Retrograde and Precarious
- The Medial Femoral Circumflex Artery (MFCA) is the primary blood supply to the adult femoral head.
- Blood flow is RETROGRADE: From the base of the neck up to the head.
- The Lateral Epiphyseal Artery (from the MFCA) supplies the majority of the weight-bearing dome.
- Intracapsular fractures disrupt the ascending retinacular vessels, risking Avascular Necrosis (AVN).
- The artery of the Ligamentum Teres (from Obturator) is negligible in adults but important in children.
- “The Posterior Superior retinacular arteries are the most critical group.
- “In children, the physis acts as a barrier, isolating the epiphysis from metaphyseal supply.
- “Displaced intracapsular fractures carry a substantial AVN risk (~15-30% in young adults even with anatomic fixation).
- “The MFCA runs between the Pectineus and Iliopsoas (or Quad Femoris) posteriorly.
MFCA Injury.
- The MFCA runs superior to the Quadratus Femoris and deep to the Piriformis tendon.
- Risk: Taking down the Quadratus Femoris too proximally or extending the piriformis release into the capsule can damage the main trunk.
- Result: Complete AVN of the head.
Thread-Out Effect.
- Placing screws in the Posterior-Superior quadrant of the neck.
- Risk: Threads exiting the cortex can catch and tear the retinacular vessels in the synovial reflection (Weitbrecht's retinacula).
- Rule: Stay central or inferior-posterior where safe.
- Origin
- Profunda Femoris
- Territory
- Superolateral Head (Weight bearing)
- Importance
- CRITICAL (80%)
- Origin
- Profunda Femoris
- Territory
- Anterior Neck
- Importance
- Minor
- Origin
- Internal Iliac
- Territory
- Fovea
- Importance
- Negligible (Adult)
- Origin
- Internal Iliac
- Territory
- Posterior Capsule
- Importance
- Minor
AIM for PSRetinacular Groups
Hook:Always AIM for the Posterior-Superior group (to protect or avoid).
F-L-I-MCruciate Anastomosis
Hook:The Anastomosis at the level of the Lesser Trochanter ('Film').
PIPMFCA Course
Hook:The path of the most important artery.
Overview
The vascular supply to the femoral head is unique because it is retrograde. Vessels travel up the femoral neck to reach the articular surface. This precarious arrangement means that any fracture of the femoral neck is likely to sever these vessels, leaving the head without a valid blood supply.
Neurovascular
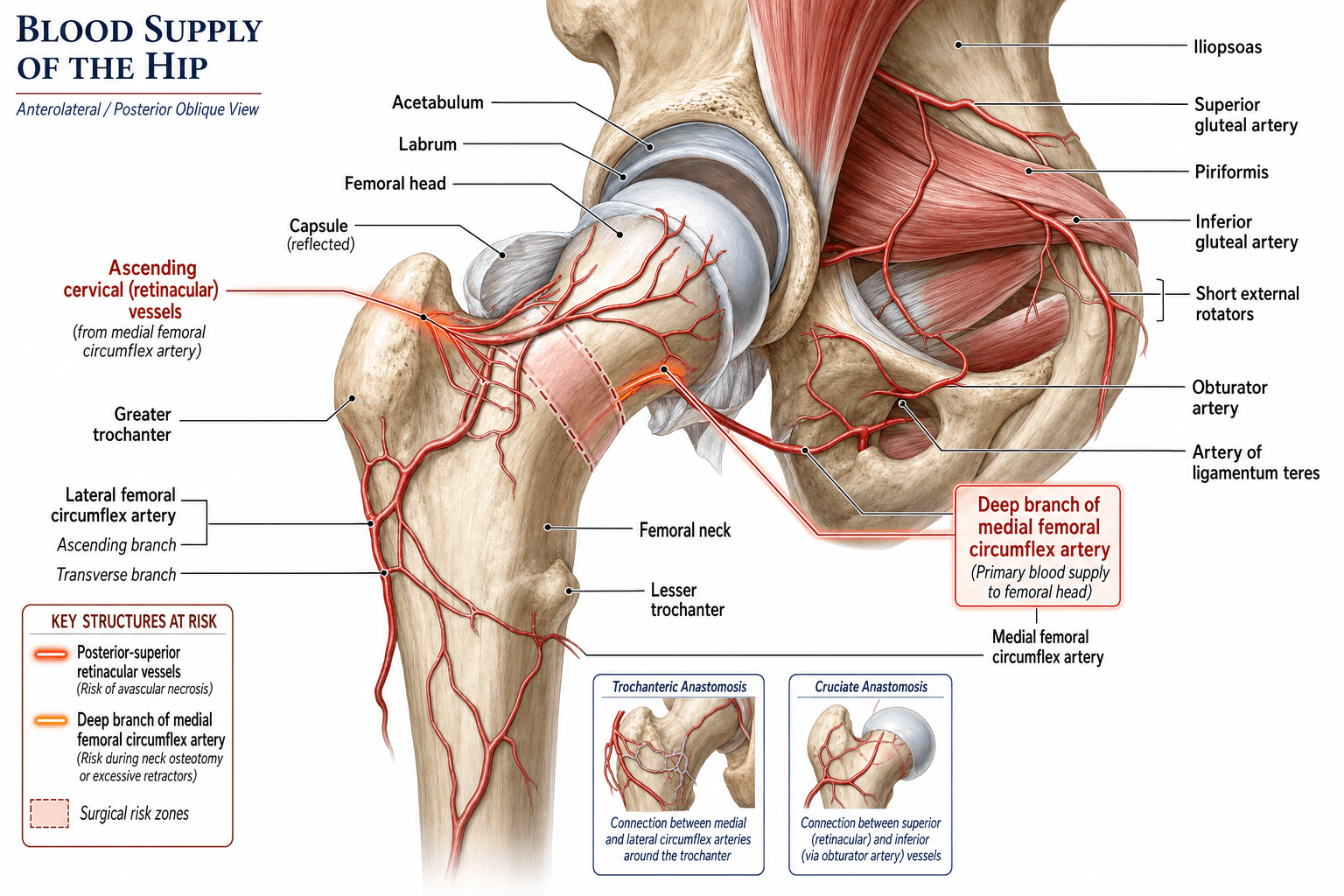
Medial Femoral Circumflex Artery (MFCA)
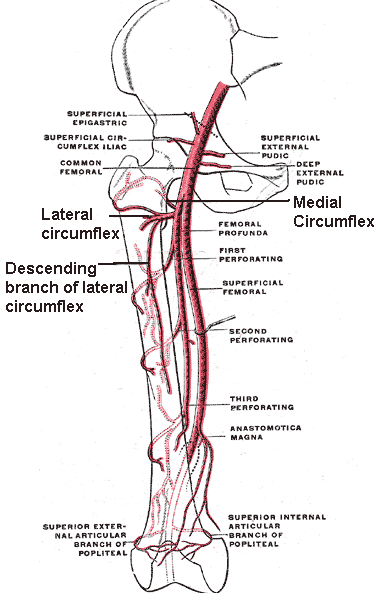
- Origin: Usually from the Profunda Femoris (posteriorly), but can arise directly from the Common Femoral.
- Course: Winds medially around the femur, passing between the Pectineus and Iliopsoas. It then passes Superior to the Adductor Brevis and Inferior to the Obturator Externus.
- Deep Branch: The main trunk runs deep to the Quadratus Femoris.
- Terminal Branch: Gives off the "Lateral Epiphyseal Artery" (See Retinacular system).
This artery supplies the posterior, superior, and lateral aspects of the head (the weight-bearing zone).
Vascular Rings
The concept of "Rings" helps conceptualize the flow.
1. Extracapsular Ring
- Location: Base of the Neck.
- Formed by: Anastomosis of MFCA (Posteriorly) and LFCA (Anteriorly).
- Function: The base station. If disrupted (Basicervical fracture), supply fails.
This ring ensures redundancy from both medial and lateral sources.
Pathology: AVN
Avascular Necrosis (Osteonecrosis)
- Mechanism: Ischemia leads to death of osteocytes (within 12-24 hours).
- Creeping Substitution: The body attempts to revascularize and remodel necrotic bone. New woven bone is laid on dead trabeculae.
- Collapse: If the remodeling phase weakens the structure (resorption exceeds formation), the subchondral bone collapses (Crescent Sign).
- Result: Articular incongruity and secondary OA.
The critical "point of no return" is often debated, but prompt reduction (within 6 hours? 24 hours?) is advocated for young patients.
VITTAVN Pathophysiology
Hook:Mechanisms of cell death.
Classification Relevance
Garden Classification (Femoral Neck Fractures)
Directly correlates with vascular integrity.
- Grade I (Valgus Impacted): Trabeculae angulated. Minimal displacement. Vessels likely Intact. Risk of AVN is low (less than 15%).
- Grade II (Complete, Undisplaced): Break is complete but anatomical reduced. Vessels Intact/Kinked.
- Grade III (Complete, Partially Displaced): Vessels Tethered/Torn. Posterior retinaculum may still be intact.
- Grade IV (Complete, Fully Displaced): Head is dissociated. Vessels Torn. Risk of AVN is high.
Clinical decision making (Fix vs Replace) is driven by this predicted vascular survival. Caveat: the Garden grade has only moderate interobserver reliability, and many surgeons collapse it to a binary undisplaced vs displaced decision in practice.
In children the AVN risk tracks the fracture level (and so the vessels divided), graded by the Delbet classification — the paediatric counterpart to Garden, with AVN risk falling as the fracture moves distally away from the retinacular entry point:
- Type I — transepiphyseal (through the physis, with or without dislocation of the epiphysis): highest AVN risk (up to roughly 80-100 percent when the epiphysis is dislocated), as the epiphyseal vessels are stripped.
- Type II — transcervical (mid-neck): the commonest type; high AVN risk (roughly 40-50 percent).
- Type III — cervicotrochanteric / basicervical (base of neck): lower AVN risk (roughly 20-30 percent).
- Type IV — intertrochanteric (extracapsular): lowest AVN risk (under about 10 percent), as the retinacular supply is largely spared.
The principle mirrors the adult: the more proximal the fracture, the more of the ascending retinacular supply is lost. Anatomic reduction, stable fixation and decompression of the capsular haematoma are advocated to limit AVN.
Clinical Assessment
Fracture Neck of Femur.
- Shortened and Externally Rotated leg.
- Indicates displacement (Garden III/IV).
- Implication: The posterior retinaculum is likely torn via the rotation.
Posterior Dislocation.
- Dashboard injury.
- The head is forced out of the acetabulum posteriorly.
- Vascular Risk: Tensions/Tears the MFCA and Ligamentum Teres.
- Urgency: Reduced immediately to restore flow (reduce tamponade/kinking).
Investigations
Technetium-99m
- Mechanism: Uptake depends on blood flow and osteoblastic activity.
- Cold Spot: Indicates avascularity (early phase).
- Hot Spot: Indicates revascularization/healing (late phase).
Useful to predict head viability post-fracture, but rarely changes acute management.
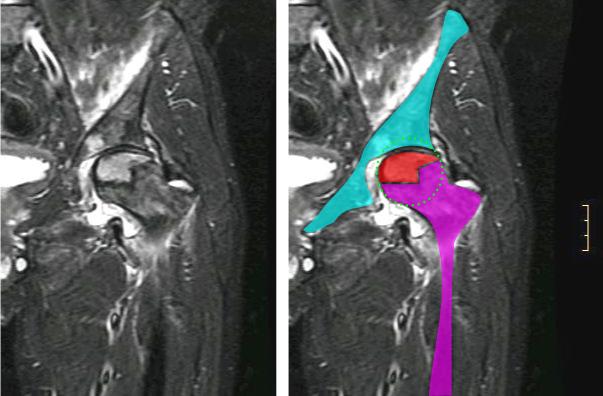
Differential Diagnosis of Femoral Head Marrow Signal / Osteonecrosis
When a young or middle-aged patient presents with hip pain and abnormal femoral head marrow on MRI, the following entities mimic or overlap with post-traumatic AVN. Distinguishing them changes management.
- Typical Patient / Trigger
- After displaced #NOF or dislocation
- Key Distinguishing Feature
- Vascular disruption of retinacular vessels; double-line sign on T2
- Course
- Risk of segmental collapse (crescent sign)
- Typical Patient / Trigger
- Steroids, alcohol, sickle cell, SLE, caisson disease
- Key Distinguishing Feature
- Often bilateral; serpentine demarcation line
- Course
- May collapse if untreated
- Typical Patient / Trigger
- Middle-aged men, pregnant women (3rd trimester)
- Key Distinguishing Feature
- Diffuse marrow oedema WITHOUT focal subchondral line
- Course
- Self-limiting, resolves in months
- Typical Patient / Trigger
- Elderly, osteoporotic, low bone mass
- Key Distinguishing Feature
- Low-signal subchondral line parallel to endplate, oedema
- Course
- Can mimic and progress to collapse
- Typical Patient / Trigger
- Fever, raised inflammatory markers, child or immunocompromised
- Key Distinguishing Feature
- Joint effusion, synovitis, restricted aspiration
- Course
- Surgical emergency
Management Strategy
Strategy for Vascular Preservation
- Injury
- Undisplaced
- Strategy
- Urgent Fixation (Cannulated Screws)
- Injury
- Displaced
- Strategy
- Emergent Reduction + Fixation (preserve head)
- Injury
- Undisplaced
- Strategy
- Fixation (Screws/DHS)
- Injury
- Displaced
- Strategy
- Arthroplasty (Hemi/Total) - Abandon head
- Capsulotomy: In young patients, releasing the capsule (hematoma) is thought to reduce intracapsular pressure and improve flow, though evidence is mixed.
- Anatomic Reduction: Essential to "un-kink" the retinacular vessels.
The concept of "unkinking" the vessels by reduction is the primary rationale for urgent surgery.
Surgical Technique
Cannulated Screw Fixation
- Goal: Compression without rotation.
- Configuration: Inverted Triangle (One inferior, Two superior).
- Safety:
- Inferior Screw: Passes through the calcar (dense bone).
- Posterior-Superior Screw: RISK ZONE. If the threads penetrate the posterior cortex, they catch the lateral epiphyseal vessels.
- Technique: Careful lateral viewing to ensure threads are strictly intracapsular/intra-osseous.
"Not too long, not too posterior."
The MFCA dictates safety in the posterior and Ganz surgical-dislocation approaches (keep obturator externus intact). The direct anterior approach (DAA) uses the internervous Hueter interval — superficially between sartorius (femoral nerve) and tensor fasciae latae (superior gluteal nerve), deep between rectus femoris and gluteus medius — and has its own vascular landmark:
- The ascending branch of the lateral femoral circumflex artery (LFCA) crosses the distal part of the interval and is the classic "DAA bleeder"; it is identified and ligated or cauterised early to keep the field dry.
- Because the DAA works anteriorly, it does not disturb the posterosuperior retinacular vessels, so it is vascularly kind to the femoral head — a theoretical advantage, although any dislocation is still through the (less critical) anterior capsule.
- The lateral femoral cutaneous nerve runs near the interval and is the commonest complication (meralgia paraesthetica) — a neurological, not vascular, hazard, but worth pairing with the LFCA point.
Complications
- AVN: Late segmental collapse. Painful. Requires THR.
- Non-Union: Vascular failure prevents healing.
- Late Segmental Collapse: Can occur up to 2-3 years post injury.
- Hardware Failure: "Back out" or "Cut out" of screws due to poor bone stock or non-union.
Rehabilitation Protocol
- Fixation: Touch weight bearing or Partial weight bearing to protect the blood supply/reduction? Controversy exists. Most allow WBAT (Weight Bear As Tolerated) in stable constructs.
- Replacement: Immediate Full Weight Bearing. Vascularity is no longer an issue.
Prognosis
- Displaced Fracture (young adults): non-union roughly 10-30%, AVN roughly 15-30% even with anatomic fixation (Upadhyay RCT reported overall AVN 16.3%).
- Undisplaced Fracture: non-union approximately 5%, AVN under 10%.
- Paediatric: AVN risk rises with proximal fracture level; transepiphyseal (Delbet type I) fractures carry the highest risk.
Guidelines, Registries & Global Practice
Global Epidemiology
- Hip fractures are projected to reach 4.5-6 million annually worldwide by 2050, with the burden shifting toward Asia.
- Intracapsular (femoral neck) fractures account for roughly half of all proximal femoral fractures; in adults under 50 they are usually high-energy and carry a disproportionate AVN/non-union risk.
- AVN after displaced neck fracture in young adults is reported at roughly 15-30% even with optimal treatment; non-union at 10-30%.
Side-by-Side Guideline Comparison
- AAOS (US)
- Arthroplasty over internal fixation
- NICE / BOA-BOAST (UK)
- Arthroplasty (THR if mobile, independent, not cognitively impaired)
- AO Foundation
- Replacement when head viability is doubtful
- AAOS (US)
- Anatomic reduction + fixation to preserve head
- NICE / BOA-BOAST (UK)
- Reduction and fixation; minimise delay to theatre
- AO Foundation
- Urgent anatomic reduction; preserve retinacular vessels
- AAOS (US)
- Surgery within 24-48h reduces complications
- NICE / BOA-BOAST (UK)
- Surgery on day of or day after admission (governance target)
- AO Foundation
- Treat young displaced fractures urgently
Registry Evidence
- NJR (UK), AOANJRR (Australia), AJRR (US), SHAR (Sweden): Track arthroplasty done for failed fixation/AVN; total hip replacement generally outperforms hemiarthroplasty in younger, active patients for function and revision in displaced neck fractures.
- National Hip Fracture Databases (UK NHFD and similar): "time to theatre" is a quality metric, but the strongest modifiable driver of head salvage remains reduction quality, not the clock alone (see Upadhyay).
High- vs Limited-Resource Practice Variation
- High-resource: MRI for early AVN, dedicated trauma lists, choice of THR vs fixation, and surgical-dislocation expertise for select head/neck pathology.
- Limited-resource: Cannulated screws or DHS predominate because of cost and implant availability; muscle-pedicle bone grafting (e.g. quadratus femoris pedicle) is still used in some centres to biologically augment fixation in young patients.
Paediatric Note
- The artery of the ligamentum teres is important in infants; septic arthritis of the hip in this group causes a pressure tamponade that can infarct the epiphysis and is a surgical emergency.
Controversies & Areas of Uncertainty
The "hip attack" / 6-hour dogma is challenged by the Upadhyay RCT, which found delay beyond 48 hours did not increase AVN or non-union in young adults. Reduction quality and posterior comminution were the dominant predictors. Most still operate urgently, but the evidence for a hard time cut-off is weak.
Intracapsular tamponade is real, but whether decompressing the haematoma improves head survival is unproven. It is biologically plausible and low-risk, so many surgeons do it for young patients despite the absence of high-level evidence.
FAITH showed higher AVN with the sliding hip screw than with parallel cancellous screws, raising the question of whether reaming and a single large central device add vascular or thermal insult to an already compromised head.
The "young" cutoff is contested. Below this band, head preservation is favoured; above it, registries and trials increasingly favour arthroplasty (often THR) for displaced fractures. The middle band remains an individualised decision.
MCQ Practice Points
Q: Which artery provides the majority of blood supply to the adult femoral head? A: Medial Femoral Circumflex Artery (Deep Branch).
Q: Where are the retinacular vessels located relative to the capsule? A: Intracapsular but Extrasynovial. (They run on the neck under the synovial lining).
Q: At what age is the artery of the ligamentum teres most significant? A: Infancy (under 4 years).
Q: The Cruciate Anastomosis involves which vessels? A: First Perforator, Medial Circumflex, Lateral Circumflex, Inferior Gluteal. (Not Superior Gluteal).
Q: Which movement is most likely to tear the MFCA? A: Posterior Dislocation.
Q: The Artery of the Ligamentum Teres is a branch of which vessel? A: Obturator Artery. (Posterior branch).
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“Describe the precise course of the Medial Femoral Circumflex Artery.”
“You are fixing a femoral neck fracture with cannulated screws. Why do you avoid the posterior superior quadrant for screw placement?”
“A 30-year-old cyclist falls and sustains a displaced intracapsular femoral neck fracture. It is 10 PM. What is your plan?”
“A 38-year-old on long-term steroids for lupus has bilateral groin pain. MRI shows a serpentine subchondral line in both femoral heads. How does the vascular mechanism here differ from a fractured hip, and how does that change management?”
Anatomy
- Main: MFCA (Deep Branch)
- Minor: LFCA (Anterior)
- Retinacula: Posterior-Superior dominant
- Lig Teres: Negligible in adults
Vascular Rings
- 1. Extracapsular (Base of Neck)
- 2. Retinacular (Ascending on Neck)
- 3. Subsynovial (Head Entry Point)
- Ring of Crock = MFCA + LFCA Anastomosis
Clinical
- Fracture: Garden III/IV = AVN Risk
- Approach: Preserve Quadratus Femoris
- Emergent: Young Displaced #NOF
- Screw Hazard: Post-Sup Quadrant
Evidence Base
Normal Vascular Anatomy of the Femoral Head
- Classic injection-radiograph study of the adult femoral head vasculature
- Described the lateral epiphyseal vessels (from the MFCA) as supplying the bulk of the weight-bearing superolateral head
- Showed the foveal (ligamentum teres) artery supplies only a small medial zone in the adult
Distribution and Anastomoses of Arteries Supplying the Head and Neck of the Femur
- Angiographic and dissection study mapping the extracapsular ring and ascending cervical (retinacular) vessels
- Confirmed the posterosuperior retinacular group as the principal source to the epiphysis
- Defined the anastomotic redundancy that fails after subcapital fracture
Anatomy of the Medial Femoral Circumflex Artery and its Surgical Implications
- Dissection of 24 cadaver hips with latex injection
- The deep branch of the MFCA crosses posterior to obturator externus and anterior to the conjoint tendon, perforating the capsule at gemellus superior
- Obturator externus protected the deep branch from rupture during dislocation in any direction after complete capsulotomy
Surgical Dislocation of the Adult Hip Without the Risk of AVN
- 213 hips over 7 years using a trochanteric-flip osteotomy with anterior dislocation
- External rotators left intact so the MFCA is protected by obturator externus
- No case developed avascular necrosis on follow-up
Changing Patterns of Proximal Femoral Vascularity
- Described age-related evolution of proximal femoral blood supply from infancy to skeletal maturity
- The physis acts as a barrier isolating the epiphysis from metaphyseal vessels until closure
- Ligamentum teres contribution is significant in infancy and involutes with growth
Delayed Internal Fixation of Femoral Neck Fractures in Young Adults (RCT)
- 102 patients aged 15-50 with displaced (Garden III/IV) fractures randomised to closed vs open reduction
- No difference in union or AVN between closed and open reduction; overall AVN was 16.3%
- Delay of more than 48 hours did not increase union failure or AVN; posterior comminution, poor reduction and malplaced screws drove non-union
FAITH: Sliding Hip Screw vs Cancellous Screws (RCT)
- 1108 patients aged 50+ randomised to sliding hip screw vs cancellous screws
- No overall difference in 24-month reoperation (20% vs 22%)
- Avascular necrosis was higher with the sliding hip screw (9% vs 5%; HR 1.91); smokers and displaced/base-of-neck fractures may favour the SHS