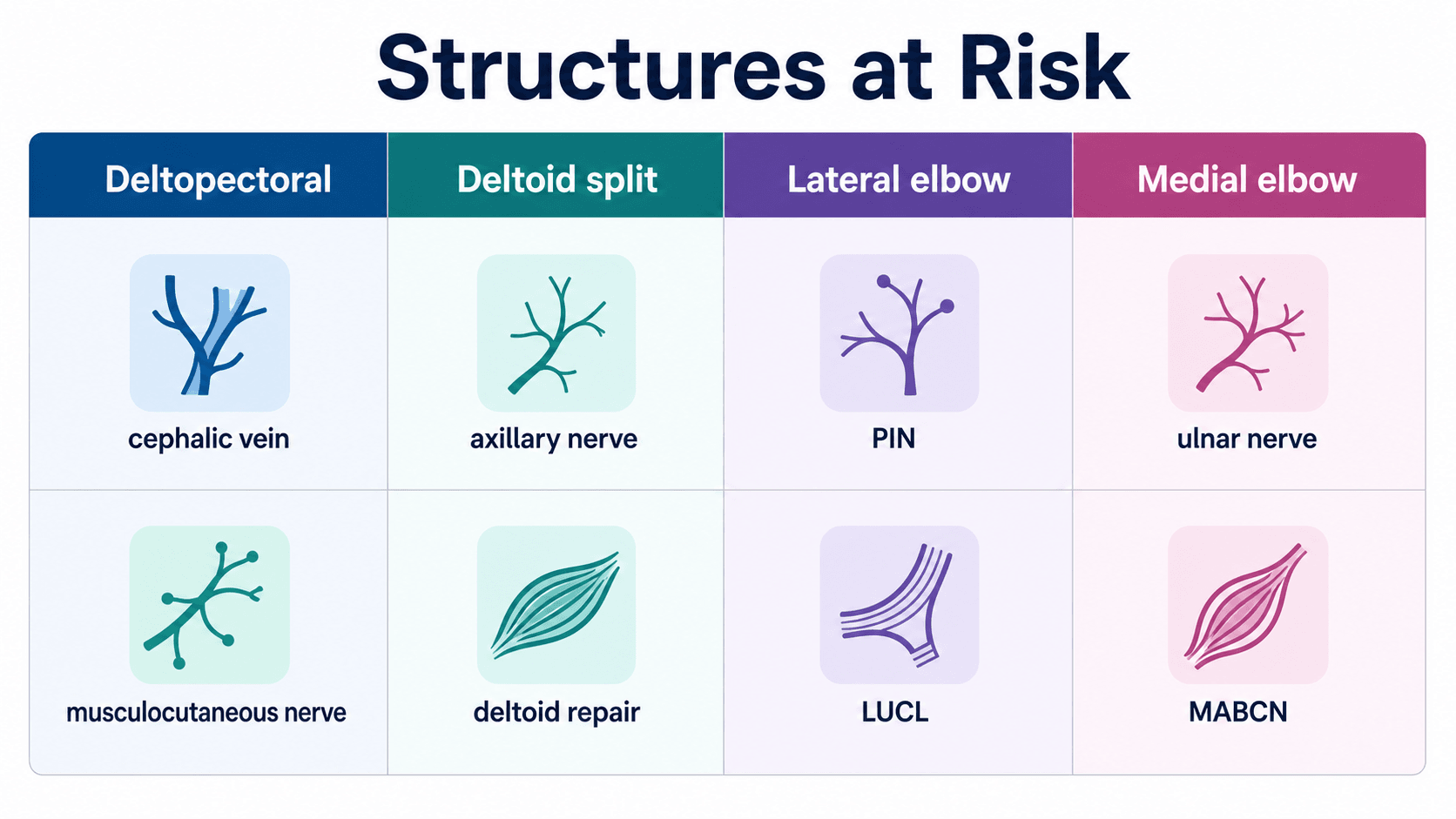
- Deltopectoral shoulder exposure is a true internervous plane between deltoid and pectoralis major, but cephalic vein, musculocutaneous nerve and axillary nerve still matter.
- Deltoid-splitting exposure is limited by the axillary nerve on the deep surface of deltoid; excessive distal extension risks deltoid paralysis.
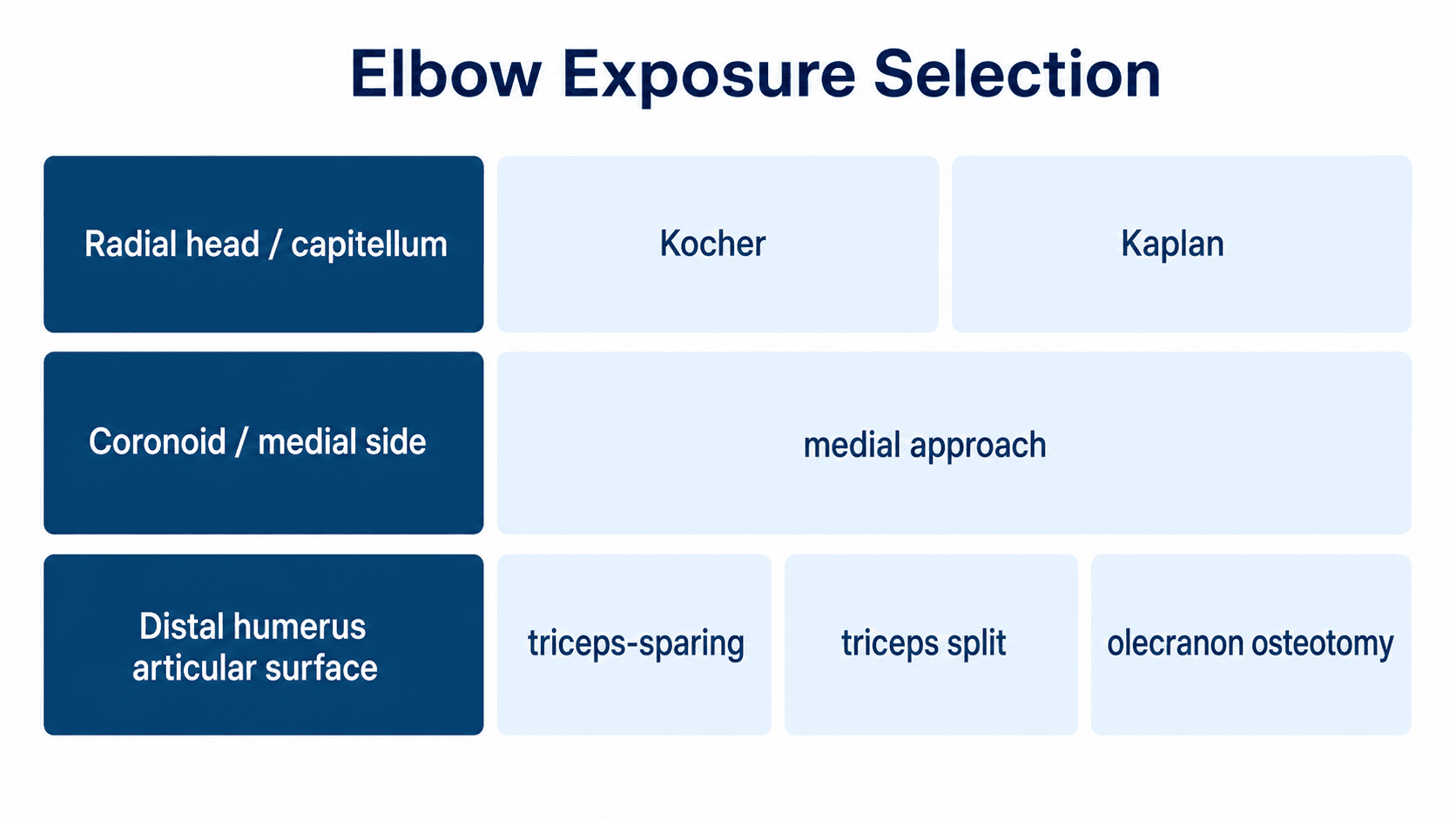
- Lateral elbow exposure requires deliberate choice between Kocher and Kaplan, with specific attention to the posterior interosseous nerve and lateral ligament complex.
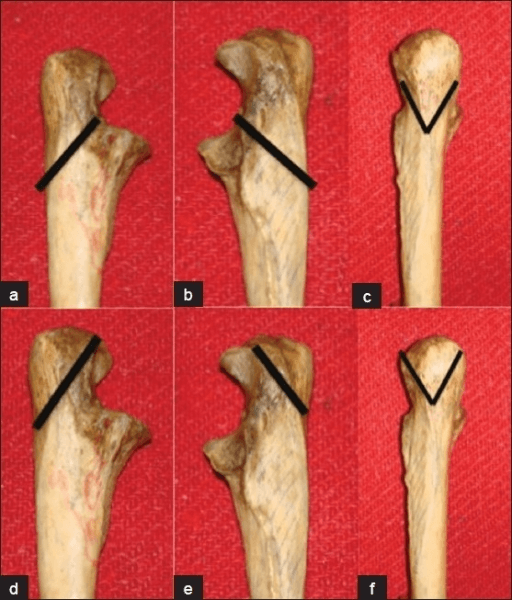
- Posterior distal humerus exposure is a triceps-management decision: triceps-sparing, triceps split, triceps reflection or olecranon osteotomy.
- “A named approach is not enough. Explain why that approach reaches the specific target better than the alternatives.
- “For shoulder surgery, loss of deltoid, cuff or subscapularis function can be more disabling than the scar.
- “For elbow surgery, the approach must preserve stability and allow early motion; stiffness is a major enemy.
- “If a ligament or tendon insertion is divided for exposure, the repair is part of the operation, not an optional closing step.
Surgical Approaches to the Shoulder and Elbow
Wrong exposure, excessive retraction, missed nerve baseline, poor soft-tissue repair or inadequate articular visualisation can cause the failure. The safest approach is the one that gives enough access without sacrificing the structures needed for postoperative function.
Overview/Epidemiology
Shoulder and elbow approaches are common in trauma, arthroplasty, instability, sports surgery, reconstruction and infection surgery. They are high-yield because a small technical error can produce a large functional problem: deltoid weakness, subscapularis failure, elbow instability, ulnar neuropathy, posterior interosseous nerve palsy, triceps insufficiency or disabling stiffness.
The approach must be chosen from the problem, not from habit. A deltopectoral shoulder exposure is versatile, but it is not the best answer for every proximal humerus target. A lateral elbow approach is logical for radial head and capitellar work, but a complex distal humerus fracture may need posterior articular visualisation. A posterior elbow incision can be combined with several different triceps strategies, each with different exposure and morbidity.
Good approach planning answers three questions:
- What must be exposed? Joint, column, tuberosity, glenoid, coronoid, radial head, humeral shaft or implant.
- What must be protected? Nerve, vessel, tendon, ligament, cuff, deltoid, triceps and skin envelope.
- What must be repaired? Subscapularis, capsule, rotator interval, LUCL, MCL, triceps or olecranon osteotomy.
Do not choose an approach because it is familiar. Choose it because it gives direct access to the reduction, implant, reconstruction or debridement target with acceptable risk.
Anatomy/Biomechanics
The shoulder and elbow are soft-tissue dependent joints. The shoulder depends on the deltoid, rotator cuff, subscapularis, capsule and glenoid version; the elbow depends on congruent articular anatomy, collateral ligaments, capsule, triceps and early motion. An approach that damages these structures can compromise the reconstruction.
Shoulder region
Key structures:
- Cephalic vein: marks the deltopectoral interval; it may be taken medially or laterally depending preference and exposure.
- Deltoid: primary power muscle for elevation; denervation or detachment failure is disabling.
- Pectoralis major: medial boundary of the deltopectoral interval.
- Conjoint tendon: landmark for deep anterior shoulder exposure; excessive medial retraction risks musculocutaneous nerve traction.
- Subscapularis: must be managed carefully in arthroplasty and instability surgery; failure causes weakness, pain and anterior instability.
- Axillary nerve: at risk with inferior shoulder dissection, deltoid splitting and aggressive retraction.
- Rotator cuff footprint: critical during tuberosity fixation, cuff repair and proximal humerus surgery.
Elbow region
Key structures:
- Ulnar nerve: vulnerable in medial and posterior elbow exposure; preoperative symptoms must be documented.
- Posterior interosseous nerve: vulnerable during lateral elbow approaches, radial neck work and distal extension.
- Lateral ulnar collateral ligament: protects against posterolateral rotatory instability; if released, it must be repaired.
- Medial collateral ligament: primary valgus stabiliser; important in medial elbow exposure and coronoid work.
- Triceps: posterior exposure strategy determines articular visualisation and postoperative extension strength.
- Capsule: release improves exposure but can destabilise the elbow if collateral structures are not repaired.
The deltoid, subscapularis, LUCL, MCL and triceps are not simply structures crossed during exposure. They are functional stabilisers and power units. If they are divided, their repair must be planned before they are divided.
Internervous Plane
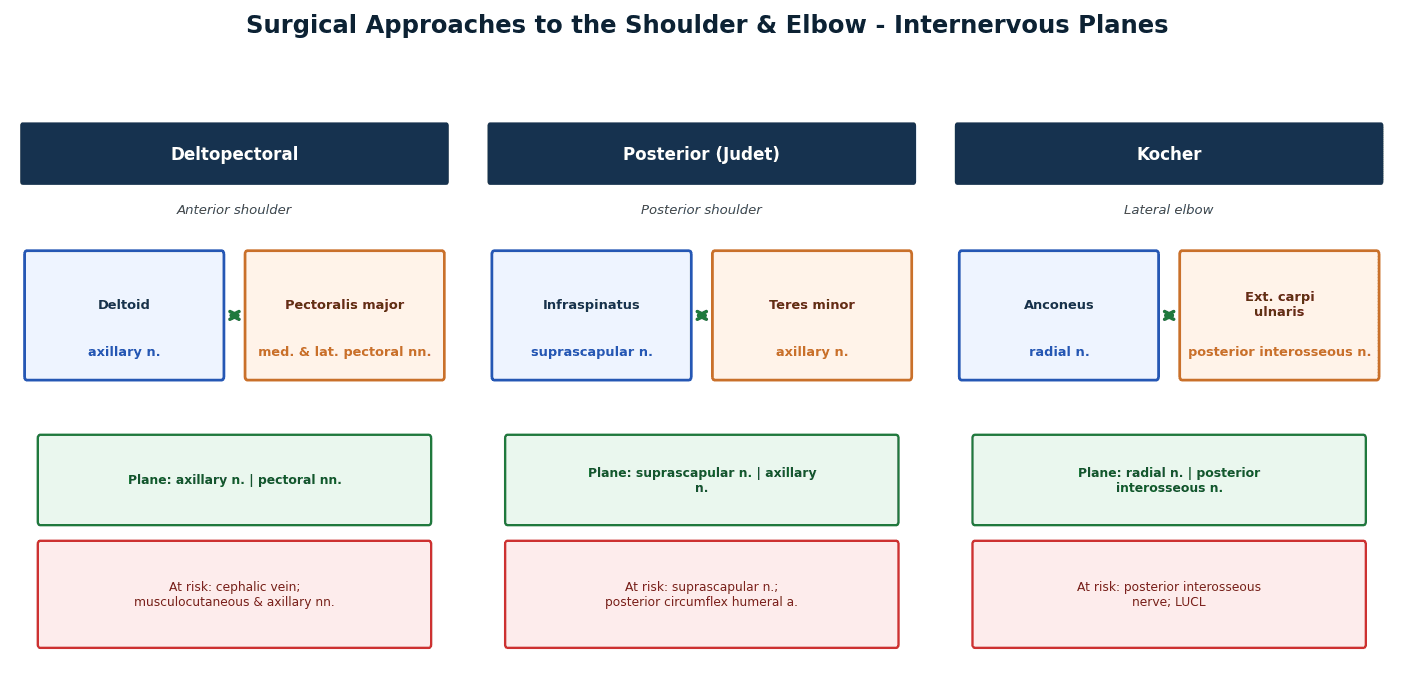
Internervous planes matter because they allow exposure without denervating a muscle group. Some approaches use true internervous intervals; others are muscle-splitting or tendon-reflecting approaches that are safe only if the split is limited and the repair is reliable.
- Plane
- Deltoid supplied by axillary nerve; pectoralis major supplied by pectoral nerves
- Practical consequence
- True internervous interval, but deep retraction still risks musculocutaneous and axillary nerves
- Plane
- Muscle split through deltoid fibres
- Practical consequence
- Not a full internervous plane; distal split is limited by axillary nerve
- Plane
- Deltoid/cuff split or interval depending technique
- Practical consequence
- Useful for posterior glenoid and scapular work; protect axillary and suprascapular nerve regions
- Plane
- Anconeus and ECU
- Practical consequence
- Common lateral elbow interval; protect PIN and preserve or repair LUCL
- Plane
- ECRB and EDC
- Practical consequence
- More anterior radiocapitellar access; PIN risk increases with distal/anterior dissection
- Plane
- Triceps management strategy rather than a single internervous plane
- Practical consequence
- Exposure depends on triceps-sparing, triceps split, reflection or olecranon osteotomy
Even a true internervous plane can become unsafe if retraction is aggressive, the incision is extended in the wrong direction, or the surgeon forgets the deep nerve course.
Clinical Assessment
The preoperative assessment should decide whether the planned approach is safe and adequate.
History
- Previous operations, scars, infection, instability surgery, arthroplasty or fracture fixation.
- Current pathology: trauma, arthritis, instability, cuff disease, infection, tumour or nonunion.
- Neurological symptoms: deltoid weakness, lateral arm numbness, ulnar nerve paraesthesia, radial/PIN weakness.
- Functional requirements: overhead work, sport, manual labour, transfers, walking aid use.
- Anticoagulation, diabetes, smoking, inflammatory disease and wound-healing risk.
Examination
- Shoulder: deltoid function, axillary sensation, cuff strength, subscapularis tests, active and passive range, instability signs and skin condition.
- Elbow: range of motion, ulnar nerve symptoms, intrinsic hand function, PIN function, collateral stability, swelling, open wounds and soft-tissue envelope.
- Trauma: vascular status, compartments, open wounds, contamination, associated fractures and reduction urgency.
What must be documented
- Baseline nerve function before surgery.
- Skin scars and intended incision relationship.
- Vascular status.
- Open-wound location and whether it conflicts with definitive exposure.
- Active motion and stiffness, especially at the elbow.
Investigations
Imaging should answer the exposure question, not just confirm the diagnosis.
Radiographs
- Shoulder trauma series: AP, scapular Y and axillary or modified axillary view.
- Elbow AP and lateral views, with radiocapitellar and ulnohumeral alignment.
- True lateral elbow radiographs for dislocation, coronoid, olecranon and distal humerus work.
- Long humerus views when shaft extension or radial nerve risk is relevant.
CT
CT is especially useful for:
- proximal humerus fracture pattern and tuberosity involvement
- glenoid bone loss or posterior glenoid deformity
- scapula and glenoid fractures
- distal humerus articular comminution
- radial head and capitellar fractures
- coronoid fracture morphology
- preoperative planning for osteotomy or revision implants
MRI and ultrasound
MRI is useful when rotator cuff, subscapularis, labrum, capsule, infection extension or muscle quality changes the operation. Ultrasound can assess cuff integrity in selected patients but does not replace CT for fracture morphology.
If the plan is a lateral elbow approach, imaging should show that the target is lateral or radiocapitellar. If the plan is posterior distal humerus exposure, CT should justify the need for articular visualisation and column fixation.
Approach Selection
Shoulder approach selection
- Preferred exposure
- Deltopectoral
- Why
- Reliable anterior access to humeral head, glenoid and subscapularis management
- Avoid if
- Severe anterior scarring or unusual pathology requiring posterior access
- Preferred exposure
- Deltopectoral
- Why
- Access to subscapularis, capsule and anterior glenoid
- Avoid if
- Poor soft tissues or arthroscopic procedure preferred
- Preferred exposure
- Deltoid-splitting or deltopectoral
- Why
- Lateral split gives direct tuberosity access; deltopectoral is more extensile
- Avoid if
- Complex fracture requiring head, lesser tuberosity or arthroplasty access
- Preferred exposure
- Usually deltopectoral
- Why
- Better anterior access to tuberosities, head, bicipital groove and conversion options
- Avoid if
- Poor soft tissue may require staged or alternative strategy
- Preferred exposure
- Posterior shoulder or Judet-type exposure
- Why
- Direct posterior access
- Avoid if
- Anterior pathology alone
Elbow approach selection
- Preferred exposure
- Kocher or Kaplan
- Why
- Direct radiocapitellar access
- Key risk
- PIN injury, LUCL injury
- Preferred exposure
- Kaplan or extensile lateral
- Why
- More anterior radiocapitellar visualisation
- Key risk
- PIN with distal anterior dissection
- Preferred exposure
- Medial approach through or around FCU/flexor-pronator mass
- Why
- Direct access to medial coronoid and sublime tubercle
- Key risk
- Ulnar nerve and MCL
- Preferred exposure
- Posterior approach with chosen triceps strategy
- Why
- Bicolumnar fixation and articular reduction
- Key risk
- Ulnar nerve, triceps morbidity, stiffness
- Preferred exposure
- Posterior subcutaneous approach
- Why
- Direct access to olecranon
- Key risk
- Prominent metalwork and wound problems
Patient Positioning
Positioning must allow exposure, reduction, imaging, implant insertion and safe anaesthesia access. A perfect incision is not enough if fluoroscopy, reduction tools or the assistant cannot work.
Shoulder positioning
- Beach-chair: common for arthroplasty, instability and cuff surgery; check head, neck, blood pressure and arm access.
- Supine with bump: useful for deltopectoral exposure and fracture work when fluoroscopy is needed.
- Lateral decubitus: common for arthroscopy and some posterior work; protect pressure points and brachial plexus traction.
- Prone or floating shoulder setups: selected scapula and posterior shoulder exposures.
Elbow positioning
- Supine with arm across chest: useful for lateral elbow, radial head and selected distal humerus work.
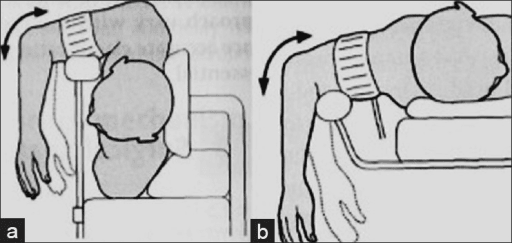
- Lateral decubitus: common for posterior distal humerus exposure; arm supported over bolster.
- Prone: useful for posterior elbow and distal humerus exposure; confirm anaesthetic and airway access.
- Hand table or arm board: useful for medial/lateral elbow approaches and fluoroscopy.
Check fluoroscopy, tourniquet access, reduction manoeuvres, plate trajectory and the planned extension of exposure before the limb is prepared and draped.
Surgical Technique
Universal approach steps
- Confirm the procedure, side, imaging and implants.
- Review baseline nerve function.
- Position the patient and confirm fluoroscopy before preparing the limb.
- Mark landmarks and planned extension lines.
- Incise through safe skin and subcutaneous planes.
- Identify the planned interval before deep dissection.
- Protect named nerves and vessels deliberately.
- Confirm the exposure reaches the target before committing to fixation or reconstruction.
- Repair divided stabilisers, tendons, capsule or osteotomy.
- Document the approach, structures protected and repair performed.
If a deltoid split is inadequate, do not extend distally into the axillary nerve zone. Convert or extend safely. If a posterior elbow exposure is inadequate, change the triceps strategy deliberately rather than tearing through the interval.
Complications
- Key complications
- Cephalic vein bleeding, musculocutaneous traction, axillary nerve injury, subscapularis failure, stiffness
- Prevention
- Gentle retraction, know nerve course, reliable subscapularis repair, rehabilitation plan
- Key complications
- Axillary nerve injury, deltoid weakness, inadequate exposure, cuff injury
- Prevention
- Limit distal split, blunt dissection, convert if inadequate
- Key complications
- Axillary or suprascapular nerve risk, deltoid/cuff morbidity, stiffness
- Prevention
- Precise anatomy, avoid aggressive medial retraction, repair cuff/deltoid
- Key complications
- PIN palsy, LUCL insufficiency, radiocapitellar stiffness, heterotopic ossification
- Prevention
- Controlled distal dissection, ligament repair, early safe motion
- Key complications
- Ulnar neuropathy, MABCN neuroma, valgus instability, stiffness
- Prevention
- Document baseline, protect cutaneous nerves, plan ulnar nerve handling, repair MCL/flexor-pronator
- Key complications
- Ulnar neuropathy, triceps weakness, olecranon nonunion, prominent metalwork, stiffness
- Prevention
- Secure nerve strategy, robust triceps/osteotomy repair, early motion when safe
Red flags after surgery
- New deltoid paralysis or lateral arm numbness.
- New PIN palsy with finger/thumb extension weakness.
- Worsening ulnar nerve symptoms.
- Loss of elbow stability after lateral approach.
- Inability to actively extend elbow after posterior approach.
- Wound breakdown over olecranon or shoulder incision.
- Increasing pain, fever, drainage or acute stiffness suggesting infection or haematoma.
Differentiating a new postoperative nerve deficit
A new motor or sensory deficit after an upper limb approach must be localised quickly, because the differential ranges from a recoverable traction neurapraxia to a divided nerve needing exploration. The pattern of weakness usually points to the nerve at risk for that specific approach.
- Approach most associated
- Deltoid split, inferior shoulder dissection
- Typical motor sign
- Weak shoulder abduction, deltoid wasting
- Sensory sign
- Numb lateral upper arm (regimental badge)
- Usual cause and action
- Traction or split too distal; if no recovery on serial review, image and consider exploration
- Approach most associated
- Lateral elbow (Kocher / Kaplan)
- Typical motor sign
- Weak finger and thumb extension, wrist drifts radially (wrist extension preserved)
- Sensory sign
- No sensory loss (motor nerve)
- Usual cause and action
- Distal or supinated dissection; observe a neurapraxia, explore if division suspected
- Approach most associated
- Medial and posterior elbow
- Typical motor sign
- Weak intrinsics, weak FDP to ring/little finger, clawing
- Sensory sign
- Numb little and ulnar ring finger
- Usual cause and action
- Mobilisation, tight transposition or kinking; check construct, may settle by 12 months
- Approach most associated
- Deltopectoral with deep medial retraction
- Typical motor sign
- Weak elbow flexion and supination
- Sensory sign
- Numb lateral forearm
- Usual cause and action
- Conjoint-tendon over-retraction; usually traction neurapraxia, relieve retraction
- Approach most associated
- Distal humeral extension / shaft
- Typical motor sign
- Wrist drop, weak finger and thumb extension
- Sensory sign
- Numb dorsal first web space
- Usual cause and action
- Spiral-groove handling; protect and document, explore if iatrogenic division suspected
Postoperative Care
Postoperative care depends on what was repaired, not only on the skin approach.
Shoulder
- Protect subscapularis repair after arthroplasty or instability surgery according to repair method.
- Monitor axillary nerve and deltoid function.
- Start passive and active-assisted motion according to reconstruction stability.
- Avoid early resisted internal rotation after subscapularis repair.
- Follow fracture fixation or arthroplasty radiographs when indicated.
Elbow
- Balance soft-tissue healing against the high risk of stiffness.
- Check ulnar, radial/PIN and median nerve function after surgery.
- Use a hinged brace when stability or ligament repair requires protection.
- Begin controlled motion as early as fixation and soft-tissue repair permit.
- Monitor olecranon osteotomy fixation, triceps repair and wound pressure points.
The elbow stiffens quickly. A good operation includes a realistic motion plan that protects fixation and repair while avoiding unnecessary prolonged immobilisation.
Outcomes/Prognosis
Outcomes are determined by pathology, patient factors, surgical execution and rehabilitation. The approach contributes by enabling reduction or reconstruction while minimising additional morbidity.
Shoulder outcomes depend on restoration of stable arthroplasty mechanics, tuberosity/cuff healing, subscapularis function, deltoid function and avoidance of nerve injury. A well-executed deltopectoral approach is repeatable and versatile, but poor subscapularis management can create pain, weakness and instability. A deltoid split can be efficient for lateral targets, but nerve injury is a major failure.
Elbow outcomes depend on articular reduction, stability, ulnar nerve status, triceps function and early motion. For distal humerus fractures, an exposure that gives inadequate articular visualisation can compromise reduction; an exposure that gives excellent visualisation but creates triceps or osteotomy morbidity must be justified and repaired well.
Guidelines, Registries & Global Practice
There is no single international guideline that prescribes a specific shoulder or elbow approach; exposure choice is a surgeon-led decision governed by anatomy, pathology and the registry-level evidence on the underlying operation. The unifying principles are universal: document preoperative nerve status, position safely, choose exposure from imaging, protect named structures and plan early rehabilitation.
Global epidemiology and burden
Proximal humerus fractures are among the most common fragility fractures, typically third behind hip and distal radius fractures in older adults, and most are managed without an open approach at all. Distal humerus fractures show a bimodal distribution (high-energy young men, low-energy elderly women) and are rising with population ageing. This epidemiology drives the global debate over when an operative exposure is even warranted, which is the backdrop to approach selection.
Side-by-side guidance and registry evidence
- Domain
- Displaced proximal humerus fracture
- Signal
- No benefit of surgery over non-operative care for most displaced fractures; fewer patients need an open shoulder approach than historically performed
- Evidence level
- Level I RCT
- Domain
- Subscapularis management in TSA
- Signal
- Tenotomy and lesser tuberosity osteotomy give equivalent function; LTO heals more reliably (Levine RCT, PMID 30771825)
- Evidence level
- Level I RCT
- Domain
- Open injuries and trauma pathways
- Signal
- Emphasise early senior decision-making, soft-tissue assessment and orthoplastic input before definitive exposure
- Evidence level
- Guideline / consensus
- Domain
- Distal humerus and elbow trauma
- Signal
- Posterior approaches with a deliberate triceps strategy give bicolumnar access; preserve and protect the ulnar nerve
- Evidence level
- Expert consensus / technique
- Domain
- Fracture care pathways
- Signal
- Focus on shared decision-making, imaging and rehabilitation rather than mandating a specific exposure
- Evidence level
- Guideline
- Domain
- Shoulder arthroplasty
- Signal
- Track implant survival and revision; the deltopectoral exposure underpins most anatomic and reverse arthroplasty volume
- Evidence level
- Registry observational
Practice variation
- When to expose at all: PROFHER and related trials shifted many displaced proximal humerus fractures towards non-operative care, reducing deltopectoral exposures in elderly patients while reverse shoulder arthroplasty (deltopectoral) has grown for selected complex patterns.
- Subscapularis strategy: practice varies between tenotomy, peel and lesser tuberosity osteotomy; the evidence supports any well-executed and well-repaired technique.
- Triceps and ulnar nerve handling in the elbow: olecranon osteotomy versus triceps-sparing exposures, and in situ versus transposed ulnar nerve, remain surgeon-preference decisions supported by Level I and IV evidence rather than mandated by guideline.
- System factors: implant availability, trauma network maturity, orthoplastic support and rehabilitation access drive much of the international variation in exposure and timing.
Local practice reminders
- Document neurological findings clearly before shoulder and elbow trauma surgery.
- Discuss complex elbow trauma early with surgeons experienced in elbow reconstruction when available.
- Plan rehabilitation access before procedures that need early supervised motion.
- In arthroplasty, use the approach and implant system that the treating team can perform reliably and revise safely.
References
- 1Chalmers PN, Van Thiel GS, Trenhaile SW. "Surgical Exposures of the Shoulder". Journal of the American Academy of Orthopaedic Surgeons. 2016PubMed
- 2Zlotolow DA, Catalano LW 3rd, Barron OA, Glickel SZ. "Surgical exposures of the humerus". Journal of the American Academy of Orthopaedic Surgeons. 2006PubMed
- 3Hausman MR, Kator JL, Kim JM. "Surgical Approaches to the Elbow in Fixation of Traumatic Injuries". Journal of the American Academy of Orthopaedic Surgeons. 2025PubMed
- 4Levine WN, Munoz J, Hsu S, Byram IR, Bigliani LU, Ahmad CS, et al.. "Subscapularis tenotomy versus lesser tuberosity osteotomy during total shoulder arthroplasty for primary osteoarthritis: a prospective, randomized controlled trial". Journal of Shoulder and Elbow Surgery. 2019PubMed
- 5Yildirim C, Demirel M, Bayram E, Ekinci M, Yilmaz M. "Acromion-axillary nerve distance and its relation to the arm length in the prediction of the axillary nerve position: a clinical study". Journal of Orthopaedic Surgery and Research. 2022PubMed
- 6Hohenberger GM, Schwarz AM, Maier MJ, Grechenig P, Dauwe J, et al.. "Safe zone for the posterior interosseous nerve with regard to the lateral and posterior approaches to the proximal radius". Surgical and Radiologic Anatomy. 2018PubMed
- 7Coles CP, Barei DP, Nork SE, Taitsman LA, Hanel DP, Henley MB. "The olecranon osteotomy: a six-year experience in the treatment of intraarticular fractures of the distal humerus". Journal of Orthopaedic Trauma. 2006PubMed
- 8Dehghan N, Nauth A, Hall J, Vicente M, McKee MD, Schemitsch EH. "In Situ Placement Versus Anterior Transposition of the Ulnar Nerve for Distal Humerus Fractures Treated With Plate Fixation: A Multicenter Randomized Controlled Trial". Journal of Orthopaedic Trauma. 2021PubMed
- 9Rangan A, Handoll H, Brealey S, Jefferson L, Keding A, Corbacho B, et al.. "Surgical vs nonsurgical treatment of adults with displaced fractures of the proximal humerus: the PROFHER randomized clinical trial". JAMA. 2015PubMed
At a Glance Table
- Common target
- Glenohumeral joint and proximal humerus
- Approach options
- Deltopectoral most common; superior or posterior in selected cases
- Main danger
- Subscapularis failure, axillary nerve injury, instability
- Common target
- Capsulolabral complex and subscapularis interval
- Approach options
- Deltopectoral open exposure or arthroscopic portals
- Main danger
- Musculocutaneous nerve, axillary nerve, subscapularis management
- Common target
- Lateral proximal humerus and rotator cuff insertion
- Approach options
- Deltoid-splitting or deltopectoral depending fracture pattern
- Main danger
- Axillary nerve and deltoid dysfunction
- Common target
- Radiocapitellar joint
- Approach options
- Kocher or Kaplan lateral elbow approach
- Main danger
- Posterior interosseous nerve and LUCL
- Common target
- Medial trochlea, coronoid, sublime tubercle, MCL
- Approach options
- Medial approach through or around flexor-pronator mass
- Main danger
- Ulnar nerve and medial antebrachial cutaneous nerve
- Common target
- Articular surface and both columns
- Approach options
- Posterior approach with triceps-sparing, triceps split, triceps reflection or olecranon osteotomy
- Main danger
- Ulnar nerve, triceps dysfunction, osteotomy complications and stiffness
SAFERDescribe Any Upper Limb Approach
Hook:A good approach answer should be safe before it is detailed.
AMURUpper Limb Nerve Check
Hook:Before shoulder and elbow surgery, know the nerve at risk.
Clinical Scenarios
Practise clinical reasoning and management decisions out loud
“You are asked to describe a deltopectoral approach for shoulder arthroplasty.”
“A patient has a displaced radial head fracture requiring fixation or replacement. Describe the lateral elbow exposure and the structures at risk.”
“CT shows a comminuted intra-articular distal humerus fracture requiring bicolumnar fixation. How do you choose the posterior exposure?”
Approach Answer
- Position, imaging and landmarks.
- Interval or muscle strategy.
- Danger structures.
- Exposure target.
- Repair and rehabilitation.
Shoulder
- Deltopectoral: deltoid and pectoralis major interval.
- Protect cephalic vein, musculocutaneous nerve and axillary nerve.
- Subscapularis repair matters.
- Deltoid split is limited by axillary nerve safety.
Elbow
- Kocher: anconeus and ECU.
- Kaplan: ECRB and EDC.
- Medial approach: ulnar nerve and MABCN.
- Posterior approach: choose triceps strategy.
Do Not Miss
- Baseline nerve function.
- PIN in lateral elbow exposure.
- LUCL repair if released.
- Ulnar nerve in posterior or medial elbow surgery.
- Early safe motion after elbow surgery.
“Shoulder and elbow approaches should be described as functional exposures: choose the target, use the correct interval, protect the named nerves, repair stabilisers and plan rehabilitation.”
Evidence Base
Surgical Exposures of the Shoulder
- Open shoulder surgery is challenging because the deltoid and rotator cuff envelop the joint, and in most approaches exposure is limited by the proximity and importance of the axillary nerve.
- Deltopectoral, deltoid-splitting and posterior approaches each have distinct advantages, disadvantages and risks, with variations and extensions of each.
- Mastery of all three exposures gives the surgeon flexibility to address the widest variety of pathology.
Surgical Exposures of the Humerus
- No truly safe fully extensile approach to the humerus exists because the spiralling radial nerve crosses the posterior midshaft; the nerve must be mobilised at the spiral groove for maximal exposure.
- The anterolateral approach uses an internervous plane between axillary and deltoid nerves proximally and radial and musculocutaneous nerves distally; deltopectoral remains the most widely used proximal exposure.
- Distal intra-articular exposure depends on triceps mobilisation by olecranon osteotomy or triceps release, coupled with triceps-splitting or paratricipital extension.
Subscapularis tenotomy versus lesser tuberosity osteotomy in TSA (RCT)
- 60 shoulders randomised to subscapularis tenotomy or lesser tuberosity osteotomy during anatomic total shoulder arthroplasty for primary osteoarthritis.
- No significant difference in range of motion or clinical outcome scores at one year between the two techniques.
- Lesser tuberosity osteotomy healed more reliably (bone-to-bone union in 93.1%) than tenotomy (no full-thickness tear in 86.7% on ultrasound), but added operative and repair time.
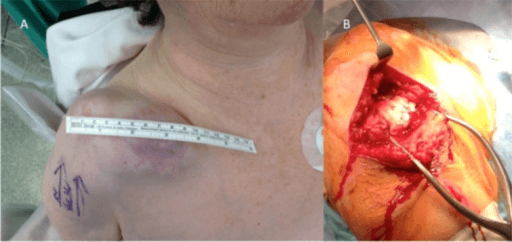
Acromion-axillary nerve distance: safe zone for the deltoid-splitting approach
- In 37 patients undergoing proximal humerus fixation, mean acromion-axillary nerve distance was 6 cm (range 5.5-6.6 cm) and the axillary nerve index (nerve distance / arm length) averaged 0.18.
- The axillary nerve position was predictable from anatomy in only 18% of patients, underlining wide individual variation.
- A zone of 5.5 cm distal to the anterolateral edge of the acromion can be regarded as the safe limit for an anterolateral deltoid-splitting incision.