Plan the reconstruction before entering theatre
- Templating is not just implant sizing; it is the plan for hip centre, leg length, offset, fixation, exposure and backup equipment.
- A poorly positioned or uncalibrated radiograph can make an accurate-looking template wrong.
- The acetabular plan sets hip centre, cup size, medialisation, inclination, version and bone coverage.
- The femoral plan sets stem size, fixation, neck cut, offset, version, leg length and need for special stems or osteotomy.
- The final implant decision is made intraoperatively after exposure, bone assessment, trial reduction, stability and leg-length checks.
- “Check the radiograph before templating: AP pelvis quality, rotation, calibration marker, lateral view and full femur when needed.
- “Templating the contralateral hip is helpful only if the opposite hip is normal and not itself dysplastic, arthritic or deformed.
- “Lengthening the leg without restoring offset and stability is not a good plan.
- “In complex anatomy, plan the backup before incision: smaller/larger stems, cemented option, modular stem, augments, cables, plates or dual mobility.
- “Spinopelvic stiffness changes functional cup position; a safe plan includes standing and sitting assessment when instability risk is high.
THA Templating and Preoperative Planning
A template that predicts a stem or cup size is useful, but it is not the operation. The surgeon must still judge bone quality, press-fit, version, offset, leg length, stability and soft-tissue tension in theatre.

CALIBRTemplating Sequence
Hook:CALIBR keeps templating anchored to calibration, biomechanics and operative reality.
MARKERRadiograph Quality
Hook:MARKER makes the image quality check explicit before sizing implants.
BONESBackup Plan
Hook:BONES is the equipment and bailout checklist before starting a THA.
Overview and Epidemiology
Preoperative planning for total hip arthroplasty is the process of deciding how the arthritic or fractured hip will be reconstructed before surgery. Templating is one part of that process. It estimates component size and position, but the wider plan also includes exposure, fixation, leg length, offset, centre of rotation, stability risk, blood loss, implant inventory and bailout options.
The need for planning is universal. A routine osteoarthritis hip still needs an AP pelvis, a lateral view and a clear plan for cup and stem sizing. A complex hip requires more: dysplasia, protrusio, post-traumatic deformity, previous osteotomy, retained metalwork, childhood hip disease, fracture neck of femur, obesity, osteoporosis and spinal stiffness can all make a standard template misleading.
It clarifies the intended hip centre, component size range, neck cut, offset option, leg-length goal and equipment list. It also makes the surgeon think through the case before the incision.
It cannot assess real bone quality, guarantee press-fit, replace safe exposure, correct a bad radiograph, or remove the need for trial reduction and intraoperative judgement.
Planning is broader than component size
- Preoperative planning in primary THA is a structured reconstruction exercise.
- The plan includes restoration of anatomy, implant selection and anticipation of technical problems.
- The template helps the operation only when the image and assumptions are correct.
Pathophysiology/Mechanism
The mechanism of planning is biomechanical reconstruction. The native hip transmits load through a centre of rotation, a femoral offset, an abductor lever arm and a leg-length relationship. THA changes these variables. If the reconstruction shortens offset, the abductors work at a disadvantage and the hip may feel weak or unstable. If length is overcorrected, the patient may have nerve stretch, pain or dissatisfaction. If the cup is placed too high or too lateral, hip mechanics and wear may suffer. If the femoral stem is undersized or malaligned, fixation may fail.
The most important planning variables are:
- Hip centre: restore or deliberately reconstruct the centre of rotation.
- Cup position: size, medialisation, inclination, version, coverage and screw plan if needed.
- Femoral fixation: cemented, cementless, hybrid, modular, long stem or special implant.
- Neck cut: level and orientation that allow the planned stem and length restoration.
- Offset: femoral and global offset, abductor tension and impingement-free motion.
- Leg length: planned correction balanced against nerve and soft-tissue safety.
- Version and stability: combined anteversion, impingement, spinopelvic mechanics and head/liner choice.
Lengthening alone can make a hip tight without restoring abductor mechanics. Offset restoration improves abductor tension and stability, but excessive offset can increase soft-tissue tension and trochanteric pain. The plan must balance both.
Classification
For templating, classification should make the case easier to plan. The most useful classification is not a single named system; it is a practical complexity assessment.
- Planning implication
- Contralateral hip may help estimate anatomy if normal.
- Typical action
- 2D digital template from calibrated AP pelvis and lateral hip.
- Planning implication
- Routine cemented or cementless fixation according to age and bone quality.
- Typical action
- Prepare expected size plus adjacent sizes.
- Planning implication
- Aim to restore anatomy and stability.
- Typical action
- Confirm intraoperatively with trials and landmarks.
Clinical Presentation/Assessment
Clinical assessment for THA templating is not just the diagnosis of arthritis. It is an operative planning assessment.
History
Ask about pain, walking distance, walking aids, instability symptoms, previous hip surgery, childhood hip disease, fracture history, spine disease, neurological disease, infection risk, anticoagulation, metal allergy history and patient priorities. Clarify perceived leg-length inequality, shoe raises and whether the patient would prefer equal length, stability or nerve safety if a tradeoff is unavoidable.
Examination
Examine gait, Trendelenburg sign, fixed flexion deformity, abduction contracture, true and apparent leg length, pelvic obliquity, lumbar stiffness, rotational profile, hip range of motion, abductor power, knee deformity, foot deformity and neurovascular baseline. The examination helps explain why the radiographic plan may not match the functional limb length.
- What it means
- Apparent leg length may not equal bony leg length.
- Planning response
- Plan standing assessment and counsel carefully.
- What it means
- Cup position and dislocation risk are affected by spinopelvic mechanics.
- Planning response
- Use standing and sitting lateral spine-pelvis views when indicated.
- What it means
- Offset restoration and stability are more important.
- Planning response
- Consider high-offset options and stability-enhancing bearing where appropriate.
- What it means
- The canal may not accept a routine stem.
- Planning response
- Order full femur imaging and consider CT or modular stem.
- What it means
- Baseline documentation is essential and nerve stretch risk may limit lengthening.
- Planning response
- Avoid excessive lengthening and document preoperative status.
Imaging and Investigations
Radiograph quality determines template quality. If the image is not fit for planning, the safest decision is to repeat or extend imaging.

Standard imaging set
- AP pelvis: both hips, pelvis centred, visible teardrops, obturator foramina, lesser trochanters and proximal femora.
- Cross-table lateral or lateral hip: femoral morphology, version clues, osteophytes and anterior/posterior deformity.
- Calibration marker: placed at the level of the greater trochanter or hip where possible; poor marker position reduces accuracy.
- Full-length femur: previous fracture, osteotomy, deformity, retained implants, long stem planning or suspected canal abnormality.
- Standing and sitting lateral pelvis/spine: spinal stiffness, lumbar fusion, sagittal imbalance or high dislocation-risk planning.
CT, EOS and three-dimensional planning
CT or EOS is useful when two-dimensional templating cannot answer the question: severe dysplasia, protrusio, post-traumatic deformity, previous osteotomy, rotational deformity, retained metalwork, custom implant planning or unclear acetabular bone stock. Three-dimensional planning can improve anatomical understanding and size prediction in complex cases, but it does not remove the need for intraoperative judgement.
Radiographic magnification and marker placement matter
- Radiographic technique and calibration marker position affect magnification accuracy.
- A marker that is not at the hip level can create sizing error.
- The image must be checked before the implant size estimate is trusted.
Management
Management in this topic means the planning process that leads to a safe operation.
Plan the cup before the stem. Identify the teardrop, native acetabular floor, superolateral acetabular margin and intended hip centre. Choose cup size that gives stable bone contact without excessive medialisation, over-reaming or loss of bone stock.
- Decision
- Restore native centre or deliberately plan a safe alternative.
- Key risk
- High or lateral centre can impair mechanics.
- Decision
- Estimate size and adjacent sizes.
- Key risk
- Oversizing can fracture or remove bone; undersizing can be unstable.
- Decision
- Use controlled medialisation to improve coverage when appropriate.
- Key risk
- Protrusio or thin medial wall needs protection.
- Decision
- Plan safe orientation adjusted for anatomy and spinopelvic risk.
- Key risk
- Malposition increases instability, edge loading and wear.
- Decision
- Plan screws, graft, augments, cage or custom options when needed.
- Key risk
- Unrecognised deficiency leads to poor fixation.
Surgical Technique
Templating technique should be systematic and repeatable.
Step-by-step 2D digital templating
- Confirm patient, side and image quality.
- Calibrate magnification using a marker at hip level when available.
- Draw or recognise pelvic reference lines and check rotation.
- Template the acetabulum: hip centre, cup size, medialisation, inclination, coverage and screw plan.
- Template the femur: neck cut, stem size, fixation, offset option, version and canal fit.
- Compare planned reconstruction with the contralateral side only if the opposite hip is reliable.
- Estimate leg-length correction and offset restoration.
- Record the expected sizes and adjacent sizes.
- List implants, instruments and backup equipment.
- Reassess the plan intraoperatively after exposure, trialling and stability testing.
Intraoperative checks
The operation should test the preoperative plan. Check the neck cut before broaching. Assess acetabular landmarks before reaming. During trial reduction, assess stability in extension and external rotation, flexion and internal rotation, soft-tissue tension, impingement, leg length and offset. If the trial hip is unstable, do not close because the template looked acceptable.
If the planned size does not fit, the bone feels poor, the cup is unstable, the femur cracks or the trial hip is unstable, change the plan. The purpose of templating is preparation, not forced execution.
Complex Planning
Complex primary THA should be recognised before the day of surgery. The radiograph below shows a dysplastic hip reconstruction example. It is included because complex anatomy requires a different planning mindset: hip centre, acetabular deficiency, femoral canal shape, version, shortening, offset and backup implants all need to be considered before theatre.

- Imaging addition
- CT or three-dimensional planning when needed.
- Planning addition
- Small cup range, medialisation, augments/graft, narrow stem, modularity and shortening osteotomy plan.
- Imaging addition
- AP pelvis plus CT if medial wall is unclear.
- Planning addition
- Avoid uncontrolled medial migration; prepare graft or reinforcement strategy.
- Imaging addition
- Full-length femur and CT if canal/version unclear.
- Planning addition
- Hardware removal, long/modular stem, cables and fracture plan.
- Imaging addition
- Template opposite hip if reliable; assess bone quality.
- Planning addition
- Cemented stem, stability strategy and frailty-related perioperative plan.
- Imaging addition
- Standing and sitting lateral pelvis/spine views.
- Planning addition
- Functional cup position and dual mobility discussion when risk is high.
Complications
Templating errors are not theoretical; they appear as operative and postoperative complications.
- Planning failure
- Clinical and radiographic length were not reconciled.
- Prevention
- Assess pelvic obliquity, true/apparent length and planned correction.
- Planning failure
- Offset was reduced or trochanteric mechanics were ignored.
- Prevention
- Template femoral and global offset and trial abductor tension.
- Planning failure
- Spinopelvic stiffness, component position or soft-tissue tension was not planned.
- Prevention
- Assess stability risk and plan cup orientation, head/liner and offset.
- Planning failure
- Stem was oversized or bone quality underestimated.
- Prevention
- Prepare adjacent sizes, cables and cemented option.
- Planning failure
- Acetabular deficiency or protrusio was missed.
- Prevention
- Plan bone stock, medial wall, screw fixation, graft or augment.
- Planning failure
- Inventory was not matched to the plan.
- Prevention
- Record expected and backup sizes before theatre.
Clinical Pitfalls

- Why it fails
- Cup position, length and offset estimates are distorted.
- Safer approach
- Repeat imaging or interpret with caution.
- Why it fails
- Magnification can make the planned implant size wrong.
- Safer approach
- Use marker, known implant, or prepare adjacent sizes.
- Why it fails
- Anterior bowing, femoral shape and deformity can be missed.
- Safer approach
- Always review lateral and full femur when indicated.
- Why it fails
- The other hip may also be dysplastic, arthritic or deformed.
- Safer approach
- Use it only if it is genuinely normal.
- Why it fails
- Unexpected bone, fracture or instability forces improvisation.
- Safer approach
- Write expected and backup implants into the plan.
Why It Matters
Poor planning causes predictable problems: wrong component availability, poor exposure strategy, inadequate restoration of leg length or offset, malpositioned hip centre, unstable trial reduction, intraoperative fracture, unplanned cement conversion, inability to remove metalwork or a rushed decision to use an implant that is not ideal.
Good planning improves theatre efficiency and reduces avoidable surprises. It also improves consent, because the surgeon can explain why the hip is routine or complex, what reconstruction is intended and what alternatives may be needed if the anatomy is different from the radiograph.
- Why it matters
- Magnification error changes component sizing.
- Example of changed plan
- Repeat AP pelvis or use known implant/marker calibration.
- Why it matters
- Hip centre affects length, offset, abductor mechanics and cup coverage.
- Example of changed plan
- Medialise a protrusio cup or use graft/augment in dysplasia.
- Why it matters
- Canal shape, deformity and bone quality determine fixation.
- Example of changed plan
- Use cemented stem, modular stem, short stem, long stem or osteotomy.
- Why it matters
- Spinopelvic stiffness and soft-tissue deficiency affect cup position and bearing choice.
- Example of changed plan
- Use adjusted cup orientation, larger head or dual mobility.
- Why it matters
- The plan must survive unexpected fracture, poor bone or unavailable size.
- Example of changed plan
- Have cables, cement, revision stem, augments and alternative liners ready.
Guidelines, Registries and Global Practice
THA is one of the most studied operations in orthopaedics, with more than one million primaries performed worldwide each year and registries tracking implant survival across millions of cases. Planning principles are globally consistent, but imaging access and implant availability vary widely.
Global epidemiology
- Hip osteoarthritis is the dominant indication in high-income settings; in many lower- and middle-income regions, sequelae of childhood hip disease, dysplasia, post-traumatic deformity and avascular necrosis make a larger share of the templating workload, raising the proportion of complex primaries.
- Demand is rising with ageing populations; THA volumes are projected to increase substantially over the coming decades across most registry nations.
Society guidance, side by side
- Emphasis relevant to templating
- Evidence-based management of hip osteoarthritis and shared decision-making before arthroplasty.
- Practical takeaway
- Plan documented reconstruction goals and consent before listing.
- Emphasis relevant to templating
- Standardised pathways, calibrated digital templating and implants with strong registry survivorship (ODEP ratings).
- Practical takeaway
- Choose implants with proven survival and template on quality images.
- Emphasis relevant to templating
- Restoration of hip biomechanics: centre of rotation, offset and leg length.
- Practical takeaway
- Plan biomechanics, not just implant size.
- Emphasis relevant to templating
- Spinopelvic assessment and functional cup orientation in at-risk patients.
- Practical takeaway
- Add standing and sitting imaging when instability risk is high.
Registry signals that inform planning
- Large arthroplasty registries (NJR for England, Wales, Northern Ireland and the Isle of Man; AOANJRR Australia; AJRR US; the Swedish and Norwegian registries; NZJR) track revision and implant survival by fixation, bearing and head size.
- Registry-level findings that shape the plan: larger femoral heads and dual-mobility constructs reduce dislocation-related revision; cemented fixation lowers periprosthetic fracture risk in older patients with poor bone; and implant choice should favour constructs with documented long-term survivorship rather than novel designs without registry data.
High- versus limited-resource practice
- Well-resourced setting
- Calibrated digital radiographs, CT or EOS for complex cases, commercial software.
- Limited-resource setting
- Plain film with acetate overlays or a known-diameter marker; PACS plus tablet templating shown to match commercial software.
- Well-resourced setting
- Full range plus backup stems, augments, dual mobility and revision options on the shelf.
- Limited-resource setting
- Restricted range; plan around available sizes and prepare cemented fallback.
- Well-resourced setting
- 3D planning, custom or modular implants, navigation.
- Limited-resource setting
- Greater reliance on careful 2D planning, contralateral comparison and intraoperative judgement.
When asked to justify an implant, a strong answer anchors to registry survivorship and biomechanical restoration rather than personal preference. Choosing a construct with proven long-term survival and planning offset, leg length and stability is more defensible than chasing a novel design.
Areas of Uncertainty and Controversy
Templating is mature but several questions remain genuinely debated, and examiners reward a candidate who can state both sides.
- Argument for
- Randomised data show far higher exact size and offset prediction than 2D.
- Argument against / nuance
- Added radiation, cost and time; most primary hips are reconstructed accurately with good 2D radiographs plus intraoperative trialling.
- Argument for
- Magnification varies widely with habitus and geometry, so markers reduce sizing error.
- Argument against / nuance
- Marker malposition can introduce its own error; some series show little size difference with versus without a marker (KingMark data).
- Argument for
- Reduces dislocation in spinopelvic-imbalance and high-risk patients.
- Argument against / nuance
- Concerns over intraprosthetic dislocation, cost and lack of very long-term registry data in younger patients.
- Argument for
- Spinopelvic imbalance moves the functional safe zone; static Lewinnek targets miss it.
- Argument against / nuance
- No single validated functional target; over-correction can create new impingement.
- Argument for
- Speeds planning and may standardise output.
- Argument against / nuance
- Still requires verification against the actual radiograph and intraoperative judgement; not a replacement for the surgeon.
Summary
THA templating is a structured reconstruction plan. Start with adequate calibrated imaging, define the clinical goal, then plan the acetabulum, femur, leg length, offset, stability and backup implants. The plan should be specific enough to prepare theatre and consent the patient, but flexible enough to change when the bone, trials or stability assessment prove that the template is wrong.
References
- 1Della Valle AG, Padgett DE, Salvati EA. "Preoperative planning for primary total hip arthroplasty.". Journal of the American Academy of Orthopaedic Surgeons. 2005PubMed
- 2Alnahhal A, Aslam-Pervez N, Sheikh HQ. "Templating Hip Arthroplasty.". Open Access Macedonian Journal of Medical Sciences. 2019PubMed
- 3Colombi A, Schena D, Castelli CC. "Total hip arthroplasty planning.". EFORT Open Reviews. 2019PubMed
- 4Holliday M, Steward A. "Pre-operative templating for total hip arthroplasty: How does radiographic technique and calibration marker placement affect image magnification?". Journal of Medical Radiation Sciences. 2021PubMed
- 5Whiddon DR, Bono JV. "Digital templating in total hip arthroplasty.". Instructional Course Lectures. 2008PubMed
- 6Sariali E, et al.. "Accuracy of the preoperative planning for cementless total hip arthroplasty. A randomised comparison between three-dimensional computerised planning and conventional templating.". Orthopaedics and Traumatology: Surgery and Research. 2012PubMed
- 7Holzer LA, et al.. "The accuracy of digital templating in uncemented total hip arthroplasty.". Archives of Orthopaedic and Trauma Surgery. 2019PubMed
- 8Pongkunakorn A, et al.. "Digital Templating of THA Using PACS and an iPhone or iPad is as Accurate as Commercial Digital Templating Software.". Clinical Orthopaedics and Related Research. 2023PubMed
- 9Girgis SF, et al.. "The Accuracy of Digital Preoperative Templating in Primary Total Hip Replacements.". Cureus. 2023PubMed
- 10Buller LT, et al.. "EOS Imaging is Accurate and Reproducible for Preoperative Total Hip Arthroplasty Templating.". Journal of Arthroplasty. 2021PubMed
Clinical Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old has end-stage hip osteoarthritis and is listed for primary THA. The AP pelvis has a calibration marker, but the pelvis is rotated and the lateral hip is poor. How do you proceed with templating?”
“A patient with severe dysplastic hip arthritis is planned for THA. The femur is narrow and anteverted, the acetabulum is deficient and the leg is short. What changes in your preoperative plan?”
“A 72-year-old with a previous L3 to S1 lumbar fusion is listed for primary THA for osteoarthritis. The referring team asks whether anything changes in your planning. What is your approach to templating and component selection?”
Core Principle
- Templating is a reconstruction plan, not just implant sizing.
- Bad radiographs produce bad plans.
- The intraoperative trial must confirm or change the preoperative plan.
Image Set
- AP pelvis, lateral hip and calibration marker are standard.
- Full femur is needed for deformity, previous osteotomy, retained implants or long stems.
- Standing and sitting spine-pelvis views are useful for high instability-risk patients.
Acetabulum
- Plan hip centre, cup size, medialisation, inclination, version and coverage.
- Check protrusio, dysplasia and bone deficiency before theatre.
- Prepare screws, graft, augments or revision shells when indicated.
Femur
- Plan fixation, stem size, neck cut, offset, version and canal fit.
- Prepare adjacent sizes and backup fixation.
- Cemented, modular, long or narrow stems may be needed in complex anatomy.
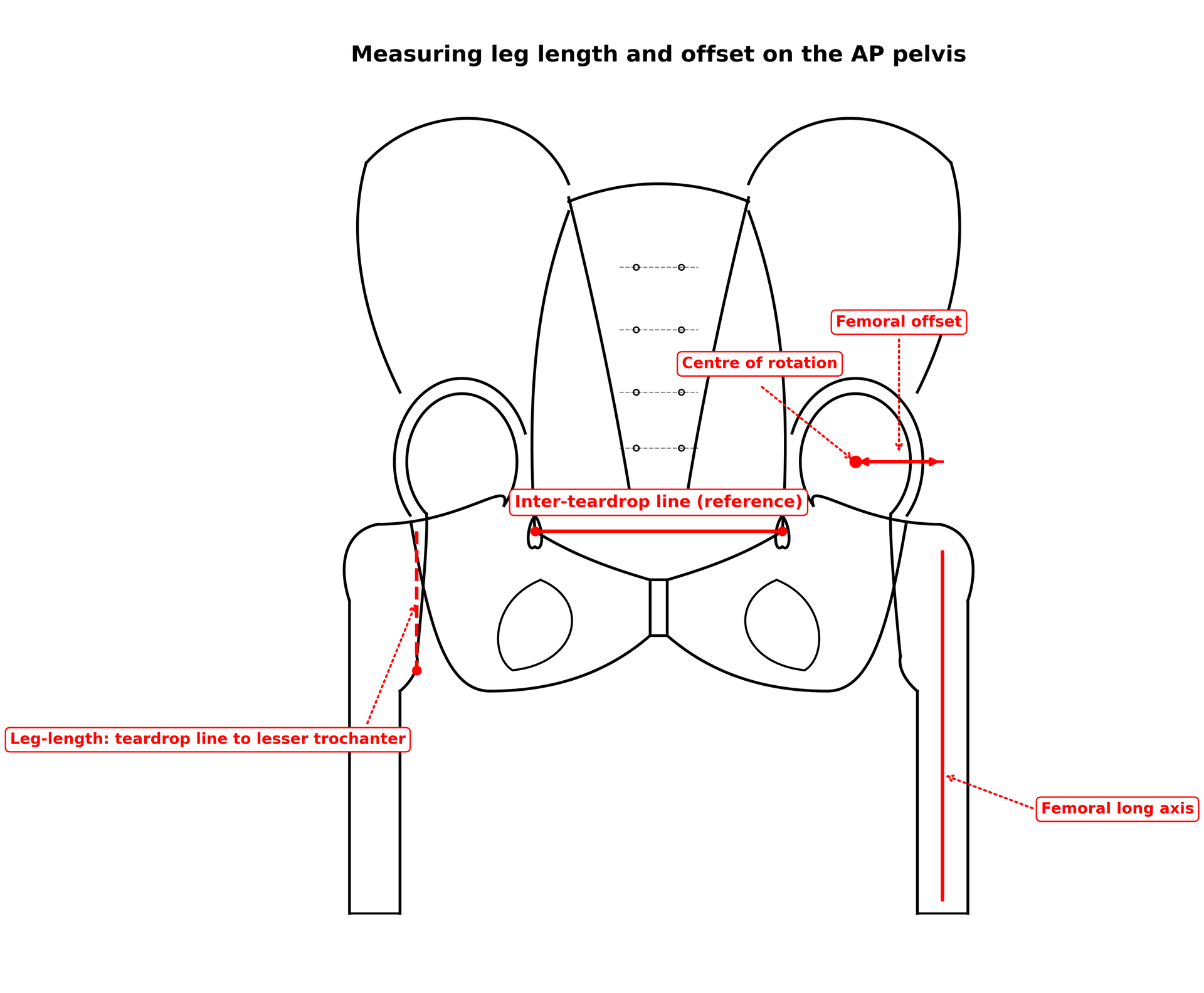
Biomechanics
- Restore leg length and offset together.
- Account for pelvic obliquity and spine stiffness.
- Trial stability and impingement before accepting final implants.
Pitfalls
- No calibration marker, rotated pelvis and poor lateral view.
- Blindly copying the opposite hip.
- No backup sizes or stability strategy.
- Ignoring spinopelvic mechanics in high-risk patients.
Evidence Summary
The literature supports templating as a useful planning tool, but not as a perfect size predictor. Digital templating commonly predicts implant size within one size in many series, with accuracy affected by radiograph quality, calibration, body habitus, implant system, surgeon experience and abnormal anatomy. Three-dimensional planning may improve anatomical understanding and size prediction in complex cases, but routine primary THA still depends on good radiographs and intraoperative judgement.
Templating Hip Arthroplasty
- Templating is widely used for implant selection and reconstruction planning.
- Accuracy varies across studies and methods.
- Calibration and radiographic technique are recurring sources of error.
Digital templating accuracy and its limits
- Exact size prediction was achieved in only 42% of femoral and 37% of acetabular components, but 87% of femoral and 78% of acetabular components were accurate within one size.
- Femoral templating was significantly more reliable when performed by a senior surgeon than a resident.
- Overweight and obesity reduced femoral templating accuracy, whereas acetabular accuracy was unaffected by experience or BMI.
Total hip arthroplasty planning
- Modern THA planning includes component position, hip biomechanics and patient-specific anatomy.
- Spinopelvic mechanics and functional cup orientation are important in selected patients.
- Planning should be adapted to patient anatomy and instability risk.
3D CT planning outperforms 2D templating for size and offset
- In a randomised comparison of cementless THA, exact prediction of both stem and cup size was achieved in 96% with 3D CT planning versus only 16% with conventional 2D templating.
- Leg-length prediction was tighter with 3D planning (mean error minus 1.8 mm, SD 3.6) than with 2D templating (mean 1.37 mm, SD 6.4).
- Femoral offset was also predicted more reliably with 3D planning, comparable to navigation.
EOS imaging is accurate and reproducible for templating
- EOS templating predicted the exact acetabular and femoral component size in 71% and 66% of cases respectively, and within one size in 98%.
- Exact size prediction was significantly more likely with EOS than with conventional radiographs, with excellent interobserver agreement.
- EOS delivers lower radiation dose than conventional radiographs and supports three-dimensional reconstruction.