Wear Debris → Macrophage Activation → Osteolysis | HXLPE Reduces Wear 95% | Early Detection Critical
- Polyethylene wear is the primary cause of late THA failure and aseptic loosening
- Particle size 0.1-1μm is most biologically active - triggers macrophage response
- Highly cross-linked PE (HXLPE) reduces wear by over 90% compared to conventional
- Osteolysis is silent - often massive bone loss before symptoms develop
- Annual surveillance radiographs are mandatory for early detection
- “Osteolysis = biological response to wear particles, not mechanical loosening
- “Effective joint space (EJS) concept - particles access bone via capsular defects
- “HXLPE trade-off: reduced wear but lower fracture toughness and oxidation
- “Isolated liner exchange only if well-fixed shell and no significant osteolysis
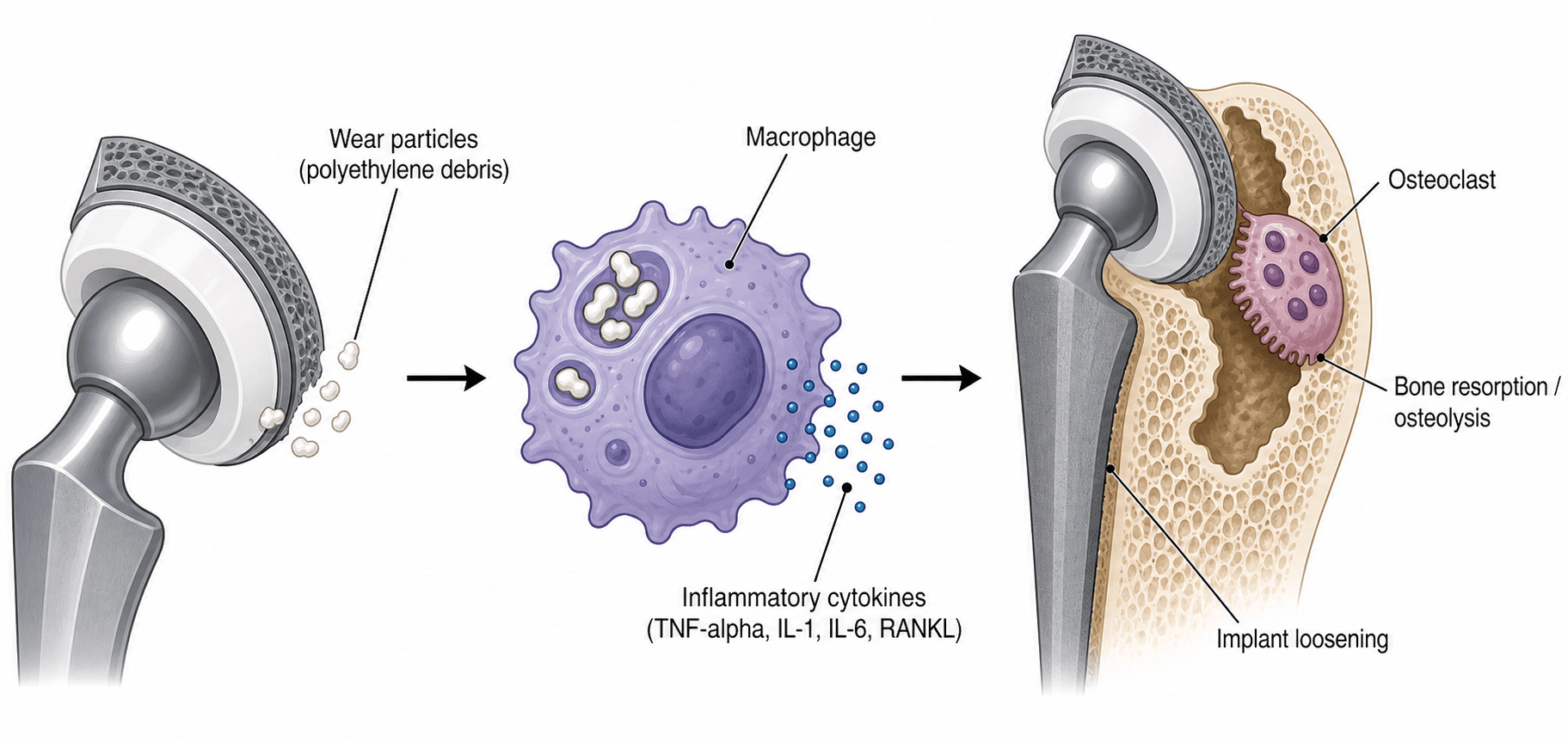
Wear particles activate macrophages which release cytokines (TNF-α, IL-1, IL-6) and RANKL. This triggers osteoclast activation and bone resorption. The process is biological, not mechanical - hence "particle disease."
Highly cross-linked polyethylene (radiation doses over 50 kGy) reduces wear by over 90%. This has transformed THA longevity but involves trade-offs: reduced fracture toughness and potential oxidation. Not recommended for young, high-demand patients with large heads.
Effective joint space concept: particles migrate through capsular defects (screw holes, gaps) to reach bone-implant interface. Osteolysis progresses silently - massive bone loss can occur before symptoms. Annual radiographs mandatory.
Early detection is key. Annual AP/lateral pelvis radiographs. Look for radiolucent lines, expanding lesions, implant migration. CT or MRI for suspected osteolysis. Address before catastrophic bone loss or fracture.
- Imaging Findings
- Focal osteolysis under 2cm, stable implants
- Decision
- Monitor closely
- Treatment Options
- Annual radiographs, consider CT to quantify, patient education
- Imaging Findings
- Expanding lesions over 2cm, stable implants
- Decision
- Consider isolated liner exchange
- Treatment Options
- Remove source of wear, curettage and bone graft lesions
- Imaging Findings
- Large osteolysis, implant migration or loosening
- Decision
- Revision THA required
- Treatment Options
- Remove all components, address bone defects, structural grafts
- Imaging Findings
- Periprosthetic fracture through osteolytic bone
- Decision
- Urgent revision with fracture fixation
- Treatment Options
- ORIF + revision, impaction grafting, potential structural support
Overview and Epidemiology
Polyethylene wear and osteolysis represent the primary mode of late failure in total hip arthroplasty. Understanding the mechanisms, prevention, and management of particle disease is fundamental to modern arthroplasty practice.
- First-generation THA (Charnley) used conventional ultra-high molecular weight polyethylene (UHMWPE)
- Linear wear rates of 0.1-0.2mm per year were common
- By 10-15 years, significant osteolysis developed in 10-30% of cases
- Revision for osteolysis became the leading indication in many series
- Introduction of highly cross-linked polyethylene (HXLPE) in late 1990s
- Wear reduction of over 90% compared to conventional PE
- Dramatic reduction in osteolysis rates (under 5% at 10-15 years)
- HXLPE is now the standard bearing surface for primary THA
In the 1990s-2000s, osteolysis became the leading cause of THA revision, accounting for up to 30% of revision procedures. The introduction of HXLPE has fundamentally changed this landscape, making wear-related failure uncommon in modern primary THA.
- Conventional PE THAs still in situ from 1980s-2000s continue to present with osteolysis
- Surveillance is mandatory - many patients asymptomatic until catastrophic failure
- HXLPE has shifted the failure mode from wear to instability/infection
- Registry data (AOANJRR): Revision for wear/osteolysis has declined significantly since HXLPE adoption
- Young, active patients (high activity level)
- Larger femoral heads (greater linear distance traveled)
- Thin polyethylene liners (under 6mm minimum thickness)
- Malpositioned components (impingement, edge loading)
- Third-body debris (PMMA, metal, bone cement fragments)
Anatomy and Pathophysiology of Particle Disease
Polyethylene wear mechanisms:
The generation of polyethylene wear particles occurs through three primary mechanisms:
- Molecular bonding between bearing surfaces during contact
- Material transfer from polyethylene to metal/ceramic head
- Continuous loading and unloading creates particle release
- Contributes 30-40% of total wear
- Hard surface (femoral head) plows through soft surface (PE liner)
- Creates scratches, grooves, and deformation
- Roughened femoral heads accelerate abrasive wear
- Contributes 40-50% of total wear
- Interposed particles (PMMA cement, metal debris, bone) act as abrasives
- Dramatically accelerates wear rates (can increase 10-100 fold)
- Common sources: cement from acetabular preparation, metal from impingement
- Contributes 10-30% but highly variable
Particles in the 0.1-1 micrometer range are most biologically active. This size optimally activates macrophages. Smaller particles (under 0.1μm) are less phagocytosed. Larger particles (over 1μm) trigger less inflammatory response. The conventional PE wear process generates billions of particles in this critical size range.
Particle disease cascade:
- Process
- PE wear at bearing surface
- Key Mediators
- Adhesive, abrasive, third-body mechanisms
- Result
- Billions of submicron particles
- Process
- Migration via effective joint space
- Key Mediators
- Screw holes, gaps in press-fit, osteotomies
- Result
- Particles reach bone-implant interface
- Process
- Foreign body response initiated
- Key Mediators
- Pattern recognition receptors, phagocytosis
- Result
- Macrophage activation and frustrated phagocytosis
- Process
- Pro-inflammatory cascade
- Key Mediators
- TNF-α, IL-1β, IL-6, PGE2
- Result
- Inflammatory microenvironment created
- Process
- Osteoclastogenesis signal
- Key Mediators
- RANKL upregulated, OPG downregulated
- Result
- Osteoclast differentiation and activation
- Process
- Osteoclast-mediated
- Key Mediators
- Cathepsin K, acid phosphatase, H+ ATPase
- Result
- Progressive peri-implant bone loss
Effective joint space concept:
The "effective joint space" describes the pathways by which particles access bone:
- Screw holes in acetabular shells (most common pathway)
- Gaps in press-fit fixation or at bone-implant interface
- Osteotomies (greater trochanter, femoral neck cut)
- Capsular defects allowing synovial fluid migration
- Metaphyseal calcar region in uncemented femoral stems
Bone resorption is painless until mechanical failure occurs. Patients remain asymptomatic while massive osteolysis develops. By the time pain develops, there may be catastrophic bone loss or impending fracture. This is why annual surveillance radiographs are non-negotiable.
Osteolysis patterns:
- Common in
- Cementless cups with screws
- Access Route
- Screw holes
- Clinical Significance
- Can lead to cup migration, column deficiency
- Common in
- All designs
- Access Route
- Direct erosion
- Clinical Significance
- Risk of intrapelvic migration
- Common in
- Uncemented stems
- Access Route
- Metaphyseal junction
- Clinical Significance
- Subsidence risk
- Common in
- Cemented stems
- Access Route
- Cement-bone interface
- Clinical Significance
- Periprosthetic fracture risk
PARTICLEPARTICLE - Osteolysis Pathophysiology
Hook:PARTICLE walks through the complete cascade from debris to bone loss
Backside Wear: The Other Particle Source
The three classic wear mechanisms (adhesive, abrasive, third-body) describe the articular bearing surface. But a modular acetabular liner also has a non-articular backside that abuts the metal shell, and micromotion between liner and shell generates particles from this surface - backside wear. It is easily forgotten yet clinically important, because these particles are delivered straight to bone through the acetabular screw holes - the very conduits of the effective joint space - making backside wear a major and often-underappreciated driver of acetabular osteolysis.
- Articular (bearing) wear
- Head-on-liner articulation
- Backside wear
- Non-articular liner-shell interface
- Articular (bearing) wear
- Adhesive, abrasive, third-body
- Backside wear
- Micromotion of the liner against the metal shell
- Articular (bearing) wear
- Via the effective joint space generally
- Backside wear
- Delivered directly to bone through acetabular screw holes
- Articular (bearing) wear
- Bearing couple, head size, component position
- Backside wear
- Locking-mechanism quality, screw-hole number, liner-shell conformity
- Articular (bearing) wear
- HXLPE, hard bearings, optimal positioning
- Backside wear
- Robust locking mechanism, fewer or plugged screw holes, polished congruent shell, monoblock or cemented liner
The classic three wear mechanisms describe the articular bearing surface, but a modular polyethylene liner also has a non-articular backside abutting the metal shell. Micromotion there generates 'backside wear', and those particles reach bone directly through the acetabular screw holes - the conduits of the effective joint space - so backside wear is a major and often-overlooked cause of acetabular osteolysis. It is minimised by a robust liner locking mechanism, fewer screw holes (or hole plugs), a polished congruent shell, and monoblock or cemented-liner constructs that remove the micromotion interface altogether.
Classification Systems
Wear classification:
Polyethylene wear is not formally "classified" but is measured and characterized:
- Total head penetration into liner measured from radiographs
- Calculated as mm of linear penetration
- Annualized wear rate = total penetration / years in situ
- Conventional PE: 0.1-0.2mm/year typical
- HXLPE: under 0.02mm/year expected
- Calculated from linear wear using geometric formulas
- More accurate representation of total material loss
- Accounts for head size (larger heads travel more distance)
- Typically reported as mm³/year
- Concentric: uniform wear around entire liner (normal pattern)
- Eccentric: focal wear in one area (suggests malposition or impingement)
- Accelerated: increasing wear rate over time (suggests third-body or component issues)
Paprosky Acetabular Defect Classification:
Used to describe bone loss patterns and guide reconstruction:
- Description
- Minimal
- Bone Loss
- Intact rim and columns
- Reconstruction
- Standard cementless cup
- Description
- Superior migration
- Bone Loss
- Superior and medial wall defect
- Reconstruction
- High hip center or standard with graft
- Description
- Ischial osteolysis
- Bone Loss
- Ischium and inferior wall loss
- Reconstruction
- Standard cup with medial augment
- Description
- Teardrop osteolysis
- Bone Loss
- Medial wall defect
- Reconstruction
- Mesh or augment for medial support
- Description
- Superior and medial migration
- Bone Loss
- Less than 50% host bone contact
- Reconstruction
- Structural graft, augments, jumbo cup
- Description
- Superior and medial migration
- Bone Loss
- Less than 50% host bone contact, ischial lysis
- Reconstruction
- Custom triflange, cage + liner
Paprosky Femoral Defect Classification:
- Description
- Minimal loss
- Metaphyseal Bone
- Intact
- Canal Status
- Normal or minimally expanded
- Description
- Metaphyseal damage
- Metaphyseal Bone
- Compromised
- Canal Status
- Expanded but intact diaphysis
- Description
- Severe metaphyseal loss
- Metaphyseal Bone
- Severely compromised
- Canal Status
- More than 4cm intact diaphyseal tube
- Description
- Severe metaphyseal loss
- Metaphyseal Bone
- Severely compromised
- Canal Status
- Less than 4cm intact diaphyseal tube
- Description
- Extensive loss
- Metaphyseal Bone
- Absent
- Canal Status
- Isthmus gone, canal widened extensively
This classification guides surgical planning for revision in the setting of osteolysis.
Highly Cross-Linked Polyethylene (HXLPE)
Manufacturing process:
HXLPE is created through gamma or electron beam irradiation of conventional UHMWPE:
- Radiation dose: 50-100 kGy (vs under 25 kGy for sterilization)
- Cross-linking: Radiation creates free radicals that form covalent bonds between polymer chains
- Increased cross-link density: Restricts polymer chain mobility
- Result: Dramatically increased wear resistance
Post-irradiation processing:
To eliminate free radicals (which cause oxidative degradation):
- Remelting at over 150°C
- Eliminated free radicals but reduced crystallinity
- Lower fracture toughness and mechanical properties
- Some oxidation in vivo
- Annealing below melting temperature (130-150°C)
- Preserves more crystallinity
- Better mechanical properties
- Vitamin E doping (antioxidant stabilization)
- Superior oxidation resistance
- Sequential irradiation and annealing
- Antioxidant (Vitamin E) blended before cross-linking
- Mechanical properties closer to conventional PE
- Excellent oxidation resistance
- Conventional UHMWPE
- 0.1-0.2 mm/year
- HXLPE (100 kGy)
- 0.01-0.02 mm/year
- Clinical Implication
- 90-95% wear reduction
- Conventional UHMWPE
- 10-30%
- HXLPE (100 kGy)
- Under 5%
- Clinical Implication
- Dramatic reduction in particle disease
- Conventional UHMWPE
- Higher (more resistant)
- HXLPE (100 kGy)
- Lower (more brittle)
- Clinical Implication
- Rim fractures reported with large heads, thin liners
- Conventional UHMWPE
- Good (if shelf-aged properly)
- HXLPE (100 kGy)
- Variable (first-gen poor, newer excellent)
- Clinical Implication
- Second/third-gen HXLPE superior
- Conventional UHMWPE
- 6mm
- HXLPE (100 kGy)
- 8-10mm
- Clinical Implication
- Need thicker liner for same mechanical strength
Clinical evidence:
Multiple studies now have 15-20 year follow-up on HXLPE. Results consistently show:
- Wear rates 90-95% lower than conventional PE
- Osteolysis rates under 5% (vs 10-30% conventional)
- No increase in revisions for fracture or other complications
- HXLPE is now the standard of care for primary THA bearing surfaces
Limitations and contraindications:
While HXLPE is standard, there are scenarios where caution is warranted:
- Concern
- Thin liner, rim fracture risk
- Recommendation
- Use 36mm or smaller, ensure adequate liner thickness
- Concern
- Theoretical oxidation over 40-50 years
- Recommendation
- Consider ceramic-on-HXLPE or ceramic-on-ceramic
- Concern
- Mechanical stress on brittle material
- Recommendation
- Some surgeons prefer ceramic bearings
- Concern
- Cannot achieve adequate liner thickness
- Recommendation
- May need conventional PE or ceramic bearings
WEARWEAR - Polyethylene Wear Mechanisms
Hook:WEAR reminds you of the critical particle size and pathways to osteolysis
HXLPEHXLPE - Highly Cross-Linked Polyethylene
Hook:HXLPE is the standard bearing but know the trade-offs for exam discussion
Clinical Presentation and Assessment
Presentation patterns:
Osteolysis typically presents in one of four ways:
- Discovered on routine surveillance radiographs
- Patient has no complaints
- THA functioning well clinically
- Critical to detect at this stage before progression
- Gradual onset groin or thigh pain
- Worse with activity
- May have mechanical symptoms (clunking, instability)
- Often indicates implant loosening or impending failure
- Recurrent dislocations
- PE liner wear can reduce effective head size
- Abductor damage from acetabular osteolysis
- Malposition from component migration
- Periprosthetic fracture through osteolytic bone
- Acute presentation with severe pain, inability to weight-bear
- Worst-case scenario - often massive bone loss
Annual radiographs for life are mandatory for all THA patients. Osteolysis is almost always asymptomatic in early stages. By the time pain develops, there may be massive bone loss requiring complex reconstruction. Detecting osteolysis early allows intervention before catastrophic failure.
Physical examination:
In early osteolysis (asymptomatic):
- Examination is completely normal
- Full range of motion, no pain
- No instability
- Abductor strength intact
- This is why imaging is essential
In advanced osteolysis with loosening:
- Antalgic gait
- Groin or thigh pain with range of motion
- Pain with internal/external rotation (acetabular) or axial loading (femoral)
- Leg length discrepancy (if subsidence)
- Instability signs (Trendelenburg, apprehension)
Laboratory workup:
Rule out infection before attributing symptoms to osteolysis:
- ESR and CRP - should be normal in pure osteolysis
- Joint aspiration if elevated inflammatory markers
- Cell count, differential, cultures
- Alpha-defensin or other synovial biomarkers
Osteolysis is sterile inflammation. ESR/CRP should be normal or minimally elevated. If inflammatory markers are significantly elevated (CRP over 20), infection must be ruled out before proceeding with treatment for osteolysis. When in doubt, aspirate.
Differential diagnosis of the painful or radiolucent THA:
Periprosthetic radiolucency or a painful THA is not automatically wear-related osteolysis. The most important alternative to exclude is infection. Work through the following differential before committing to a wear/osteolysis pathway.
- Distinguishing features
- Often asymptomatic; scalloped/geographic lysis, eccentric (worn) head, conventional or older PE bearing
- Key investigation
- Serial radiographs + CT; normal ESR/CRP
- Why it matters
- Treat the wear source; address bone defect
- Distinguishing features
- Rest/start-up pain, sinus, early failure; can perfectly mimic osteolysis
- Key investigation
- ESR/CRP, joint aspiration (cell count, culture, alpha-defensin)
- Why it matters
- Must exclude first - changes the entire algorithm to staged revision
- Distinguishing features
- Metal-on-metal or fretting/corrosion at modular junctions; pseudotumour, effusion
- Key investigation
- Serum cobalt/chromium ions, MARS MRI
- Why it matters
- Different management (revise bearing/junction); not PE particle disease
- Distinguishing features
- Progressive migration, complete radiolucent line over 2 mm, pain on loading
- Key investigation
- Serial radiographs comparing to baseline
- Why it matters
- May coexist with osteolysis; mandates component revision
- Distinguishing features
- Proximal femoral bone loss (calcar rounding) around stiff stems, not expansile
- Key investigation
- Radiographs; pattern recognition
- Why it matters
- Usually benign and non-progressive - avoid unnecessary revision
- Distinguishing features
- Acute pain, inability to weight-bear, often through osteolytic bone
- Key investigation
- Radiographs (Vancouver classification)
- Why it matters
- May be the presenting event of advanced osteolysis
- Distinguishing features
- Lumbar spine, vascular claudication, hernia, greater trochanteric pain / abductor tendinopathy
- Key investigation
- Spine and vascular assessment, targeted examination
- Why it matters
- Avoids revising a well-functioning, well-fixed THA
Investigations and Imaging
- AP pelvis - bilateral comparison, cup position, acetabular osteolysis
- AP hip - close-up of affected hip
- Lateral hip - frog-leg or cross-table lateral for femoral osteolysis
- Radiolucent lines at bone-implant interface (wider than 2mm progressive)
- Expanding lesions - scalloped, geographic bone loss
- Implant migration - change in position compared to baseline
- Component loosening - radiolucent line over 2mm, migration over 2mm
- Thin or absent polyethylene - eccentric head position indicating wear
- Classification
- DeLee and Charnley
- Zones
- I (superior), II (axial), III (inferior)
- Classification
- Gruen zones
- Zones
- 1-7 (seven zones around stem)
- Classification
- Engh zones
- Zones
- Proximal (1-7), distal (8-14)
Always compare to baseline immediate postoperative radiographs. Osteolysis is a progressive process - documenting progression over time is more important than a single time point. Measure lesion size, document zones involved, assess component position changes.
- Gold standard for quantifying osteolysis extent
- 3D reconstructions show true bone loss volume
- Guides surgical planning (bone graft needs, structural support)
- Reduces metal artifact with modern protocols
- Recommended for: large lesions, surgical planning, unclear plain film findings
- Metal artifact reduction sequences (MARS protocol)
- Excellent for soft tissue assessment
- Can detect early osteolysis not visible on plain films
- Useful for: abductor tears, fluid collections, soft tissue masses
- Not routine but valuable in selected cases
- Bone scan (Tc-99m MDP) - non-specific, shows increased uptake
- White cell scan (In-111 WBC) - differentiates infection from aseptic loosening
- Mainly used when infection is suspected
- Principle
- Computer-assisted measurement of head penetration
- Advantages
- Accurate, reproducible
- Limitations
- Requires specialized software
- Principle
- Measurement from center of head to reference points
- Advantages
- Simple, widely available
- Limitations
- Less accurate for small amounts
- Principle
- Automated edge detection software
- Advantages
- Very accurate, minimal observer error
- Limitations
- Requires high-quality images
Annual wear rate calculation:
- Measure total linear penetration
- Divide by years since implantation
- Conventional PE: 0.1-0.2mm/year is typical
- HXLPE: under 0.02mm/year expected
- Accelerating wear rate (increasing over time) is concerning
Interpreting Wear: Bedding-in, Creep, and the Osteolysis Threshold
Measured head penetration on serial radiographs is not all true wear. It is biphasic and has two components, and misreading it leads to over-calling wear in the first year or two.
Two phases: an early bedding-in (running-in) phase - roughly the first year - with higher apparent penetration, followed by a lower, linear steady-state phase. The wear rate should be taken from the steady-state slope, not from total penetration divided by years (which over-estimates the rate early on).
- Creep (cold flow)
- Plastic/viscoelastic deformation under load (head beds in without material loss)
- True wear
- Removal of material from the surface
- Creep (cold flow)
- None
- True wear
- Billions of submicron particles
- Creep (cold flow)
- Dominates the early bedding-in phase (first ~1 year)
- True wear
- Continues at a steady linear rate thereafter
- Creep (cold flow)
- No
- True wear
- Yes - the driver of particle disease
- Creep (cold flow)
- Inflates apparent early penetration
- True wear
- Measure from the steady-state slope, not total penetration over years
The osteolysis threshold: osteolysis is uncommon when the steady-state linear wear rate is below approximately 0.05 mm/year (the commonly cited 'osteolysis threshold'). Conventional polyethylene (approximately 0.1-0.2 mm/year) exceeds it, whereas HXLPE (approximately 0.01-0.03 mm/year) sits well below it - the mechanistic reason cross-linking nearly abolishes osteolysis.
Radiographic head penetration is biphasic - a higher early 'bedding-in' phase then a lower linear steady-state - and has two components: CREEP (plastic cold-flow of the polyethylene, no material loss and no particles), which dominates the first year, and TRUE WEAR (material removal that generates the particles driving osteolysis). Calculate the wear rate from the steady-state slope, not total penetration divided by years, or you will over-call wear early on. Clinically, osteolysis is uncommon below a steady-state wear rate of about 0.05 mm/year (the 'osteolysis threshold'): conventional polyethylene exceeds it while HXLPE sits well below it.
Management Algorithm
- Asymptomatic patient
- Small focal lesions (under 2cm diameter)
- Stable implants (no migration, well-fixed)
- Low activity level, elderly patient
- Significant medical comorbidities
- Radiographs: every 6-12 months (more frequent if progressive)
- CT scan: baseline to quantify extent, repeat if progression suspected
- Patient education: symptoms to watch for (pain, instability)
- Activity modification: reduce high-impact activities if possible
- Early intervention threshold: if progression documented
Observation is not indefinite. If lesions are progressively enlarging, or cross the 2cm threshold, or if any symptoms develop, surgical intervention should be strongly considered. Don't wait for catastrophic failure.
Conservative management is appropriate in this scenario.
Surgical Technique for Revision with Osteolysis
- Familiar anatomy
- Extensile (can extend proximally and distally)
- Excellent visualization of acetabulum and femoral canal
- Higher dislocation risk - requires meticulous repair
- Less dislocation risk
- Can compromise abductors (important to preserve)
- Limited distal extension
- For difficult stem extraction or severe femoral osteolysis
- Preserves abductors
- Allows cement removal and canal preparation
- Fixed with cables or wires at closure
- Protect neurovascular structures - sciatic nerve in posterior, femoral vessels anteriorly
- Preserve bone stock - meticulous removal of implants without additional bone loss
- Expose osteolytic lesions - may need windowing to access posterior column or calcar
- Mark component positions - helps with templating and final positioning
Approach selection depends on prior approach and extent of reconstruction needed.
Complications
- Incidence
- 5-10% after isolated liner exchange
- Prevention/Management
- Complete revision if shell loose, ensure adequate fixation
- Incidence
- 10-20% (higher than primary)
- Prevention/Management
- Large heads, dual mobility, repair soft tissues, correct malposition
- Incidence
- 3-5% (higher than primary)
- Prevention/Management
- Prolonged antibiotics, meticulous technique, rule out infection preop
- Incidence
- 5-10% intraop, 2-5% postop
- Prevention/Management
- Gentle technique, protect osteoporotic bone, bypass weak areas
- Incidence
- 1-3% after revision
- Prevention/Management
- Know anatomy, protect during retraction, avoid excess traction
- Incidence
- Under 1% but catastrophic
- Prevention/Management
- Identify vessels on CT, careful medial wall work, available vascular backup
- Incidence
- 10-20% at 10 years
- Prevention/Management
- Meticulous technique, adequate bone grafting, optimize patient factors
- Incidence
- 10-15%
- Prevention/Management
- Set realistic expectations, rule out infection, PT and pain management
- Massive bone loss before detection
- May require complex reconstruction with allografts, cages
- Multiple surgeries potentially required
- Function may never return to baseline
- Prevention is key: annual surveillance radiographs
- Rare but reported with large heads and thin liners
- Typically rim fractures at impingement sites
- Causes pain, instability, metallosis from shell-head contact
- Prevention: ensure adequate liner thickness (8-10mm minimum), avoid large heads if small cups
- Graft resorption or nonincorporation
- Leads to recurrent bone loss or component loosening
- More common with structural allografts vs morselized
- May require re-revision with alternative fixation strategy
- Common after revision due to bone loss or component positioning
- Patients often tolerate some lengthening better than shortening
- Shoe lift may be needed
- Excessive discrepancy (over 2cm) can cause back pain, gait abnormality
Postoperative Care and Rehabilitation
Post-revision protocol:
- Hip abduction pillow or brace
- DVT prophylaxis (chemoprophylaxis + mechanical)
- Pain management (multimodal analgesia)
- Early mobilization (sit to chair, stand)
- Check drains, neurovascular status
- Physical therapy: progressive weight-bearing per surgeon protocol
- Weight-bearing restrictions depend on bone grafting, fixation
- If structural allograft or pelvic discontinuity: toe-touch weight-bearing 6-12 weeks
- If standard revision without major graft: weight-bearing as tolerated
- Hip precautions (no flexion over 90, no adduction, no internal rotation if posterior approach)
- Gait training with walker or crutches
- Wound check at 2 weeks, remove sutures if non-absorbable
- Continue weight-bearing restrictions per protocol
- Outpatient PT 2-3 times per week
- Hip abductor strengthening exercises
- Monitor for complications (infection, dislocation)
- Radiographs at 6 weeks: assess component position, rule out early loosening
- Progress to full weight-bearing if healing appropriate
- Wean from assistive devices
- Increase strengthening exercises
- Return to driving at 6-8 weeks (if right hip and adequate control)
- Radiographs at 3 months
- Most patients off all assistive devices
- Return to low-impact activities (swimming, cycling, golf)
- Continue strengthening program
- Address any persistent pain or functional limitations
- Radiographs at 1 year, then annually for life
- Full activity as tolerated (avoid high-impact if possible)
- Annual surveillance to detect early failure
- Maintain musculoskeletal fitness and healthy weight
- Patient education on symptoms requiring earlier follow-up
- Standard revision (no major graft): weight-bearing as tolerated from day 1
- Morselized allograft cavitary defects: weight-bearing as tolerated (graft is impacted)
- Structural allograft segmental defects: toe-touch 6 weeks, progressive to full by 12 weeks
- Pelvic discontinuity repair: toe-touch 8-12 weeks minimum
- Periprosthetic fracture fixation: depends on construct stability, often 6-12 weeks protected
- Hip precautions for 6-12 weeks (posterior approach)
- No high-impact activities indefinitely (running, jumping)
- Low-impact activities encouraged (swimming, cycling, golf)
- Return to work: desk job 4-6 weeks, manual labor 3-6 months
SURVEILLANCESURVEILLANCE - Follow-up Protocol
Hook:SURVEILLANCE emphasizes the comprehensive monitoring approach required
Outcomes and Prognosis
Outcomes by intervention:
- 10-Year Survival
- 80-90% stable
- Main Failure Mode
- Progression requiring surgery
- Notes
- Success depends on patient compliance with surveillance
- 10-Year Survival
- 70-80%
- Main Failure Mode
- Unrecognized shell loosening
- Notes
- Best outcomes with strict selection criteria
- 10-Year Survival
- 80-90%
- Main Failure Mode
- Aseptic loosening, infection
- Notes
- Superior to isolated liner exchange in most cases
- 10-Year Survival
- 75-85%
- Main Failure Mode
- Aseptic loosening, dislocation
- Notes
- Depends on bone loss severity and fixation achieved
- Early detection (small lesions, stable components)
- Adequate bone stock or successful grafting
- Well-fixed revision components
- Young age (better healing, longer life expectancy for benefit)
- Absence of comorbidities
- Patient compliance with restrictions
- Delayed detection (massive bone loss)
- Pelvic discontinuity or severe defects
- Prior failed revisions
- Infection
- Medical comorbidities (diabetes, smoking, osteoporosis)
- Obesity
The best outcomes are in preventing osteolysis from occurring in the first place. This is achieved through:
- HXLPE for all primary THAs (reduces wear 90%)
- Optimal component positioning (avoid impingement, edge loading)
- Annual surveillance radiographs (detect early, intervene before catastrophic failure)
- Patient education on lifelong follow-up importance
Guidelines, Registries & Global Practice
Global epidemiology and burden:
Total hip arthroplasty is one of the most commonly performed and successful elective operations worldwide, and primary volumes are rising steeply. In the United States, primary THA demand was projected to grow by 174% to roughly 572,000 procedures per year by 2030, with hip revision demand projected to double by 2026 (Kurtz et al., J Bone Joint Surg Am 2007). As the implanted population grows and ages in situ, the cumulative number of patients at risk of late polyethylene wear and osteolysis increases correspondingly, even though the per-implant risk has fallen sharply with cross-linked bearings. Osteoarthritis is the dominant indication globally (the large majority of primaries), with post-traumatic arthritis, inflammatory arthritis, osteonecrosis and dysplasia accounting for the remainder.
Registry evidence on bearing surfaces (the global picture):
National joint registries — including the AOANJRR (Australia), the NJR (England, Wales, Northern Ireland and the Isle of Man), the AJRR (USA), the Swedish (SHAR), Norwegian and NZJR registries — have been decisive in bearing-surface governance. Two registry-driven lessons dominate:
- Registry signal
- Now the dominant primary bearing; markedly reduced revision for wear/osteolysis since widespread adoption
- Practical consequence
- Reference bearing for most primary THA
- Registry signal
- Historically higher late revision for wear/osteolysis (3x revision vs XLPE in the 20-year RCT, Devane et al. 2025)
- Practical consequence
- Largely superseded for primary THA
- Registry signal
- Registries identified high early revision for adverse reaction to metal debris (pseudotumour, ALTR)
- Practical consequence
- Largely withdrawn from routine practice
- Registry signal
- Very low wear; small risks of squeaking and ceramic fracture
- Practical consequence
- Selective use, often in younger patients
Because cross-linked PE has nearly removed wear as a dominant failure mode, registries now report infection and instability/dislocation as the leading causes of revision in contemporary THA.
Guidelines and consensus, side by side:
There is broad international agreement and few hard inter-guideline conflicts on this topic; the practical recommendations align across regions:
- Position relevant to wear/osteolysis
- Cross-linked PE preferred over conventional PE to reduce wear and osteolysis
- Evidence basis
- Supported by RCT/registry data
- Position relevant to wear/osteolysis
- Use bearings/implants with ≥10-year revision benchmarks (ODEP ratings); routine implant choice favours well-evidenced low-wear bearings
- Evidence basis
- Benchmark- and registry-driven
- Position relevant to wear/osteolysis
- Cross-linked (incl. antioxidant-stabilised) PE endorsed as standard for most primaries; bearing individualised for young/high-demand patients
- Evidence basis
- RCT and registry evidence
- Position relevant to wear/osteolysis
- Define cross-linking, sterilisation and oxidation-resistance testing for UHMWPE bearings
- Evidence basis
- Materials/laboratory standards
Practice variation:
- Bearing choice in young, high-demand patients is the main area of genuine debate: ceramic-on-XLPE and ceramic-on-ceramic are used variably by region and surgeon preference, weighing wear reduction against squeaking/fracture risk and cost.
- Resource setting: in limited-resource settings, conventional UHMWPE and metal-on-PE remain in wider use for cost reasons, so wear-related osteolysis remains a more prominent late problem than in high-income systems that have transitioned almost entirely to cross-linked bearings.
- Pharmacological prevention: bisphosphonates (e.g. alendronate) reduce early periprosthetic bone loss after cementless THA but have not been shown to durably prevent osteolysis, so they are not recommended as a substitute for low-wear bearings (Zeng et al., Orthopedics 2011, systematic review).
Frame this topic globally: cross-linked polyethylene is the international standard bearing, validated by both long-term RCTs (Devane et al. 20-year RCT) and multiple national registries (AOANJRR, NJR and others). The same registries withdrew metal-on-metal after detecting high revision for adverse reaction to metal debris. The remaining live controversy is bearing choice in the young, high-demand patient (ceramic-on-XLPE vs ceramic-on-ceramic).
MCQ Practice Points
Q: What size polyethylene wear particles are most biologically active in causing osteolysis? A: 0.1-1 micrometer. This size range optimally activates macrophages and triggers the inflammatory cascade. Smaller particles (under 0.1μm) are less readily phagocytosed. Larger particles (over 1μm) elicit less inflammatory response.
Q: By approximately what percentage does highly cross-linked polyethylene (HXLPE) reduce wear compared to conventional polyethylene? A: Over 90% (typically 90-95%). HXLPE wear rates are approximately 0.01-0.02mm per year compared to 0.1-0.2mm per year for conventional PE.
Q: What key cytokines are released by macrophages in response to polyethylene wear particles that drive osteolysis? A: TNF-α (tumor necrosis factor alpha), IL-1β (interleukin-1 beta), IL-6, and PGE2. These pro-inflammatory cytokines upregulate RANKL expression, which drives osteoclast differentiation and activation, leading to bone resorption.
Q: What does the term 'effective joint space' refer to in the context of THA osteolysis? A: The pathways by which wear particles access the bone-implant interface. Common pathways include screw holes in acetabular shells, gaps in press-fit fixation, osteotomies, and capsular defects. Particles migrate through these pathways to reach bone and trigger osteolysis.
Q: What is the main trade-off of highly cross-linked polyethylene compared to conventional polyethylene? A: Lower fracture toughness (more brittle). The cross-linking process that increases wear resistance also reduces the material's resistance to crack propagation. However, clinical studies show no increase in mechanical failures when HXLPE is used with appropriate liner thickness and head size.
Q: What is the recommended radiographic surveillance interval for patients with total hip arthroplasty? A: Annual radiographs for life. Osteolysis is typically asymptomatic until late-stage failure. Annual AP and lateral pelvis radiographs allow early detection of osteolysis, implant loosening, or other complications before catastrophic failure occurs.
Q: What is the most important prerequisite for isolated liner exchange in a patient with osteolysis? A: Well-fixed acetabular shell with absolutely no loosening. The shell must be completely stable with no radiolucent lines and no migration. Intraoperative stress testing should confirm stability. If there is any doubt, complete acetabular revision is safer and more durable.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman presents for routine annual follow-up of her right THA performed 12 years ago with conventional polyethylene. She is completely asymptomatic and very active. AP pelvis radiograph shows a 2.5cm radiolucent lesion in DeLee-Charnley zone I (superior acetabulum). There are no radiolucent lines around the cup or stem. How do you manage this?”
“A 72-year-old man with a 15-year-old right THA (conventional PE) presents to the emergency department with sudden onset severe right hip pain and inability to weight-bear after a minor fall at home. Radiograph shows a Vancouver B3 periprosthetic femoral fracture with massive osteolysis around the femoral stem and acetabular component. The stem is clearly loose. How do you manage this complex problem?”
“You are planning a primary THA in a 38-year-old male manual laborer with post-traumatic osteoarthritis. He is very active, plays recreational sports, and has 40-50 years of expected implant service life. He asks why you're recommending HXLPE when he's heard it's 'more brittle' and 'might break.' Discuss your bearing surface decision and address his concerns.”
WEAR MECHANISMS
- Adhesive wear: surface-to-surface molecular bonding and transfer
- Abrasive wear: hard surface plowing through soft PE (scratching)
- Third-body wear: interposed particles (PMMA, metal) acting as abrasives
- Critical particle size: 0.1-1μm (most biologically active)
PARTICLE DISEASE CASCADE
- 1. PE particles generated at bearing surface
- 2. Particles access bone via effective joint space (screw holes, gaps)
- 3. Macrophages recognize and phagocytose particles
- 4. Cytokine release: TNF-α, IL-1β, IL-6, PGE2
- 5. RANKL upregulation drives osteoclast differentiation
- 6. Osteoclast-mediated bone resorption (osteolysis)
HXLPE PROPERTIES
- Manufacturing: 50-100 kGy radiation creates cross-links
- Wear reduction: over 90% vs conventional PE
- Wear rate: 0.01-0.02mm/year (vs 0.1-0.2mm/year conventional)
- Trade-off: lower fracture toughness (more brittle)
- Prevention: adequate thickness (8-10mm), appropriate head size (32-36mm)
- Long-term data: 15-20 year follow-up confirms durability, under 5% osteolysis
SURVEILLANCE PROTOCOL
- Annual AP and lateral pelvis radiographs for life (mandatory)
- Compare to baseline postoperative films
- Look for: radiolucent lines, expanding lesions, component migration
- CT scan to quantify osteolysis if suspected on plain films
- Osteolysis is typically asymptomatic - imaging essential for detection
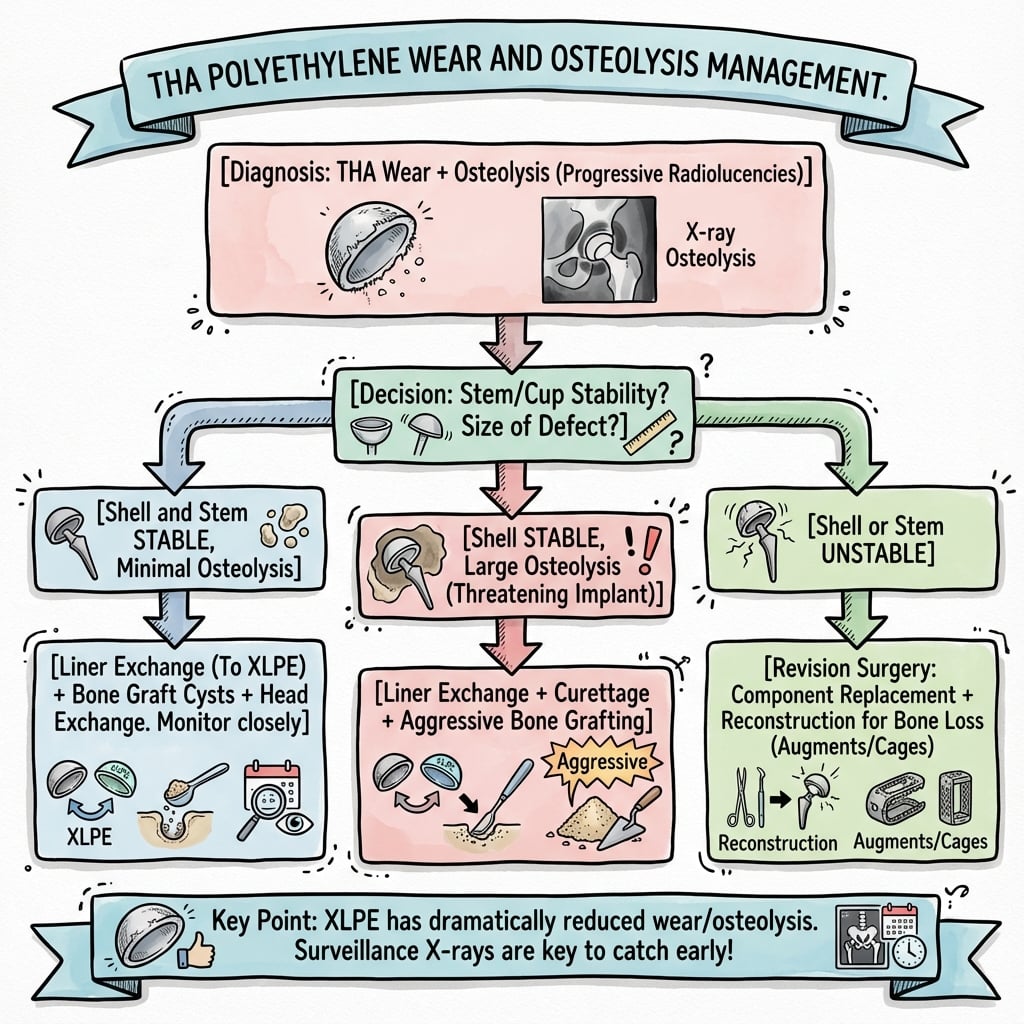
MANAGEMENT ALGORITHM
- Small lesions (under 2cm), stable components: observe with close surveillance
- Large lesions (over 2cm), stable components: isolated liner exchange vs revision
- Isolated liner exchange: strict criteria (well-fixed shell, accessible lesions)
- Complete revision: symptomatic, loose components, large/progressive osteolysis
- Curettage and bone graft all osteolytic lesions
- Use HXLPE liner to prevent recurrent wear
SURGICAL PRINCIPLES
- Acetabular: assess shell stability (stress test intraop), revise if any doubt
- Femoral: bypass osteolytic areas with long stem (4-6cm contact in good bone)
- Bone grafting: morselized for cavitary, structural for segmental defects
- Impaction grafting technique for contained defects
- HXLPE liner essential to prevent recurrence
- Large head (32-36mm) to minimize dislocation risk
KEY EXAM PEARLS
- Osteolysis is biological (particle disease), not purely mechanical
- Prevention is superior to treatment: HXLPE for all primary THAs
- Annual surveillance radiographs are non-negotiable for life
- Asymptomatic osteolysis is the ideal time to intervene (before disaster)
- AOANJRR data: wear revisions declined dramatically with HXLPE adoption
- Metal-on-metal abandoned due to adverse reactions and pseudotumor
Evidence Base
- Longest-term RCT to date: 122 patients randomised to cross-linked (Marathon) versus conventional (Enduron) liners with otherwise identical components, minimum 20-year follow-up.
- After bedding-in, steady-state wear was 0.034 mm/year for XLPE versus 0.181 mm/year for conventional PE.
- Conventional-PE liners had a revision rate roughly three times higher than XLPE (28 versus 9 of the 37 revisions).
- 768 primary THAs (head sizes 26-36 mm) across eight centres followed to 7-13 years.
- Serial radiographs showed no periprosthetic osteolysis in any of the three studies.
- Mean femoral head penetration did not correlate with time in vivo for standard head sizes; 36 mm heads trended higher but stayed below the osteolysis threshold.
- Wear debris primarily targets macrophages and osteoclast-precursor cells, with osteoblasts, fibroblasts and lymphocytes also involved.
- Particles activate MAP-kinase pathways and NF-κB, up-regulating pro-inflammatory signalling and RANKL while suppressing protective cytokines.
- Reducing particle size to lower wear may paradoxically increase biological activity; no approved pharmacological treatment for osteolysis exists.
- 199 patients randomised to a vitamin E-blended HXLPE cup versus a conventional UHMWPE monoblock cup.
- Femoral head penetration was lower with vitamin E HXLPE (0.028 mm/year) than UHMWPE (0.035 mm/year).
- Six-year survival to revision was 98% for both cups with no aseptic loosening and no adverse reactions attributable to vitamin E.
- 96 acetabular revisions for wear/osteolysis compared isolated liner exchange, cemented liner into a well-fixed shell, full acetabular revision, and roof-ring/antiprotrusio cage (mean 5.7-year follow-up).
- Component-retention procedures (liner exchange / cemented liner) had a lower reoperation risk but achieved complete bone-defect healing in only 27% versus 57% with full revision.
- All four strategies significantly improved Harris Hip Score.
- 138 cementless acetabular revisions followed to a minimum of 20 years.
- Survivorship with shell revision for aseptic loosening as the end point was 95% at 20 years.
- Reoperations for polyethylene wear and osteolysis first appeared around 12 years, reinforcing the need for lifelong surveillance even after revision.
- US primary THA demand projected to grow 174% to 572,000 procedures by 2030.
- Hip revision demand projected to double by 2026.
- Quantifies the rising population at risk of wear- and osteolysis-related failure as primary volumes expand.
- Across major registries (AOANJRR, NJR England & Wales), metal- or ceramic-on-cross-linked polyethylene is now the dominant primary THA bearing.
- Metal-on-metal bearings were largely withdrawn after registries identified high revision rates for adverse reaction to metal debris.
- Registry revision for wear/osteolysis has fallen substantially since widespread cross-linked PE adoption, shifting the leading revision causes towards infection and instability.