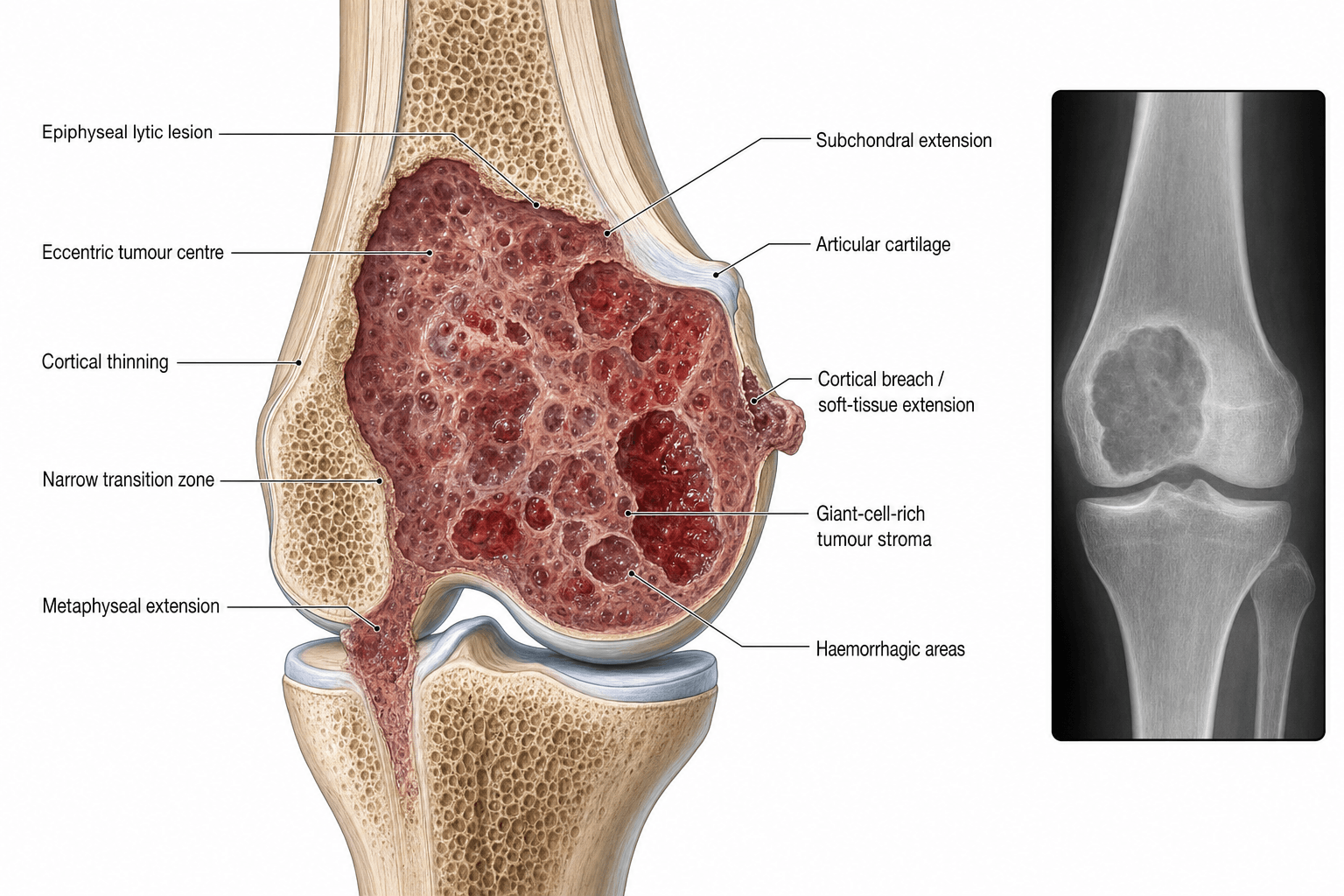
Epiphyseal Lytic Lesion | RANKL-Driven | Campanacci Classification | Extended Curettage
- Epiphyseal/metaphyseal lytic lesion abutting subchondral bone in skeletally mature patient
- Driven by RANKL overexpression from neoplastic stromal cells recruiting osteoclast-like giant cells
- Extended curettage with high-speed burr and adjuvants is gold standard for operable tumours
- Denosumab (RANKL inhibitor) for unresectable, recurrent, or metastatic disease
- Lung metastases occur in 1-3 percent but are typically indolent and amenable to resection
- “Think GCT in any lytic epiphyseal lesion in a 20-40 year old
- “Subchondral location (abuts joint surface) is characteristic
- “Campanacci grade determines surgical vs medical management
- “Giant cells are REACTIVE (osteoclasts), not neoplastic
- “Always rule out brown tumour of hyperparathyroidism in differential
Clinical Imaging
Giant Cell Tumour Radiographic Features
Imaging is discussed in the Investigations section below. Key plain film features include a purely lytic, eccentric, metaepiphyseal lesion with non-sclerotic margins abutting the subchondral bone plate. No periosteal reaction unless fracture present. No matrix mineralisation or sclerotic rim.
Metaepiphyseal, abutting subchondral bone. Occurs in skeletally mature individuals after physeal closure. Distal femur and proximal tibia account for approximately 50 percent of cases. Sacrum is the most common axial site.
Neoplastic stromal cells overexpress RANKL, recruiting reactive osteoclast-like multinucleated giant cells. The giant cells are NOT the tumour — the mononuclear stromal cell is the true neoplastic component.
Grade I = well-defined, intact cortex (latent). Grade II = expanded cortex, still contained (active). Grade III = cortical breakthrough with soft tissue mass (aggressive). Grade determines surgical approach.
Extended intralesional curettage with high-speed burr and adjuvants (phenol, cryotherapy, or cement) for operable lesions. Denosumab for unresectable, sacral, or metastatic disease. Wide resection for recurrent Grade III.
| Presentation | Diagnosis | Treatment | Key Pearl |
|---|---|---|---|
| Lytic epiphyseal lesion, 20-40 yr old | Campanacci Grade I-II, biopsy confirmed | Extended curettage + bone graft or cement | Subchondral location is the hallmark |
| Aggressive cortical breakthrough | Campanacci Grade III with soft tissue mass | Wide resection and reconstruction vs denosumab | MRI essential for soft tissue extent |
| Sacral or spinal GCT, unresectable | CT-guided biopsy, RANKL confirmation | Denosumab first line (long-term) | Monitor for hypercalcaemia on cessation |
CELLSGCT Location and Demographics
Hook:CELLS = Closed physes, Epiphyseal, Lytic, Lower femur/upper tibia, Sacrum for GCT!
ICECampanacci Classification
Hook:ICE = Intact, Cortex expanded, Extraosseous — the Campanacci grades in order!
CREAMTreatment Options for GCT
Hook:CREAM = Curettage, Resection, Embolisation, Adjuvants, Medical therapy — the 5 pillars of GCT treatment!
Overview and Epidemiology
Giant cell tumour of bone (GCTB) is the most common aggressive benign bone tumour in young adults. It is locally aggressive with high recurrence rates and a small but real risk of benign lung metastasis. Understanding the RANKL pathway has revolutionised management with denosumab, making this tumour a model for targeted therapy in musculoskeletal oncology. It is a high-yield exam topic across FRACS, FRCS, and ABOS.
- Incidence: 5-8 percent of all primary bone tumours
- Age: Peak 20-40 years; rare in skeletally immature
- Sex: Slight female predominance (approximately 55-60%)
- Sites: Distal femur (25-30%), proximal tibia (20-25%), distal radius (10-15%), sacrum (5-10%)
- Rare in: Hands, feet, and spine below sacrum
- Local aggressiveness: Destroys bone, threatens joint, pathologic fracture risk
- Recurrence: 15-25 percent after extended curettage, up to 50 percent after simple curettage
- Lung metastasis: 1-3 percent — histologically benign but can be progressive
- Joint compromise: Subchondral location threatens articular cartilage and joint function
- Malignant transformation: Less than 1 percent (usually radiation-associated)
Pathophysiology
GCTB is unique among bone tumours because its pathogenesis is driven by a well-characterised molecular pathway. The neoplastic mononuclear stromal cells (the true tumour cells) overexpress RANKL (Receptor Activator of Nuclear Factor Kappa-B Ligand) on their surface. This binds to RANK receptors on osteoclast precursors, driving their fusion into multinucleated osteoclast-like giant cells. These giant cells are REACTIVE (not neoplastic) and are responsible for the aggressive bone resorption that characterises GCTB. This RANKL-RANK interaction is the therapeutic target of denosumab.
| Cell Type | Origin | Role | Neoplastic? |
|---|---|---|---|
| Mononuclear stromal cells | Mesenchymal origin | True tumour cell, overexpresses RANKL | Yes — the neoplastic component |
| Multinucleated giant cells | Osteoclast lineage (reactive) | Bone resorption via RANKL stimulation | No — reactive, recruited by stromal cells |
| Mononuclear histiocytes | Macrophage/monocyte lineage | Supportive inflammatory component | No — reactive, recruited population |
RANKL expressed by neoplastic stromal cells binds RANK on osteoclast precursors, driving osteoclastogenesis. Normal osteoprotegerin (OPG) acts as a decoy receptor, but in GCTB the RANKL excess overwhelms OPG. Denosumab is a monoclonal antibody that mimics OPG by binding RANKL, blocking osteoclast activation and giant cell formation.
In skeletally immature patients, the physis acts as a barrier. GCTB arises in the metaphysis and extends to the epiphysis only after physeal closure. This explains why GCTB is virtually always metaepiphyseal in adults and rare before skeletal maturity. The subchondral extension is due to the rich vascular supply of the subchondral bone plate.
Classification and Types
Campanacci Radiographic Classification
| Grade | Radiographic Features | Clinical Behaviour | Typical Treatment |
|---|---|---|---|
| Grade I (Latent) | Well-defined margins, intact cortex, may have thin sclerotic rim | Slow growth, minimal symptoms, low recurrence risk | Extended curettage with adjuvant and bone graft or cement |
| Grade II (Active) | Ill-defined margins, expanded but intact cortex, no soft tissue mass | Progressive symptoms, moderate recurrence risk after curettage | Extended curettage with adjuvant (phenol/cryo/cement) |
| Grade III (Aggressive) | Cortical destruction, soft tissue mass, aggressive permeative pattern | Rapid growth, high recurrence, pathologic fracture risk | Wide resection and reconstruction, or denosumab plus curettage |
Campanacci grade correlates with local recurrence risk and guides the balance between joint-preserving intralesional surgery and wide resection.
Clinical Assessment
- Age: 20-40 years (classic demographic)
- Pain: Deep, aching, progressive, worse with weight-bearing
- Swelling: May be palpable if superficial bone (tibia, radius)
- Joint symptoms: Stiffness or reduced range if subchondral extension
- Pathologic fracture: Up to 10-15 percent present with fracture through weakened cortex
- Inspect: Swelling, deformity if fracture, overlying skin changes
- Palpate: Tender over involved bone, possible palpable mass
- Range of motion: Assess adjacent joint — subchondral involvement may limit motion
- Neurovascular: Distal neurovascular status, especially with sacral or vertebral GCTB
- Lung auscultation: Baseline assessment (lung mets rare but possible)
Never proceed to definitive surgery based on imaging alone. An image-guided core needle biopsy (under CT or fluoroscopy) must confirm the diagnosis before curettage or resection. The biopsy tract must be placed in a position that can be excised if wide resection is ultimately required. Trocar biopsy is preferred over fine needle aspiration for adequate tissue.
Differential diagnosis of a lytic epiphyseal lesion includes:
- Chondroblastoma (younger patient, sclerotic rim, calcifications)
- Aneurysmal bone cyst (younger, more metaphyseal, fluid-fluid levels)
- Brown tumour of hyperparathyroidism (check calcium and PTH)
- Clear cell chondrosarcoma (older patient, femoral head)
- Metastasis or myeloma (older patient, different demographics)
- Infection or Brodies abscess (usually metaphyseal, sclerotic rim)
| Condition | Age | Key Radiographic Feature | Discriminator |
|---|---|---|---|
| GCT of bone | 20-40 years | Lytic, metaepiphyseal, abuts subchondral plate, no matrix | Skeletally mature, purely lytic, no sclerotic rim |
| Chondroblastoma | 10-20 years | Epiphyseal, sclerotic rim, may have chondroid calcification | Skeletally immature, open physis, chondroid matrix |
| Aneurysmal bone cyst | 10-20 years | Metaphyseal, expansile, fluid-fluid levels on MRI | Younger age, blood-filled cavities, no giant cell stroma |
| Brown tumour (hyperparathyroidism) | Any age | Lytic, may be multiple, subperiosteal resorption elsewhere | Elevated calcium, elevated PTH, multilocular, multiple lesions |
| Clear cell chondrosarcoma | 30-50 years | Epiphyseal (femoral head), may calcify | Older patient, slower growth, histological clear cells |
| Giant cell-rich osteosarcoma | 15-30 years | Aggressive lytic lesion, may have mineralised matrix | Atypical mitoses, malignant osteoid, aggressive features |
Always check serum calcium and PTH in any patient with a lytic bone lesion that could be a GCT — brown tumour of hyperparathyroidism is the classic mimic and is treated medically, not surgically. This is a perennial exam favourite.
Investigations
Investigation Protocol
Views: PA and lateral of the affected bone, include adjacent joint
Classic features: Purely lytic, eccentric, metaepiphyseal lesion with non-sclerotic margins, abutting subchondral bone. Cortex may be thinned, expanded, or breached. No matrix mineralisation. No periosteal reaction unless fractured.
Campanacci grade is assessed on plain radiographs primarily.
Sequences: T1, T2, STIR, and T1 post-gadolinium
Findings: Low-to-intermediate T1 signal, heterogeneous high T2 signal. Defines soft tissue extension, joint involvement, and relationship to neurovascular structures. Fluid-fluid levels suggest secondary ABC change.
Critical for surgical planning: Marrow extent, soft tissue mass, articular cartilage integrity.
Indication: Assess cortical integrity, thin-section detail of bone destruction, and guide biopsy
Chest CT: Baseline staging for lung metastasis (1-3 percent risk)
CT-guided biopsy: Preferred technique for tissue diagnosis with trocar approach
Serum calcium and PTH: Rule out brown tumour of hyperparathyroidism (essential differential)
Alkaline phosphatase: May be elevated with extensive bone destruction
Renal function: Baseline before denosumab if medical therapy contemplated
The key radiographic triad for GCTB is: (1) lytic lesion, (2) metaepiphyseal location abutting subchondral bone, (3) skeletally mature patient age 20-40. If all three are present, GCTB is the leading diagnosis — but biopsy is always mandatory before definitive treatment. Do not confuse the non-sclerotic margin of GCTB with the sclerotic rim typical of benign lesions like chondroblastoma or ABC.
Management Algorithm
Extended Intralesional Curettage (Gold Standard)
Goal: Complete tumour removal while preserving the adjacent joint and limb function
Surgical Protocol
Approach: Direct approach to the tumour through a large cortical window (must be adequately sized for visualisation). Avoid neurovascular structures.
Window: Must be large enough for complete visualisation and instrumentation — a small window leads to inadequate curettage and higher recurrence.
Mechanical: Thorough curettage with large and small curettes, extending to healthy bone margins in all directions
High-speed burr: Burr all walls of the cavity to remove tumour extending into bony crevices — this is the key step that distinguishes extended from simple curettage
Phenol: Apply 5 percent phenol to cavity walls for chemical necrosis of residual tumour cells, followed by alcohol rinse
Cryotherapy: Liquid nitrogen for thermal necrosis (risk of fracture, skin necrosis)
Zinc chloride or hydrogen peroxide: Alternative chemical adjuvants
PMMA cement: Provides both structural support and thermal/chemical kill of residual cells (exothermic reaction)
Cement (PMMA): Preferred for immediate structural stability and adjuvant effect. Subchondral bone graft between cement and articular cartilage is recommended to protect the joint surface.
Bone graft: Allograft or autograft for smaller defects where joint preservation is paramount.
Augmentation: Plates, screws, or intramedullary device if structural integrity is compromised (especially after burring of extensive cortex)
The difference between simple curettage (recurrence rate approaching 50 percent) and extended curettage (recurrence rate 15-25 percent) is: (1) a large enough cortical window for adequate exposure, (2) thorough use of a high-speed burr on all cavity walls, and (3) application of a local adjuvant. These three steps must be emphasised in any exam answer on GCT surgery.
Complications
| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| Local recurrence | 15-25% after extended curettage | Inadequate margins, no adjuvant use, Campanacci Grade III | Re-curettage or wide resection depending on extent |
| Pathologic fracture | 10-15% at presentation, additional risk post-curettage | Large lesion, cortical breach, weight-bearing bone | Internal fixation and cement at time of curettage; or staged approach |
| Lung metastasis (benign) | 1-3% of patients | Campanacci Grade III, local recurrence, distal radial location | Observation if stable; wedge resection if progressive or symptomatic |
| Joint degeneration | Variable, related to subchondral involvement | Large tumour, inadequate subchondral bone graft | Joint preservation vs arthroplasty depending on age and extent |
| Malignant transformation | Less than 1% | Prior radiation therapy to the site | Treat as high-grade sarcoma — wide resection and oncologic management |
| Post-curettage fracture | 5-10% after cryotherapy or extensive burring | Large cortical window, cryotherapy use, weight-bearing site | Prophylactic fixation at index surgery reduces risk |
Lung metastases from GCTB are histologically benign (identical to the primary tumour) but can be progressive. They typically present within 3 years of the primary diagnosis. Risk factors include local recurrence, Campanacci Grade III, and distal radial location. Management ranges from observation (if stable and asymptomatic) to wedge resection (if progressive). Denosumab has shown efficacy in controlling pulmonary metastases. Chest CT at diagnosis and during follow-up is recommended.
Outcomes and Prognosis
| Treatment | Local Recurrence | Joint Preservation | Functional Outcome |
|---|---|---|---|
| Extended curettage + adjuvant | 15-25% | High (approximately 80-90%) | Good to excellent in most cases |
| Simple curettage (no adjuvant) | 40-55% | High initially but decreases with recurrence | Functional but high re-operation rate |
| Wide resection | Less than 10% | Lost — requires reconstruction | Dependent on reconstruction type |
| Denosumab (unresectable) | Tumour control in 80-90% while on therapy | Variable — may allow delayed surgery | Good disease control but long-term therapy needed |
Favourable prognosis: Campanacci Grade I-II, primary tumour (no prior surgery), adequate extended curettage with adjuvant, distal femur or proximal tibia (accessible surgical site)
Poor prognosis factors: Campanacci Grade III, recurrent tumour (especially after multiple prior surgeries), sacral or spinal location, pathologic fracture, young age (less than 25 years)
Follow-up protocol: Radiographs of primary site every 3-6 months for 2 years, then 6-12 months to 5 years, then annually. Chest imaging (CT or radiograph) at baseline and during follow-up for lung metastasis surveillance.
Evidence Base and Key Trials
Giant-cell tumor of bone
- Landmark series defining the Campanacci radiographic classification (Grades I-III) for GCTB
- Established correlation between radiographic grade and local recurrence risk
- Reported outcomes for curettage versus resection in a large series of patients
- Showed that surgical margins and adjuvant use significantly impact recurrence rates
Denosumab in treatment of giant cell tumour of bone: results of a phase 2 study
- Phase 2 trial of denosumab (anti-RANKL monoclonal antibody) in patients with unresectable or metastatic GCTB
- Demonstrated tumour response (elimination or marked reduction of giant cells) in 86% of patients
- Clinical benefit with pain reduction and functional improvement in the majority of treated patients
- Established the RANKL pathway as a validated therapeutic target in GCTB
Safety and efficacy of denosumab for adults and skeletally mature adolescents with giant cell tumour of bone: interim analysis of an open-label, parallel-group, phase 2 study
- Larger phase 2 study confirming denosumab efficacy in both operable and unresectable GCTB
- Disease stability or response in approximately 96% of unresectable patients at median follow-up
- Tumour response included new bone formation and decreased giant cell infiltration on histology
- Acceptable safety profile with hypocalcaemia as the most notable adverse effect
Giant cell tumor of long bone: a Canadian Sarcoma Group study
- Multi-institutional review of patients with GCTB of long bones treated with intralesional surgery
- Local recurrence rate of approximately 22% after extended curettage with adjuvant therapy
- Use of high-speed burr and cement reduced recurrence compared with simple curettage
- Identified Campanacci Grade III and subchondral involvement as risk factors for recurrence
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old woman presents with progressive right knee pain for 6 months, worse with weight-bearing. Plain radiographs show a purely lytic lesion in the distal femoral metaepiphysis abutting the subchondral bone plate, with thinned but intact cortex and no matrix mineralisation. The lesion measures approximately 5 cm. What is your diagnosis, investigations, and management plan?”
“A 38-year-old man presents with progressive low back and left leg pain with radiculopathy. MRI reveals a large destructive lytic lesion involving the sacrum from S1 to S3 with soft tissue extension and nerve root encroachment. CT-guided biopsy confirms giant cell tumour of bone. The tumour is deemed unresectable due to sacral nerve root involvement and proximity to the thecal sac. How would you manage this patient?”
MCQ Practice Points
Q: What is the most common site for giant cell tumour of bone? A: Around the knee — distal femur (25-30%) and proximal tibia (20-25%) together account for approximately 50% of all GCTs. The distal radius is the third most common site (10-15%). The sacrum is the most common axial location.
Q: Which cell is the true neoplastic component in GCTB? A: The mononuclear stromal cell, NOT the multinucleated giant cell. The giant cells are reactive osteoclasts recruited via RANKL overexpression by the neoplastic stromal cells. Understanding this is essential because denosumab targets RANKL (produced by stromal cells) to eliminate the reactive giant cells.
Q: Describe the Campanacci classification for GCTB. A: Grade I (latent): well-defined, intact cortex, may have sclerotic rim. Grade II (active): cortex thinned and expanded but intact, no soft tissue mass. Grade III (aggressive): cortical breakthrough with soft tissue extension. Grade guides surgical decision-making — higher grades may require wide resection rather than joint-preserving curettage.
Q: What surgical technique reduces GCT recurrence from approximately 50% to approximately 15-25%? A: Extended curettage — specifically: (1) an adequately large cortical window, (2) thorough curettage with high-speed burr on all cavity walls, and (3) application of a local adjuvant (phenol, cryotherapy, or PMMA cement). Simple curettage without these steps has recurrence rates approaching 50%.
Q: What is the significance of lung metastases in GCTB? A: Lung metastases occur in 1-3% of GCTB patients and are histologically benign (identical to the primary tumour). They can be progressive and symptomatic but are not true malignant transformation. Management ranges from observation (if stable) to wedge resection (if progressive). Denosumab has shown efficacy in controlling pulmonary disease. Risk factors include Campanacci Grade III, local recurrence, and distal radial location.
Q: What condition must be excluded before treating a lytic epiphyseal lesion as GCTB? A: Brown tumour of hyperparathyroidism. Both conditions produce lytic bone lesions with giant cells on histology. Check serum calcium and PTH — if both are elevated, the diagnosis is hyperparathyroidism (treated medically or with parathyroid surgery), not GCTB.
Guidelines, Registries & Global Practice
- GCTB incidence is similar worldwide: 5-8% of primary bone tumours across all populations studied
- Peak age consistently 20-40 years across ethnic groups with slight female predominance
- Geographic variation: Higher proportion of sacral and spinal GCTB reported in some Asian series, though whether this reflects true incidence or referral bias is debated
- Lung metastasis rate of 1-3% reported consistently across international cohorts
- High-resource: MRI staging, extended curettage with high-speed burr and adjuvants, denosumab for unresectable disease, chest CT surveillance
- Limited-resource: Plain radiograph-based Campanacci grading, curettage (adjuvant use variable), denosumab access may be limited by cost
- Universal principle: Biopsy before definitive surgery is mandatory regardless of setting
- Denosumab availability: Regulatory approval and funding varies significantly between countries — access remains a global inequity issue
| Source | Surgical Approach | Medical Therapy | Surveillance |
|---|---|---|---|
| NCCN / AO (international oncology guidelines) | Extended curettage with adjuvant for operable; wide resection for recurrent Grade III | Denosumab for unresectable, metastatic, or when surgery causes unacceptable morbidity | Local imaging every 3-6 months for 2-3 years; chest imaging for lung mets |
| ESMO / European sarcoma groups | Similar surgical principles; emphasis on referral to specialist sarcoma centres | Denosumab recommended for unresectable; neoadjuvant use under investigation | Minimum 5-year follow-up with local imaging; chest CT at baseline |
| BOA / British Sarcoma Group (UK) | Specialist bone tumour centre management; MDT discussion mandatory | Denosumab via specialist commissioning for unresectable or metastatic GCTB | Follow-up per British Sarcoma Group protocols |
| Japanese Orthopaedic Association / Asian guidelines | Extended curettage standard; higher threshold for wide resection | Denosumab approved; some centres use as neoadjuvant to facilitate joint-preserving surgery | Regular local and chest imaging; longer follow-up for sacral lesions |
There is no dedicated GCTB registry comparable to arthroplasty registries. Outcome data come from institutional case series, the NCCN database, and pooled analyses. Denosumab has transformed the management of unresectable GCTB but optimal treatment duration, cessation strategies, and long-term safety data remain active areas of investigation. The evidence base is strongest for extended curettage as the surgical gold standard, with denosumab reserved for specific indications.
All suspected GCTB should be referred to a specialist bone tumour or sarcoma multidisciplinary team (MDT).
Record at initial assessment:
- Clinical and radiographic Campanacci grade
- Biopsy performed and confirmed (never treat without histology)
- Serum calcium and PTH checked to exclude brown tumour
- Chest imaging (CT or radiograph) for baseline staging
- Discussion at MDT meeting documented
Medicolegal pitfall: Operating on a lytic bone lesion without a biopsy, mistaking a sarcoma for GCTB, or treating brown tumour of hyperparathyroidism surgically — all are well-documented sources of litigation worldwide.
Controversies & Areas of Uncertainty
Some centres use 3-6 months of denosumab to shrink tumours and facilitate joint-preserving curettage, especially for Campanacci Grade III lesions. However, the neoplastic stromal cells persist and tumour recurrence after cessation is well-documented. The optimum duration of pre-operative denosumab and the risk of making histological assessment more difficult (due to giant cell elimination) remain debated.
Phenol, cryotherapy, and PMMA cement all reduce recurrence compared with simple curettage, but no single adjuvant has demonstrated clear superiority in head-to-head trials. The choice is often surgeon-dependent and institution-specific. Cryotherapy carries higher fracture risk; phenol requires careful handling; cement provides structural support but may complicate revision surgery.
For unresectable GCTB, the optimal duration of denosumab is unknown. Long-term therapy raises concerns about osteonecrosis of the jaw, atypical fractures, and cost. Stopping denosumab carries a risk of rapid rebound tumour growth. No consensus exists on whether denosumab can be safely stopped, tapered, or must be continued lifelong.
PMMA cement provides immediate stability and has a thermal adjuvant effect but may complicate revision if recurrence occurs. Bone graft is biological but takes months to incorporate and provides no adjuvant benefit. Many surgeons use a hybrid approach: subchondral bone graft to protect articular cartilage with cement filling the remainder of the defect.
Key Facts
- Most common aggressive benign bone tumour in young adults (20-40 years)
- 5-8% of all primary bone tumours, slight female predominance
- 50% occur around the knee (distal femur + proximal tibia)
- Neoplastic stromal cells overexpress RANKL, recruiting reactive osteoclast-like giant cells
Diagnosis
- Lytic metaepiphyseal lesion abutting subchondral bone in skeletally mature patient
- Campanacci Grade I (intact cortex), II (expanded cortex), III (soft tissue extension)
- Always biopsy before definitive surgery — CT-guided core needle biopsy preferred
- Check calcium and PTH to exclude brown tumour of hyperparathyroidism
Surgical Management
- Extended curettage = adequate window + high-speed burr + adjuvant (phenol/cryo/cement)
- Recurrence: simple curettage approximately 50% vs extended curettage 15-25%
- Wide resection for recurrent Grade III, expendable bones, or joint destruction
- Reconstruction: cement, bone graft, plates, or megaprosthesis depending on defect
Medical Management
- Denosumab (anti-RANKL monoclonal antibody) for unresectable or metastatic disease
- Loading: 120 mg SC days 1, 8, 15 then monthly — calcium and vitamin D mandatory
- Disease control in 80-90% while on therapy — rebound on cessation is documented
- Monitor for hypocalcaemia, osteonecrosis of the jaw, and atypical fractures
Complications and Follow-up
- Local recurrence 15-25% after extended curettage — most within 3 years
- Lung metastasis in 1-3% (histologically benign, may require wedge resection)
- Malignant transformation less than 1% (usually radiation-associated)
- Follow-up: local imaging every 3-6 months for 2 years, then 6-12 months to 5 years