Subungual Location | Classic Triad | Complete Excision Curative
- Classic triad: Severe pain, cold sensitivity, point tenderness
- Love's test: Pencil tip reproduces exact pain
- Hildreth's test: Tourniquet relieves pain
- MRI gold standard - hyperintense T2, enhancing lesion
- Complete excision curative - recurrence from incomplete removal
- “Patient can point to exact spot with one finger (pathognomonic)
- “Pain disproportionate to tumor size (usually less than 10mm)
- “Trans-ungual approach for subungual lesions preserves nail
Pain + Cold sensitivity + Point tenderness. Patient can localize to exact spot with one finger. Pain disproportionate to tiny tumor size.
Love's test: Pencil tip reproduces pain at exact spot. Hildreth's test: Tourniquet application relieves pain.
MRI gold standard - hyperintense on T2, enhances with gadolinium. May see bony scalloping on X-ray. Ultrasound useful for superficial lesions.
Complete excision is curative (90%+ success). Trans-ungual approach for subungual. Recurrence 10-20% if incomplete.
Glomus Tumors of the Hand
GLOMUSPAIN
Hook:GLOMUS PAIN
Introduction
Glomus tumors are rare benign neoplasms arising from the glomus body, a specialized arteriovenous anastomosis involved in thermoregulation. In the hand, these tumors most commonly occur in the subungual region (50-75% of cases), particularly in the fingertips. Despite their small size (usually less than 10 mm), glomus tumors cause disproportionately severe pain, exquisite point tenderness, and marked cold sensitivity—a clinical triad that is virtually pathognomonic.
The diagnosis is primarily clinical, supported by imaging (MRI or ultrasound), and treatment is complete surgical excision, which is curative and provides dramatic symptom relief in over 90% of cases.
CLASSIC
Hook:CLASSIC TRIAD
Epidemiology
Incidence: Rare, exact incidence unknown (estimated less than 2% of all soft tissue tumors)
Key Demographics:
- Age: 20-50 years (peak incidence 30-40 years)
- Gender: Female predominance (3:1 ratio for solitary lesions)
- Location: Fingers greater than hand greater than other sites
- Subungual: 50-75% of hand glomus tumors
- Thumb: Most common digit affected
Diagnostic delay (global): Across published series, the interval from symptom onset to diagnosis ranges from roughly 18 months (Saaiq) to an average of 7-10 years (Van Geertruyden), reflecting the rarity of the lesion and low primary-care awareness rather than any regional health-system factor.
Anatomy and Pathophysiology
Normal Glomus Body:
- Specialized arteriovenous anastomosis (Sucquet-Hoyer canal)
- Concentrated in distal extremities (fingertips, palms)
- Function: Thermoregulation via shunting blood flow
- Richly innervated by sympathetic nerve fibers
- Located in dermis and subcutaneous tissue
Components:
- Afferent arteriole: Brings arterial blood
- Glomus cells: Modified smooth muscle cells surrounding anastomosis
- Efferent venule: Drains blood to venous system
- Nerve supply: Extensive unmyelinated nerve fibers (explains pain)
Tumor Pathology:
- Benign neoplasm of glomus cells
- Well-circumscribed, encapsulated
- Size: Typically 3-10 mm (rarely larger)
- Three histologic types:
- Glomus tumor proper (75%): Predominantly glomus cells
- Glomangioma: Vascular component prominent (20%)
- Glomangiomyoma: Smooth muscle component (5%)
Pain Mechanism:
- Extensive unmyelinated nerve fibers within and around tumor
- Pressure on nerves causes severe pain
- Temperature changes (cold) cause vasoconstriction, increased pressure
- Mechanical pressure (Love's test) reproduces pain
Clinical Variants
Solitary Glomus Tumor (90% of cases):
- Single lesion
- Subungual or fingertip location typical
- Female predominance
- Sporadic occurrence
- Symptomatic (pain, cold sensitivity)
Multiple Glomus Tumors (10% of cases):
- Multiple lesions, may be hundreds
- Often extradigital locations
- Male predominance
- Autosomal dominant inheritance (some families)
- Less painful than solitary lesions
- Associated with NF1 in some cases
Glomangiomatosis:
- Rare diffuse form
- Involves entire digit or hand segment
- Presents in childhood
- More vascular, may have mass effect
Malignant Glomus Tumour (Glomangiosarcoma) and the Folpe Classification
The Folpe EvidenceCard defines the malignancy criteria, the WHO row references them, and a viva follow-up asks "could this be malignant transformation?" - but the body never sets out the classification or answers that question. It is high-yield and reassuring.
- Malignancy is rare, and it is defined histologically, not by "transformation." Folpe et al. (from 52 unusual glomus tumours) proposed a four-category scheme now adopted by the WHO:
- Benign glomus tumour - the ordinary lesion.
- Symplastic glomus tumour - high nuclear grade alone with no other worrying feature; despite the scary nuclei it behaves benignly.
- Glomus tumour of uncertain malignant potential (UMP) - has a concerning feature (high mitotic activity with superficial location only, or large size only, or deep location only) but does not meet full malignant criteria.
- Malignant glomus tumour (glomangiosarcoma) - deep location AND size greater than 2 cm, or atypical mitotic figures, or moderate-to-high nuclear grade with 5 or more mitoses per 50 high-power fields.
- Behaviour tracks the category. In Folpe's series, metastasis occurred in 38% of tumours meeting the malignant criteria, but in none classified as symplastic, UMP or glomangiomatosis. The drivers of metastatic risk were deep location, size greater than 2 cm, and atypical mitoses.
- The reassuring bottom line for the hand. A small, superficial, subungual fingertip lesion is essentially always benign - malignant glomus tumours are typically deep and large (greater than 2 cm). Reserve concern (and wide excision plus sarcoma-service referral) for a deep, large or histologically atypical lesion, not for the classic painful subungual nodule.
Q: How is a malignant glomus tumour defined and how worried should you be about a subungual hand lesion? A: By the Folpe criteria: malignant (glomangiosarcoma) = deep AND greater than 2 cm, or atypical mitoses, or high nuclear grade with 5 or more mitoses per 50 HPF; symplastic (high grade only) and uncertain malignant potential behave benignly. Metastasis occurred in 38% of malignant-criteria tumours but none of the others. A small, superficial, subungual hand lesion is essentially always benign - reserve wide excision and sarcoma referral for a deep, large (greater than 2 cm) or atypical tumour.
The Multiple and Familial Forms: Glomuvenous Malformation and NF1-Associated Glomus Tumours
The Clinical Variants and Controversies sections note that multiple glomus tumours are less painful, may be autosomal dominant and are "associated with NF1", but the genetics that make this a distinct entity are never developed - and they explain why the multiple form looks and behaves so differently.
- Familial multiple glomangiomas = glomuvenous malformations (GVM). The inherited multiple form is now recognised as a venous-type malformation, caused by autosomal-dominant loss-of-function mutations in the GLOMULIN (GLMN) gene (with a "paradominant"/second-hit mechanism explaining the patchy distribution). They present as multiple bluish, partially compressible nodules or plaques, often extradigital and segmental, appear younger, show a slight male predominance, and are much less painful than the solitary lesion - the opposite of the classic exquisitely-tender sporadic subungual tumour.
- NF1-associated glomus tumours are a separate link. Patients with neurofibromatosis type 1 have an increased incidence of glomus tumours, characteristically multiple and in the digits/subungual region and genuinely painful, arising from biallelic NF1 inactivation (a somatic second hit in the glomus cells). So unexplained fingertip pain in an NF1 patient should prompt a search for a glomus tumour (the NF1 syndrome itself is covered in the neurofibromatosis topic).
- Why it matters. The multiple/familial form is easy to under-treat (lesions are numerous and less symptomatic), the genetics carry inheritance implications for GVM (autosomal dominant), and recognising the NF1 association changes who you screen. The solitary sporadic tumour remains the painful, curable, subungual lesion of the rest of this topic.
Q: How do the multiple/familial glomus lesions differ from the solitary tumour, and what is the genetic basis? A: The familial multiple form is a glomuvenous malformation from autosomal-dominant GLOMULIN (GLMN) mutations - multiple bluish compressible nodules, often extradigital, younger, slight male predominance, and much less painful than the solitary lesion. Separately, NF1 patients have an increased incidence of multiple, painful, digital/subungual glomus tumours (biallelic NF1 loss) - so fingertip pain in NF1 warrants a look. The classic solitary, exquisitely painful subungual tumour (female, sporadic) is the curable lesion covered elsewhere in this topic.
Clinical Presentation
Classic Symptom Triad
Severe Localized Pain (present in greater than 90% of cases):
Characteristics:
- Paroxysmal: Intermittent severe episodes
- Lancinating or burning: Sharp, electric-shock-like quality
- Disproportionate to size: Small tumor causes severe pain
- Nocturnal: Often worse at night
- Positional: Worse with hand dependency
- Intensity: Patients describe as "unbearable" or "worst pain ever"
Pain Triggers:
- Pressure on affected area
- Cold exposure (most specific trigger)
- Bumping or trauma to fingertip
- Tight gloves or shoes (if in foot)
- Temperature changes
Impact on Life:
- Avoidance of cold environments
- Difficulty sleeping
- Occupational limitations
- Psychological distress from chronic pain
- Protective behavior of affected digit
The severity and specificity of pain often leads to initial psychiatric or neurological referrals before correct diagnosis.
Physical Examination
Inspection:
- Subungual lesions:
- Bluish-red discoloration through nail (40-60% of cases)
- Nail ridging or deformity (pressure erosion of bone)
- Visible mass if nail removed
- Extraungual lesions:
- Small nodule, skin-colored to bluish
- May not be visible externally
- Nail changes: Longitudinal ridging, thinning over tumor
Palpation:
- Point tenderness: Exquisite tenderness at tumor site
- Size: Often impalpable due to small size
- Consistency: Firm if palpable
- Mobility: Attached to deeper structures
Special Tests:
Love's Test (Pinprick Test):
- Apply pressure to suspected area with blunt object or pinhead
- Positive: Severe pain elicited at exact tumor location
- Specificity: High for glomus tumor
- Technique: Systematic palpation of entire nail bed, note exact pain point
Hildreth's Test (Tourniquet Test):
- Apply finger tourniquet to occlude venous return
- Palpate suspected area with Love's test
- Positive: Pain relieved with tourniquet inflation
- Mechanism: Reduces venous pressure, decreases tumor engorgement
- Less reliable than Love's test, not routinely necessary
Cold Sensitivity Test:
- Immerse digit in ice water or apply ice
- Positive: Severe pain within seconds
- Highly specific for glomus tumor
- Patients often refuse test due to anticipated pain
Transillumination:
- Negative (unlike mucous cysts)
- Solid mass does not allow light transmission
Differential Diagnosis
- painCharacter
- Severe, paroxysmal, lancinating
- coldSensitivity
- Marked (hallmark)
- pointTenderness
- Exquisite, pinpoint
- appearance
- Bluish-red through nail (40-60%)
- imaging
- MRI: Enhancing lesion, T2 bright
- treatment
- Surgical excision (curative)
- painCharacter
- Painless usually
- coldSensitivity
- Absent
- pointTenderness
- Minimal or absent
- appearance
- Brown-black pigmentation, Hutchinson's sign
- imaging
- MRI: Mass, variable enhancement
- treatment
- Amputation ± sentinel node biopsy
- painCharacter
- Minimal pain
- coldSensitivity
- Absent
- pointTenderness
- Minimal
- appearance
- Translucent, dorsal DIP joint
- imaging
- Radiograph: DIP OA, osteophytes
- treatment
- Excision with osteophyte removal
- painCharacter
- Minimal pain initially
- coldSensitivity
- Absent
- pointTenderness
- Minimal
- appearance
- Ulcerated, verrucous, irregular
- imaging
- MRI: Infiltrative mass, bone invasion
- treatment
- Wide excision or amputation
- painCharacter
- Mild discomfort
- coldSensitivity
- Absent
- pointTenderness
- Mild
- appearance
- Hyperkeratotic, cauliflower texture
- imaging
- Not needed, clinical diagnosis
- treatment
- Cryotherapy, salicylic acid, excision
- painCharacter
- Painless unless infected
- coldSensitivity
- Absent
- pointTenderness
- Minimal (unless infected)
- appearance
- Skin-colored, central punctum
- imaging
- Ultrasound: Cystic lesion
- treatment
- Excision with cyst wall
- painCharacter
- Sharp, electric-shock pain
- coldSensitivity
- Variable
- pointTenderness
- Present (Tinel's sign)
- appearance
- Not visible, palpable nodule
- imaging
- MRI: Nerve thickening
- treatment
- Excision, nerve burial, or relocation
The classic triad (severe pain, cold sensitivity, point tenderness) makes glomus tumor diagnosis straightforward despite its rarity.
Investigations
Imaging
MRI - Investigation of Choice:
Protocol:
- Dedicated small field-of-view imaging of affected digit
- T1-weighted sequences: Isointense to muscle
- T2-weighted sequences: Hyperintense (high signal)
- Post-contrast T1 with fat saturation: Intense enhancement
- High-resolution (3T preferred over 1.5T for small lesions)
Findings:
- Well-circumscribed, homogeneous mass
- Size: Typically 3-10 mm
- Location: Subungual (nail bed) or pulp
- T1: Isointense to muscle
- T2: Hyperintense (bright)
- T1+C: Intense homogeneous enhancement
- Bone: May show pressure erosion (scalloping) of distal phalanx
Sensitivity and Specificity:
- Sensitivity: 85-95% for lesions greater than 2 mm
- Specificity: 50-75% (other vascular lesions may mimic)
- Negative MRI: Does not exclude glomus tumor (sensitivity not 100%)
Utility:
- Confirm suspected diagnosis
- Localize tumor pre-operatively (guide surgical approach)
- Distinguish from other subungual lesions
- Assess for multiple lesions
MRI is highly sensitive but clinical diagnosis remains paramount. Negative MRI with classic triad should still prompt surgical exploration.
Biopsy
Not Routinely Indicated:
- Clinical diagnosis with imaging confirmation usually sufficient
- Risk of incomplete excision with biopsy
- May cause bleeding, hematoma
- Tumor small, excision is both diagnostic and therapeutic
Consider Biopsy If:
- Atypical imaging features raising concern for malignancy
- Large lesion (greater than 2 cm) suggesting alternative diagnosis
- Multiple lesions with uncertain diagnosis
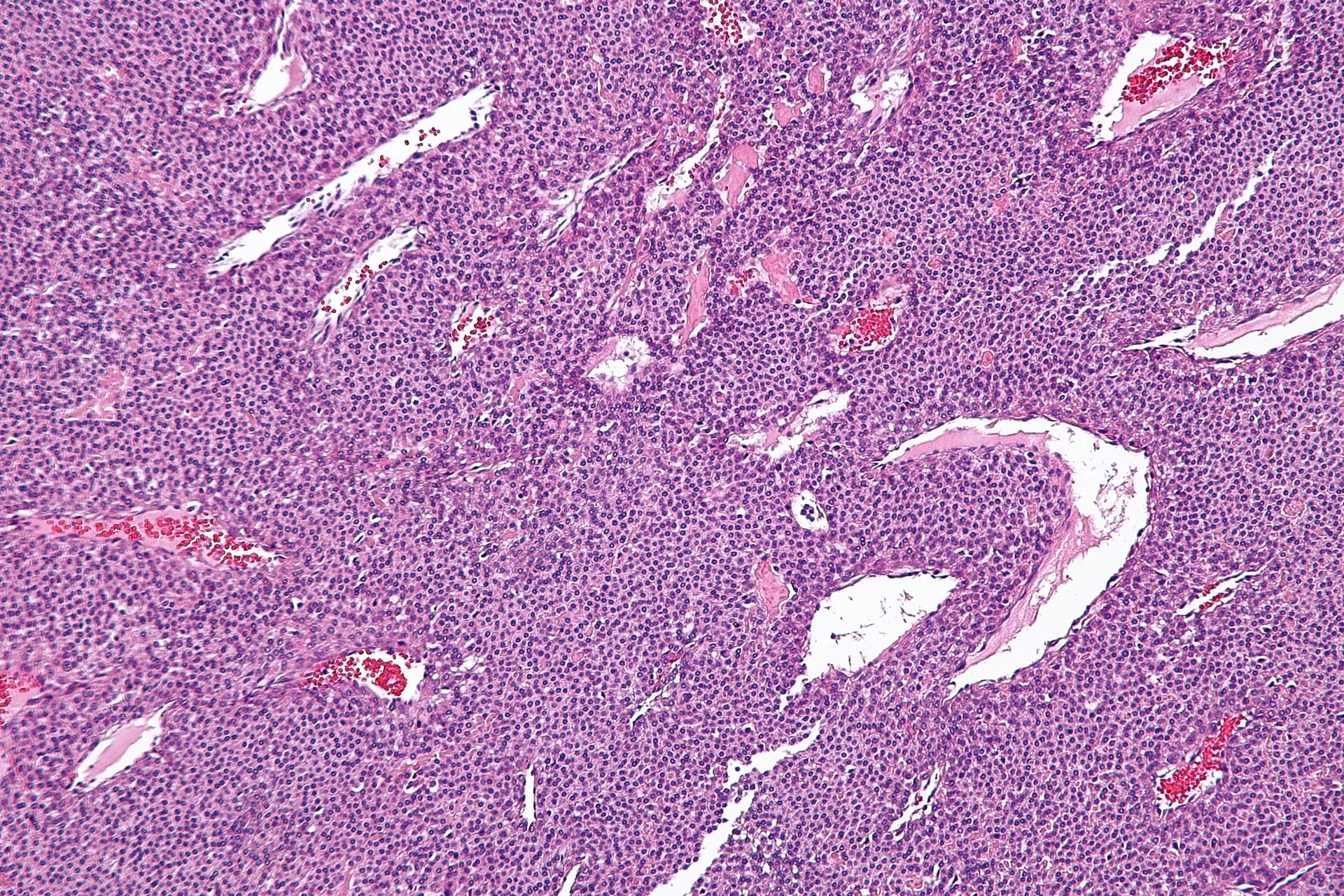
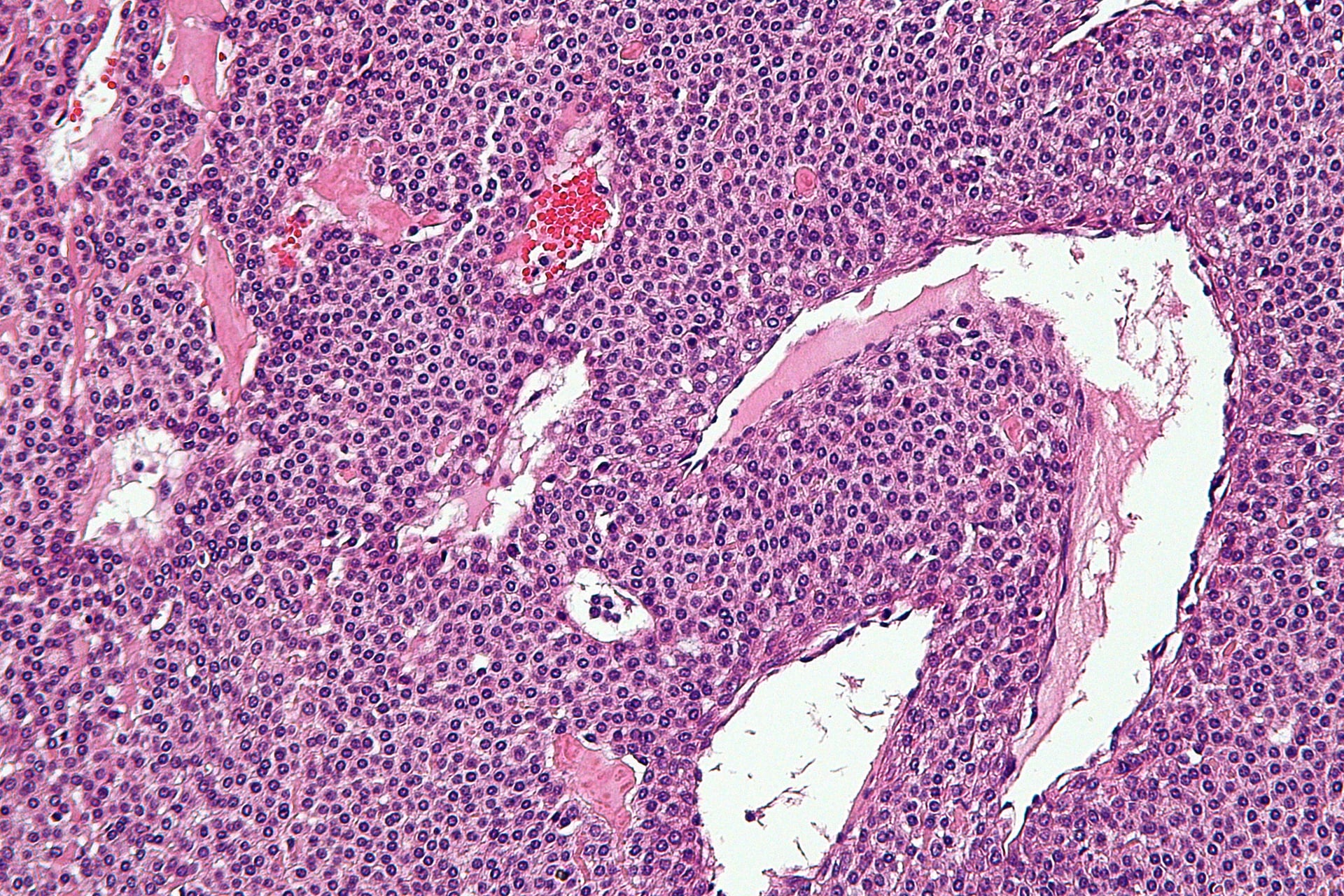
Histopathology (after surgical excision):
- Well-circumscribed mass
- Three cell types:
- Glomus cells: Uniform, round, centrally located nuclei
- Vascular component: Capillary-sized vessels
- Smooth muscle: Surrounding vessels
- Immunohistochemistry:
- Glomus cells: Positive for smooth muscle actin (SMA), vimentin
- Negative for S100, cytokeratin, desmin
- No mitoses, no atypia (benign)
Non-Operative Management
Limited Role
Observation:
- Not recommended for symptomatic lesions
- Pain quality of life impairment significant
- No spontaneous resolution
- Progressive bone erosion may occur
Indications for Non-Operative Approach:
- Incidental finding, asymptomatic (rare)
- Patient refuses surgery
- Significant comorbidities precluding surgery
- Diagnostic uncertainty (may observe with interval imaging)
Medications:
- Analgesics: Limited efficacy for neuropathic-type pain
- Gabapentin/pregabalin: Minimal benefit
- NSAIDs: Ineffective for symptom control
- Calcium channel blockers (nifedipine): Anecdotal reports, weak evidence
Pre-operative Counseling
Realistic Expectations:
- Surgery highly successful (greater than 90% cure rate)
- Complete symptom relief typical
- Recurrence low (less than 10%, usually incomplete excision)
- Nail may not grow back normally if matrix damaged
- Small scar at surgical site
Surgical Risks:
- Incomplete excision (recurrence)
- Nail deformity
- Infection (rare)
- Prolonged pain (if nerve injury)
- Cold intolerance may persist briefly even after excision
Surgical Management
EXCISE
Hook:EXCISE
Indications
Symptomatic Glomus Tumor:
- Classic triad (pain, cold sensitivity, point tenderness)
- Confirmed or suspected on imaging
- Failed observation (if attempted)
Relative Indications:
- Incidental finding with mild symptoms
- Patient preference for definitive treatment
Surgical Approaches
Subungual (Nail Bed) Approach - Most Common:
Indications:
- Subungual glomus tumor (50-75% of hand cases)
- Tumor distal to lunula
- Identified on MRI or ultrasound
Technique:
- Anesthesia: Digital block (avoid epinephrine in some centers)
- Tourniquet: Finger tourniquet for hemostasis
- Nail removal:
- Elevate nail plate from nail bed with freer elevator
- Complete nail plate removal
- Preserve nail matrix proximally (avoid permanent deformity)
- Tumor identification:
- Often visible as bluish-red lesion in nail bed
- Correlate with pre-operative imaging and point tenderness
- May require meticulous exploration if not immediately visible
- Excision:
- Careful dissection around tumor capsule
- Complete excision en bloc (avoid rupture or piecemeal removal)
- Preserve nail bed germinal and sterile matrix
- Remove small margin of surrounding nail bed if adherent
- Hemostasis: Release tourniquet, meticulous hemostasis
- Nail bed repair: Absorbable 6-0 or 7-0 sutures if nail bed defect
- Nail plate replacement: Replace nail plate as biologic dressing (or silicone conformer)
- Closure: Non-adherent dressing, protective splint
Key Technical Points:
- Tourniquet essential for visualization
- Complete excision critical (recurrence if incomplete)
- Protect germinal matrix (avoid permanent nail deformity)
- Tumor may be very small (3-5 mm), requires meticulous search
This approach provides excellent exposure and is the gold standard for subungual tumors.
Intraoperative Challenges
Tumor Not Visible:
- Small size (3-5 mm) may make identification difficult
- Correlate with pre-operative imaging (measure distance from landmarks)
- Use Love's test intraoperatively (without tourniquet, patient awake)
- Meticulous exploration of entire nail bed
- Consider ultrasound-guided localization (wire or dye injection pre-op)
Multiple Tumors:
- Glomangiomatosis or multiple glomus tumors
- May require extended exploration
- Consider interval imaging if symptoms persist
Bone Involvement:
- Pressure erosion of distal phalanx
- Curettage of bone if tumor adherent
- Usually no bone grafting needed (remodels)
Post-operative Management
Immediate Post-operative (0-2 weeks):
- Bulky protective dressing
- Elevate hand above heart level (reduce swelling, pain)
- Pain management: Typically minimal after tumor removed
- Dressing change at 48-72 hours
- Monitor for hematoma, infection
Early Rehabilitation (2-6 weeks):
- Suture removal at 10-14 days
- Gentle active motion as tolerated
- Protect nail bed (avoid trauma)
- Scar massage once wound healed
Nail Regrowth (3-6 months):
- Nail grows approximately 1 mm per week
- Full nail regrowth takes 3-6 months
- May have ridging or irregularity initially
- Usually normalizes by 6-12 months
Return to Activities:
- Light activities at 2 weeks
- Full unrestricted activities at 6 weeks
- Avoid forceful gripping until nail fully regrown
Outcomes
Symptom Relief:
- Pain relief: Immediate and dramatic in greater than 90% of cases
- Cold sensitivity: Resolves in greater than 85%
- Patient satisfaction: Extremely high (greater than 95%)
Recurrence:
- Overall recurrence rate: 5-10%
- Cause: Incomplete excision (tumor cells left behind)
- Risk factors: Poorly localized tumor, surgeon inexperience, multiple tumors
- Management of recurrence: Revision excision (usually successful)
Nail Deformity:
- Transient nail changes: 30-40% (ridging, irregular growth)
- Permanent nail deformity: Less than 5% (germinal matrix injury)
- Cosmetically acceptable: Most cases
Complications
- incidence
- 5-10%
- cause
- Incomplete excision, tumor cells left behind
- prevention
- Complete en bloc excision, careful intraoperative search
- management
- Revision excision, imaging to localize recurrence
- outcome
- Revision successful in greater than 90%
- incidence
- Less than 5%
- cause
- Germinal matrix injury during dissection
- prevention
- Meticulous dissection, protect matrix, fine instruments
- management
- Observation (some improve over years), nail reconstruction
- outcome
- Usually cosmetically acceptable
- incidence
- 30-40%
- cause
- Temporary matrix disruption, inflammation
- prevention
- Gentle tissue handling, matrix repair
- management
- Observation, reassurance
- outcome
- Resolves in 6-12 months
- incidence
- Less than 2%
- cause
- Bacterial contamination
- prevention
- Sterile technique, prophylactic antibiotics (controversial)
- management
- Antibiotics, wound care, rarely I&D
- outcome
- Good with early treatment
- incidence
- 5-10%
- cause
- Inadequate hemostasis
- prevention
- Meticulous hemostasis after tourniquet release
- management
- Elevation, compression, rarely evacuation
- outcome
- Resolves with conservative treatment
- incidence
- Less than 5%
- cause
- Incomplete excision, neuroma, nerve injury
- prevention
- Complete tumor excision, protect digital nerves
- management
- Imaging for recurrence, neuroma excision if identified
- outcome
- Variable, depends on cause
- incidence
- Less than 10%
- cause
- Nerve trauma, sympathetic dysfunction
- prevention
- Gentle dissection, avoid nerve injury
- management
- Observation, usually improves over months
- outcome
- Most resolve by 6-12 months
Management of Recurrence
Evaluation:
- History: Recurrent pain, cold sensitivity
- Examination: Point tenderness at or near original site
- MRI: Localize recurrent tumor
- Consider alternative diagnoses (neuroma, scar tenderness)
Revision Surgery:
- Indications: Symptomatic recurrence
- Pre-operative imaging: Essential for localization
- Technique: Re-explore original site, wider excision
- Success rate: Greater than 90% for first revision
- Counsel patient: Slightly higher risk of nail deformity with revision
Guidelines, Registries & Global Practice
Global Epidemiology
- Glomus tumours account for under 2% of soft-tissue tumours and roughly 1-5% of all hand tumours, with similar demographics reported worldwide.
- Solitary lesions: female predominance (about 3:1) and peak presentation in the fourth-to-fifth decades across hand series from Europe, the Middle East, North America and South Asia.
- Multiple/familial glomus tumours (about 10%) skew male, present younger, are less painful, and may show autosomal-dominant inheritance; a minority are NF1-associated.
- Subungual location dominates hand series (50-82%); the thumb and index finger are most frequently involved. Foot lesions are rare and commonly misdiagnosed as ingrown toenails.
Guidance & Evidence Landscape
There is no dedicated society guideline (no AAOS, BOA-BOAST, AO or EFORT statement) for glomus tumours, reflecting their rarity. Practice is governed by Level IV/V evidence and pathology consensus:
- Practical position
- Adopts Folpe criteria - most are benign; "malignant glomus tumour" requires deep location + size over 2 cm, atypical mitoses, or high nuclear grade with high mitotic count
- Practical position
- Clinical triad + targeted imaging; complete marginal excision is curative; protect the nail matrix
- Practical position
- High-resolution contrast MRI or high-frequency ultrasound; a negative study does not exclude the diagnosis
No arthroplasty/implant registry data apply (no implants are used); outcome data derive entirely from single-centre case series.
High- vs Limited-Resource Practice Variation
- Well-resourced settings: 3T small-field-of-view contrast MRI or high-frequency (over 15 MHz) Doppler ultrasound for localisation; day-case excision under regional/local anaesthesia; routine histopathology.
- Limited-resource settings: diagnosis rests on the clinical triad plus Love's and Hildreth's tests, with excision under digital block and tourniquet; histology confirms the diagnosis and excludes malignancy where available. Several large series (e.g. from South Asia) show that clinically-driven excision without advanced imaging still achieves complete relief and very low recurrence.
Pathology & Therapy
- Every excised specimen should be sent for histopathology to confirm the diagnosis and exclude the rare malignant variant.
- Hand therapy has a limited role: not required pre-operatively and usually unnecessary after uncomplicated excision; reserved for persistent stiffness, scar sensitivity or nail-related problems.
Controversies & Areas of Uncertainty
The entire glomus-tumour literature is Level IV/V (retrospective case series and pathology reviews). There are no randomised trials and no validated diagnostic scoring system, so the points below are areas of genuine debate rather than settled fact.
1. Is pre-operative MRI necessary at all? Al-Qattan's group abandoned routine MRI, arguing that a confident clinical triad justifies straight-to-theatre exploration (and that MRI's negative predictive value is only ~20%). Others retain MRI to localise the lesion, exclude multiplicity and reduce operative search time. Pragmatic position: image when the diagnosis is uncertain, the lesion is impalpable/non-visible, symptoms are atypical, or revision is planned; clinical confidence can otherwise carry the decision.
2. Diagnostic test reliability. Love's test is sensitive but not specific; Hildreth's test and the cold-sensitivity test are more specific but less reproducible and are not validated against a reference standard. No single sign is diagnostic - the combination is what carries weight, and a negative test never excludes the tumour.
3. Surgical approach for subungual lesions. Transungual (nail-plate removal) gives the best exposure but risks nail-matrix injury and dystrophy. Lateral subperiosteal/periungual ("Keyser-Littler") approaches aim to spare the nail but offer less direct vision and may raise the incomplete-excision/recurrence risk. The trade-off (nail cosmesis vs. completeness of excision) is unresolved and surgeon-dependent.
4. True recurrence vs. incomplete excision vs. a missed second lesion. Reported "recurrence" of 5-20% almost certainly conflates residual tumour from incomplete first excision, a synchronous lesion missed at index surgery, and rare genuine de novo recurrence. Because management is the same (re-image, re-explore, excise completely), the distinction is largely academic - but it matters for how recurrence rates are quoted and compared.
5. Magnetic susceptibility and multiplicity. Multiple/familial glomus tumours (glomangiomas, sometimes NF1-associated) behave differently from solitary lesions and are easy to under-treat; whether routine screening imaging is warranted in the multiple form is unsettled.
Summary
Glomus tumors are rare benign neoplasms arising from the glomus body, a specialized arteriovenous anastomosis involved in thermoregulation. They occur most commonly in the subungual region (50-75% of hand cases), affecting women more than men (3:1), with peak incidence at 30-40 years.
The classic clinical triad—severe paroxysmal pain, exquisite point tenderness (Love's test positive), and marked cold sensitivity—is virtually pathognomonic and allows clinical diagnosis even before imaging. Despite their small size (typically 3-10 mm), glomus tumors cause disproportionately severe pain that significantly impacts quality of life.
MRI is the gold standard investigation, demonstrating a well-circumscribed T2-hyperintense lesion with intense enhancement on post-contrast T1 sequences. Sensitivity is 85-95%, but negative MRI with classic triad should still prompt surgical exploration. Plain radiographs show bone erosion (scalloping of distal phalanx) in only 20-40% of cases.
Surgical excision is the treatment of choice, providing immediate dramatic pain relief in greater than 90% of cases. The key surgical principle is complete en bloc excision to prevent recurrence. Surgical approach depends on tumor location: subungual (nail removal, tumor excised from nail bed), transungual (for proximal lesions under lunula), or extraungual (direct approach for pulp/lateral tumors).
Outcomes are excellent with high patient satisfaction (greater than 95%), immediate pain relief, and resolution of cold sensitivity in greater than 85%. Recurrence occurs in 5-10% due to incomplete excision and is managed with revision surgery (successful in greater than 90%). Nail deformity is usually transient (30-40%) with permanent deformity rare (less than 5%) if germinal matrix protected during surgery.
The major clinical challenge is diagnostic delay (average 5-7 years from symptom onset to diagnosis) due to the rarity of the condition and lack of awareness. Increased recognition of the classic triad by general practitioners can expedite diagnosis and referral, reducing patient suffering.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old woman presents with a 3-year history of severe, paroxysmal pain in her right thumb tip. She describes the pain as lancinating and unbearable, particularly triggered by cold exposure. She has to wear gloves constantly and cannot tolerate getting ice from the freezer. Examination shows exquisite point tenderness on the radial aspect of the nail bed. How would you assess and manage this?”
“A 45-year-old man has had fingertip pain for 7 years. He has seen multiple specialists including neurology and psychiatry. MRI was reported as negative. He insists his symptoms are real and not psychological. On examination, you identify a small area of point tenderness on the radial nail bed but no visible abnormality. What is your approach?”
“A 28-year-old woman had excision of a subungual glomus tumor 18 months ago with initial symptom resolution. She now has recurrence of severe pain and cold sensitivity in the same thumb. She also has developed a permanent nail ridge deformity. MRI shows a 4 mm enhancing lesion adjacent to her previous excision site. How would you counsel and manage her?”
One-Liner Definition
- Glomus tumors are rare benign neoplasms arising from the glomus body (specialized arteriovenous anastomosis)
- Most commonly subungual in location
- Classic triad: severe paroxysmal pain, exquisite point tenderness, marked cold sensitivity
Classic Clinical Triad
- Severe paroxysmal lancinating pain (disproportionate to tumor size)
- Exquisite point tenderness (Love's test positive)
- Marked cold sensitivity (highly specific symptom, patients avoid cold exposure)
Epidemiology
- Rare (less than 2% of soft tissue tumors)
- Peak age 30-40 years, Female predominance 3:1
- Subungual location 50-75% of hand cases, Thumb most commonly affected
- Long diagnostic delay common (average 5-7 years)
Key Examination Findings
- Pinpoint tenderness at tumor site (Love's test)
- Bluish-red discoloration through nail (40-60% if subungual)
- Nail ridging or deformity from bone erosion
- Cold sensitivity test: pain with ice water immersion
- Hildreth's test: pain relief with tourniquet (less reliable)
Investigations
- MRI (gold standard): T2 hyperintense, intense enhancement on T1+contrast, well-circumscribed 3-10 mm lesion, Sensitivity 85-95%
- Ultrasound alternative: Hypoechoic, hypervascular on Doppler
- Radiographs: Bone erosion in 20-40% (scalloping of distal phalanx)
Surgical Indications
- Symptomatic glomus tumor (pain, cold sensitivity)
- Failed observation
- Patient desire for definitive treatment
- Surgery is curative in greater than 90%
Surgical Approaches
- Subungual: Nail removal, tumor excision from nail bed (most common)
- Transungual: Eponychium reflection, matrix incision (for proximal lesions)
- Extraungual: Direct incision over tumor (for pulp or lateral lesions)
- Key: Complete en bloc excision
Critical Surgical Steps
- Complete tumor excision en bloc (avoid piecemeal removal to prevent recurrence)
- Protect germinal matrix (avoid permanent nail deformity)
- Meticulous hemostasis after tourniquet release
- Correlate with pre-op imaging for localization if tumor not immediately visible
Outcomes
- Pain relief: Immediate and dramatic in greater than 90%
- Recurrence: 5-10% (from incomplete excision)
- Nail deformity: Transient 30-40%, permanent less than 5%
- Patient satisfaction: Greater than 95%
- Revision successful in greater than 90% if recurrence
Complications
- Recurrence (5-10%, incomplete excision)
- Nail deformity (permanent less than 5%, transient 30-40%)
- Infection (less than 2%)
- Hematoma (5-10%)
- Persistent cold sensitivity (less than 10%, usually resolves)
Common Viva Questions
- What is a glomus body? (Specialized arteriovenous anastomosis for thermoregulation)
- Why such severe pain? (Extensive unmyelinated nerve fibers within and around tumor)
- What is Love's test? (Pinprick pressure reproduces severe pain at tumor location)
- Negative MRI with classic triad: What do you do? (Explore surgically, MRI sensitivity not 100%)
Pearls and Pitfalls
- PEARLS: Classic triad is pathognomonic, MRI gold standard but negative doesn't exclude
- Complete excision key to preventing recurrence
- Immediate dramatic pain relief post-op confirms diagnosis
- PITFALLS: Long diagnostic delay common (5-7 years), Incomplete excision causes recurrence
- Germinal matrix injury causes permanent nail deformity