Hardcastle/Myerson Classification of Lisfranc Injuries
The Hardcastle/Myerson classification
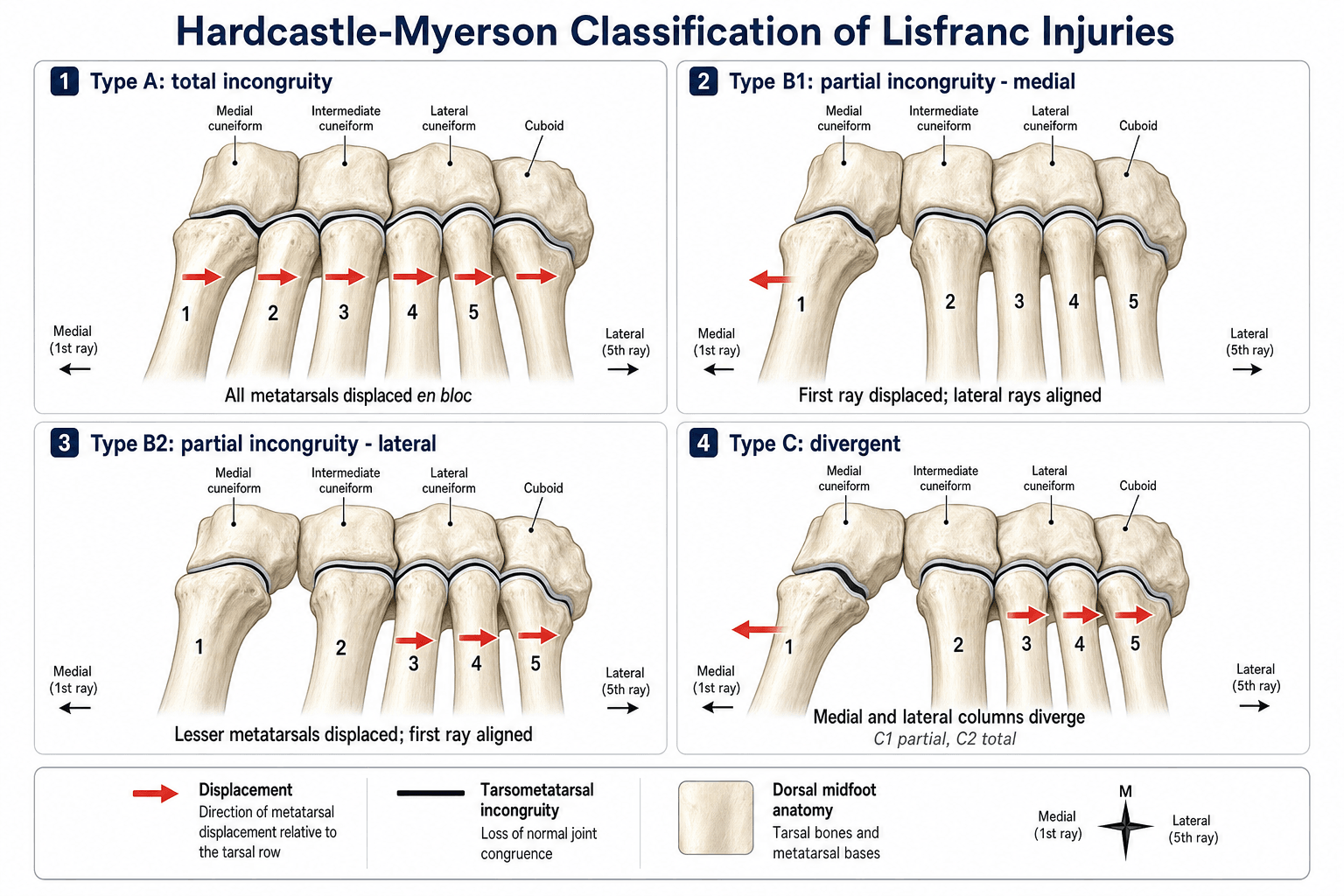
The classification divides tarsometatarsal injuries into three patterns based on the direction and extent of metatarsal displacement relative to the cuneiforms and cuboid.
- Pattern
- Homolateral (total incongruity)
- Displacement
- All five metatarsals displace in the same direction (usually lateral)
- Typical mechanism
- Direct crush or indirect axial load with the foot plantar-flexed
- Pattern
- Isolated medial
- Displacement
- First metatarsal/medial column displaces medially; lesser rays aligned
- Typical mechanism
- Low-energy twisting or inversion
- Pattern
- Isolated lateral
- Displacement
- Second to fifth metatarsals displace laterally; first ray remains stable
- Typical mechanism
- Common pattern; axial load with the foot pronated
- Pattern
- Divergent partial
- Displacement
- Medial column displaces medially, lateral column laterally (partial)
- Typical mechanism
- High-energy; often with intercuneiform instability
- Pattern
- Divergent total
- Displacement
- Complete medial and lateral column dissociation
- Typical mechanism
- Catastrophic energy; frequent associated injuries
ABCThe three main patterns
Hook:A-B-C: All together, Bits isolated, Crash apart.
The second tarsometatarsal joint is the keystone of the Lisfranc complex: the second metatarsal base is recessed proximally between the medial and lateral cuneiforms (in a mortise) and is the primary bony stabiliser of the midfoot. The Lisfranc ligament runs from the medial cuneiform to the second metatarsal base. Loss of this keystone in any pattern mandates anatomic reduction and rigid fixation to prevent late collapse and post-traumatic arthritis.
Nunley-Vertullo classification — athletic midfoot sprains
Hardcastle/Myerson describes frank fracture-dislocations; the Nunley-Vertullo classification is the high-yield system for the subtle midfoot sprain in the athlete, which sits on a spectrum from a partial ligament sprain to frank diastasis and is easy to miss. It stages the injury on weight-bearing radiographs (and historically bone scintigraphy):
- Stage I — sprain, no diastasis and no arch height loss (positive bone scan only): non-operative.
- Stage II — diastasis (1–5 mm) without arch height loss: anatomic reduction and fixation.
- Stage III — diastasis with loss of arch height (loss of the medial longitudinal arch on the lateral view): reduction and fixation.
Nunley and Vertullo achieved an excellent outcome in 93% of 15 athletes with this staged, weight-bearing-based approach — reinforcing that anatomic alignment is the key, and that weight-bearing films are needed to find the injury.
Limitations & modern context
- It is descriptive, not prognostic. Hardcastle/Myerson does not quantify energy or cartilage damage; two type C injuries can have very different outcomes depending on comminution and the soft-tissue envelope.
- CT is essential for surgical planning. Plain radiographs underestimate comminution and intercuneiform instability; coronal and sagittal reformats are obtained before definitive fixation.
- Weight-bearing / stress radiographs are more sensitive than non-weight-bearing films for instability — a static film can look normal in an unstable injury, so a normal NWB film never excludes a Lisfranc injury.
- Primary arthrodesis vs ORIF. For primarily ligamentous injuries a randomised trial (Ly & Coetzee) favoured primary arthrodesis of the medial two/three rays; for bony fracture-dislocations ORIF remains standard, with fusion reserved for irreparable joints. Large Level-1 evidence across all patterns is still limited.
- It does not capture pure ligamentous injuries well — these need weight-bearing/stress imaging or MRI; the Nunley-Vertullo system is better suited to the athletic ligamentous spectrum.
Clinical presentation & examination
A Lisfranc injury follows an axial load on a plantar-flexed foot, a crush, or a low-energy athletic twist, and presents with midfoot swelling and tenderness over the tarsometatarsal joints and pain or inability to bear weight. The classic clinical clue is the plantar ecchymosis sign - bruising on the plantar aspect of the midfoot - which is suggestive of a Lisfranc injury. Stress the midfoot to reproduce pain: the pronation-abduction stress test (stabilise the hindfoot and passively pronate and abduct the forefoot) and the piano-key test (dorsoplantar stress of individual rays) are positive. The key safety message is that this injury is commonly missed - a normal-looking non-weight-bearing film never excludes it - so any midfoot injury with these signs needs a high index of suspicion and weight-bearing/stress views to confirm or refute instability.
Radiographic diagnosis & instability
- AP view: the medial border of the second metatarsal base must be collinear with the medial border of the intermediate (middle) cuneiform. A step-off or a gap of more than 2 mm between the first and second metatarsal bases indicates instability.
- "Fleck sign": a small bony avulsion in the first intermetatarsal space (off the Lisfranc ligament) is pathognomonic.
- Lateral view: the dorsal cortex of the metatarsals should not sit above the dorsal cortex of the corresponding tarsal bone (dorsal displacement = injury).
- Weight-bearing / stress views are essential — a non-weight-bearing film can look normal in a genuinely unstable injury. CT defines comminution and intercuneiform instability before fixation.


Treatment — fix or fuse
- 1Prove instabilityWeight-bearing or stress radiographs (and CT for comminution). A displacement of more than 2 mm, or any divergent/homolateral pattern, is unstable and operative. A truly stable, undisplaced injury can be treated non-operatively in a boot/non-weight-bearing.
- 2Aim for anatomic reduction of the keystoneRestore the second-TMT keystone first. Anatomic reduction is the single strongest predictor of a good outcome — accept nothing over 2 mm.
- 3Fix the reconstructable joint (ORIF)Open reduction with trans-articular screws or dorsal bridging plates across the first, second and third TMT joints. The fourth and fifth (lateral column) tolerate slight incongruity and are often fixed with K-wires, removed later, to preserve mobility.
- 4Fuse the destroyed or ligamentous jointPrimary arthrodesis of the medial two or three rays for an irreparably comminuted joint surface, or for a primarily ligamentous injury, where it gives better and more durable outcomes than ORIF (Ly & Coetzee).
- Recommended treatment
- Anatomic ORIF in essentially all cases
- Fixation method
- Dorsal plates or trans-articular screws across the first, second and third TMT joints
- Key consideration
- Restore the second-TMT keystone first; span with external fixation if swelling is severe
- Recommended treatment
- ORIF if unstable on weight-bearing views
- Fixation method
- Screw or small plate from first metatarsal to medial cuneiform
- Key consideration
- Check for associated intercuneiform/medial column ligamentous injury
- Recommended treatment
- ORIF of the unstable rays
- Fixation method
- Trans-articular screws to the cuneiforms/cuboid; K-wires for the lateral column
- Key consideration
- Fourth and fifth TMT joints tolerate slight incongruity — preserve their motion
- Recommended treatment
- ORIF, or primary arthrodesis of the medial column
- Fixation method
- Medial-column arthrodesis if comminuted; lateral column reduced and fixed
- Key consideration
- High-energy — screen for compartment syndrome and associated fractures
Anatomic reduction of the Lisfranc complex (within 2 mm at the second tarsometatarsal joint) is the strongest predictor of a good outcome; malreduction is the major determinant of post-traumatic arthritis. In Kuo et al.'s ORIF series, post-traumatic osteoarthritis still developed in about a quarter of patients, and the quality of reduction was the major determinant of result. If the joint surface is destroyed, primary arthrodesis gives more predictable pain relief than attempted fixation of comminuted fragments.
Rigid fixation is not the only option. As an alternative to trans-articular screws and dorsal plates, a suture-button device - for example a button-and-cord passed from the medial cuneiform to the second metatarsal base - provides flexible stabilisation of the Lisfranc complex. It is used mainly for purely ligamentous or selected low-grade unstable injuries, and its attractions are avoiding a second operation to remove hardware and preserving some physiological midfoot micromotion. The caution: holding an anatomic reduction is less certain than with rigid fixation in comminuted or grossly unstable patterns, and long-term comparative evidence remains limited - so anatomic reduction of the keystone stays the goal whatever the implant, and rigid fixation or primary arthrodesis remain the choice for the destroyed or high-energy joint.
What it classifies, and why it matters
Lisfranc injuries are uncommon and easily missed, and their results are often unsatisfactory unless the joint is anatomically reduced. Hardcastle's original work (119 patients across five centres) argued that these injuries should be classified by the type of injury rather than the deforming force, and that — whatever the initial severity — prognosis depends on accurate reduction and its maintenance. Myerson later refined the system into the A / B1 / B2 / C1 / C2 subtypes used today and tied each pattern to a fixation strategy.
The classification matters because it organises the surgical decision: type A and C injuries almost always need open anatomic reduction and fixation; type B can be subtle and demands weight-bearing or stress imaging to confirm instability; and a high-energy divergent injury with a destroyed medial column may be better fused than fixed.
Exam & revision
Everything below condenses the classification for revision and viva practice.
- Three patterns: A homolateral (en bloc), B isolated (B1 medial / B2 lateral), C divergent (C1 partial / C2 total).
- The second TMT is the keystone — recessed between the cuneiforms; the Lisfranc ligament runs medial cuneiform → second metatarsal base.
- Instability: more than 2 mm at the first–second metatarsal base, malalignment of the second metatarsal base with the intermediate cuneiform, or the fleck sign — confirmed on weight-bearing/stress films.
- Anatomic reduction is the strongest predictor of outcome; restore the keystone within 2 mm.
- Fix vs fuse: ORIF the reconstructable joint; primary arthrodesis for the destroyed joint or a primarily ligamentous injury (Ly & Coetzee).
- Nunley-Vertullo stages the subtle athletic midfoot sprain (I non-op; II/III reduce + fix).
2 mm and the fleckRadiographic instability
Hook:Two millimetres and a fleck: the AP-view signs that prove a Lisfranc injury is unstable.
Fix most, fuse the destroyed or ligamentousFix or fuse
Hook:Fix most; fuse the destroyed joint or the primarily ligamentous injury.
Exam viva
Practise clinical reasoning and management decisions out loud
“A 28-year-old footballer presents after a twisting injury to the foot. Non-weight-bearing radiographs appear normal, but the weight-bearing AP shows a 3 mm gap between the first and second metatarsal bases. How do you classify and manage this injury?”
“A 45-year-old driver is involved in a high-speed motor vehicle collision. Radiographs show divergent displacement of the first metatarsal medially and the second to fifth metatarsals laterally with comminution of the medial cuneiform. Classify the injury and outline your surgical plan.”
The three patterns (A, B, C)
- Type A: all five metatarsals displaced together (homolateral) — usually lateral
- Type B: partial/isolated — B1 medial column, B2 lateral column
- Type C: divergent — C1 partial, C2 total; medial and lateral columns move apart
Radiographic instability
- Medial border of second metatarsal base aligns with medial border of intermediate cuneiform
- Gap/step-off more than 2 mm (weight-bearing AP) = unstable; fleck sign pathognomonic
- Weight-bearing/stress films + CT mandatory; NWB film can look normal
Fix versus fuse
- ORIF the reconstructable joint; restore the second-TMT keystone within 2 mm
- Primary arthrodesis for irreparable comminution or a primarily ligamentous injury
- Fourth/fifth (lateral column) TMT tolerate slight incongruity — preserve motion
Athletic spectrum (Nunley-Vertullo)
- Stage I: sprain, no diastasis, no arch loss → non-operative
- Stage II: diastasis without arch loss → reduce + fix
- Stage III: diastasis with arch-height loss → reduce + fix
Evidence
Injuries to the tarsometatarsal joint. Incidence, classification and treatment
- Retrospective study of 119 Lisfranc injuries collected from five centres.
- Proposed classifying these injuries by the type of injury rather than the deforming force — the original three-pattern (homolateral / isolated / divergent) classification.
- Whatever the initial severity, prognosis depended on accurate reduction and its maintenance.
Fracture dislocations of the tarsometatarsal joints: end results correlated with pathology and treatment
- 76 Lisfranc fracture-dislocations in 72 patients; 49% achieved a good/excellent result and the quality of the initial reduction was the major determinant of outcome.
- Refined Hardcastle into the A / B1 / B2 / C1 / C2 subtypes and emphasised the second-TMT keystone.
- Displacement greater than 2 mm or a talometatarsal angle greater than 15° after closed reduction mandated open reduction.
According to PubMed, the original classification and the reduction-prognosis principle come from Hardcastle et al. 1982 (DOI); the A/B/C subtype modification and the over-2-mm / talometatarsal-angle thresholds from Myerson et al. 1986 (DOI); the ORIF outcome data (AOFAS 77, 25% arthritis, reduction the key determinant) from Kuo et al. 2000 (DOI); the primary-arthrodesis-vs-ORIF randomised data for ligamentous injuries from Ly & Coetzee 2006 (DOI); and the athletic midfoot-sprain staging from Nunley & Vertullo 2002 (DOI). The keystone anatomy and fix-versus-fuse principles are standard foot-and-ankle teaching.