Quadratus Femoris Space Narrowing | Posterior Hip Pain | MRI QF Oedema
- Ischiofemoral space (IFS) measured on axial MRI between lateral ischial cortex and medial lesser trochanter cortex
- Normal IFS is greater than 25 mm; values less than 15 mm are diagnostic of impingement
- Quadratus femoris space (QFS) measured between converging muscle bellies of QF and psoas/iliacus tendons
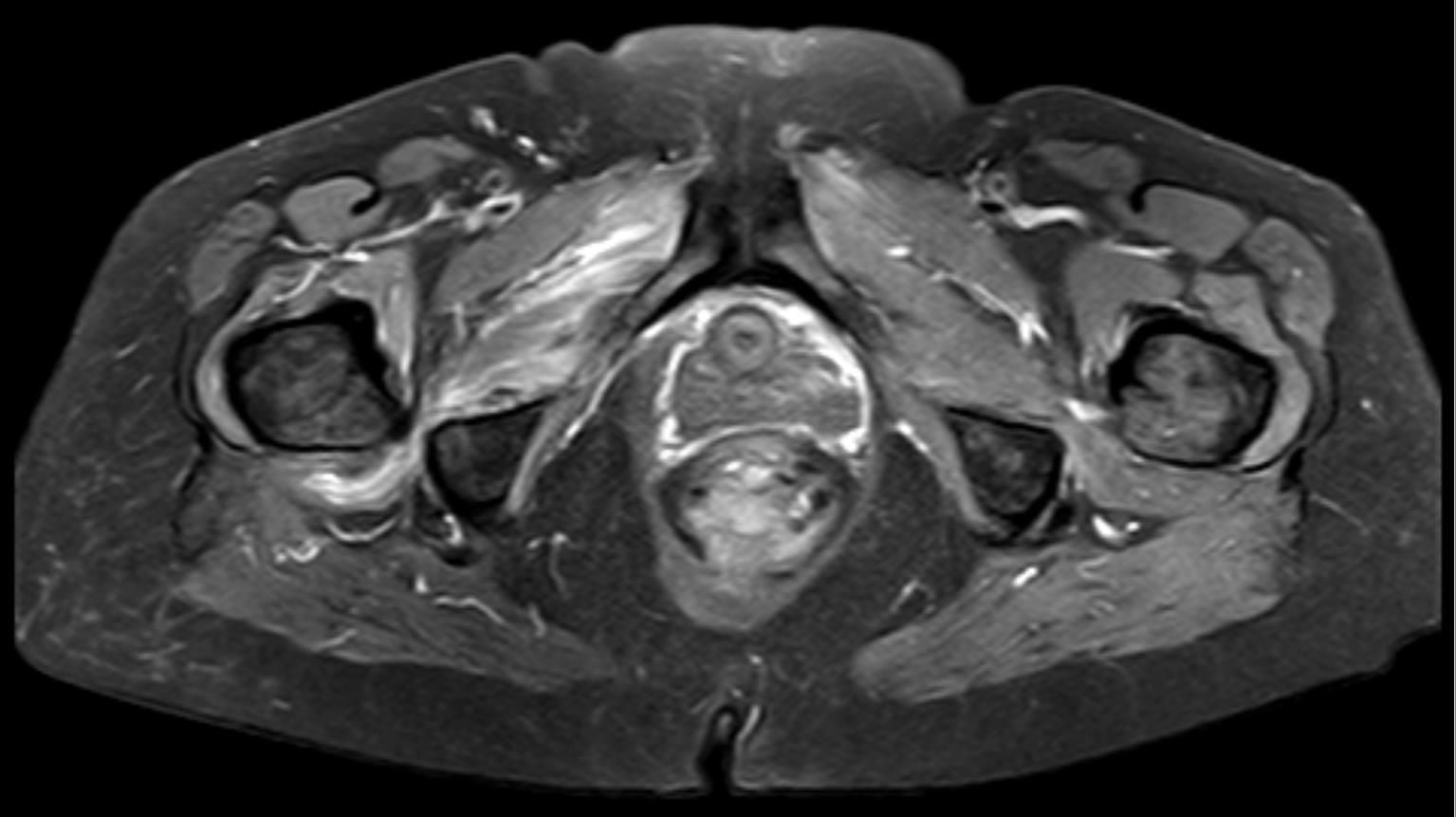
- MRI shows QF muscle oedema (T2/STIR hyperintensity) as the hallmark finding
- Conservative management succeeds in approximately 80 percent of patients; surgery reserved for refractory cases
- “Posterior hip/buttock pain reproduced by long-stride walking or extension-adduction-external rotation
- “Differential: piriformis syndrome, hamstring origin tendinopathy, lumbar radiculopathy, FAI
- “Measure IFS and QFS on axial MRI at the level of the quadratus femoris
- “Endoscopic lesser trochanter osteoplasty is the gold-standard surgical option
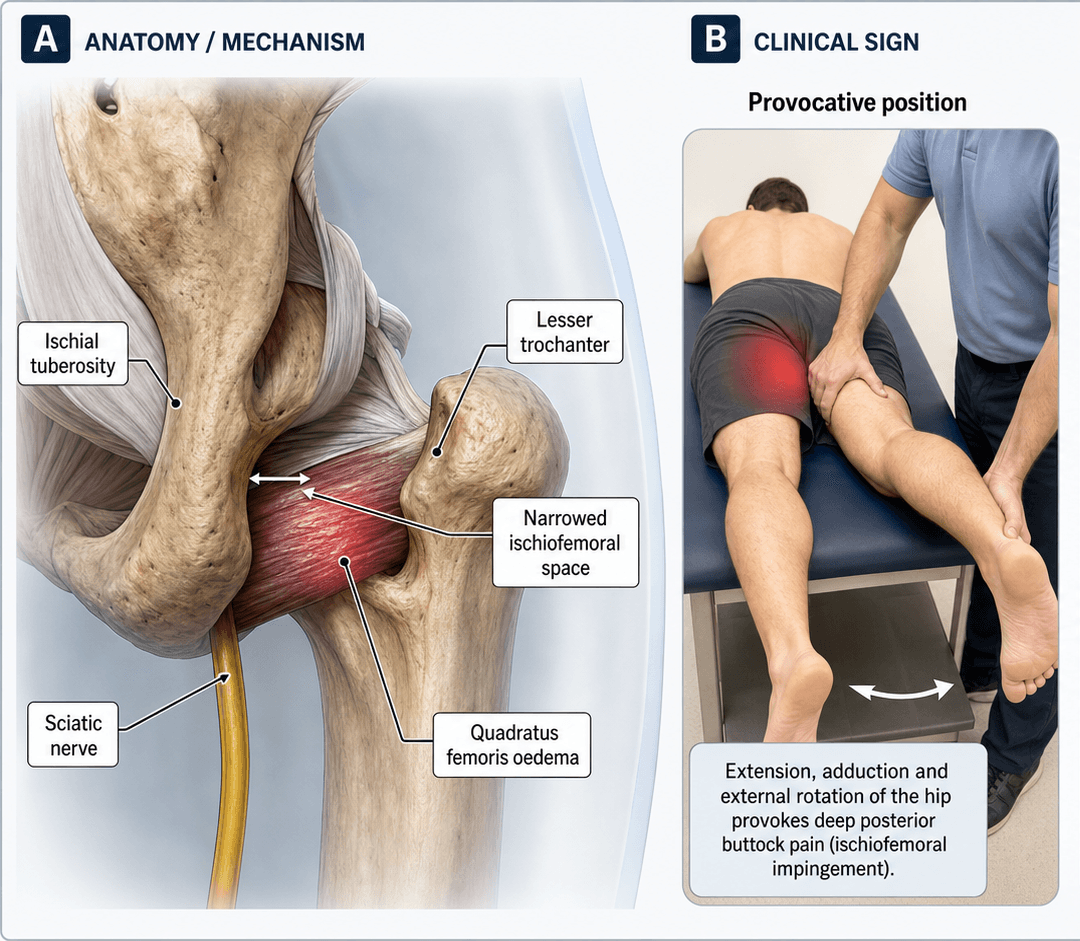
Quadratus femoris runs from the lateral ischial tuberosity to the quadrate tubercle of the proximal femur. It is compressed in the narrowed space between the ischium and the lesser trochanter. The ischiofemoral space (IFS) and quadratus femoris space (QFS) are measured on axial MRI.
Posterior hip and deep buttock pain worsened by long-stride walking, extension, and adduction. Pain may radiate distally. Often mistaken for piriformis syndrome or hamstring pathology. Female predominance approximately 3:1.
QF muscle oedema on T2/FS or STIR sequences is the hallmark. Measure IFS (ischium to lesser trochanter) and QFS (between converging soft tissues) on axial cuts. IFS less than 15 mm and QFS less than 10 mm suggest impingement.
Conservative first: activity modification, NSAIDs, physiotherapy (pelvic tilt correction, gait retraining), image-guided corticosteroid injection. Surgery (endoscopic osteoplasty) reserved for refractory cases failing 3 to 6 months of non-operative care.
- Diagnosis
- MRI: IFS less than 15 mm, QF oedema
- Treatment
- Activity modification + physiotherapy + injection
- Key Pearl
- Most respond to conservative care (approximately 80 percent)
- Diagnosis
- MRI: narrowed IFS from medialized cup or prominent LT
- Treatment
- Injection first; consider component revision vs osteoplasty
- Key Pearl
- Secondary IFI must address underlying surgical cause
- Diagnosis
- Confirmed IFI with reproducible clinical signs
- Treatment
- Endoscopic (or open) lesser trochanter osteoplasty
- Key Pearl
- Relieve QF compression; avoid sciatic nerve injury
SPACEIschiofemoral Impingement MRI Measurements
Hook:SPACE the axial MRI at the QF level to measure ischiofemoral narrowing!
Overview and Epidemiology
Ischiofemoral impingement (IFI) is an increasingly recognised but still under-diagnosed cause of posterior hip and deep buttock pain. It results from narrowing of the space between the ischial tuberosity and the lesser trochanter, compressing the quadratus femoris muscle and, in some cases, the sciatic nerve. The condition was first described by Johnson in 1977 but gained widespread attention only in the MRI era. A high index of suspicion is required because symptoms overlap with piriformis syndrome, hamstring origin tendinopathy, and lumbar radiculopathy.
- Female predominance: approximately 3:1 ratio
- Typical age: 30 to 70 years (peak 40 to 60 years)
- Bilateral in approximately 25 percent of cases
- Post-THA: accounts for a significant proportion of secondary IFI
- Underdiagnosed: often mistaken for piriformis or hamstring pathology
- Posterior hip pain: limits walking distance, sitting tolerance
- Functional limitation: long-stride walking, stairs, running
- Quality of life: chronic pain if undiagnosed, analogous to FAI before its recognition
- Iatrogenic risk: post-THA medialized cup or increased offset can provoke IFI
Pathophysiology
The ischiofemoral space (IFS) is the narrowest distance between the lateral cortex of the ischial tuberosity (at the level of the quadratus femoris origin) and the medial cortex of the lesser trochanter. The quadratus femoris space (QFS) is the narrowest distance between the superolateral surface of the hamstring tendons and the posteromedial surface of the iliopsoas tendon or lesser trochanter. The quadratus femoris muscle occupies this interval. When the space narrows (whether from developmental bony morphology, post-surgical change, or pathological processes), the QF muscle is compressed against the ischium and lesser trochanter during hip extension and adduction, leading to mechanical impingement, muscle oedema, and eventually fatty infiltration or tearing.
- Landmarks
- Lateral ischium to medial lesser trochanter
- Normal Value
- Greater than 25 mm (approximate)
- Impingement Threshold
- Less than 15 mm
- Landmarks
- Hamstring tendons to iliopsoas/LT
- Normal Value
- Greater than 15 mm (approximate)
- Impingement Threshold
- Less than 10 mm
- Landmarks
- T2/STIR signal intensity in QF belly
- Normal Value
- Isointense to skeletal muscle
- Impingement Threshold
- Hyperintense (oedema pattern)
Normal: QF functions as a hip external rotator and adductor, gliding freely in the IFS during movement
Narrowed space: QF compressed between ischium and LT during terminal extension and adduction
Repetitive microtrauma: leads to muscle oedema, inflammation, and eventual fatty atrophy
Sciatic nerve: may be secondarily irritated as it passes just posterior to QF
Wider pelvis: increased interischial distance alters the ischiofemoral angle
Femoral anteversion: greater average anteversion positions the lesser trochanter closer to the ischium in extension
Smaller QF muscle bulk: less soft-tissue cushion in the ischiofemoral interval
Hormonal and gait factors: wider stance and coxalgic gait patterns may exacerbate narrowing
Classification and Types
Classification by Aetiology
- Mechanism
- Developmental bony morphology: prominent LT, narrow IFS
- Clinical Context
- Female patient, insidious onset, no prior surgery
- Treatment Implication
- Conservative first; endoscopic osteoplasty if refractory
- Mechanism
- Medialized cup, increased offset, leg-lengthening
- Clinical Context
- Posterior hip pain after total hip arthroplasty
- Treatment Implication
- Consider component revision vs endoscopic decompression
- Mechanism
- Exostosis, malunion of lesser trochanter or ischial fracture
- Clinical Context
- History of proximal femur or pelvis fracture
- Treatment Implication
- Address bony deformity; osteoplasty or excision of exostosis
- Mechanism
- Valgus intertrochanteric osteotomy repositions LT medially
- Clinical Context
- Prior proximal femoral osteotomy (often paediatric)
- Treatment Implication
- Corrective osteotomy vs endoscopic decompression
- Mechanism
- Coxa valga, DDH, femoral retroversion altering IFS
- Clinical Context
- Young patient with hip dysplasia or abnormal morphology
- Treatment Implication
- Address underlying deformity; consider realignment surgery
Primary IFI is the most common form encountered in the exam setting. Secondary causes, particularly post-THA, are increasingly recognised in clinical practice.
Clinical Assessment
- Pain location: Posterior hip, deep buttock, rarely radiating below the knee
- Aggravating activities: Long-stride walking, running, prolonged sitting, extension with adduction
- Relieving factors: Rest, short strides, hip flexion
- Prior surgery: Specifically ask about prior THA, osteotomy, or fracture fixation
- Female sex: Strong association; ask about insidious onset
- Inspection: Usually normal; assess gait pattern (antalgic or Trendelenburg)
- Palpation: Tenderness deep in the buttock, distal to the gluteal fold, difficult to localise
- Range of motion: Pain at terminal extension with adduction; flexion typically comfortable
- Special tests: Long-stride walking test, IFI test (extension-adduction-external rotation), FAIR test
Technique: With the patient standing, ask them to take a long stride with the affected leg trailing (hip extension with adduction). This narrows the ischiofemoral space.
Positive test: Reproduction of the characteristic deep posterior hip or buttock pain.
Alternative (supine): Passive extension of the hip with adduction and external rotation.
FAIR test (Flexion, Adduction, Internal Rotation) is also often positive due to compression of the QF, but is more classically associated with piriformis syndrome and deep gluteal syndrome.
Key point: No single clinical test is pathognomonic. The diagnosis requires clinical suspicion PLUS MRI confirmation. Always correlate imaging with symptoms.
- Key Discriminating Features
- Pain with extension-adduction, long-stride walking; QF tenderness
- Imaging
- MRI: narrowed IFS, QF oedema
- Critical Test
- Long-stride walking test; measure IFS/QFS on axial MRI
- Key Discriminating Features
- Pain with FAIR manoeuvre; may have sciatic distribution
- Imaging
- MRI: piriformis hypertrophy or anomaly; no QF oedema
- Critical Test
- FAIR test with sciatic nerve latency on EMG
- Key Discriminating Features
- Proximal hamstring pain, worse with sit-to-stand and sprinting
- Imaging
- MRI: hamstring tendon oedema/tear at ischial origin
- Critical Test
- Palpation over ischial tuberosity; resisted knee flexion
- Key Discriminating Features
- Radiculopathic pain below knee, neurological signs
- Imaging
- MRI lumbar spine: disc protrusion, stenosis
- Critical Test
- SLR, neurological exam, EMG/NCS
- Key Discriminating Features
- Groin pain (not buttock), flexion-adduction-internal rotation
- Imaging
- MRI: cam/pincer morphology, labral tear
- Critical Test
- FADIR test positive; FABER may be positive
- Key Discriminating Features
- Sacroiliac region pain, positive FABER and Gaenslen
- Imaging
- MRI/CT SI joints; diagnostic injection
- Critical Test
- SI joint provocation tests; diagnostic block
Post-THA posterior hip pain is a common exam scenario. While the differential includes infection, loosening, and instability, ischiofemoral impingement is increasingly recognised. A medialized acetabular cup, excessive femoral offset, or leg-lengthening can narrow the ischiofemoral space. If plain films and infection workup are negative, consider MRI to measure the IFS. Management may require component revision if implant positioning is the primary driver.
A common exam framing error is to treat ischiofemoral impingement and "deep gluteal syndrome" as separate diagnoses. They are not parallel: deep gluteal syndrome (DGS) is the umbrella term for non-discogenic, extrapelvic entrapment or irritation of the sciatic nerve in the subgluteal (deep gluteal) space, and IFI is one of its recognised causes. Other DGS causes include piriformis syndrome, obturator internus/gemelli pathology, proximal hamstring origin pathology, fibrovascular adhesive bands, and vascular (gluteal vein varicosities) lesions.
- Why it matters: in IFI the sciatic nerve runs immediately posterior to the quadratus femoris, so a narrowed ischiofemoral space can compress not only the QF muscle but also the adjacent nerve - which is why some patients report radiating, sciatica-like leg pain rather than pure mechanical buttock pain.
- Exam point: when asked for the differential of posterior hip/buttock pain, frame it as "DGS causes" and place IFI within that family, then separate them by the discriminating manoeuvre (long-stride/extension-adduction for IFI; FAIR for piriformis) and the MRI finding (QF oedema in a narrowed IFS for IFI). This is also why a structured deep-gluteal-space MRI and, in selected refractory cases, sciatic nerve assessment are part of the workup.
DEEPIschiofemoral Impingement Clinical Features
Hook:DEEP posterior hip pain with QF oedema = think ischiofemoral impingement!
Investigations
Imaging Protocol
Views: AP pelvis, lateral hip (cross-table or frog), and Dunn view
Look for: Prominent lesser trochanter, coxa valga, evidence of prior osteotomy, post-THA component position (medialized cup, leg-lengthening), exostoses
Limitation: Cannot directly measure the IFS (requires cross-sectional imaging); normal radiographs do not exclude IFI
Essential sequences: Axial T1 and T2/FS or STIR through the hip at the level of the quadratus femoris
Measure: IFS (lateral ischial cortex to medial lesser trochanter cortex) and QFS (between converging soft-tissue borders)
Look for: Quadratus femoris muscle oedema (T2/STIR hyperintensity), fatty infiltration, partial tears, hamstring tendon pathology, sciatic nerve signal change
Thresholds: IFS less than 15 mm and QFS less than 10 mm suggest IFI (must be clinically correlated)
Indication: Detailed bony anatomy assessment when planning osteoplasty; 3D reconstruction for surgical planning
Value: Precise measurement of bony IFS, lesser trochanter morphology, and ischial configuration
Pre-operative: Maps the extent of bony resection needed for endoscopic or open decompression
Technique: Ultrasound or CT-guided corticosteroid and local anaesthetic injection into the QF muscle belly or ischiofemoral space
Diagnostic value: Significant pain relief supports the diagnosis of IFI as the pain generator
Therapeutic value: Can provide weeks to months of symptomatic relief to facilitate rehabilitation
The diagnosis of IFI is clinical plus radiological. MRI findings of QF oedema and narrowed IFS must correlate with characteristic symptoms (posterior hip pain reproduced by extension-adduction). Up to 10 to 15 percent of asymptomatic individuals have narrowing of the IFS on MRI. The ischiofemoral space also varies dynamically with hip position (narrows in extension and adduction), so static measurements are a snapshot. Always treat the patient, not the MRI.
Management Algorithm
Conservative Management (First Line for All Patients)
Goal: Reduce QF compression and inflammation, restore normal gait mechanics, and avoid surgical intervention
Conservative Protocol
Activity modification: Avoid long-stride walking, running, and prolonged hip extension; use shorter strides
NSAIDs: Oral anti-inflammatory medication for symptomatic relief
Physiotherapy: Pelvic tilt correction, gait retraining (shorter stride length), hip abductor and core strengthening
Education: Explain mechanism of impingement and activity modification rationale
Image-guided injection: Corticosteroid plus local anaesthetic into the QF muscle belly or ischiofemoral space under ultrasound or CT guidance
Diagnostic value: Greater than 50 percent pain relief supports IFI diagnosis
Therapeutic benefit: Reduces inflammation, facilitates engagement with physiotherapy
Continue physiotherapy: Progress strengthening and gait retraining
Assess progress: Pain scores, functional improvement, walking distance
Repeat injection: May consider a second injection at 3 months if partial response
Advanced physiotherapy: Lumbopelvic stability, eccentric loading, dynamic movement control
If still refractory at 6 months: Consider surgical referral for endoscopic decompression
Approximately 80 percent of patients with primary IFI improve with conservative management. The keys are gait modification (shorter strides reduce hip extension and therefore narrow the IFS less), hip abductor strengthening to improve pelvic stability, and targeted injection to break the inflammatory cycle. Do not rush to surgery in primary IFI.
A non-operative option distinct from corticosteroid that the standard injection discussion above omits is image-guided botulinum toxin (BoNT-A) injection into the quadratus femoris. Rather than suppressing inflammation, it works by chemically relaxing (partially denervating) the QF, which reduces the muscle's bulk and resting tone in the ischiofemoral interval and so decreases the dynamic compression that drives symptoms.
- Diagnostic value: like a local-anaesthetic block, meaningful relief after QF botulinum toxin supports the QF/IFI as the true pain generator.
- Therapeutic value: effect lasts several months and can be used as a bridge while gait-retraining and abductor strengthening take effect, or as a temporising measure in patients who are poor surgical candidates or wish to avoid bony decompression.
- Caveats: the effect is temporary and may need repeating; transient QF/external-rotator weakness can occur; accurate ultrasound or CT guidance is essential given the sciatic nerve's immediate posterior relationship to the QF.
Exam point: in a refractory primary-IFI patient who responded to a diagnostic injection but wants to avoid (or delay) osteoplasty, botulinum toxin to the QF is a legitimate intermediate step between corticosteroid injection and endoscopic decompression.
RESTIschiofemoral Impingement Treatment Ladder
Hook:REST the patient first before considering surgical decompression for IFI!
Complications
- Incidence
- Reported in case series, rare overall
- Risk Factors
- Endoscopic surgery, proximity of nerve to QF
- Management
- Intra-operative nerve monitoring; identify and protect nerve throughout
- Incidence
- 5 to 10 percent post-operatively
- Risk Factors
- Bony resection, inadequate haemostasis
- Management
- Prophylactic NSAIDs; excision if symptomatic and mature
- Incidence
- Not well quantified; under-recognised
- Risk Factors
- Limited endoscopic visualisation, inadequate resection
- Management
- Intra-operative assessment of IFS widening; post-operative CT if symptoms persist
- Incidence
- Variable; reported in small series
- Risk Factors
- Incomplete resection, ongoing impingement from ischial side
- Management
- Repeat MRI, consider revision surgery or ischioplasty
- Incidence
- If chronic fatty atrophy present pre-operatively
- Risk Factors
- Long duration of symptoms prior to surgery
- Management
- Rehabilitation may be prolonged; muscle may not fully recover
The sciatic nerve courses directly posterior to the quadratus femoris muscle and is therefore immediately adjacent to the surgical field during endoscopic decompression. Nerve identification and protection is the single most important surgical consideration. Neurological examination (dorsiflexion, plantarflexion, sensation in the foot) must be documented pre-operatively and monitored post-operatively. Any new neurological deficit requires urgent evaluation.
Outcomes and Prognosis
- Expected Outcome
- Approximately 80 percent significant improvement
- Time to Improvement
- 6 to 12 weeks with physiotherapy and injection
- Long-term Prognosis
- Good if activity modification maintained; recurrence possible
- Expected Outcome
- Good to excellent outcomes in case series
- Time to Improvement
- 3 to 4 months for full recovery
- Long-term Prognosis
- Favourable when decompression adequate and nerve uninjured
- Expected Outcome
- Variable; depends on revision complexity
- Time to Improvement
- 3 to 6 months for full recovery
- Long-term Prognosis
- Good if implant position corrected; risk of recurrent instability
- Expected Outcome
- Functional improvement likely; full muscle recovery uncertain
- Time to Improvement
- 6 months or more for rehabilitation
- Long-term Prognosis
- Residual weakness possible; pain relief generally achievable
Best prognosis: Short duration of symptoms, primary IFI, preserved QF muscle on MRI (no fatty atrophy), good response to injection, compliant with rehabilitation
Poor prognosis: Long-standing symptoms with QF fatty atrophy, post-THA IFI with severe component malposition, failed prior surgery, coexisting lumbar or intra-articular pathology
Key message: Treat early and conservatively. Surgery is reserved for the minority who fail non-operative management.
Guidelines, Registries & Global Practice
- IFI is reported worldwide with female predominance across all ethnicities
- Post-THA IFI is increasingly recognised as implant design and positioning evolve
- Underdiagnosis is global: many patients are labelled with piriformis syndrome or non-specific buttock pain before the correct diagnosis
- No registry data specifically for IFI; most evidence comes from case series and institutional reviews
- High-resource: MRI-first approach with axial IFS/QFS measurement; image-guided injection widely available; endoscopic surgery in specialist centres
- Limited-resource: Diagnosis based on clinical pattern and response to injection; CT may substitute for MRI if unavailable; open decompression more common
- Universal principle: Diagnosis requires clinical suspicion PLUS imaging correlation; conservative management is first-line regardless of setting
- Surgery: Concentrated in tertiary hip arthroscopy centres; outcomes vary with surgeon experience
- Diagnosis Emphasis
- Clinical suspicion + MRI IFS/QFS measurement + QF oedema; injection for diagnostic confirmation
- Acute Treatment
- Activity modification, gait retraining, hip abductor strengthening, image-guided injection
- Surgery / Decompression
- Endoscopic lesser trochanter osteoplasty for refractory cases; nerve protection mandatory
- Diagnosis Emphasis
- MRI with axial sequences; rule out lumbar spine, intra-articular, and piriformis pathology first
- Acute Treatment
- Conservative care for minimum 3 to 6 months before considering surgery
- Surgery / Decompression
- Endoscopic preferred over open; component revision for post-THA IFI if implant malpositioned
- Diagnosis Emphasis
- Posterior hip pain algorithm; IFI considered after lumbar and SIJ excluded
- Acute Treatment
- Physiotherapy-led rehabilitation; image-guided injection for diagnostic and therapeutic purposes
- Surgery / Decompression
- Specialist hip arthroscopy centres; MDT discussion for post-THA cases
- Diagnosis Emphasis
- Cross-sectional imaging (MRI/CT) to define bony anatomy and soft-tissue involvement
- Acute Treatment
- Standard non-operative protocol; injection under imaging guidance
- Surgery / Decompression
- Endoscopic or open osteoplasty with attention to sciatic nerve anatomy
There is no dedicated joint registry or outcome database for ischiofemoral impingement. The evidence base consists entirely of retrospective case series (level 4 evidence) and expert opinion. No randomised controlled trials have been published comparing surgical to non-surgical management or endoscopic to open decompression. Treatment recommendations are therefore principle-based: diagnose with clinical plus MRI correlation, treat conservatively first, and reserve surgery for refractory cases with careful sciatic nerve protection.
Record in every suspected IFI presentation:
- Clinical examination findings including long-stride walking test result
- MRI measurements: IFS and QFS values in millimetres on axial sequences
- Presence or absence of QF muscle oedema on T2/STIR
- Response (or lack thereof) to image-guided injection
- Duration of conservative management before considering surgical referral
IFI is an evolving diagnosis. Documenting objective MRI measurements and clinical response to injection strengthens the diagnostic pathway and protects against missed or delayed diagnosis.
Controversies & Areas of Uncertainty
The IFS less than 15 mm and QFS less than 10 mm cut-offs are derived from case-control studies, not population-based normative data. Dynamic narrowing occurs with hip extension, meaning static MRI may underestimate or overestimate the clinical significance of measured narrowing. Some authors argue for a spectrum rather than binary thresholds.
Up to 10 to 15 percent of asymptomatic individuals have IFS measurements below the diagnostic threshold on MRI. This raises the question of whether narrowing alone is sufficient for diagnosis or whether QF oedema and clinical correlation should be mandatory requirements. Most authorities now require all three: clinical symptoms, MRI narrowing, and QF signal change.
Lesser trochanter osteoplasty is the most commonly described surgical approach, but some authors advocate ischial-sided decompression (ischioplasty) or combined procedures. There are no comparative studies. The choice is currently based on which side contributes more to the narrowing and surgeon preference.
Post-THA IFI is recognised but its true incidence is unknown. Some argue it is under-diagnosed as a cause of unexplained post-arthroplasty buttock pain, while others caution against over-attributing pain to IFI when component issues (loosening, infection, instability) have not been fully excluded. A systematic approach to post-THA pain evaluation should include IFI in the differential.
MCQ Practice Points
Q: What muscle is primarily compressed in ischiofemoral impingement? A: The quadratus femoris muscle, which runs from the lateral border of the ischial tuberosity to the quadrate tubercle of the proximal femur. It is trapped in the narrowed space between the ischium and the lesser trochanter, producing its characteristic oedema pattern on MRI.
Q: What are the MRI diagnostic criteria for ischiofemoral impingement? A: Ischiofemoral space (IFS) less than 15 mm measured on axial MRI between the lateral ischial cortex and the medial lesser trochanter cortex, quadratus femoris space (QFS) less than 10 mm, and quadratus femoris muscle oedema on T2/STIR sequences. Clinical correlation is essential as asymptomatic narrowing exists.
Q: How do you distinguish ischiofemoral impingement from piriformis syndrome clinically? A: Both cause deep buttock pain. IFI is worsened by extension-adduction (long-stride walking) and shows QF oedema on MRI. Piriformis syndrome is worsened by flexion-adduction-internal rotation (FAIR test), may have sciatic nerve symptoms, and shows piriformis hypertrophy or anomaly on MRI. The key discriminator is the MRI finding: QF oedema points to IFI, piriformis abnormality points to piriformis syndrome.
Q: What is the management algorithm for primary ischiofemoral impingement? A: Step 1: Activity modification (shorter strides) + NSAIDs + physiotherapy (gait retraining, hip abductor strengthening). Step 2 (if no improvement at 4 to 6 weeks): Image-guided corticosteroid injection into the QF. Step 3 (if refractory at 3 to 6 months): Endoscopic lesser trochanter osteoplasty. Approximately 80 percent of patients improve with conservative management alone.
Q: What is the most important structure at risk during endoscopic decompression for IFI? A: The sciatic nerve, which courses immediately posterior to the quadratus femoris muscle. It must be identified and protected throughout the procedure. Pre-operative neurological examination should be documented, and any new post-operative deficit (particularly foot drop from common peroneal nerve involvement) requires urgent evaluation.
Q: What surgical factors predispose to post-THA ischiofemoral impingement? A: Acetabular cup medialisation (narrows the IFS by moving the centre of rotation medially), excessive femoral offset (positions the lesser trochanter closer to the ischium), and leg-lengthening (alters the ischiofemoral relationship). Component revision should be considered if malposition is the primary driver rather than osteoplasty alone.
Clinical Imaging
Ischiofemoral Impingement Imaging Findings
The key imaging modality is MRI, which demonstrates both the bony anatomy (ischiofemoral and quadratus femoris space measurements) and soft-tissue pathology (quadratus femoris muscle oedema). Axial sequences at the level of the quadratus femoris are essential for measurement. Correlation with clinical examination findings is critical, as asymptomatic narrowing of the ischiofemoral space has been reported in up to 10-15 percent of routine hip MRI studies.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old woman presents with a 6-month history of deep left buttock pain, worse with long-stride walking and relieved by rest and shorter strides. She has no prior hip surgery. Examination reveals tenderness in the deep buttock, pain reproduced by passive extension-adduction of the hip, and no neurological deficit. Lumbar spine examination is unremarkable. Her GP has ordered a lumbar MRI which was normal. What is your diagnosis and how would you investigate?”
“A 68-year-old woman presents with deep right buttock pain 14 months after an uncomplicated right total hip arthroplasty. The hip is stable, wound healed, and infection markers are normal. Radiographs show a well-fixed cementless prosthesis with the acetabular cup appearing slightly medialized compared to the contralateral native hip. She describes pain with walking that is relieved by shorter strides. Examination shows a positive long-stride walking test reproducing her buttock pain and no neurological deficit. How would you manage this?”
Key Anatomy
- IFS = narrowest distance between lateral ischial cortex and medial lesser trochanter cortex
- QFS = narrowest distance between hamstring tendons and iliopsoas/LT soft-tissue borders
- Quadratus femoris occupies the ischiofemoral interval; compressed when space narrows
- Sciatic nerve lies immediately posterior to QF (key surgical landmark)
Diagnosis
- Clinical: posterior hip or deep buttock pain worsened by long-stride walking and extension-adduction
- MRI: IFS less than 15 mm, QFS less than 10 mm on axial sequences at QF level
- MRI hallmark: QF muscle oedema (T2/STIR hyperintensity); may see fatty infiltration in chronic cases
- Image-guided injection into QF is both diagnostic (pain relief confirms source) and therapeutic
Differential Diagnosis
- Piriformis syndrome: FAIR test positive, piriformis anomaly on MRI, no QF oedema
- Hamstring origin tendinopathy: ischial tuberosity tenderness, tendon tear on MRI
- Lumbar radiculopathy: radicular pain below knee, neurological signs, abnormal lumbar MRI
- Post-THA IFI: consider component medialisation, increased offset, leg-lengthening
Treatment Algorithm
- Conservative first: activity modification (shorter strides), NSAIDs, physiotherapy (gait retraining)
- Injection (4 to 6 weeks): image-guided corticosteroid into QF for diagnostic and therapeutic value
- Endoscopic osteoplasty (3 to 6 months refractory): lesser trochanter resection with nerve protection
- Post-THA: consider component revision if implant malposition is the primary driver
Surgical Pearls
- Endoscopic lesser trochanter osteoplasty is the preferred approach for primary IFI
- Sciatic nerve identification and protection is mandatory (runs directly posterior to QF)
- Preserve iliopsoas tendon attachment during osteoplasty to maintain hip flexion power
- Heterotopic ossification prophylaxis should be considered post-operatively
Exam Traps
- Do NOT diagnose IFI on MRI alone (asymptomatic narrowing exists in 10 to 15 percent)
- Do NOT confuse with piriformis syndrome (different anatomy, different MRI findings)
- Do NOT rush to surgery without 3 to 6 months of conservative management (80 percent respond)
- Do NOT forget to check sciatic nerve function pre- and post-operatively
Evidence Base and Key Trials
Ischiofemoral impingement: evaluation with new MRI parameters and assessment of their reliability
- Proposed standardised MRI measurement of the ischiofemoral space (IFS) and quadratus femoris space (QFS) on axial sequences
- Demonstrated excellent inter- and intra-observer reliability for IFS and QFS measurements
- Patients with IFI had significantly narrowed IFS (mean approximately 13 mm) compared to controls (mean approximately 26 mm)
- QF muscle oedema on T2/STIR sequences was the most consistent soft-tissue finding
Diagnosis and 2-year outcomes of endoscopic treatment for ischiofemoral impingement
- Endoscopic lesser trochanter osteoplasty performed safely with good clinical outcomes at 2-year follow-up
- Surgical technique described in detail including patient positioning, portal placement, and nerve protection
- Outcome measures (modified Harris Hip Score, pain scores) showed significant improvement post-operatively
- No sciatic nerve injuries reported in the series with meticulous nerve identification technique
Ischiofemoral impingement syndrome: a meta-analysis
- Meta-analysis confirming female predominance (approximately 3:1) and the spectrum from primary to secondary IFI
- Conservative treatment (physiotherapy, injections) is first-line with approximately 80 percent success rate
- Endoscopic lesser trochanter osteoplasty is the preferred surgical approach for refractory cases
- IFS less than 15 mm and QFS less than 10 mm are the most commonly used diagnostic thresholds
Treatment strategies for ischiofemoral impingement: a systematic review
- Systematic review of all published IFI treatment studies confirming conservative management as first-line therapy
- Endoscopic lesser trochanter osteoplasty demonstrates favourable outcomes in refractory cases
- Sciatic nerve proximity remains the primary surgical risk; nerve identification and protection is mandatory
- Highlights the need for standardised outcome measures and higher-quality prospective studies
Extra-articular hip impingement: a systematic review examining operative treatment of psoas, subspine, ischiofemoral, and greater trochanteric/pelvic impingement
- Systematic review covering all extra-articular hip impingement including IFI, confirming the increasing recognition of these conditions
- Endoscopic decompression for IFI shows promising short-term outcomes with low complication rates
- Post-THA IFI is an important iatrogenic subset requiring component position assessment
- Emphasised that accurate diagnosis requires clinical suspicion plus MRI correlation, not imaging alone