Inflammation | Proliferation | Remodeling
- Similar to tendon healing - three overlapping phases
- Type III collagen first, gradually replaced by Type I
- Never achieves normal properties - healed ligament weaker than original
- Intra-articular ligaments heal poorly (ACL) vs extra-articular (MCL) heal well
- Controlled motion beneficial for ligament healing
- “MCL heals well (extra-articular), ACL does not (intra-articular)
- “ACL fails to heal due to synovial fluid, lack of blood supply, gap
- “Healed MCL 50-70% of normal tensile strength
- “Similar phases to tendon: inflammation, proliferation, remodeling
Inflammatory (0-1 week): Hematoma, inflammatory cells, growth factors. Proliferative (1-6 weeks): Fibroblasts, Type III collagen. Remodeling (6 weeks+): Type I collagen, cross-linking.
MCL heals well - extra-articular, blood supply, contained hematoma. ACL heals poorly - intra-articular, synovial fluid washes away clot, poor blood supply, retraction.
Type III collagen produced initially (thin, disorganized). Replaced by Type I during remodeling (thick, organized). Cross-links form. Never achieves normal properties.
Healed ligament achieves 50-70% of normal tensile strength at best. Increased cross-sectional area compensates. Stiffness also reduced. Functional recovery possible.


SGRBACL Healing Failure
Hook:SGRB = Synovial fluid, Gap, Reduced blood, Biology explain ACL healing failure!
CHEBMCL Healing Success
Hook:CHEB = Contained Hematoma, Extra-articular, Blood supply explain MCL healing!
Overview
Ligament healing follows similar principles to tendon healing but with important differences based on anatomical location. Extra-articular ligaments like the MCL heal reliably, while intra-articular ligaments like the ACL do not heal and require surgical reconstruction if normal function is to be restored.
Clinical Relevance
Understanding why some ligaments heal and others do not guides treatment decisions. MCL injuries are typically managed non-operatively. ACL injuries require reconstruction in active patients. Healing biology informs rehabilitation protocols.
Mechanisms - Healing Phases
Inflammatory Phase (Days 0-7)
Ligament injury triggers an inflammatory response. Hematoma forms and serves as scaffold for healing. Inflammatory cells arrive and release cytokines and growth factors. This phase is essential for initiating repair.
For extra-articular ligaments like the MCL, the hematoma is contained and provides a stable scaffold. For intra-articular ligaments like the ACL, synovial fluid disperses the hematoma and growth factors, disrupting this critical first step.
Proliferative Phase (Weeks 1-6)
Fibroblasts migrate into the healing zone and proliferate. Type III collagen synthesis begins. Granulation tissue forms. The healing tissue is highly cellular and disorganized. Mechanical strength is minimal during this phase.
Remodeling Phase (Weeks 6 to Years)
Type III collagen is gradually replaced by Type I collagen. Collagen fibers align along stress lines. Cross-links form between collagen molecules. Cellularity decreases. Mechanical properties improve but never return to normal.
The ACL fails to heal because: (1) Synovial fluid prevents clot formation and washes away growth factors, (2) The torn ends retract creating a gap with no scaffold, (3) Intra-articular blood supply is limited, (4) The ACL lacks the capacity for intrinsic repair seen in extra-articular ligaments.
Mechanobiology: Controlled Motion vs Immobilization
The summary, exam pearls and cheat sheet all state that "controlled motion is beneficial," and a viva will ask how motion influences collagen alignment and how an internal brace alters healing — so the underlying mechanobiology deserves developing.
Immobilization is harmful. Prolonged immobilization produces a disorganised matrix with randomly oriented collagen, adhesions, reduced matrix turnover, and a loss of tensile strength and stiffness. Critically, it also causes resorption and weakening at the bone–ligament insertion, so the insertion site becomes the weak link after a period of immobilisation.
Controlled cyclic loading is beneficial. Mechanical stress is a signal: it aligns fibroblasts and collagen fibres along the lines of stress (a soft-tissue analogue of Wolff's law), promotes larger-diameter fibrils and better cross-linking, raises tensile strength and stiffness, and reduces adhesions — improving the quality and organisation of the healing scar, not just its bulk.
But it is dose-dependent — an "envelope of function". Too little load gives a weak, disorganised scar; appropriate controlled load optimises organised healing; excessive load too early causes gap formation, elongation or re-rupture. This dose-response is exactly why rehabilitation uses early protected range of motion and graduated functional loading, and is the rationale for hinged bracing and for internal-brace augmentation (sharing load to protect a repair through the vulnerable phase — though whether the brace also stress-shields the healing ligament remains debated, as noted in the controversies). General bone mechanotransduction is developed in the osteocytes-mechanotransduction topic, and the viscoelastic material behaviour of ligament in the viscoelasticity topic.
Cyclic loading aligns fibroblasts and collagen along stress lines, enlarges fibrils and raises tensile strength, whereas immobilisation yields a disorganised, weaker scar with adhesions and insertion-site resorption. The effect is dose-dependent — excessive early load causes gap/re-rupture — so rehab uses protected, graduated loading, the rationale for hinged bracing and internal-brace augmentation.
Differential Diagnosis of Poor Ligament/Soft-Tissue Healing
When a ligament injury fails to recover as expected, the differential is broader than the index injury. Distinguish a biologically non-healing ligament (e.g. ACL) from a missed associated injury or a systemic cause of impaired healing.
- Key Discriminator
- Synovial environment, gap, retraction
- Confirmatory Clue
- MRI shows discontinuity; persistent pivot shift
- Key Discriminator
- Multidirectional or rotatory instability
- Confirmatory Clue
- Stress radiographs, examination under anaesthesia
- Key Discriminator
- Superficial MCL flips superficial to pes anserinus
- Confirmatory Clue
- MRI; explains a non-healing 'grade II' MCL
- Key Discriminator
- Recurrent giving way, effusions
- Confirmatory Clue
- MRI meniscal/chondral injury, bone bruising
- Key Discriminator
- Generalised poor wound healing
- Confirmatory Clue
- HbA1c, smoking history, nutritional markers
- Key Discriminator
- Generalised hyperlaxity, recurrent injury
- Confirmatory Clue
- Beighton score, family history
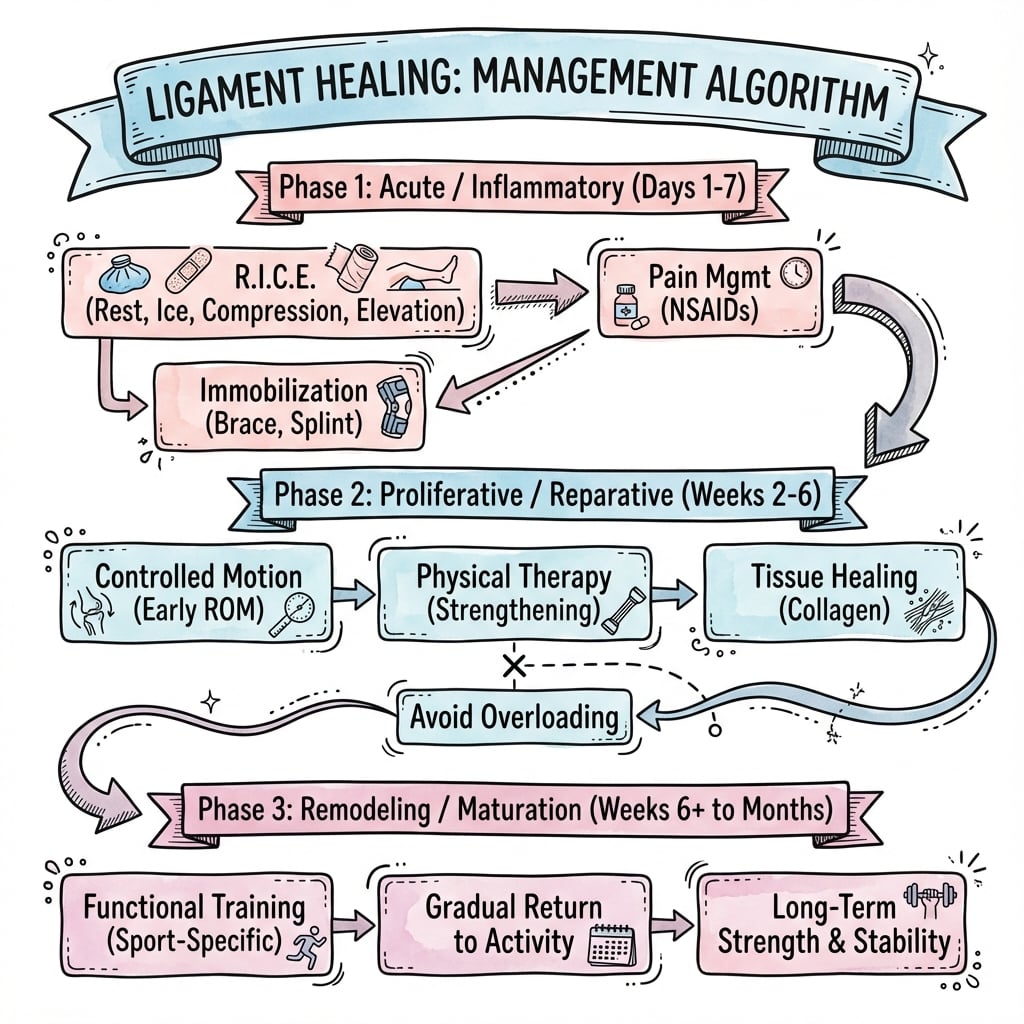
Management Algorithm
Clinical Relevance - MCL vs ACL
MCL Healing (Extra-articular)
The MCL heals predictably with conservative management in most cases. The extra-articular location allows hematoma formation and containment. Periligamentous tissues provide blood supply. The healing MCL is enlarged but functional.
Management: Protected motion, hinged brace, rehabilitation. Surgery rarely needed for isolated MCL injuries. Valgus stress protected during healing.
Outcome: Functional recovery expected. Healed MCL has 50-70% of normal tensile strength but increased cross-sectional area. Most patients return to function.
ACL Healing (Intra-articular)
The ACL does not heal spontaneously. Synovial environment is hostile to healing. Reconstruction is required to restore stability in active patients wanting to return to pivoting activities.
Why Reconstruction: The ACL cannot heal itself. Leaving the knee ACL-deficient leads to instability and risk of secondary meniscal and chondral damage. Reconstruction uses graft to replace function.
Modern Research: ACL repair (primary suture, internal bracing, or scaffold bridging as in BEAR) is being revisited for proximal/midsubstance tears with good tissue. Reconstruction remains the standard for most complete tears in pivoting athletes.
Intra-articular vs Extra-articular Healing — Side by Side
- Extra-articular (MCL)
- Contained — forms a healing scaffold
- Intra-articular (ACL)
- Dispersed by synovial fluid; no stable clot
- Extra-articular (MCL)
- Retained at injury site
- Intra-articular (ACL)
- Diluted and washed away
- Extra-articular (MCL)
- Ends stay apposed
- Intra-articular (ACL)
- Ends retract, leaving a gap
- Extra-articular (MCL)
- Rich periligamentous vessels
- Intra-articular (ACL)
- Sparse; relies on synovium and fat pad
- Extra-articular (MCL)
- Absent
- Intra-articular (ACL)
- Hostile plasmin-rich, anti-clotting milieu
- Extra-articular (MCL)
- Reliable scar healing, 50-70% strength
- Intra-articular (ACL)
- No spontaneous healing of complete tears
- Extra-articular (MCL)
- Non-operative (brace, protected motion)
- Intra-articular (ACL)
- Reconstruction (or selected repair/BEAR)
Graft Ligamentization & Tendon-to-Bone Healing
Because the torn ACL "cannot heal" and is replaced with a graft, examiners ask the obvious follow-up: how does the graft heal? A tendon graft does not stay tendon — it remodels into an ACL-like structure through a process called ligamentization, in overlapping phases:
- Early (avascular) phase (first weeks): the free graft is initially avascular, with central necrosis and falling cellularity. Mechanically it depends on its initial fixation, while its intrinsic material strength declines.
- Revascularization & cellular repopulation (around 6 to 12 weeks): host cells and vessels (from synovium and fat pad) invade the graft. This is the window in which the graft is mechanically weakest — the "ligamentization valley" — and is the biological reason rehabilitation is protected and graduated rather than aggressive in the first few months.
- Remodeling / maturation (months to over a year): collagen realigns, crimp returns and cellularity normalises, so the graft becomes ACL-like. As with native ligament scar, it never fully matches the original ACL (smaller fibrils, incomplete cross-link maturation), and maturation can take well over a year.
Tendon-to-bone (tunnel) healing — the fixation interface. The graft must also integrate within the bone tunnel. Soft-tissue grafts (e.g. hamstring) heal by an indirect, fibrovascular interface with Sharpey-like fibres maturing over weeks to months, whereas bone-block grafts (bone–patellar tendon–bone) achieve faster, more direct bone-to-bone union. This difference in interface biology is one driver of graft choice and of how early the construct can be loaded. (The detailed enthesis/insertion-site biology is developed in the tendon-bone-interface-enthesis topic.)
A tendon ACL graft undergoes ligamentization: early avascular necrosis → revascularization and cellular repopulation (mechanically weakest at ~6 to 12 weeks — the basis for protected early rehab) → remodeling over a year into an ACL-like but never-identical structure. In the tunnel, soft-tissue grafts integrate slower via an indirect Sharpey-fibre interface, while bone-block (BTB) grafts heal faster bone-to-bone.
Guidelines, Registries & Global Practice
Global Epidemiology
- ACL injuries occur in roughly 30 to 80 per 100,000 person-years, concentrated in 15 to 45-year-olds and in pivoting/cutting sports; females carry a several-fold higher sport-adjusted risk.
- Isolated MCL injury is the most common knee ligament injury overall and the great majority are managed non-operatively with reliable healing.
Side-by-Side Guidance
- Emphasis
- Evidence-based reconstruction for instability
- Practical Recommendation
- Reconstruction recommended for active patients with instability; repair selected/emerging
- Emphasis
- Shared decision-making, rehab-first pathways
- Practical Recommendation
- Structured rehabilitation; reconstruction if persistent functional instability
- Emphasis
- Individualised, tear-pattern based
- Practical Recommendation
- Recognises a role for repair/augmentation in selected proximal tears; reconstruction default
- Emphasis
- Biology favours non-operative healing
- Practical Recommendation
- Brace and protected motion for isolated grade I-III MCL; surgery for select distal/combined
Registry & Outcome Signals
- National ligament/ACL registries (e.g. Scandinavian and UK datasets) track graft choice, revision and reinjury, informing graft selection and rehabilitation rather than healing biology per se.
- Emerging BEAR and primary-repair data are not yet captured at registry scale, so practice change should remain cautious.
High- vs Limited-Resource Practice
- Well-resourced settings: ready access to MRI, arthroscopic reconstruction, and increasingly repair/BEAR in selected patients, with supervised criteria-based rehabilitation.
- Limited-resource settings: non-operative management and bracing dominate; isolated MCL injuries heal reliably without surgery, and structured rehabilitation is the highest-value intervention where arthroscopy is scarce.
Controversies & Areas of Uncertainty
- Does the ACL truly never heal? The BEAR II trial shows engineered intra-articular healing is possible in selected young patients, but the numerically higher reinjury rate, narrow inclusion (complete midsubstance tears treated within ~45 days), and limited long-term and registry data mean reconstruction stays the default for most pivoting athletes.
- Patient selection for primary repair. Excellent outcomes are confined to proximal avulsion tears with good tissue. There is no validated, reproducible intra-operative grading of tissue quality, so selection remains subjective and operator-dependent.
- Internal bracing — protection or stress-shielding? Suture tape augmentation may protect an early repair, but it could also stress-shield the healing ligament and alter its remodelling; the BEAR II reinjury signal and small repair cohorts leave this unresolved.
- Biological augmentation (PRP, growth factors, scaffolds). Animal data (PDGF-BB, collagen-platelet composite) are encouraging, but human evidence that PRP meaningfully improves ligament healing or outcome remains inconsistent.
- Grade III MCL and combined injuries. Whether high-grade or distal (superficial-MCL avulsion / Stener-like) MCL tears, and the MCL component of combined ACL/MCL injuries, need repair or augmentation rather than bracing is still debated.
MCQ Practice Points
Q: Why does the ACL fail to heal? A: Intra-articular location, synovial fluid disperses hematoma, torn ends retract, poor blood supply. No scaffold forms for healing and growth factors are washed away.
Q: What percentage of normal tensile strength does a healed MCL achieve? A: 50-70% of normal. The healed MCL compensates with increased cross-sectional area. Functional recovery is expected despite inferior tissue quality.
Q: What are the three phases of ligament healing? A: Inflammatory (0-1 week), Proliferative (1-6 weeks), Remodeling (6 weeks+). Same as tendon healing with Type III to Type I collagen transition.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“An examiner asks you to explain why the MCL heals with conservative treatment while the ACL does not.”
“The examiner asks you to take them through the phases of ligament healing and explain why a healed ligament never matches the original.”
“A 17-year-old has a complete proximal ACL tear. The examiner asks whether the ACL can ever heal and where primary repair or bridge-enhanced repair fit against reconstruction.”
Healing Phases
- Inflammatory (0-1 week): Hematoma, cells
- Proliferative (1-6 weeks): Type III collagen
- Remodeling (6+ weeks): Type I collagen
MCL Heals Well
- Extra-articular location
- Contained hematoma as scaffold
- Adequate blood supply
- Achieves 50-70% normal strength
ACL Does Not Heal
- Intra-articular location
- Synovial fluid disperses clot
- Ends retract creating gap
- Poor blood supply
Clinical Management
- MCL: Conservative (brace, protected motion)
- ACL: Reconstruction if stability needed
- Healed tissue never equals normal
- Controlled motion aids healing
Evidence Base
- Synthesised molecular biology and biomechanics of normal and healing rabbit MCL
- Scar matrix has flaws, smaller-than-normal collagen fibril diameters, and failed cross-link maturation
- These deficiencies explain scar weakness and increased creep despite enlarged cross-sectional area
- Joint motion and systemic hormones (pregnancy) modulate both normal and healing ligament behaviour
- Screened growth factors in vitro then applied to a transected rabbit MCL model
- PDGF-BB and EGF best stimulated fibroblast proliferation; TGF-beta1 best stimulated matrix synthesis
- High-dose PDGF-BB significantly increased ultimate load, elongation and energy-to-failure at 6 weeks (dose-dependent)
- Adding TGF-beta1 to PDGF-BB gave no further structural gain
- Porcine model of ACL reconstruction, collagen-platelet composite augmentation, and bioenhanced primary repair
- T2*-weighted MRI volume predicted healing tissue structural properties (R-squared up to 0.56)
- Combining volume and signal intensity predicted maximum load, yield load and stiffness (R-squared up to 0.73)
- Established a non-invasive surrogate for the strength of a healing ACL repair or graft
- Randomised 100 patients (median age 17) with complete midsubstance ACL tears to bridge-enhanced repair (n=65) vs autograft reconstruction (n=35)
- At 2 years BEAR was non-inferior for IKDC subjective score (88.9 vs 84.8) and AP laxity side-to-side difference (1.61 vs 1.77 mm)
- BEAR gave superior hamstring strength index (98.2% vs 63.2%)
- Reinjury requiring further ipsilateral ACL surgery: 14% BEAR vs 6% ACLR (not significant)
- First 11 consecutive patients with proximal avulsion ACL tears treated by arthroscopic suture-anchor primary repair
- At minimum 5-year follow-up 9 of 10 had IKDC objective grade A and full range of motion
- Mean Lysholm 96, subjective IKDC 92 — excellent durable scores
- Outcomes confined to carefully selected proximal tears with excellent tissue quality
- 56 consecutive arthroscopic ACL repairs, 27 with additional internal brace augmentation
- Overall failure rate 10.7% at mean 3.2-year follow-up
- Failure 7.4% with vs 13.8% without internal bracing (not statistically significant)
- 73% achieved objective IKDC grade A in a selected population