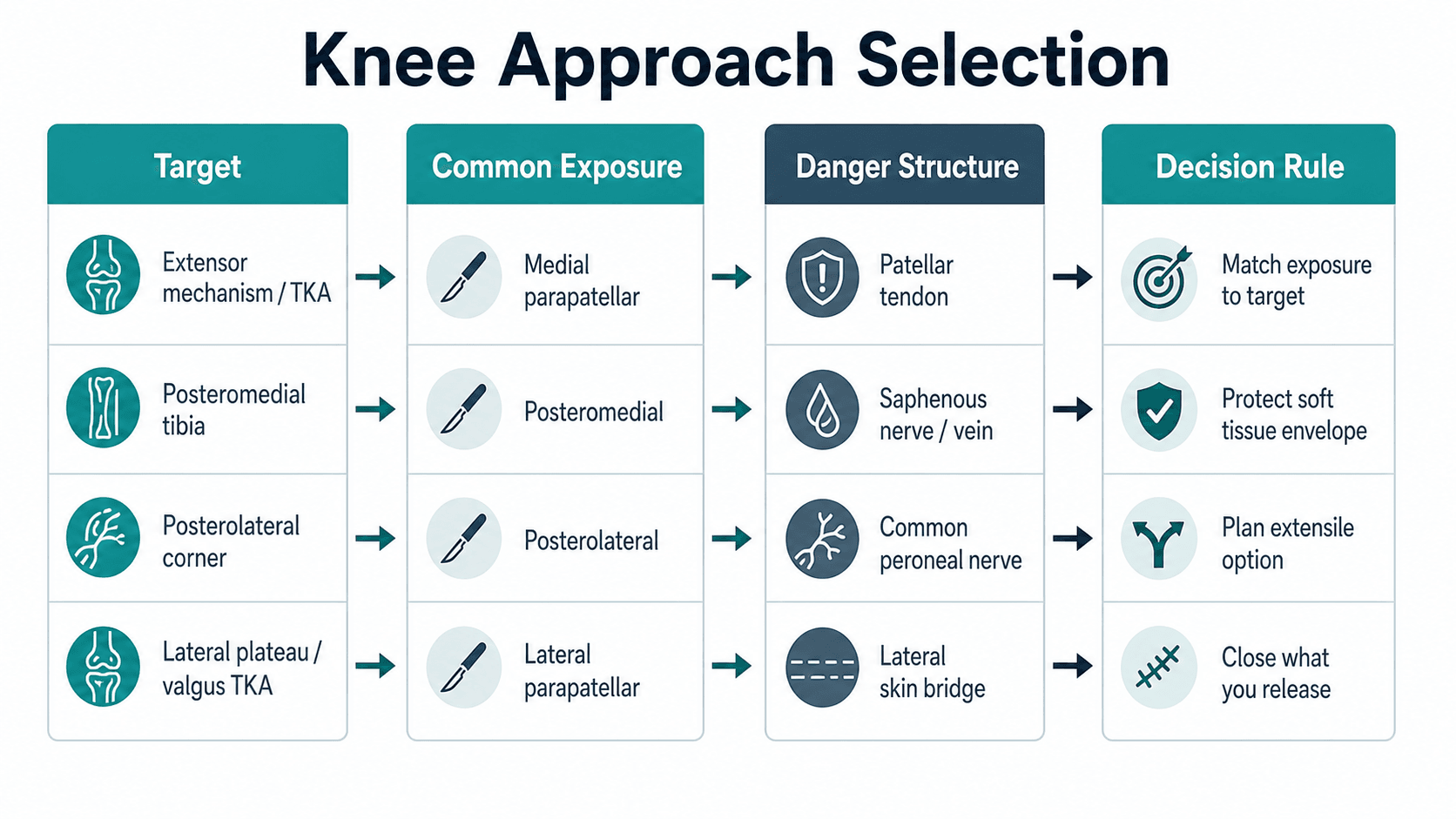
Expose the target, protect the extensor mechanism, close what you release
- Do not describe a knee approach by incision alone. State position, landmarks, interval, target, danger structures and closure.
- The medial parapatellar approach is extensile and reliable, but the patellar tendon and blood supply must be protected.
- Subvastus and midvastus approaches may preserve extensor mechanism continuity, but exposure is less extensile and patient selection matters.
- Posteromedial approaches risk the saphenous nerve and vein; posterolateral approaches require deliberate common peroneal nerve protection.
- The best approach is the one that reaches the pathology safely without compromising soft-tissue envelope, fixation or later reconstruction.
- “A valgus TKA may need lateral releases or a lateral parapatellar approach when the lateral side is the contracted side.
- “A posteromedial tibial plateau fragment needs a posterior buttress; an anterolateral plate alone may not control it.
- “Common peroneal nerve identification is not optional in posterolateral knee exposure.
- “Closure is part of the approach: arthrotomy, retinaculum, capsule, quadriceps split, subvastus sleeve and released tendons must be restored deliberately.
Surgical Approaches to the Knee
Choose the approach by the structure that needs reduction, fixation, release or reconstruction. A familiar approach becomes unsafe when it cannot reach the target or forces excessive soft-tissue stripping.
- Useful Exposure
- Medial parapatellar, midvastus or subvastus
- Reason
- Extensor mechanism access, patellar eversion or subluxation, and implant workflow.
- Useful Exposure
- Medial parapatellar with extensile options
- Reason
- Reliable exposure and ability to extend proximally or distally.
- Useful Exposure
- Medial approach with lateral releases or lateral parapatellar approach
- Reason
- Approach must allow safe balancing of the contracted side.
- Useful Exposure
- Posteromedial approach
- Reason
- Direct reduction and buttress fixation of posterior medial shear.
- Useful Exposure
- Posterolateral approach
- Reason
- Direct access to fibular head, LCL, popliteus and PLC structures.
PLATEApproach Description
Hook:PLATE keeps a knee approach description practical.
FINDPosterolateral Safety
Hook:Find the nerve before deep posterolateral work.
Overview and Indications
Knee approaches are chosen by target pathology. The decision is different for total knee arthroplasty, tibial plateau fixation, extensor mechanism repair, multiligament reconstruction, infection washout and revision surgery. A safe answer starts with what must be seen or controlled: the extensor mechanism, medial plateau, posteromedial fragment, lateral plateau, posterolateral corner, patella, distal femur, proximal tibia or prosthetic joint.
An approach is a controlled route: position, landmarks, interval, deep exposure, danger structures, extension options and closure. The skin incision is only the visible start.
Relevant Anatomy
The knee is unforgiving because the soft-tissue envelope is thin, the extensor mechanism is essential for function, and several approaches work close to named nerves and vessels. The approach must preserve skin bridges, protect the patellar tendon insertion, avoid devascularising the patella unnecessarily and respect neurovascular structures.
Quadriceps tendon, patella, retinaculum and patellar tendon determine exposure and postoperative function. A patellar tendon avulsion is a major complication.
Saphenous nerve and great saphenous vein are at risk around medial and posteromedial exposures. The pes anserinus may need controlled mobilisation.
The common peroneal nerve wraps around the fibular neck and must be identified for posterolateral work or when severe valgus correction places it at stretch risk.
Multiple incisions around the knee can threaten skin vascularity. Plan previous scars, future flaps and fixation incisions before committing to a new approach.
"Protect the patellar blood supply" refers to a specific anatomy: the patella is fed by a peripatellar anastomotic ring formed by the superior and inferior, medial and lateral genicular arteries, the descending genicular artery and the anterior tibial recurrent artery, with the superolateral genicular artery and the inferior-pole vessels in the infrapatellar (Hoffa) fat pad the dominant contributors. This is why a lateral retinacular release sacrifices the superolateral genicular artery, and excising the fat pad sacrifices the inferior supply - doing both (for example a medial arthrotomy plus a lateral release) is the classic "double hit" that risks patellar osteonecrosis, stress fracture and avascular fragmentation. Preserve the fat pad and the superolateral vessel where possible, and limit unnecessary retinacular stripping.

Internervous Plane and Intervals

Some knee approaches use true or practical intervals; others are controlled arthrotomies or tendon-splitting approaches. The safe principle is to name what is being protected and what is being released.
- Plane or Release
- Quadriceps tendon and medial retinacular arthrotomy around patella
- Main Use
- Primary and revision TKA, joint access
- Main Risk
- Patellar tendon avulsion, patellar blood supply, arthrotomy closure failure.
- Plane or Release
- Split vastus medialis obliquus fibres then medial arthrotomy
- Main Use
- Selected primary TKA
- Main Risk
- Limited exposure, VMO injury or extension into quadriceps tendon.
- Plane or Release
- Lift vastus medialis from intermuscular septum without quadriceps tendon split
- Main Use
- Selected primary TKA with mobile patella
- Main Risk
- Difficult exposure in obese, muscular, stiff or revision knees.
- Plane or Release
- Between medial gastrocnemius and pes/hamstring region depending target
- Main Use
- Posteromedial tibial plateau and posterior medial corner
- Main Risk
- Saphenous nerve and vein, posterior capsule, popliteal structures if too deep.
- Plane or Release
- Between biceps femoris, lateral gastrocnemius, fibular head and PLC structures
- Main Use
- PLC reconstruction and posterolateral plateau
- Main Risk
- Common peroneal nerve.
If the approach moves behind the collateral ligament plane, ask where the popliteal vessels and named nerves are before retracting.
Patient Positioning
Position should give access, imaging, reduction control and bailout options. It is not an afterthought.
- Best For
- TKA, anterior knee, anterolateral plateau, many medial approaches
- Practical Checks
- Bump, leg holder, tourniquet, foot free, fluoroscopy if fracture fixation.
- Best For
- Posteromedial tibial plateau in selected cases
- Practical Checks
- Access to posterior medial tibia while preserving imaging and anterior access.
- Best For
- Selected posterolateral or lateral plateau work
- Practical Checks
- Pad peroneal nerve, protect dependent limb, confirm C-arm access.
- Best For
- Direct posterior or selected posterolateral reconstructions
- Practical Checks
- Airway, pressure areas, vascular access and fluoroscopy must be planned.
For fracture work, confirm AP and lateral imaging before prepping. A perfect approach with unusable fluoroscopy still fails the operation.
Surgical Technique
primary TKA, many revision TKAs, infection washout, extensile anterior joint access.
- Supine position, tourniquet if used, knee free to flex.
- Midline skin incision, respecting prior scars.
- Develop full-thickness flaps only as much as needed.
- Make medial parapatellar arthrotomy through quadriceps tendon, medial retinaculum and around patella.
- Protect patellar tendon insertion at the tibial tubercle.
- Evert or sublux patella according to exposure and extensor tension.
- Release medial sleeve only as needed for deformity correction or exposure.
- Close arthrotomy securely with knee flexion check.
high arthrotomy extension into quadriceps, patellar tendon avulsion, excessive medial stripping, patellar devascularisation and weak closure.
Extensile Exposure of the Difficult or Revision Knee
When a medial parapatellar arthrotomy will not safely deliver the patella in a stiff, ankylosed or revision knee, the answer is a stepwise extensile ladder - escalate only as far as exposure requires, because each step adds morbidity:
- What it is
- Oblique cut across the proximal quadriceps tendon at the apex of the medial parapatellar arthrotomy, angled superolaterally into vastus lateralis
- Best for
- First-line extension for most stiff or revision knees
- Main drawback
- Minimal - generally no change to rehabilitation and no significant extensor lag
- What it is
- Inverted-V cut turning the quadriceps tendon distally as a tongue, which also lengthens a contracted extensor mechanism
- Best for
- Severe extensor contracture or when lengthening is required
- Main drawback
- Risk of extensor lag and quadriceps weakness; slower, protected rehabilitation
- What it is
- Osteotomise the tubercle on a long lateral bone hinge, reflect the extensor mechanism, then reattach with screws or wires
- Best for
- Greatest distal exposure, patella baja, removal of a well-fixed tibial component
- Main drawback
- Adds an osteotomy to heal; serious complications in roughly 8 to 9 percent (proximal migration, avulsion, nonunion)
The principle is escalate, do not jump: try a snip first, reserve the V-Y turndown for a true extensor contracture, and reserve the TTO for when distal exposure or component removal demands it. All three are far safer than forcing patellar eversion and avulsing the patellar tendon.
Structures at Risk and Complications
- At Risk In
- Medial/lateral parapatellar, difficult TKA exposure
- Avoidance
- Avoid forceful eversion; protect tubercle insertion; extend approach rather than avulse tendon.
- At Risk In
- Extensive medial/lateral releases and revision surgery
- Avoidance
- Limit unnecessary retinacular stripping; preserve soft-tissue attachments.
- At Risk In
- Medial and posteromedial approaches
- Avoidance
- Identify, mobilise and protect; avoid blind medial dissection.
- At Risk In
- Posterolateral exposure and severe valgus correction
- Avoidance
- Identify around fibular neck; avoid traction; document baseline and postoperative function.
- At Risk In
- Multiple incisions, trauma, revision and infection
- Avoidance
- Respect skin bridges, prior scars and flap options.
- At Risk In
- Posterior capsule and posterior tibial plateau work
- Avoidance
- Know depth, use controlled retraction and avoid blind posterior penetration.
Extend when the target cannot be safely reached, the patella cannot be mobilised, reduction cannot be judged, or implant removal requires more access. Controlled extension is safer than force.
Stop and reassess when the skin is threatened, the nerve is not identified, the patellar tendon is under excessive tension, or fluoroscopy cannot show the target.
Guidelines, Registries and Global Practice
Surgical approaches around the knee are not country-specific, but the evidence and emphasis differ between major societies and between high- and limited-resource settings.
- Emphasis
- Column- and fragment-based approach selection for the proximal tibia.
- Practical Takeaway
- Map columns on CT; a posterior column fragment drives a posterior approach and buttress.
- Emphasis
- Soft-tissue-led timing and combined orthoplastic planning in open and high-energy injuries.
- Practical Takeaway
- Plan incisions around future flaps; do not commit to an approach that compromises later coverage.
- Emphasis
- Implant position, balancing and rehabilitation outweigh small approach differences in TKA.
- Practical Takeaway
- Choose the arthroplasty exposure you execute safely; optimise alignment and balance.
- Emphasis
- Anatomy-first exposure with nerve identification for posterolateral and complex knees.
- Practical Takeaway
- Identify the common peroneal nerve before posterolateral deep work.
Arthroplasty registries (NJR UK, AJRR US, AOANJRR Australia, the Swedish and Norwegian registers) track implant survival and revision rather than approach. Their consistent message is that component position and balance, not the specific anterior arthrotomy, dominate revision risk.
Knee osteoarthritis affects hundreds of millions worldwide and TKA volumes are rising fastest in ageing and middle-income populations. Tibial plateau fractures cluster bimodally: high-energy injuries in younger patients and fragility fractures in older adults.
Routine preoperative CT with 3D reconstruction, intraoperative fluoroscopy, navigation or robotics for arthroplasty, and ready access to ortho-plastic teams for soft-tissue cover.
Approach planning may rely on plain radiographs, so a disciplined clinical and radiographic read of fragment geometry, deliberate nerve identification and respect for the soft-tissue envelope become even more important.
Controversies and Areas of Uncertainty
Knee approaches generate persistent debate where the evidence is short-term, surgeon-dependent or based on small series.
- One View
- Muscle-sparing approaches speed early extensor recovery and reduce lateral releases.
- Other View
- Differences vanish by 3 to 6 months and exposure is harder in difficult knees.
- Current Position
- Reasonable in mobile, non-obese, non-revision knees; long-term outcomes are equivalent (PMID 23218628, 23790343).
- One View
- Eversion gives maximal exposure.
- Other View
- Eversion may stress the patellar tendon and extensor mechanism.
- Current Position
- Sublux where possible; never force eversion in a stiff knee.
- One View
- Anterolateral plate alone is less invasive.
- Other View
- Posterior coronal fragments lose reduction without a posterior buttress.
- Current Position
- CT fragment mapping decides; coronal posterior fragments need a posterior approach (PMID 20881634, 27178768).
- One View
- TTO gives excellent distal exposure and addresses patella baja.
- Other View
- TTO adds an osteotomy to heal with 8 to 9% serious complications.
- Current Position
- Snip first for proximal needs; reserve TTO for greater distal exposure or component removal (PMID 21329253).
- One View
- Direct posterolateral reaches the fragment but risks the peroneal nerve.
- Other View
- Extended anterolateral avoids the nerve but may not control posterior depression.
- Current Position
- Match exposure to fragment; identify the common peroneal nerve whenever working posterolaterally.

Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A patient requires revision TKA. The knee is stiff, the patella is difficult to mobilise and the previous incision is midline.”
“CT shows a coronal split posteromedial tibial plateau fragment with posterior displacement.”
“A young patient has a grade III posterolateral corner injury with a fibular collateral ligament avulsion requiring reconstruction. How do you approach the posterolateral knee safely?”
Opening structure
- State target pathology first.
- Then state position, landmarks, interval, danger structures and closure.
- Do not describe only the skin incision.
Anterior knee
- Medial parapatellar is reliable and extensile.
- Subvastus and midvastus are selected primary TKA options.
- Protect patellar tendon insertion and patellar blood supply.
Posteromedial
- Used for posteromedial tibial plateau and posterior medial corner access.
- Protect saphenous nerve and vein.
- Buttress posterior shear directly.
Posterolateral
- Used for PLC reconstruction and selected posterolateral plateau work.
- Identify common peroneal nerve around fibular neck.
- Avoid blind release or aggressive traction.
Failure modes
- Wrong approach for target.
- Patellar tendon avulsion.
- Skin bridge compromise.
- Saphenous or peroneal nerve injury.
- Poor closure of released structures.
Evidence Base
Every card below is anchored to a verified primary source. The pattern across knee-approach research is consistent: among the standard anterior arthroplasty exposures, differences are small and short-lived, whereas for trauma the approach must be dictated by fragment geometry on CT, and for the posterolateral corner the operation is governed by nerve anatomy.
Subvastus vs medial parapatellar: meta-analysis
- Nine trials, 940 primary TKAs pooled.
- Subvastus favoured for Knee Society function score at 4 to 6 weeks (WMD 5.09) and fewer lateral retinacular releases (OR 0.34).
- No difference in range of motion, operative time, blood loss, length of stay or complications.
Mini-midvastus vs mini-medial parapatellar RCT
- 40 patients with staged bilateral TKA, each patient acting as their own control (one approach per knee).
- Inconsistent clinical differences across timepoints to two years; no difference in operative time, blood loss or lateral releases.
- Authors recommend using the approach the surgeon knows best.
Tibial tubercle osteotomy for difficult exposure
- TTO is reproducible for enhancing exposure in difficult primary and revision TKA.
- Most common complications: proximal migration, osteotomy-site pain and tubercle avulsion.
- Serious TTO-related complications reported in roughly 8 to 9% of cases.