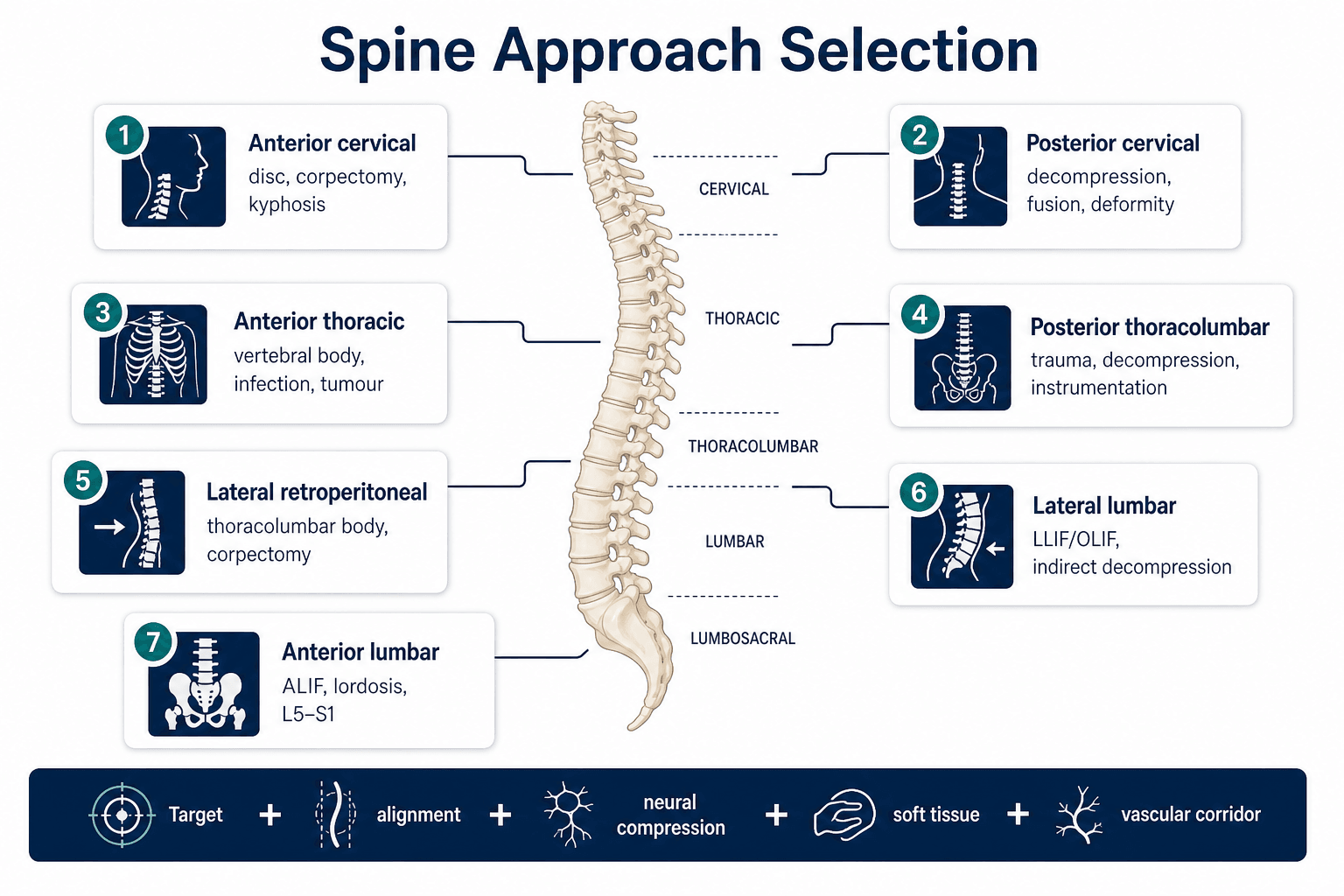
Choose the corridor that reaches the pathology without creating a new neurological, vascular or visceral problem
- The approach is chosen from pathology location, neural compression, alignment, reconstruction target and patient-specific risk.
- Anterior cervical exposure is not just an ACDF step: voice, swallowing, oesophageal, carotid, sympathetic and vertebral artery risks must be named.
- Posterior cervical fixation choice is a balance between bone purchase and neurovascular risk; lateral mass and pedicle screws are not interchangeable.
- Posterior thoracolumbar approaches are versatile, but anterior column failure, severe body loss or tumour may need anterior, lateral or combined access.
- ALIF, LLIF and OLIF are corridor-dependent procedures; the vascular, ureteric and lumbar plexus anatomy can make a technically attractive plan unsafe.
- “For myelopathy, the approach is determined by compression side, sagittal alignment, number of levels, instability and patient risk.
- “For thoracolumbar trauma, posterior fixation is common, but severe anterior column deficiency changes the reconstruction plan.
- “For ALIF, L5-S1 is often the most favourable level; higher levels require more vascular planning.
- “For LLIF, the lumbar plexus and psoas are the core hazard; for OLIF, the oblique corridor trades plexus risk for vascular and ureteric risk.
Surgical Approaches to the Cervical and Thoracolumbar Spine
Do not recite an incision first. State the pathology, level, compression side, alignment, reconstruction need, previous surgery, vascular corridor and neurological baseline before choosing the exposure.
- Useful Corridor
- Anterior cervical
- Why This Corridor
- Direct ventral decompression and anterior column reconstruction
- Main Risk
- Dysphagia, recurrent laryngeal nerve, oesophagus, carotid sheath, vertebral artery
- Useful Corridor
- Posterior cervical
- Why This Corridor
- Indirect decompression, fusion or laminoplasty across multiple levels
- Main Risk
- Cord, dura, C5 palsy, vertebral artery, axial neck pain
- Useful Corridor
- Posterior thoracolumbar
- Why This Corridor
- Fast stabilisation, decompression, reduction and instrumentation
- Main Risk
- Wrong level, dural injury, root injury, facet violation
- Useful Corridor
- Anterior thoracic or lateral retroperitoneal
- Why This Corridor
- Direct access to anterior column and body reconstruction
- Main Risk
- Pleura, diaphragm, segmental vessels, great vessels, visceral injury
- Useful Corridor
- ALIF
- Why This Corridor
- Large anterior cage, lordosis correction and posterior muscle preservation
- Main Risk
- Vascular injury, sympathetic plexus injury, ileus, retrograde ejaculation
- Useful Corridor
- LLIF or OLIF
- Why This Corridor
- Lateral or oblique anterior column access with indirect decompression
- Main Risk
- Lumbar plexus, psoas weakness, ureter, vessels, incomplete indirect decompression
TARGETApproach Selection
Hook:TARGET prevents incision-first thinking.
LEVELSpine Exposure Safety
Hook:LEVEL before decompression or instrumentation.
Overview and Indications
Spine approaches are best learned as clinical decisions rather than named incisions. The same pathology may be treated from different corridors depending on compression side, sagittal alignment, instability, previous surgery, infection, tumour, vascular anatomy and reconstruction goals.
For cervical disease, anterior exposure suits ventral disc, osteophyte, corpectomy and kyphosis correction. Posterior exposure suits multilevel posterior decompression, posterior fixation, deformity correction and cases where indirect decompression is safe because lordosis is preserved.
For thoracolumbar disease, posterior exposure is the workhorse for trauma, decompression and instrumentation. Anterior, lateral retroperitoneal or combined approaches are considered when the anterior column is the main pathology or reconstruction target. For lumbar degenerative and deformity surgery, ALIF, LLIF and OLIF are approach-dependent procedures where level and anatomy matter as much as the implant.
Ventral compression often favours anterior decompression. Posterior compression, multilevel stenosis with lordosis, or posterior instability may favour posterior exposure.
Kyphosis usually reduces the value of posterior-only indirect decompression and may require anterior release, anterior column reconstruction or combined correction.
The safest bony plan can be wrong if the vertebral artery, carotid sheath, great vessels, ureter, lumbar plexus or previous scar makes the corridor unsafe.
For cervical myelopathy, lumbar fusion, tumour and thoracolumbar trauma, the correct answer is not simply anterior or posterior. It is a reasoned choice based on compression, alignment, stability, reconstruction and patient risk.
Relevant Anatomy
The major danger structures change by region. A safe answer names them before describing the incision.
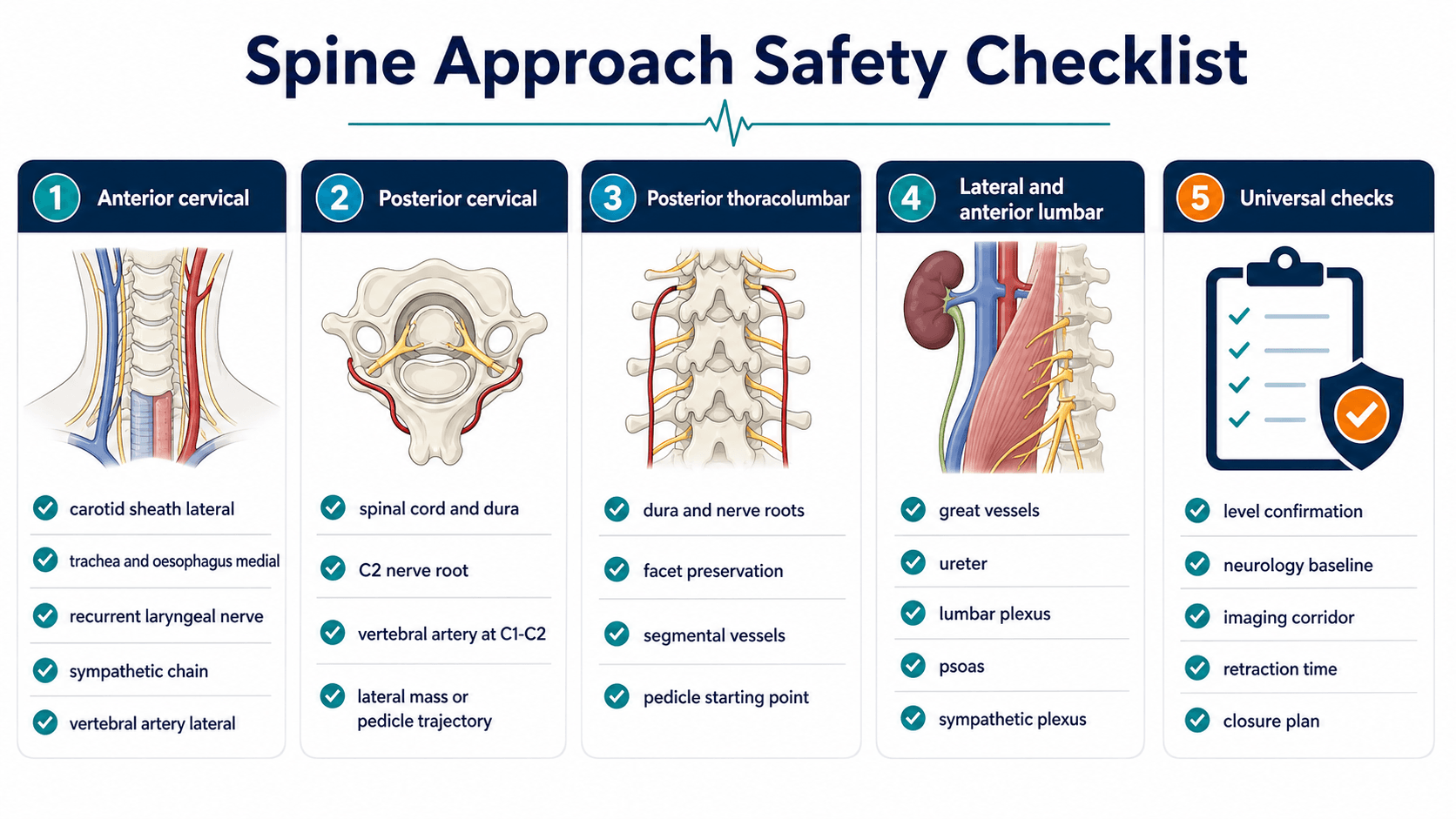
- Structures at Risk
- Carotid sheath, trachea, oesophagus, recurrent laryngeal nerve, superior laryngeal nerve, sympathetic chain, vertebral artery
- What the Surgeon Does
- Use the correct tissue plane, gentle retraction, longus colli elevation and strict midline disc/body work.
- Structures at Risk
- Cord, dura, nerve roots, vertebral artery, C2 nerve root, facet joints, posterior tension band
- What the Surgeon Does
- Maintain midline exposure, preserve facet capsules when not fusing, and choose screw trajectory from anatomy and imaging.
- Structures at Risk
- Dura, cauda equina, nerve roots, pedicles, facets, segmental vessels and paraspinal muscle
- What the Surgeon Does
- Confirm level, expose to required transverse process or facet target, and avoid unnecessary soft-tissue stripping.
- Structures at Risk
- Pleura, lung, diaphragm, aorta, vena cava, segmental vessels, thoracic duct and abdominal viscera
- What the Surgeon Does
- Plan level-specific access and vascular control; involve access specialists when needed.
- Structures at Risk
- Common iliac vessels, middle sacral vessels, ureter, hypogastric sympathetic plexus, bowel and lymphatics
- What the Surgeon Does
- Review vascular anatomy, mobilise vessels deliberately and avoid excessive plexus disruption.
- Structures at Risk
- Lumbar plexus, psoas, genitofemoral nerve, sympathetic chain, ureter, segmental vessels and great vessels
- What the Surgeon Does
- Use level-specific corridor planning, neuromonitoring when transpsoas, and avoid indirect decompression when fixed stenosis needs direct decompression.
Review CT, MRI and vascular imaging when the level, deformity, trauma, tumour or congenital anatomy could place the vertebral artery at risk. Unplanned vertebral artery injury is rare but potentially catastrophic.
Internervous Plane and Corridors
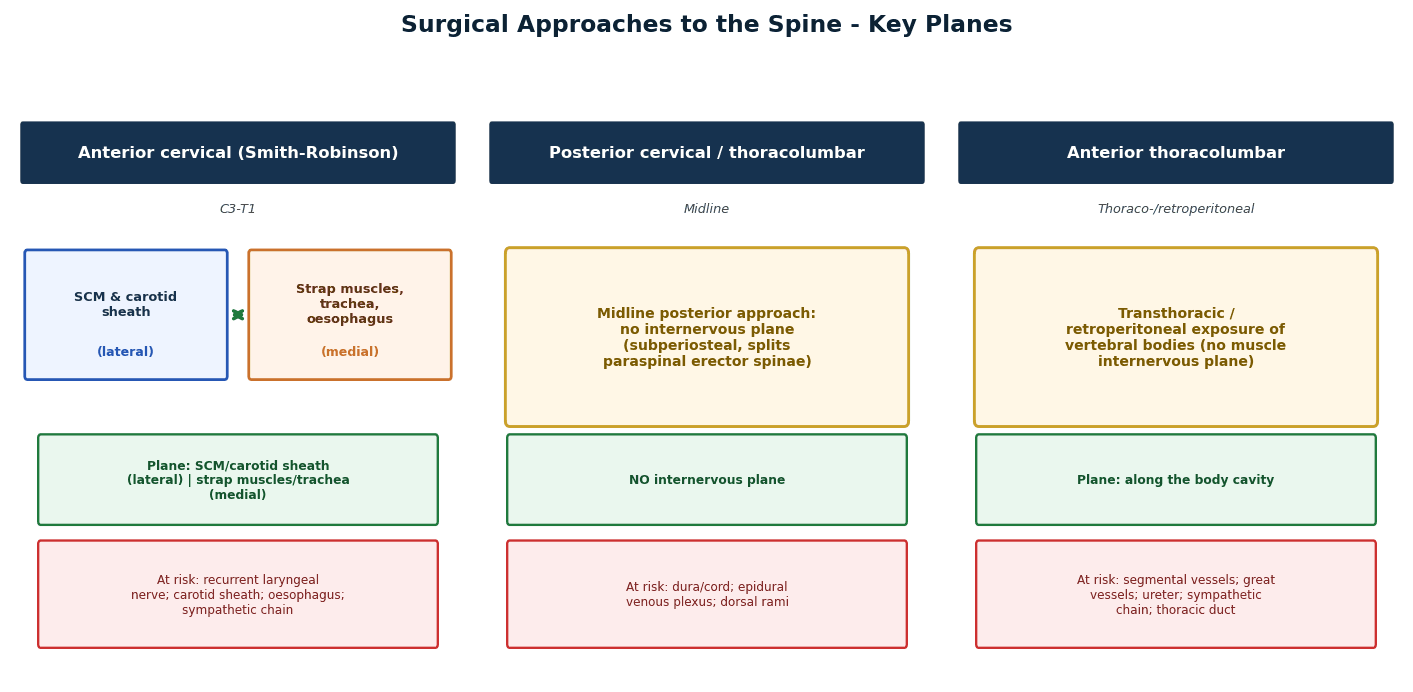
Spine approaches are not all true internervous planes. Many are corridor-based exposures through visceral, paraspinal, retroperitoneal or psoas-related pathways. The practical answer is to define the corridor, then name the neural and vascular structures that make it safe or unsafe.
- Plane or Corridor
- Between carotid sheath laterally and trachea/oesophagus medially
- Key Protection Point
- Protect recurrent laryngeal nerve, oesophagus, sympathetic chain and vertebral artery during lateral decompression.
- Plane or Corridor
- Midline posterior subperiosteal exposure to lamina, facets and lateral masses
- Key Protection Point
- No classic internervous plane; protect posterior tension band, facet capsules, cord, dura and vertebral artery.
- Plane or Corridor
- Midline posterior exposure through paraspinal muscle elevation
- Key Protection Point
- Protect dura and roots, preserve uninvolved facets and confirm pedicle starting points.
- Plane or Corridor
- Natural interval between multifidus and longissimus
- Key Protection Point
- Useful for far-lateral disc, posterolateral fusion or minimally invasive pedicle access while limiting midline muscle stripping.
- Plane or Corridor
- Thoracic, retropleural, retroperitoneal or thoracoabdominal corridor
- Key Protection Point
- Level determines pleura, diaphragm, segmental vessel and great-vessel handling.
- Plane or Corridor
- Anterior retroperitoneal corridor to disc space
- Key Protection Point
- Protect great vessels, ureter and sympathetic plexus.
- Plane or Corridor
- Lateral retroperitoneal transpsoas corridor
- Key Protection Point
- Lumbar plexus risk makes neuromonitoring, docking site and psoas retraction time critical.
- Plane or Corridor
- Oblique retroperitoneal corridor anterior to psoas
- Key Protection Point
- Avoids transpsoas plexus traversal but increases importance of ureter and vascular corridor planning.
When the exposure is not a clean internervous plane, say so. A strong answer describes the corridor, the target, and the danger structures that define the safe working zone.
Approach Selection Framework
Approach selection should be expressed as a decision sequence.
- If Yes
- Anterior cervical or anterior/lateral body access may be appropriate.
- If No
- Consider posterior decompression if dorsal compression, multilevel lordotic stenosis or posterior instability.
- If Yes
- Anterior, lateral or combined reconstruction may be needed.
- If No
- Posterior-only decompression or fixation may be adequate if alignment and stability are favourable.
- If Yes
- Plan corpectomy, anterior column reconstruction, lateral retroperitoneal access or combined fixation.
- If No
- Posterior fixation alone may be enough for many trauma patterns.
- If Yes
- Consider alternate side, alternate approach, access surgeon or staged plan.
- If No
- Proceed with normal corridor planning after imaging review.
- If Yes
- LLIF/OLIF/ALIF may restore height and alignment if stenosis is reducible.
- If No
- Use direct posterior decompression if fixed bony stenosis, severe lateral recess compression or locked deformity is present.
Lateral or anterior interbody fusion can restore height and tension ligaments, but it does not replace direct decompression when stenosis is fixed, severe, bony or clinically urgent.
Patient Positioning and Setup
Positioning must allow exposure, imaging, neuromonitoring and rescue. Confirm the level before incision and before irreversible bone removal or instrumentation.
- Position
- Supine, head neutral or slight extension
- Setup Priorities
- Shoulders taped if needed, image access, anterior neck landmarks, airway and voice risk documented.
- Position
- Prone or sitting in selected centres
- Setup Priorities
- Mayfield fixation, neutral alignment, eyes/pressure points, neuromonitoring, careful prone positioning in myelopathy.
- Position
- Prone on radiolucent table
- Setup Priorities
- Abdomen free, pressure protection, level localisation, AP and lateral imaging, neuromonitoring when indicated.
- Position
- Lateral decubitus or thoracoabdominal setup
- Setup Priorities
- Single-lung ventilation when needed, rib/diaphragm planning, vascular and pleural control.
- Position
- Supine
- Setup Priorities
- Left paramedian retroperitoneal exposure commonly used, vascular corridor reviewed, access support available when appropriate.
- Position
- Lateral decubitus
- Setup Priorities
- True lateral positioning, psoas and vessel corridor imaging, neuromonitoring for transpsoas exposure, table break when needed.
Use a repeatable level-confirmation routine: preoperative imaging review, radiopaque marker, intraoperative imaging before incision when needed, confirmation after exposure and confirmation before decompression or screw insertion.
Surgical Technique
Indications
- Ventral cervical disc herniation or osteophyte causing radiculopathy or myelopathy.
- Cervical corpectomy for retrovertebral compression.
- Anterior column reconstruction after trauma, infection, tumour or deformity.
- Focal kyphotic pathology where posterior decompression alone will not move the cord away from ventral compression.
Technique
- Position supine with the head supported and the neck neutral or gently extended.
- Mark the skin crease incision level using imaging, then confirm level with fluoroscopy.
- Incise skin and platysma; develop subplatysmal flaps as required.
- Identify the plane between the medial visceral structures and lateral carotid sheath.
- Retract trachea and oesophagus medially and carotid sheath laterally with gentle, time-aware retraction.
- Identify longus colli; elevate it subperiosteally from the vertebral bodies to seat retractors.
- Confirm the disc or vertebral level before discectomy, corpectomy or implant work.
- Keep decompression midline until the uncinate/foraminal target is deliberately approached.
- Protect endplates during preparation and avoid excessive lateral work near the vertebral artery.
- Close in layers after haemostasis, implant confirmation and assessment for oesophageal or airway concern.
Decision points
- Side choice depends on previous surgery, pathology side, surgeon familiarity and nerve risk. The recurrent laryngeal nerve course must be understood, especially in revision surgery.
- Multilevel anterior work increases dysphagia, pseudarthrosis and implant risks; posterior or combined strategies may be better for some patients.
- Revision anterior cervical surgery has higher scar and recurrent laryngeal nerve risk; preoperative laryngoscopy is useful when prior anterior neck surgery or voice symptoms exist.
Structures at Risk and Pitfalls
- Why It Matters
- Wrong-level surgery is a preventable catastrophic error.
- Prevention
- Use a documented level-confirmation routine and repeat before irreversible work.
- Why It Matters
- Dysphagia, voice change, airway swelling and oesophageal injury can follow excessive retraction.
- Prevention
- Use gentle retraction, release intermittently and minimise time.
- Why It Matters
- Vertebral artery injury may cause major bleeding, stroke, pseudoaneurysm or need for endovascular control.
- Prevention
- Review anatomy, keep decompression controlled and have a haemorrhage plan.
- Why It Matters
- Adjacent segment pain, instability or unintended fusion extension may result.
- Prevention
- Expose and instrument only the planned levels; preserve adjacent capsules.
- Why It Matters
- The patient may remain compressed despite a technically good cage.
- Prevention
- Assess stenosis type and plan direct decompression when needed.
- Why It Matters
- Venous laceration, arterial injury, thrombosis or access failure can occur.
- Prevention
- Review vascular corridor and involve access expertise when appropriate.
- Why It Matters
- Lumbar plexus injury, thigh pain, sensory symptoms or hip flexor weakness may occur.
- Prevention
- Use level-specific docking, stimulation thresholds and minimise psoas retraction time.
After anterior cervical surgery, dysphagia and voice change are not minor administrative issues. They reflect the anatomy of the exposure and should be anticipated, documented, investigated when persistent and explained during consent.
Closure and Postoperative Care
Closure is part of the approach. The spine wound may fail because of tension, dead space, infection, radiation, obesity, diabetes, long constructs or poor muscle coverage.
- Immediate Checks
- Airway, voice, swallow, haematoma, neurological status
- Specific Concerns
- Expanding neck haematoma is an emergency; persistent dysphagia or suspected oesophageal injury needs urgent assessment.
- Immediate Checks
- Cord/nerve status, C5 function, wound drain, alignment
- Specific Concerns
- C5 palsy, axial pain, wound problems and junctional failure.
- Immediate Checks
- Neurology, screw position concern, wound, ileus/pain
- Specific Concerns
- Dural leak, root deficit, infection, implant failure and junctional problems.
- Immediate Checks
- Respiratory status, chest drainage, neurology, haemodynamics
- Specific Concerns
- Pleural complication, pulmonary morbidity, vascular issue, visceral injury.
- Immediate Checks
- Vascular status, abdominal exam, ileus, neurological status
- Specific Concerns
- Vascular thrombosis/laceration, retrograde ejaculation, ileus, lymphocele.
- Immediate Checks
- Hip flexion strength, thigh sensation, abdominal wall, neurology
- Specific Concerns
- Psoas weakness, lumbar plexus symptoms, pseudohernia, vascular or ureteric injury.
Choosing Between Competing Corridors
For most spine pathologies, more than one approach is technically possible. The exam-relevant skill is to compare the realistic alternatives for a single indication and justify the choice from compression, alignment, stability, reconstruction and risk, not from familiarity.
- Option A
- Anterior cervical discectomy and fusion
- Option B
- Posterior laminoplasty or laminectomy and fusion
- What Tips the Decision
- Focal ventral compression and preserved lordosis favour anterior; multilevel posterior compression with good lordosis favours posterior.
- Option A
- Anterior corpectomy and reconstruction
- Option B
- Posterior decompression and fusion alone
- What Tips the Decision
- Fixed kyphosis reduces posterior cord drift, so anterior or combined correction is often needed.
- Option A
- Posterior instrumented stabilisation and decompression
- Option B
- Anterior or lateral corpectomy and reconstruction
- What Tips the Decision
- Posterior-only is adequate for many patterns; severe anterior column loss or progressive kyphosis favours anterior or combined work.
- Option A
- Anterior lumbar interbody fusion
- Option B
- Transforaminal or posterior lumbar interbody fusion
- What Tips the Decision
- ALIF gives larger cage and better lordosis but needs vascular planning; posterior interbody allows direct decompression if fixed stenosis is present.
- Option A
- Lateral transpsoas interbody fusion
- Option B
- Oblique anterior-to-psoas interbody fusion
- What Tips the Decision
- Transpsoas carries lumbar plexus risk; oblique avoids the plexus but raises ureteric and vascular planning importance.
A consultant-level answer names the competing corridor and explains why it was not chosen. Saying only what you would do, without comparing the alternative, sounds rehearsed rather than reasoned.
Guidelines, Registries & Global Practice
Spine approach selection is a worldwide decision informed by global epidemiology, society guidance and registry-style cohort data rather than any single national framework.
- Figure
- Most common cause of spinal cord dysfunction worldwide
- Relevance to Approach
- Drives the high global volume of anterior and posterior cervical decompression.
- Figure
- 479 patients, 16 sites, mJOA 12.50 to 14.90 at 24 months, 3.13% neurological complication rate
- Relevance to Approach
- Confirms decompression is safe and effective across health systems.
- Figure
- Around 5% pooled, higher early and with multilevel surgery
- Relevance to Approach
- A core anterior-corridor consent and counselling point everywhere.
- Figure
- Approximately 8 per 10,000 cervical procedures (AOSpine North America)
- Relevance to Approach
- Rare but catastrophic; planning structure for high-risk exposure globally.
- Emphasis Relevant to Approach
- Approach selection by compression pattern, alignment and stability; structured trauma and CSM classification
- Practical Message
- Match the corridor to the pathology, alignment and instability rather than to a default exposure.
- Emphasis Relevant to Approach
- Evidence-based CSM and degenerative lumbar guidance; appropriate use of fusion and decompression
- Practical Message
- Reserve fusion and interbody work for clear instability, deformity or reconstruction needs.
- Emphasis Relevant to Approach
- Timely decompression for myelopathy and cauda equina; judicious lumbar fusion
- Practical Message
- Prioritise neurological protection and avoid unnecessary instrumentation.
- Emphasis Relevant to Approach
- Standardised training in anterior, posterior and minimally invasive corridors
- Practical Message
- Corridor competence and access support should match the planned approach complexity.
- Well-Resourced Setting
- CT, MRI and CT angiography for vertebral artery and vascular corridor
- Limited-Resource Setting
- May rely on plain films and limited cross-sectional imaging, increasing reliance on anatomical knowledge.
- Well-Resourced Setting
- Neuromonitoring, navigation and intraoperative imaging widely available
- Limited-Resource Setting
- Freehand technique and fluoroscopy more common; meticulous landmarks are essential.
- Well-Resourced Setting
- Vascular and thoracic access surgeons available for high-risk anterior corridors
- Limited-Resource Setting
- Spine surgeon may perform access alone, favouring familiar and lower-risk corridors.
- Well-Resourced Setting
- Full range of cages, plates and expandable reconstruction options
- Limited-Resource Setting
- Implant choice may constrain whether anterior column reconstruction is feasible.
Registry-style cohorts from North America, Europe and Asia describe the same procedures; quote them as evidence for a worldwide approach decision rather than as country-specific practice.
Controversies and Areas of Uncertainty
Approach selection in spine surgery is genuinely contested in several areas. Naming the controversy and the evidence around it is high-yield.
For multilevel myelopathy with preserved lordosis, anterior and posterior strategies can give equivalent adjusted outcomes, but anterior multilevel constructs raise dysphagia and pseudarthrosis risk while posterior fusion raises C5 palsy and axial pain risk. The choice remains individualised rather than settled.
Laminoplasty preserves motion and may reduce fusion-related morbidity, but fusion may be preferred when there is kyphosis, instability, axial pain or significant facet pathology. There is no universal winner.
Pedicle screws give stronger purchase and, with navigation, may reduce overall complications, but they demand stricter trajectory control near the vertebral artery and nerve roots. Lateral mass screws remain the familiar default in the subaxial spine.
Lateral and anterior interbody fusion can decompress indirectly by restoring height and tensioning ligaments, but fixed bony stenosis, severe lateral recess compression or ossified pathology may still need direct posterior decompression. Predicting which patients respond to indirect decompression is imperfect.
If asked about laminoplasty versus fusion, transpsoas versus oblique, or pedicle versus lateral mass screws, acknowledge the genuine uncertainty and frame your answer around patient-specific factors and the available evidence.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A patient has multilevel cervical myelopathy from C4-C7. MRI shows ventral osteophytes, preserved lordosis and no fixed kyphosis. You are asked how you choose anterior versus posterior surgery.”
“A patient has a thoracolumbar burst fracture with posterior ligamentous complex injury and incomplete neurological deficit.”
“A patient has symptomatic L5-S1 disc collapse with foraminal stenosis and sagittal correction need. You are asked whether ALIF is appropriate.”
“A patient develops thigh numbness and hip flexor weakness after LLIF. Explain the likely approach-related issue and prevention.”
Opening Line
- I choose the spine approach from compression side, alignment, stability, reconstruction target, previous surgery, vascular corridor and neurological baseline.
- The incision is not the first decision; the target and risk corridor are.
Cervical
- Anterior cervical: direct ventral decompression; risks include dysphagia, recurrent laryngeal nerve, oesophagus, carotid sheath, sympathetic chain and vertebral artery.
- Posterior cervical: multilevel decompression/fusion; risks include cord, dura, C5 palsy, vertebral artery and screw trajectory complications.
- Kyphosis weakens posterior-only indirect decompression.
Thoracolumbar
- Posterior thoracolumbar approach is the trauma workhorse for fixation, reduction and decompression.
- Severe anterior column loss, tumour, infection or corpectomy target may need anterior, lateral or combined access.
- Wrong-level prevention must be explicit.
Lumbar Anterior and Lateral
- ALIF: strong for L5-S1 height and lordosis; vascular and sympathetic risks dominate.
- LLIF: transpsoas corridor; lumbar plexus and psoas symptoms dominate.
- OLIF: anterior-to-psoas corridor; vascular and ureteric planning dominate.
- Indirect decompression only works when stenosis is reducible.
Evidence Base
Anterior Versus Posterior Approach in Cervical Spondylotic Myelopathy: AOSpine North America
- Approach selection in practice tracks age, severity, focality and alignment, not surgeon preference alone.
- Anterior and posterior surgery have equivalent adjusted efficacy for CSM.
- Neck Disability Index and SF-36 improvements did not differ between approaches.