Mature Bone Formation in Soft Tissues
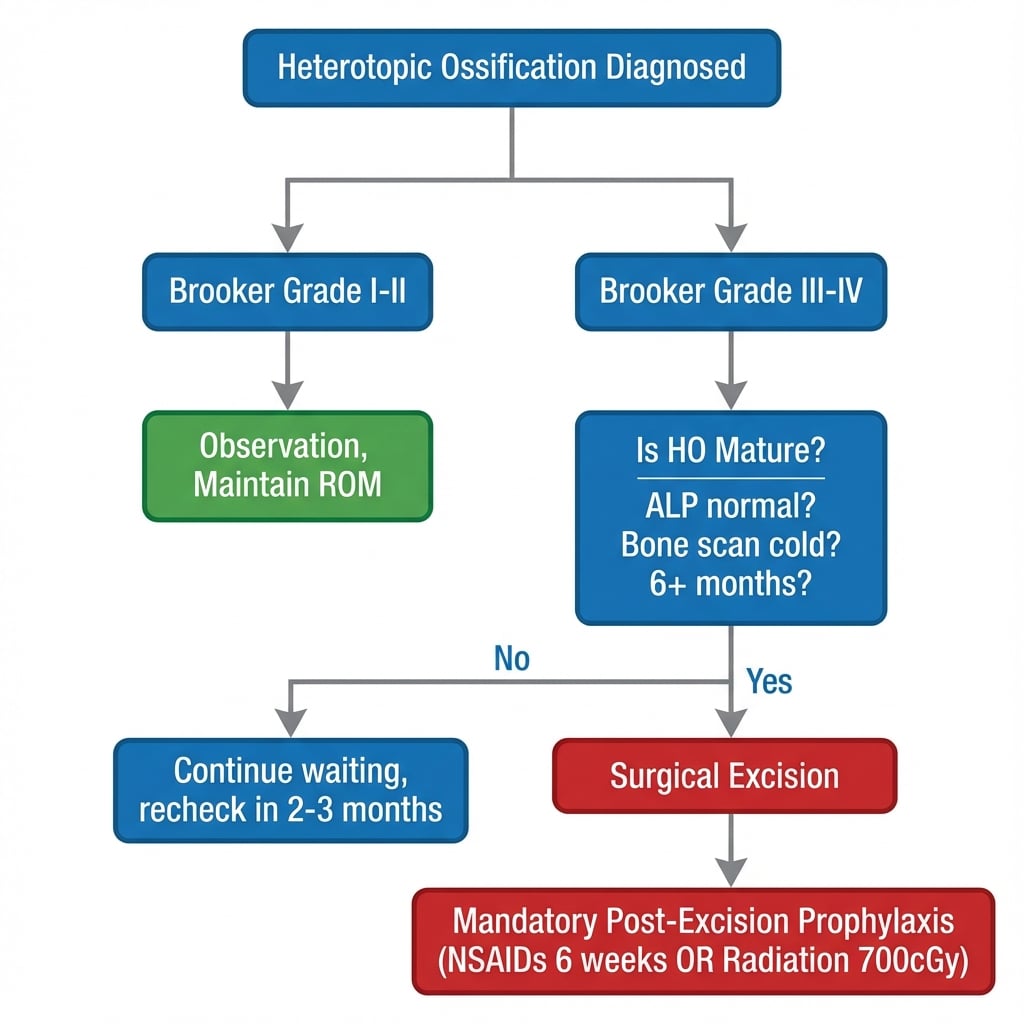
- Brooker Grade III-IV = clinically significant (affects ROM)
- Prevention more effective than treatment (NSAIDs or radiation)
- Wait 6+ months for HO to mature before excision
- High-risk: head injury, burns, spinal cord injury, previous HO
- Recurrence rate significant without post-excision prophylaxis
- “Indomethacin 75mg daily x 6 weeks is classic prophylaxis regimen
- “Single-dose radiation (700cGy) within 72h is alternative to NSAIDs
- “Check ALP to confirm HO maturation before excision
- “Post-excision prophylaxis is MANDATORY to prevent recurrence
Prophylaxis is far more effective than treatment. NSAIDs or radiation within 72h of surgery reduces HO by 80%. Know the regimens.
Do NOT excise immature HO. Wait 6-12 months until bone is mature (normal ALP, cold bone scan). Early excision = high recurrence.
Grade III-IV = clinically significant. Only these grades typically affect function. Grade I-II usually observed.
Prophylaxis after excision is MANDATORY. Recurrence rate 50%+ without it. Same regimens as primary prevention.
- Prevention
- Indomethacin 75mg x 6 weeks OR radiation 700cGy
- Treatment
- Excision if Grade III-IV
- Pearl
- Start prophylaxis within 24-72h
- Prevention
- VERY high risk - prophylaxis mandatory
- Treatment
- Wait 12+ months for maturity
- Pearl
- Often bilateral, may be severe
- Prevention
- Prophylaxis post-excision
- Treatment
- Surgical excision when mature
- Pearl
- Check ALP and bone scan before surgery
- Prevention
- None needed if primary prevention given
- Treatment
- Observation only
- Pearl
- Rarely progresses if stable at 6 months
HABITRisk Factors for HO
Hook:Patients with these HABITs are at high risk for growing bone where it shouldn't be!
Overview and Epidemiology
Heterotopic ossification (HO) is the formation of mature lamellar bone in extra-skeletal soft tissues (typically muscle and periarticular connective tissue). It is NOT dystrophic calcite or myositis ossificans traumatica (which involves muscle injury specifically).
- Total hip arthroplasty: 10-50% radiographic, 3-5% symptomatic
- Acetabular fractures: 20-40%
- Elbow surgery: 3-20%
- Spinal cord injury: 20-30%
- Traumatic brain injury: 10-20%
- Males more commonly affected
- Previous HO (strongest predictor - 50% recurrence)
- Traumatic brain injury
- Spinal cord injury
- Burns greater than 20% TBSA
- Ankylosing spondylitis
- Diffuse idiopathic skeletal hyperostosis (DISH)
- Hypertrophic osteoarthritis
Pathophysiology
HO requires three elements: (1) osteogenic precursor cells, (2) an inducing agent/signal, and (3) a permissive environment. Understanding this guides prevention strategies.
Osteogenic Precursor Cells
- Mesenchymal stem cells (MSCs) in muscle and connective tissue
- Circulating osteoprogenitor cells
- Local fibroblasts with osteogenic potential
- Endothelial cells via endothelial-to-mesenchymal transition
MSCs differentiate into osteoblasts under appropriate signals, laying down osteoid which then mineralizes to form mature bone.
Multiple mechanisms: (1) Loss of inhibitory neural signals to bone turnover, (2) Release of brain-derived osteogenic factors into circulation, (3) Systemic inflammatory response, (4) Prolonged immobilization. Head-injured patients can develop HO at sites remote from any surgery or local trauma.
Fibrodysplasia ossificans progressiva (FOP) is a rare autosomal-dominant disorder caused by a gain-of-function mutation in ACVR1/ALK2 (a BMP type I receptor), in which connective tissue progressively turns into bone. The pathognomonic clue is present at birth, before any ossification: a congenital malformation of the great toes (short, valgus, monophalangic hallux). Affected children then suffer episodic painful soft-tissue "flares" that ossify, progressing in a characteristic pattern — axial to appendicular, proximal to distal, and cranial to caudal — eventually causing widespread ankylosis. The cardinal rule is that trauma triggers ossification: biopsy, intramuscular injections (including some immunisations), dental blocks and surgical excision all provoke catastrophic flares, so surgery and biopsy are contraindicated. Recognise FOP clinically (great-toe sign plus flares), avoid the knife, and manage with flare protection and emerging ACVR1-targeted therapy (e.g. palovarotene) — never the NSAID/radiation/excision pathway used for acquired HO.
Classification Systems
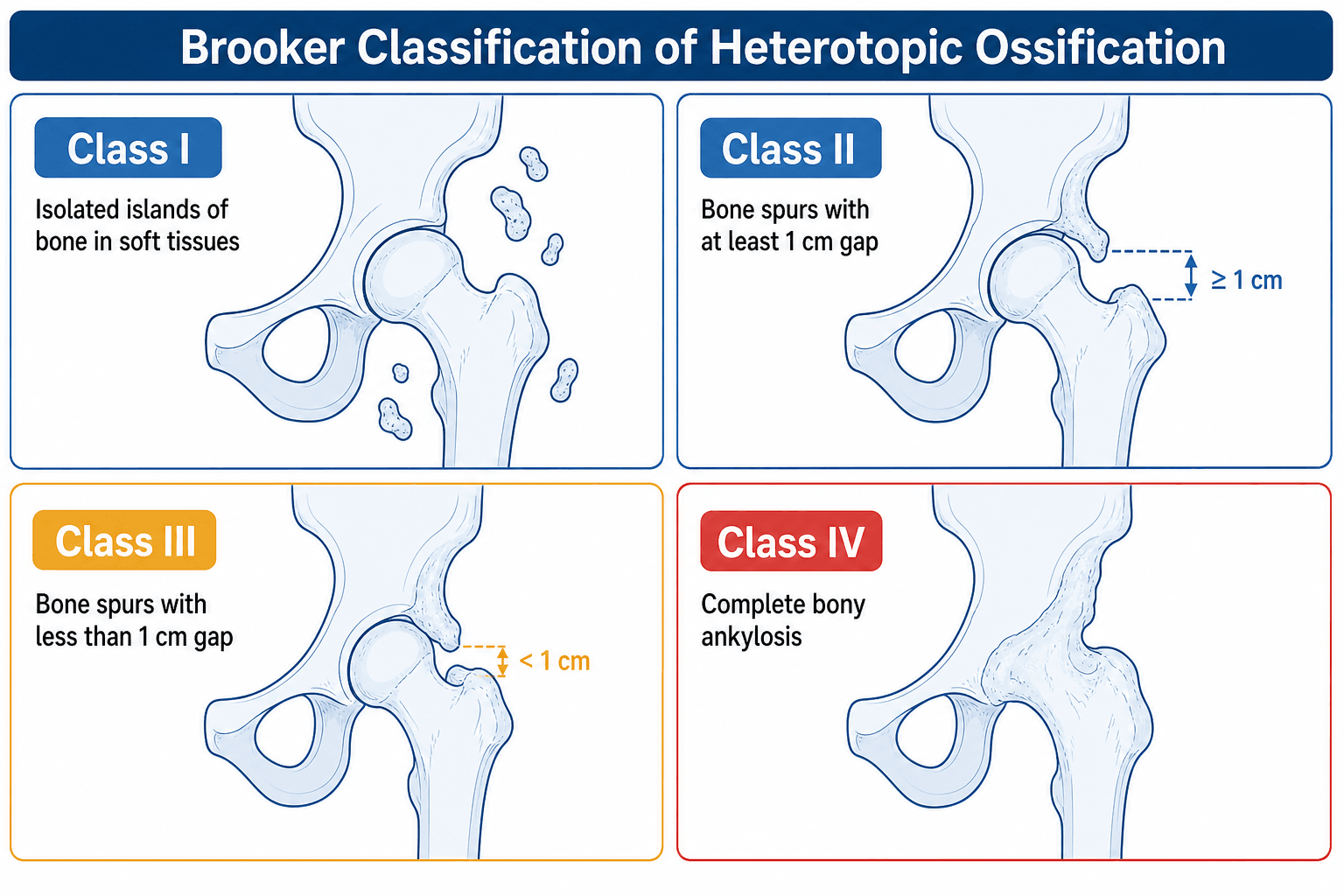
Brooker Classification (1973)
Most commonly used - for hip HO
- Description
- Islands of bone within soft tissues about the hip
- Clinical Significance
- Usually asymptomatic
- Description
- Bone spurs from pelvis or femur with gap greater than 1cm
- Clinical Significance
- Mild, usually asymptomatic
- Description
- Bone spurs from pelvis or femur with gap less than 1cm
- Clinical Significance
- Moderate - may affect ROM
- Description
- Apparent bone ankylosis of the hip
- Clinical Significance
- Severe - significant functional impairment
Clinical Rule: Grades I-II are usually observed. Grades III-IV typically require surgical consideration.
1-2-3-4Brooker Classification
Hook:1-Islands, 2-Big gap, 3-Small gap, 4-Fused (Think: the gap gets smaller as grade increases!)
Clinical Assessment
- Previous surgery/trauma to area
- Risk factors (head injury, SCI, burns)
- Timeline of symptom development
- Previous HO at any site
- Current medications (esp. NSAIDs)
- Functional limitations
- Range of motion - key functional assessment
- Palpable firm mass (late finding)
- Local warmth and swelling (early/active phase)
- Pain on movement (especially at end-range)
- Skin changes over lesion
- Neurovascular status (rare compression)
Clinical Stages of HO Development
Natural History
Local warmth, swelling, pain. May mimic infection or DVT. X-ray usually negative. Bone scan may be positive.
Early mineralization begins. Soft tissue mass becomes palpable. X-ray shows faint calcification. ALP elevated.
Progressive ossification and organization. ROM progressively limited. X-ray shows maturing bone. ALP peaks then normalizes.
Bone fully mature with cortical margins. ALP normal. Bone scan cold or minimal uptake. This is the safe window for excision.
Early HO can mimic: DVT (swelling, warmth), Infection (local inflammation), Stress fracture, Tumor (mass lesion). Bone scan and serial X-rays help differentiate. Don't miss DVT - consider duplex if lower limb.
Differential Diagnosis
- Discriminating features
- Calf/limb swelling and warmth, often without a discrete mass; risk after surgery/immobility
- Key investigation
- Duplex ultrasound; D-dimer
- Pitfall to avoid
- Anticoagulating presumed DVT when it is early HO - and vice versa, missing a real DVT
- Discriminating features
- Fever, raised CRP/ESR, wound discharge, rest pain
- Key investigation
- CRP/ESR, joint aspiration, cultures
- Pitfall to avoid
- Attributing post-THA stiffness to HO without excluding infection
- Discriminating features
- Enlarging deep mass, atypical site, no preceding trauma
- Key investigation
- MRI with contrast; biopsy if features atypical
- Pitfall to avoid
- Biopsying a 'zonal' maturing HO and over-calling malignancy
- Discriminating features
- Follows discrete muscle injury; classic peripheral (zonal) mineralisation maturing outward
- Key investigation
- Serial radiographs showing zoning
- Pitfall to avoid
- Early biopsy mimics sarcoma histologically - wait and image
- Discriminating features
- Amorphous calcium without organised trabeculae; metabolic context (renal failure, hypercalcaemia)
- Key investigation
- Calcium/phosphate, renal function
- Pitfall to avoid
- Confusing soft-tissue calcification with true lamellar HO
- Discriminating features
- Periarticular lobulated calcific masses, often familial/renal
- Key investigation
- Radiograph, phosphate profile
- Pitfall to avoid
- Treating as HO and giving futile NSAID/radiation prophylaxis
Myositis ossificans traumatica is the post-traumatic, muscle-specific form of heterotopic ossification (classically quadriceps or brachialis after a contusion or dislocation). Its defining feature is the zonal phenomenon: the lesion matures from the outside in, so a mature, well-organised, mineralised bony rim surrounds an immature, cellular centre — the exact reverse of a soft-tissue sarcoma, which is most cellular and aggressive at its periphery. Radiographically, peripheral mineralisation appears at about 3 to 6 weeks and a corticated rim defines the lesion by 6 to 8 weeks; serial films showing maturing, sharply-marginated peripheral bone are reassuring. The critical trap is that an early biopsy (before zoning) shows hypercellular, mitotically active osteoid that is histologically indistinguishable from osteosarcoma — so this is a classic "do-not-biopsy-early" lesion. Wait, image serially, and biopsy only if the appearance is atypical or progressive.
Investigations
Radiological Investigations
- Timing
- From 3-6 weeks
- Findings
- Calcification, bone formation, Brooker grading
- Role
- Primary imaging, classification
- Timing
- Mature HO
- Findings
- Precise anatomy, surgical planning
- Role
- Pre-operative planning
- Timing
- Early (1-2 weeks)
- Findings
- Increased uptake (hot) = active
- Role
- Assess maturity for timing of surgery
- Timing
- Early phase
- Findings
- Soft tissue edema, early changes
- Role
- Rarely needed, can show early HO
Maturity for surgery: Bone scan should be "cold" (no increased uptake) or minimal activity. This indicates mature HO safe for excision.
Before excising HO, confirm maturity with: (1) Normal ALP for at least 2-3 months, (2) Cold or inactive bone scan, (3) Cortical margins on X-ray, (4) Stable radiographic appearance on serial imaging. Operating on immature HO dramatically increases recurrence.

Management
Non-Operative Management
Brooker Grade I-II, minimal functional limitation, still maturing.
- Pain management
- Physiotherapy to maintain ROM (gentle - not forced)
- Monitor with serial X-rays
- Wait and watch - some HO resorbs partially
Aggressive physiotherapy does NOT cause HO (old myth) BUT forced ROM through established HO can cause fracture or bleeding.
The surgical field is highly osteogenic after excision. Without prophylaxis, recurrence rate exceeds 50%. Both NSAIDs and radiation are effective. Begin within 24-72 hours of surgery.
Surgical Technique Considerations
Hip HO Excision
- Use same approach as index surgery if possible
- Lateral/anterolateral for most THA HO
- Consider dual approaches for circumferential HO
Identify and protect neurovascular structures first (sciatic nerve at risk posteriorly). Excise HO to restore bone-capsule plane. Release contracted capsule. Ensure full ROM before closure.
Complications
Complications of HO and Its Treatment
- HO-Related
- Grade IV HO
- Surgery-Related
- -
- Management
- Surgical excision when mature
- HO-Related
- Rare but serious
- Surgery-Related
- -
- Management
- Urgent excision may be needed
- HO-Related
- -
- Surgery-Related
- 20-30% with prophylaxis
- Management
- Re-excision possible
- HO-Related
- -
- Surgery-Related
- During excision (sciatic, ulnar)
- Management
- Careful identification, protect
- HO-Related
- -
- Surgery-Related
- During manipulation
- Management
- Gentle technique, staged if needed
- HO-Related
- -
- Surgery-Related
- Promotes recurrence
- Management
- Meticulous hemostasis, drain
Sciatic nerve injury is a real risk during hip HO excision, especially for posterior/circumferential HO. Nerve may be encased in bone. Identify nerve early, trace proximally from known anatomy, and protect throughout. Neuromonitoring is advisable for complex cases.
Postoperative Care
Post-Excision Rehabilitation
Rehabilitation Protocol
Begin CPM if available. Active-assisted range of motion exercises. Maintain drains until output minimal.
Active ROM exercises. Physiotherapy daily initially. Focus on maintaining surgical gains. Weight bearing as tolerated (unless concurrent fracture).
Continue prophylaxis for full 6 weeks. Progressive strengthening. Functional training. Monitor ROM closely.
Ongoing home exercise program. Serial X-rays to monitor for recurrence. Return to functional activities.
Continuous passive motion (CPM) may help maintain ROM gains after excision, especially for elbow HO. Evidence is mixed but commonly used. Start immediately post-operatively. Goal is to maintain ROM achieved at surgery.
Outcomes and Prognosis
Prognostic Factors
- Isolated HO without neurological cause
- Good ROM before HO developed
- Mature HO at time of excision
- Prophylaxis given post-excision
- Motivated patient for rehabilitation
- Neurogenic HO (TBI, SCI)
- Previous recurrence
- Circumferential HO
- Poor pre-HO ROM baseline
- Non-compliance with physiotherapy
Prevention Strategies
Prophylaxis reduces HO incidence by 70-80%. Once HO is established, only surgical excision can restore motion, with significant morbidity and recurrence risk. Prevention is the key strategy.
NSAID Prophylaxis
Mechanism: Inhibits prostaglandin synthesis, blocking osteogenic signal.
- Dose
- 75mg daily (or 25mg TDS)
- Duration
- 6 weeks
- Notes
- Classic regimen - best evidence
- Dose
- 500mg BD
- Duration
- 6 weeks
- Notes
- Alternative if indomethacin not tolerated
- Dose
- 200mg daily
- Duration
- 6 weeks
- Notes
- COX-2 selective - fewer GI effects
- Dose
- 600-900mg daily
- Duration
- 6 weeks
- Notes
- Less effective than other NSAIDs
GI ulcer/bleed history, renal impairment, anticoagulant use, fracture healing concerns.
Begin within 24-48 hours of surgery. Delayed start reduces efficacy.
NSAIDs preferred: Most common, convenient, cheap. Use when no contraindications. Radiation preferred: NSAID contraindications (GI, renal), fracture healing concerns, difficult-to-shield anatomy. Both equally effective: No significant difference in HO prevention rates (70-80% reduction).
RINDHO Prevention Protocol
Hook:Use RIND to protect against bone growing in the wrong place - Radiation or Indomethacin for Necessary Duration!
Guidelines, Registries & Global Practice
- THA: 10-50% radiographic, 3-5% symptomatic worldwide
- Acetabular fracture (posterior/extensile approach): 20-40%, the highest-risk elective indication for prophylaxis
- Elbow trauma/fracture-dislocation: 3-20%
- Combat/blast amputations: up to 60-65% (high-energy soft-tissue injury)
- Spinal cord injury: 20-30%; traumatic brain injury: 10-20%
- Male predominance across most series
- Arthroplasty registries (NJR, AOANJRR, AJRR, SHAR) do not code HO routinely, so registry-level incidence is under-captured - cohort and trial data remain the reference
- Registry signal is indirect: HO contributes to stiffness/dissatisfaction and a minority of revisions for impingement or limited ROM
- Direct anterior and tissue-sparing hip approaches report lower HO than extensile/posterior exposures
Side-by-Side Guidance on Prophylaxis
- Position on routine prophylaxis
- Selective - target high-risk, not routine THA
- Preferred modality
- NSAID first-line; radiation if contraindicated
- Practical note
- Aligns with HIPAID showing no functional gain from routine NSAIDs
- Position on routine prophylaxis
- Risk-stratified; emphasis on documentation and consent
- Preferred modality
- Indomethacin or COX-2; radiation reserved
- Practical note
- Radiotherapy access via oncology pathways can delay the 72h window
- Position on routine prophylaxis
- Recommend prophylaxis after high-risk acetabular fixation
- Preferred modality
- Single-dose radiation or indomethacin
- Practical note
- Avoid indomethacin where concurrent long-bone fractures must unite
- Position on routine prophylaxis
- NSAIDs/radiation NOT used; surgery contraindicated (triggers flares)
- Preferred modality
- ACVR1-targeted therapy (e.g. palovarotene), flare prophylaxis
- Practical note
- Recognise FOP - great toe malformation plus flares; do NOT biopsy or excise
- Ready access to single-dose linear-accelerator radiotherapy within 24-72h
- Tc-99m bone scan / SPECT-CT and serial CT for maturity and surgical planning
- Intra-operative neuromonitoring for complex peri-articular excision
- NSAID prophylaxis dominates - cheap, oral, no specialised equipment
- Plain radiographs and serum ALP substitute for bone scan to judge maturity
- Prevention emphasised because revision/excision capacity is scarce
Record risk factors and the prophylaxis decision. Offering prophylaxis to genuinely high-risk patients is expected practice globally; consent for HO excision must include recurrence risk, neurovascular injury, and the need for post-operative prophylaxis.
Controversies and Areas of Uncertainty
Radiographic HO falls with prophylaxis, but the HIPAID RCT showed no functional benefit and increased bleeding from routine NSAIDs after hip replacement. Most authorities now restrict prophylaxis to high-risk patients rather than treating every arthroplasty.
Meta-analysis suggests postoperative radiation is modestly more effective for Brooker III-IV, but the absolute difference is around 1%. Cost, access, the 72h window, and fracture-healing concerns usually decide, not efficacy alone.
The old dogma of waiting for a "cold" bone scan and normal ALP is increasingly challenged - several series report safe early excision of mature-appearing HO with prophylaxis, particularly at the elbow, to limit secondary contracture. Bone scan/ALP remain imperfect maturity markers.
ACVR1/BMP-pathway and retinoic-acid-receptor agents (e.g. palovarotene) are validated in FOP and under study for acquired/neurogenic HO, raising the prospect of biologic prevention beyond NSAIDs and radiation.
MCQ Practice Points
Q: What is the Brooker Grade III classification for heterotopic ossification of the hip? A: Bone spurs from pelvis or femur with a gap of less than 1 cm. Grade I = islands, Grade II = gap greater than 1cm, Grade III = gap less than 1cm, Grade IV = ankylosis.
Q: What is the standard NSAID prophylaxis regimen for prevention of heterotopic ossification after high-risk hip surgery? A: Indomethacin 75mg daily (or 25mg TDS) for 6 weeks, starting within 24-48 hours of surgery. Reduces HO by 70-80%.
Q: When is the optimal timing for surgical excision of heterotopic ossification? A: Minimum 6 months after formation, when ALP has normalized and bone scan is cold. For neurogenic HO (TBI/SCI), wait 12+ months. Early excision of immature HO leads to high recurrence.
Q: What is the strongest risk factor for developing heterotopic ossification after hip surgery? A: Previous HO at any site (50% recurrence risk). Other major risk factors: TBI, SCI, burns, ankylosing spondylitis, DISH.
Q: What is the recommended single-dose radiation protocol for HO prophylaxis? A: 700-800 cGy within 72 hours of surgery (preferably within 24h). Single dose is as effective as fractionated. Pre- or post-operative delivery equally effective.
Q: What is the recurrence rate after surgical excision of HO without prophylaxis? A: Greater than 50%. With prophylaxis (NSAIDs or radiation), recurrence is 20-30%. Post-excision prophylaxis is mandatory.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 62-year-old man is 4 months post total hip arthroplasty. He had a history of ankylosing spondylitis. He now presents with progressive stiffness of the hip and reduced range of motion from 100 degrees flexion at 6 weeks to 60 degrees now. How would you assess and manage this patient?”
“You are performing a total hip arthroplasty on a 58-year-old woman who had previous heterotopic ossification after her contralateral THA which required excision. What would be your prophylaxis strategy?”
“A 28-year-old man who sustained a severe traumatic brain injury 8 months ago now presents with gradually worsening elbow stiffness bilaterally. He has a functional arc of only 30-80 degrees flexion on the right and the left elbow is nearly ankylosed. X-rays show extensive heterotopic ossification at both elbows. How would you manage this patient?”
Key Facts
- 10-50% radiographic after THA, 3-5% symptomatic
- Brooker III-IV = clinically significant
- Prevention reduces incidence by 70-80%
- Previous HO = strongest risk factor (50% recurrence)
Brooker Classification
- Grade I: Islands of bone in soft tissue
- Grade II: Bone spurs, gap greater than 1cm
- Grade III: Bone spurs, gap less than 1cm
- Grade IV: Apparent ankylosis
Prevention
- Indomethacin 75mg daily x 6 weeks
- OR Radiation 700cGy within 72h
- Start within 24-48 hours of surgery
- Both equally effective
Surgical Excision
- Wait 6+ months for maturity (12+ for neurogenic)
- Confirm normal ALP, cold bone scan
- Post-excision prophylaxis MANDATORY
- Recurrence 20-30% with prophylaxis, 50%+ without
Risk Factors (HABIT)
- Head injury / Hypertrophic OA
- Ankylosing spondylitis / DISH
- Burns / Bilateral hip OA
- Previous HO / Invasive surgery
- Trauma / Spinal cord injury
Evidence Base and Key Trials
Brooker - Original Classification of Ectopic Ossification After THR
- Original description of the four-grade radiographic classification still in universal use
- Grade I islands of bone, Grade II spurs with gap greater than 1cm, Grade III spurs with gap less than 1cm, Grade IV apparent ankylosis
- Defined incidence and a reproducible AP-pelvis grading method after total hip replacement
Kaliya-Perumal Review - Pathophysiology of HO and FOP (ACVR1/BMP)
- Acquired HO is a two-step process: inflammation/tissue injury, then endochondral bone formation
- Dysregulated BMP signalling is central; gain-of-function ACVR1 (ALK2) mutations cause fibrodysplasia ossificans progressiva
- Explains why anti-inflammatory and prostaglandin-blocking strategies (NSAIDs) attenuate HO
- ACVR1/BMP-targeted agents (e.g. palovarotene) are in clinical development for genetic HO