The Hip-Spine Relationship in THA
- Trusting the supine 'safe zone'. A cup at textbook supine inclination/anteversion can be functionally unsafe in a stiff spine — there is NO universal safe zone. Always reason from functional (standing + seated) mechanics.
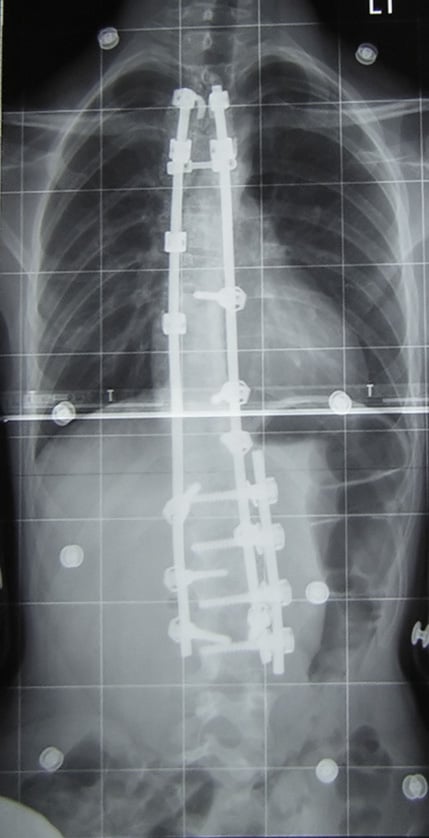
- Not asking about (or not imaging) a lumbar fusion. Prior fusion is the strongest spinopelvic risk factor (RR ~3, worse with more levels and inclusion of the sacrum) — miss it and the THA dislocates.
- Ordering only a standing film. Mobility is the standing-to-sitting CHANGE in sacral slope; without the seated lateral you cannot call a spine stiff (under 10° change).
- Confusing the parameters. PI = SS + PT; PI is fixed (morphological), SS and PT are positional. PI-LL over 10° = flatback.
- Wrong dislocation direction. 'Stuck standing' (no posterior tilt) → POSTERIOR dislocation; 'stuck sitting' (fixed posterior tilt) → ANTERIOR dislocation.
Overview
The hip, pelvis and lumbar spine move as one coordinated lumbopelvic complex. The pelvis is the hinge: its sagittal tilt simultaneously sets acetabular (cup) orientation and lumbar lordosis. When normal pelvic mobility is lost — through lumbar degeneration, deformity, or fusion — the dynamic protection that keeps a total hip stable through the sit-to-stand arc is lost, and dislocation risk rises sharply.
For most of the history of THA, cup position was judged against fixed supine "safe zones" (classically inclination/anteversion around 40°/15–20°). The hip-spine concept reframes this: acetabular orientation is dynamic, changing with posture as the pelvis tilts. A growing, ageing population with lumbar fusions has made impaired spinopelvic mobility one of the leading reasons a technically well-positioned THA still dislocates. Recognising and planning for it pre-operatively is now core adult-reconstruction practice.
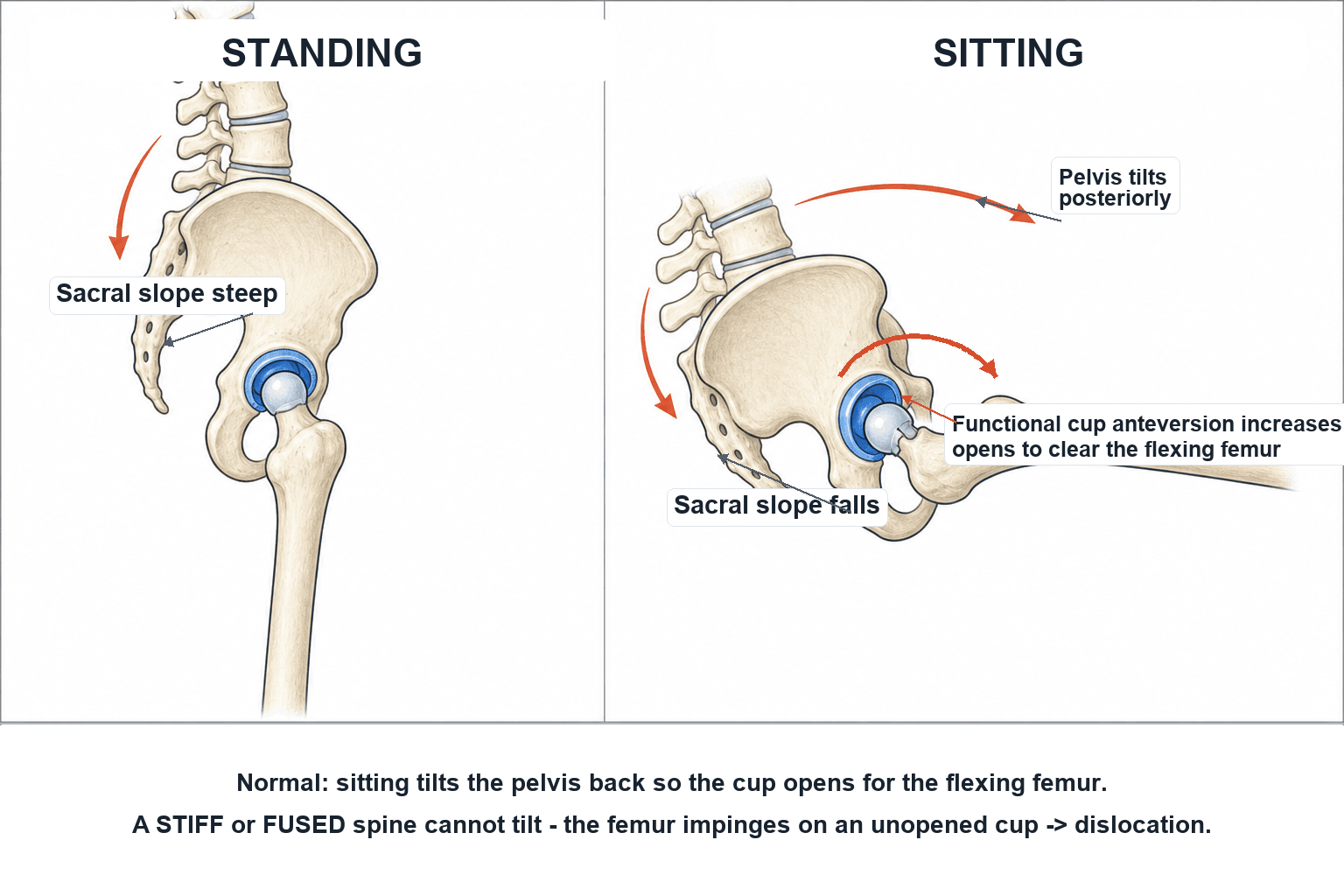
Standing to sitting, the healthy pelvis rotates posteriorly (sacral slope falls), which automatically increases functional acetabular anteversion and inclination — opening the socket to accommodate the flexing femur and prevent posterior impingement/dislocation.
With a fused or degenerate stiff lumbar spine the pelvis cannot tilt, so the femur flexes against a socket that has not opened up → posterior edge-loading and dislocation. A cup in a textbook supine "safe zone" can be functionally unsafe in this patient.
Mechanism & spinopelvic parameters
The three key parameters (lateral spinopelvic radiograph)
- Pelvic Incidence (PI): a fixed, morphological parameter — the angle between a line perpendicular to the sacral endplate and a line to the femoral head centre. It does NOT change with posture and defines the patient's pelvic "shape." PI = SS + PT.
- Sacral Slope (SS): positional — the angle of the sacral endplate to horizontal; falls when sitting (pelvis tilts back).
- Pelvic Tilt (PT): positional — the tilt of the pelvis relative to the femoral heads; increases (more posterior tilt) when sitting.
As posture changes, PI stays constant while SS and PT trade off against each other.
The examiner often pushes past "the cup opens up" to how much and why dislocation actually happens:
- Pelvic tilt drives functional cup orientation in a near-linear way — roughly each 1° of posterior pelvic tilt adds about 0.7–0.8° of functional acetabular anteversion (and reduces functional inclination by a smaller amount). So sitting (posterior tilt) functionally anteverts and opens the cup, while standing/extension (relative anterior tilt) functionally retroverts it. A pelvis stuck in relative anterior tilt (the stiff, un-tilting spine) is therefore functionally under-anteverted even when the supine film looks perfect.
- Dislocation is the end of an impingement cascade — at the extreme of motion the femoral neck/component contacts either the liner/rim (prosthetic impingement) or residual bone/osteophyte (bony impingement); that contact point becomes a fulcrum that levers the head out of the socket. Flexion-adduction-internal rotation against an under-opened cup → posterior dislocation; extension-external rotation against an over-anteverted cup → anterior dislocation.
- The protective levers all enlarge the impingement-free arc and jump distance — a higher head-to-neck ratio, a larger femoral head, skirtless heads, and above all the dual-mobility bearing (a large effective head). Jump distance (the lateral translation needed to dislocate) rises with head diameter and adequate cup coverage — and removing impinging osteophytes intra-operatively matters as much as the implant.
PI = SS + PTThe spinopelvic parameters
Hook:PI is the fixed shape; SS and PT trade off with posture; PI-LL exposes the flatback.
Classification & assessment
The Hip-Spine Classification (Vigdorchik, 2021 Otto Aufranc Award)
A practical system combining spinal alignment (normal vs flatback) with spinal mobility (mobile vs stiff) to guide component choice:
- Group 1 — normal alignment (PI-LL within 10°): 1A mobile spine, 1B stiff spine.
- Group 2 — flatback deformity (PI-LL greater than 10°): 2A mobile spine, 2B stiff spine.
Each category dictates a patient-specific cup position, and dual-mobility components are directed to the highest-risk groups (all of group 2B, and all patients with more than three fused levels). Applied prospectively, this achieved a 0.8% dislocation rate (99.2% survivorship free of dislocation at five years).
Management strategies
The central practical message: there is no single cup orientation safe for everyone. Cup inclination and version (and sometimes stem version) must be set to the patient's functional spinopelvic mechanics, while still respecting reasonable coronal targets (inclination/version of approximately 40°/20° ± 10°).
- 1Screen for impaired mobilityHistory of lumbar fusion/stiff back; standing AND seated lateral spinopelvic films; derive PI, SS change (mobility), PI-LL, PT and CSI.
- 2Classify (Hip-Spine / Bordeaux)Normal vs flatback (PI-LL over 10°) and mobile vs stiff (SS change under 10°) → group 1A/1B/2A/2B; identify the patient who cannot tilt the pelvis.
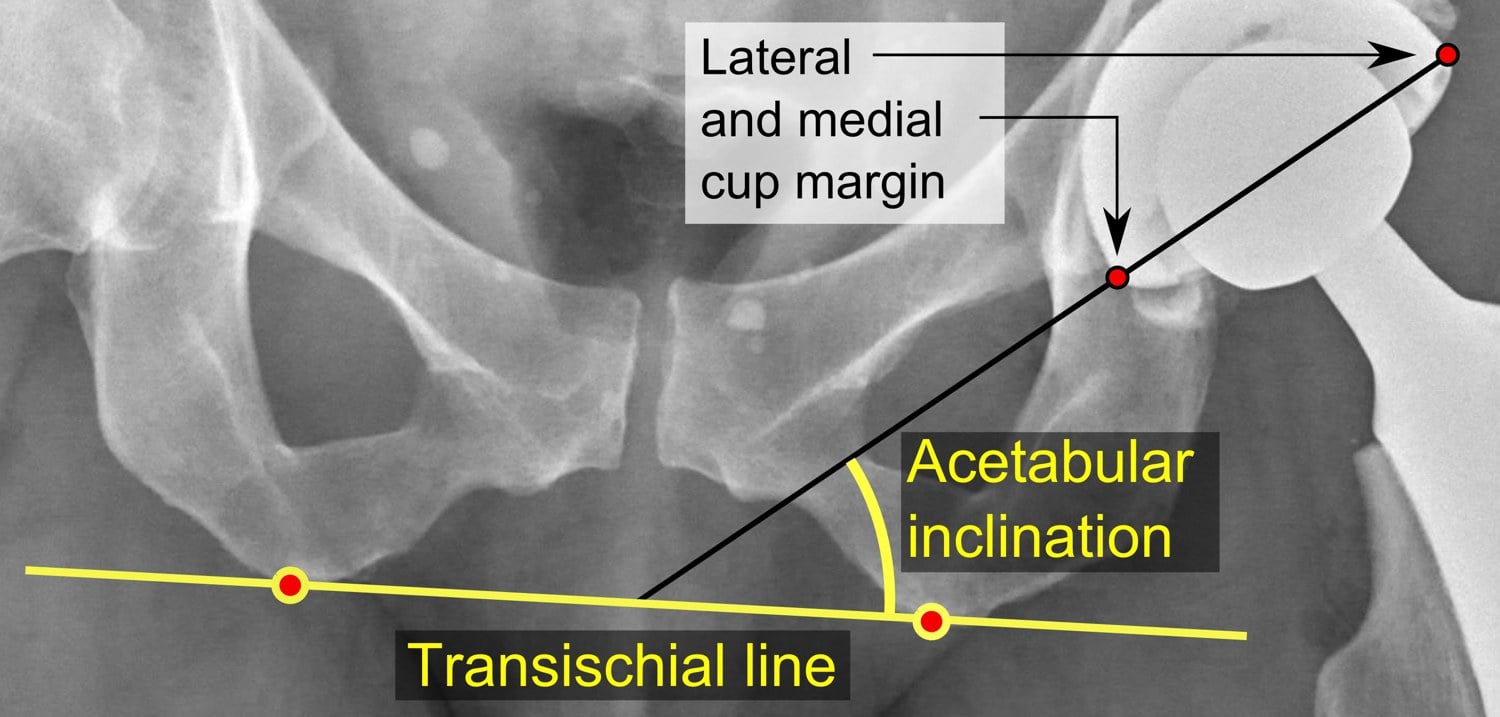
- 3Set a FUNCTIONAL cup targetIndividualise version/inclination to standing+sitting mechanics (standing CSI 205–245°), keeping coronal ~40/20 ±10°; optimise combined cup + stem version where the cup alone can't be made safe.
- 4Choose a forgiving bearingDual mobility for stiff/fused/deformed spines (larger effective head, greater jump distance); a larger head and, in selected salvage cases, a constrained liner are adjuncts. Robotics/navigation help execute the target.
The toolkit for the high-risk hip-spine patient:
- Individualised (functional) cup orientation — adjust target version/inclination from standing/sitting parameters rather than a fixed safe zone.
- Dual-mobility (DM) components — the principal solution; the large effective head and increased jump distance markedly increase the impingement-free arc and reduce dislocation (directed at stiff spines, fusions, deformity, neuromuscular disease, and femoral-neck-fracture THA).
- Larger femoral heads — increase jump distance and impingement-free range.
- Stem version / combined version — adjust femoral version to optimise combined (cup + stem) version when the cup alone cannot be made safe.
- Constrained liners — reserved for selected salvage/abductor-deficient cases (they transfer stress to fixation and have their own failure modes).
- Technology — robotic/navigated systems can execute an individualised functional cup target precisely.
Clinical relevance: the high-risk stiff & fused spine
The patients who get into trouble are those who have lost pelvic mobility. The strongest spinopelvic risk factors for dislocation are a stiff spine, a degenerate/deformed lumbar spine, and prior lumbar fusion — and the magnitude of these risks exceeds that of many traditional patient and surgical factors.
A systematic review of over one million THAs found prior spinal fusion increased dislocation risk with odds ratios from roughly 1.6 up to ~24 (relative risk around 3). The risk escalates with more fused levels and with fusions extending to the sacrum, because each removes more compensatory pelvic motion. Always ask about, and look for, a lumbar fusion before THA.
The mechanism is loss of the protective posterior pelvic tilt on sitting. Two failure patterns dominate:
- Stuck standing (pelvis fixed in relative anterior tilt, low functional anteversion): the femur flexes against an under-anteverted socket → posterior dislocation.
- Stuck sitting (pelvis fixed in posterior tilt, high functional anteversion): on standing/extension the femoral neck impinges anteriorly → anterior dislocation.
Stiffness is only one end of the mobility spectrum, and spinopelvic mechanics are not fixed for life — three points the examiner uses to test depth:
- The hypermobile spine — the opposite problem: an excessive standing-to-sitting sacral-slope change (the Bordeaux "hypermobile" group). Importantly, the stiff arthritic hip itself drives compensatory spine/pelvis hypermobility (an arthritic hip nearly doubles the change in pelvic tilt), and these spinopelvic characteristics tend to normalise after THA once hip flexion is restored — so a pre-operatively "hypermobile" pattern may simply reflect the diseased hip. A genuinely hypermobile spine over-tilts and can produce excessive functional anteversion on sitting → anterior instability.
- Mobility changes over the patient's lifetime — a spine classed mobile (1A) at the time of THA can stiffen later with progressive degeneration or a subsequent lumbar fusion, converting the patient into a higher-risk category and contributing to late dislocation years after a stable index arthroplasty.
- Sequencing when a patient needs BOTH a THA and a lumbar fusion/deformity correction — spinal realignment changes the spinopelvic parameters, so ideally plan the cup against the FINAL spinal alignment. A THA implanted before a later fusion was targeted to the pre-fusion mechanics and is at risk once the pelvis stiffens; if the spine deformity is to be corrected, doing/finalising that first (or at least anticipating it) lets the hip be planned to the definitive posture.
STIFFThe high-risk spinopelvic patient
Hook:A STIFF spine needs a forgiving (dual-mobility) hip.
Guidelines, registries & global practice
The hip-spine relationship has moved internationally from a niche concept to mainstream pre-operative planning over the last decade, driven by an ageing population with lumbar degeneration and the rising number of lumbar fusions. The unifying message across European (EFORT) and North American (Otto Aufranc / Hospital for Special Surgery) reviews is consistent: screen for impaired spinopelvic mobility, abandon the universal safe zone, and individualise component choice.
- What the evidence shows
- No — orientation must be functional
- Best supporting evidence
- Grammatopoulos 2023; Zagra 2022
- What the evidence shows
- Prior lumbar fusion (RR ~3, more with levels/sacrum)
- Best supporting evidence
- van der Gronde 2022 (systematic review)
- What the evidence shows
- Less than 10° sacral-slope change standing to sitting
- Best supporting evidence
- Vigdorchik 2021; Grammatopoulos 2023
- What the evidence shows
- PI-LL over 10°, PT over 19°, CSI outside 205–245°
- Best supporting evidence
- Grammatopoulos 2023
- What the evidence shows
- Dual mobility (+ larger head, functional version)
- Best supporting evidence
- Vigdorchik 2021; Bellova 2021
National joint registries track dislocation and revision-for-instability, and the use of dual-mobility constructs in primary THA has risen, particularly for high-risk and femoral-neck-fracture patients (long-term primary-DM data are still maturing). Across resource settings the low-cost, high-yield intervention is the same: a careful history for spinal fusion and two functional (standing and seated) radiographs — available almost anywhere — to identify the patient who needs an individualised plan.
Evidence
2021 Otto Aufranc Award: A simple Hip-Spine Classification for total hip arthroplasty: validation and a large multicentre series
- Prospective multicentre study; 2081 of 3777 screened THAs categorised by the Hip-Spine Classification (groups 1A/1B/2A/2B).
- Flatback defined as pelvic incidence minus lumbar lordosis greater than 10°; stiff spine as less than 10° change in sacral slope from standing to seated.
- Dual-mobility components were used in higher-risk groups (all of group 2B and all with more than three fused levels); survivorship free of dislocation was 99.2% at five years (0.8% dislocation rate).
Current concepts in hip-spine relationships: making them practical for total hip arthroplasty
- Reviews the lumbopelvic complex and spinopelvic parameters (sacral slope, pelvic tilt, pelvic incidence) and classification systems (most comprehensively the Bordeaux Classification).
- Historical fixed 'safe zones' may not apply to patients with impaired spinopelvic mobility; cup inclination/version and stem version may need adjustment for functional orientation.
- Stem design, bearing surface (including dual mobility) and head size are tools for abnormal hip-spine relationships, with special attention to adult spinal deformity and the fused spine.
The Hip-Spine Classification and its 0.8% dislocation rate come from Vigdorchik et al. 2021 (DOI 10.1302/0301-620X.103B7.BJJ-2020-2448.R2); the practical hip-spine framework from Zagra et al. 2022 (DOI 10.1530/EOR-21-0082); the spinopelvic dislocation-risk synthesis (fusion RR ~3) from van der Gronde et al. 2022 (DOI 10.2106/JBJS.RVW.22.00038); the functional thresholds (PI-LL over 10°, PT over 19°, CSI 205–245°) from Grammatopoulos et al. 2023 (DOI 10.1530/EOR-23-0049); and the dual-mobility rationale from Bellova et al. 2021 (DOI 10.1055/a-1527-7758).