Latarjet Procedure
Confirm the instability is anterior and structural before offering a Latarjet. Voluntary / habitual (psychogenic) instability and posterior or multidirectional instability are not corrected by an anterior bone block, and operating on them tends to fail. Also exclude an uncontrolled seizure disorder, which drives recurrent dislocation regardless of the repair.
- Best option
- Arthroscopic Bankart repair
- Reasoning
- Restores labrum/capsule; low morbidity when there is bone to work with
- Best option
- Latarjet (coracoid transfer)
- Reasoning
- Triple effect addresses bone loss and adds a dynamic sling
- Best option
- Free bone block (Eden-Hybinette iliac crest / distal tibial allograft)
- Reasoning
- Restores a large arc when the coracoid is unavailable or insufficient
- Best option
- Treat the underlying driver first
- Reasoning
- A bone block does not fix a behavioural or seizure cause
Overview and Indications

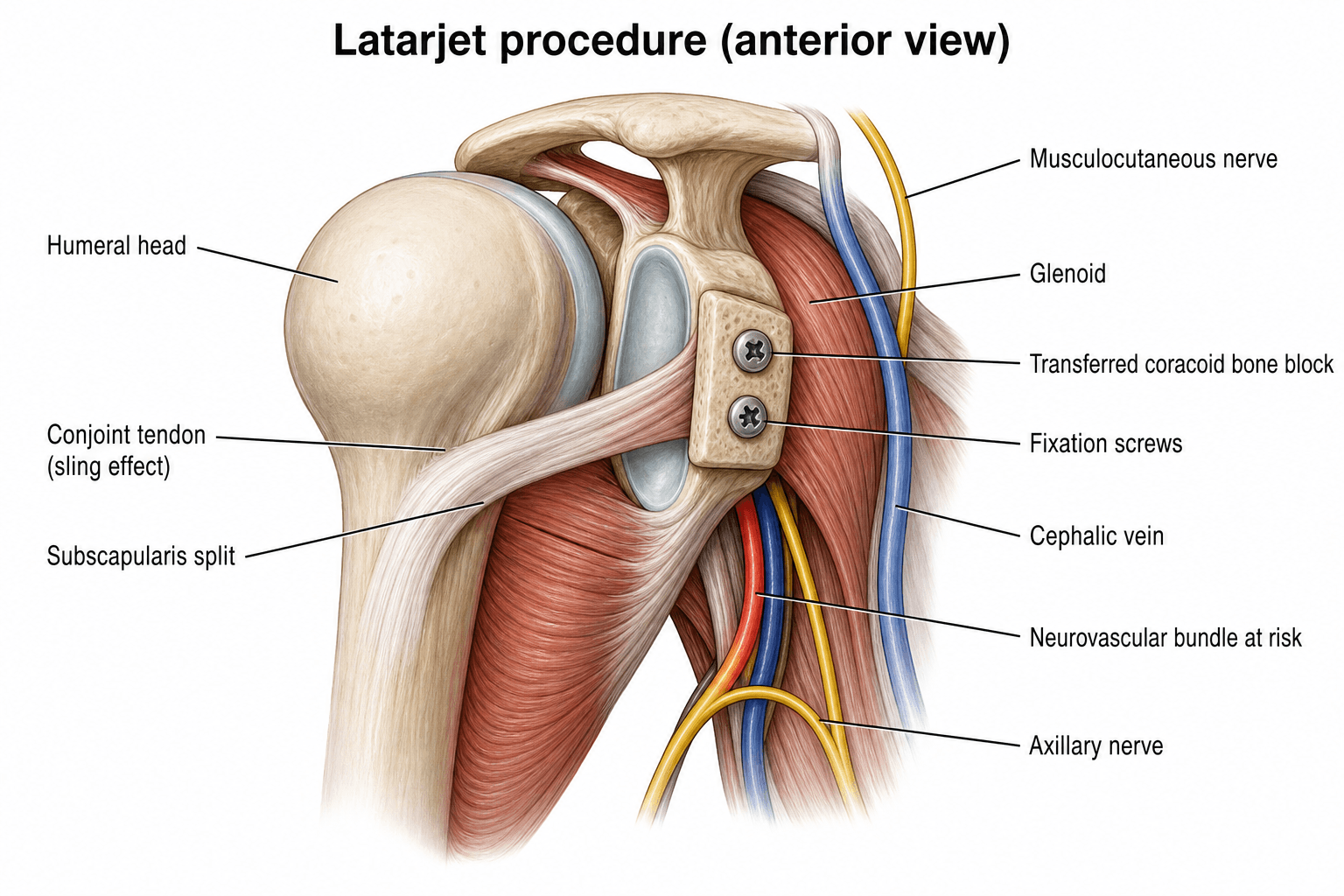
The Latarjet procedure is a coracoid-transfer operation for recurrent anterior glenohumeral instability, particularly when there is glenoid bone loss or an engaging Hill-Sachs lesion. The tip of the coracoid process (with the attached conjoint tendon) is osteotomised and transferred to the deficient anteroinferior glenoid, where it is fixed with screws. It was described by Michel Latarjet of Lyon in 1954. The related Bristow procedure transfers a smaller coracoid tip; the family is often called Bristow-Latarjet.
Indications - choosing Latarjet over arthroscopic Bankart. The central decision in anterior instability is soft-tissue (Bankart) repair versus a bony (Latarjet) procedure; bone loss, high demand and a high recurrence-risk profile push toward Latarjet:
- Glenoid bone loss. Historically a "critical" threshold of about 20-25% (the inverted-pear glenoid) defined when arthroscopic Bankart fails; more recent work lowers this to a "subcritical" ~13-15%.
- Glenoid track / engaging Hill-Sachs. A Hill-Sachs lesion whose medial margin lies outside the glenoid track is off-track and will engage the rim. An off-track or bipolar lesion is a strong indication.
- ISIS greater than 6. The Instability Severity Index Score predicts recurrence after arthroscopic repair; a score over 6 favours a bony procedure.
- Other factors: collision/contact athletes, failed prior soft-tissue stabilisation, a fragmented bony Bankart, and hyperlaxity.
Always begin by justifying why a soft-tissue repair would fail here - bone loss, an off-track Hill-Sachs, or a high ISIS. That framing earns more marks than jumping straight to the steps of the operation.
The thresholds above are only useful if you can measure them — a frequent viva follow-up:
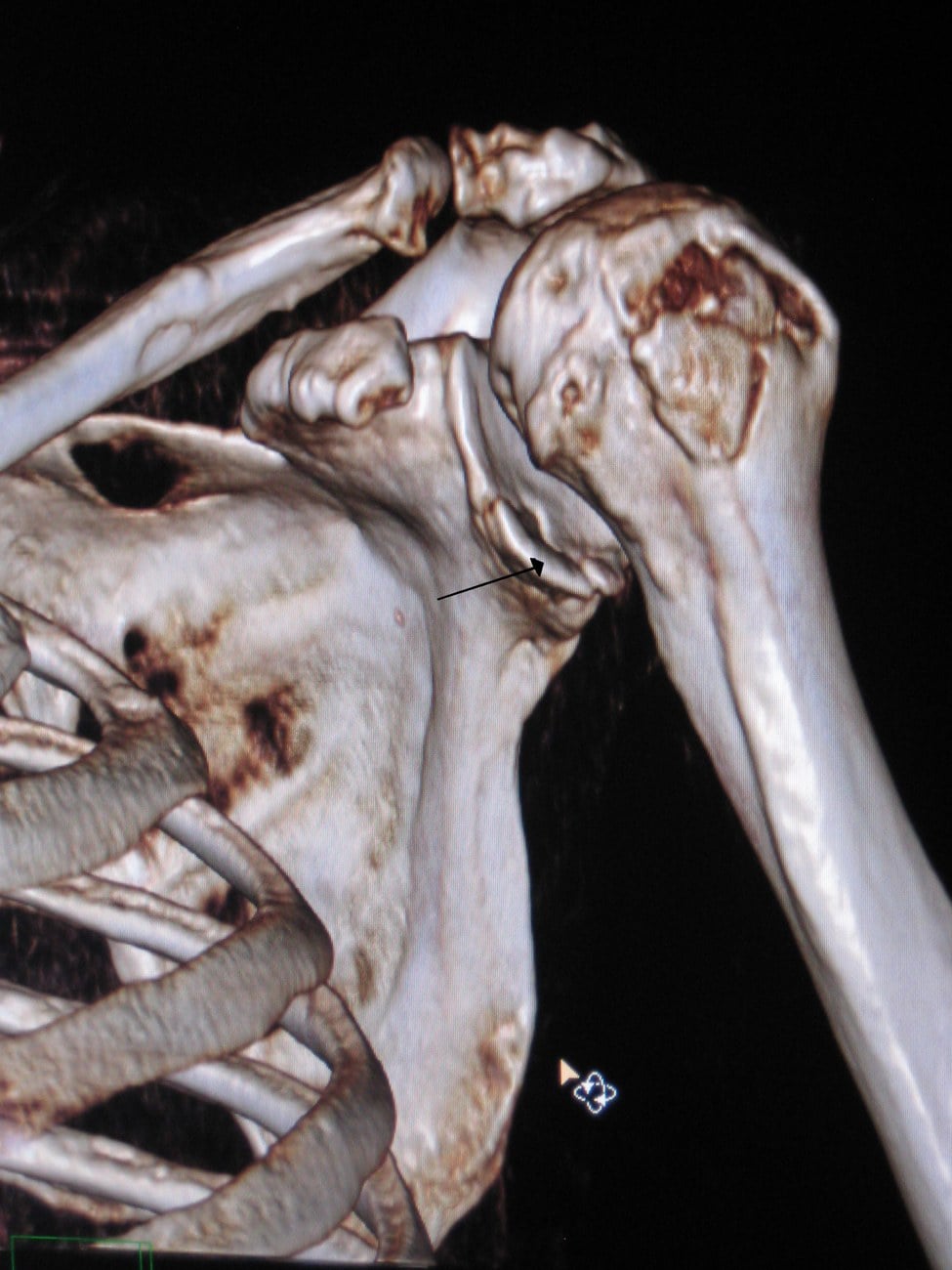
- Glenoid bone loss is best measured on a 3-D CT with the humeral head digitally subtracted, viewing the glenoid en face (sagittal-oblique). Fit a best-fit circle to the lower glenoid (which is normally circular): the surface-area (Pico) method expresses the defect area as a percentage of the circle, while the simpler linear/diameter method compares the lost width to the circle's diameter. MRI can substitute where CT is unavailable.
- The glenoid track converts this into an on-track/off-track decision. The track width is about 83% of the glenoid diameter (Di Giacomo: 0.83 × D, then subtract any anterior bone-loss width). The Hill-Sachs interval — the width of the Hill-Sachs lesion plus the intact bone bridge between it and the rotator-cuff footprint — is then compared with the track: if the Hill-Sachs interval is greater than the glenoid track the lesion is off-track (engaging); if it is smaller, the lesion is on-track.
Relevant Anatomy and the Mechanism of Stability
The coracoid and conjoint tendon:
- The coracoid process projects from the anterior scapular neck. Its tip gives origin to the conjoint tendon (short head of biceps and coracobrachialis), with pectoralis minor attaching medially and the coraco-acromial (CA) ligament laterally.
- Its undersurface provides a curved bony surface that can be apposed to the decorticated glenoid neck (the basis of the congruent-arc modification).
The transferred coracoid restores the deficient anteroinferior glenoid arc, increasing the effective glenoid surface area and concavity-compression that resist anterior translation. This directly addresses glenoid bone loss, where a pure soft-tissue repair fails.
If asked "why does the Latarjet work?", lead with the triple effect of Patte: (1) bony block, (2) dynamic conjoint-tendon sling, (3) capsular / CA-ligament repair. Emphasise that the sling effect is the key dynamic restraint in abduction-external rotation.
Internervous Plane and Surgical Interval
The Latarjet is performed through the deltopectoral approach:
- Interval: between deltoid (axillary nerve) laterally and pectoralis major (medial and lateral pectoral nerves) medially. The cephalic vein marks the interval and is usually retracted laterally with the deltoid.
- Internervous plane: the approach exploits the plane between the axillary nerve (deltoid) and the pectoral nerves (pectoralis major), so no single nerve supplies muscles on both sides of the interval.
- Deeper: the conjoint tendon is retracted medially to expose subscapularis, behind which lies the capsule and glenoid. The musculocutaneous nerve (entering the conjoint muscles a few centimetres distal to the coracoid) and the axillary nerve (along the inferior subscapularis and through the quadrilateral space) are the structures most at risk; the brachial plexus and axillary vessels lie medial to the conjoint tendon and are protected by retracting it laterally rather than medially.
Patient Positioning and Setup
- Position: beach-chair (semi-sitting) with the head secured and the arm free-draped to allow rotation; some surgeons use a lateral arm holder.
- Anaesthesia: general anaesthesia, frequently combined with an interscalene block for analgesia (counsel the patient about transient nerve effects of the block).
- Setup: the operated shoulder is positioned off the edge of the table to allow extension; image intensifier available if screw position confirmation is desired. Antibiotic prophylaxis is given, recognising that Cutibacterium acnes is the classic indolent shoulder organism.
Surgical Technique
Deltopectoral approach (cephalic vein taken laterally). Identify the coracoid and conjoint tendon. Release pectoralis minor medially and the CA ligament laterally (leaving a stump on the graft). Perform the coracoid osteotomy at the "knee" of the coracoid, harvesting roughly 2-3 cm with the conjoint tendon attached. Decorticate the undersurface and pre-drill two holes.
A graft placed too lateral / proud leaves a step that grinds the humeral head and causes glenohumeral arthritis. A graft placed too medial fails to restore the arc and leads to recurrent instability. Aim for flush placement and confirm it intra-operatively.
Structures at Risk and Complications
According to PubMed, a systematic review of Bristow-Latarjet procedures reported an overall complication rate of about 30%, although recurrent dislocation (about 3%) and unplanned reoperation (about 7%) were low [Griesser 2013].
- Neurological injury - the musculocutaneous and axillary nerves are most at risk; most deficits are transient but they are the headline complication.
- Graft problems - malposition (lateral causes arthritis, medial causes recurrence), nonunion / fibrous union, resorption / osteolysis, graft fracture.
- Hardware problems - screw breakage, prominence or irritation, sometimes requiring removal.
- Recurrent instability - uncommon, usually graft malposition or a missed humeral lesion.
- Glenohumeral arthropathy - dislocation arthropathy develops over time even in successful repairs.
- Loss of external rotation - partly intended (the sling) but excessive loss is a problem.
- Infection (consider indolent Cutibacterium acnes) and stiffness.
Tie most graft-related complications back to position: a proud (lateral) graft drives arthritis; a medial / recessed graft drives recurrence. This framing answers most "why did this Latarjet fail?" viva questions.
Guidelines, Registries and Global Practice
No single guideline dictates Bankart versus Latarjet - selection follows the bone-loss and recurrence-risk principles above (glenoid bone loss, the glenoid track, and the ISIS). International consensus statements (for example from ISAKOS and shoulder-society instability working groups) have moved toward earlier use of a bony procedure when there is subcritical glenoid bone loss or an off-track Hill-Sachs, rather than waiting for the historical 20-25% threshold.
- National shoulder-instability registries and large comparative series consistently report a lower rate of recurrent instability and revision-for-instability after Latarjet than after isolated arthroscopic Bankart repair, particularly in young contact athletes and with bone loss.
- This is balanced against a higher overall complication burden (the ~30% figure from systematic review) - so the trade-off, not a blanket preference, should be discussed with each patient.
- The Latarjet originated in France (Lyon) and has long been favoured in much of Europe; North American practice was historically weighted toward arthroscopic soft-tissue repair. Practice has converged with the bone-loss and glenoid-track paradigm.
- For very large defects or a failed Latarjet, free bone-block reconstruction (iliac-crest Eden-Hybinette or distal tibial allograft) is used where available; graft availability influences the choice between these in different settings.
The Latarjet treats the glenoid (and adds a sling), but the humeral Hill-Sachs lesion can be addressed directly by remplissage (French, "to fill"). This is an arthroscopic infraspinatus tenodesis with posterior capsulodesis that fills the Hill-Sachs defect, converting an engaging/off-track lesion into an extra-articular, non-engaging one. It is typically combined with an arthroscopic Bankart repair and is an attractive alternative to the Latarjet when the glenoid bone loss is subcritical but the Hill-Sachs is off-track — that is, when the humeral side is the dominant problem. Comparative studies and randomised trials report recurrence rates approaching those of the Latarjet in appropriately selected patients, with a lower complication profile, at the cost of some loss of external rotation. For bipolar loss with a critical glenoid deficiency, however, a bony procedure (Latarjet or free bone block) is still required.
Memory Aids
BSSTriple Effect - Bone, Sling, Strap (B-S-S)
Hook:Bone, Sling, Strap - the three ways a Latarjet holds the shoulder in
NGNNNComplications - The N's and a G
Hook:Most Latarjet failures are about a NERVE or the bone GRAFT - check both in any failed case
ISISISIS - Who Will Re-dislocate After Arthroscopic Bankart (out of 10)
Hook:Add the points to 10; a score GREATER THAN 6 means arthroscopic Bankart will likely fail - choose a Latarjet
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old rugby player has had four anterior dislocations of his dominant shoulder over two seasons. CT shows about 20% anteroinferior glenoid bone loss with an inverted-pear appearance and an engaging Hill-Sachs lesion. How would you manage him?”
“A patient returns 18 months after a Latarjet with anterior shoulder pain, crepitus, and loss of external rotation, but no further dislocations. What are the likely problems and how do you investigate?”
One-liner
- Coracoid transfer to the anteroinferior glenoid for recurrent anterior instability with bone loss
- Works via the triple effect of Patte; described by Michel Latarjet (Lyon) in 1954
Triple effect (Patte)
- Bone block (restores glenoid arc)
- Dynamic conjoint sling (ABER) - the key effect
- Capsular / CA-ligament repair (graft kept extra-articular)
Indications
- Glenoid bone loss subcritical ~13-15% / critical ~20-25%
- Engaging or off-track Hill-Sachs / bipolar loss
- ISIS greater than 6
- Contact athlete / failed prior Bankart
Technique keys
- Deltopectoral approach, subscapularis split
- Graft FLUSH at 3-5 o'clock, two screws
- Capsule to CA-ligament stump (extra-articular graft)
Complications (~30%)
- Musculocutaneous / axillary nerve injury
- Graft malposition: lateral=arthritis, medial=recurrence
- Nonunion / resorption / hardware
- Recurrence ~3%; arthropathy long-term
Alternatives
- Arthroscopic Bankart (no bone loss)
- Free bone block / Eden-Hybinette (failed Latarjet, large defect)
Evidence Base
Every citation below has been checked against its source record in PubMed. The chain of reasoning runs: bone loss drives failure of soft-tissue repair (Burkhart & De Beer) → the glenoid track refines the bony/off-track assessment (Yamamoto/Itoi) → the ISIS gives a preoperative selection score (Balg & Boileau) → coracoid transfer is durable at 15 years (Hovelius) but carries a ~30% overall complication burden (Griesser).
Burkhart and De Beer - Traumatic Glenohumeral Bone Defects and Their Relationship to Failure of Arthroscopic Bankart Repairs
- Across 194 arthroscopic Bankart repairs, patients with significant bone defects (an inverted-pear glenoid or an engaging Hill-Sachs lesion) had a 67% recurrence rate versus 4% in those without; in contact athletes the recurrence with bone defects was 89%. The authors concluded that patients with significant glenoid bone loss are not candidates for isolated arthroscopic Bankart repair and recommended reconstruction with a Latarjet coracoid graft.
Yamamoto, Itoi et al - Contact Between the Glenoid and the Humeral Head: a New Concept of the Glenoid Track
- In nine cadaveric shoulders, as the arm elevated the glenoid contact swept across the posterior humeral head as a reproducible zone - the glenoid track - whose medial margin lay about 18.4 mm (around 84% of the glenoid width) medial to the rotator-cuff footprint. A Hill-Sachs lesion extending medial to this margin (off-track) is at risk of engaging the glenoid and causing dislocation.
Balg and Boileau - The Instability Severity Index Score (ISIS): a Simple Pre-operative Score to Select Patients for Arthroscopic or Open Shoulder Stabilisation
- A 10-point preoperative score (younger age, competitive and contact/overhead sport, shoulder hyperlaxity, a Hill-Sachs lesion visible on AP radiograph, and loss of the normal glenoid contour on AP radiograph) predicted recurrence after arthroscopic Bankart repair. A score greater than 6 was associated with a 70% recurrence rate, identifying patients better served by an open bony procedure such as the Latarjet.
Hovelius et al - One Hundred Eighteen Bristow-Latarjet Repairs Prospectively Followed for Fifteen Years (Study I: Clinical Results)
- In 118 shoulders followed for a mean of about 15 years after Bristow-Latarjet repair, 98% of patients were satisfied and recurrent dislocation was rare (a single early redislocation and very few late recurrences). The clinical durability matched or exceeded other operative methods for recurrent anterior dislocation.
Griesser et al - Complications and Re-operations After Bristow-Latarjet Shoulder Stabilization: a Systematic Review
- Across 45 studies and 1,904 shoulders, the total complication rate was 30%, with recurrent dislocation in 2.9%, recurrent subluxation in 5.8%, and unplanned reoperation in about 7%. Mild loss of external rotation was common. Reoperation rates were lower with all-arthroscopic techniques, which conversely showed greater loss of external rotation.