Local Anaesthetics
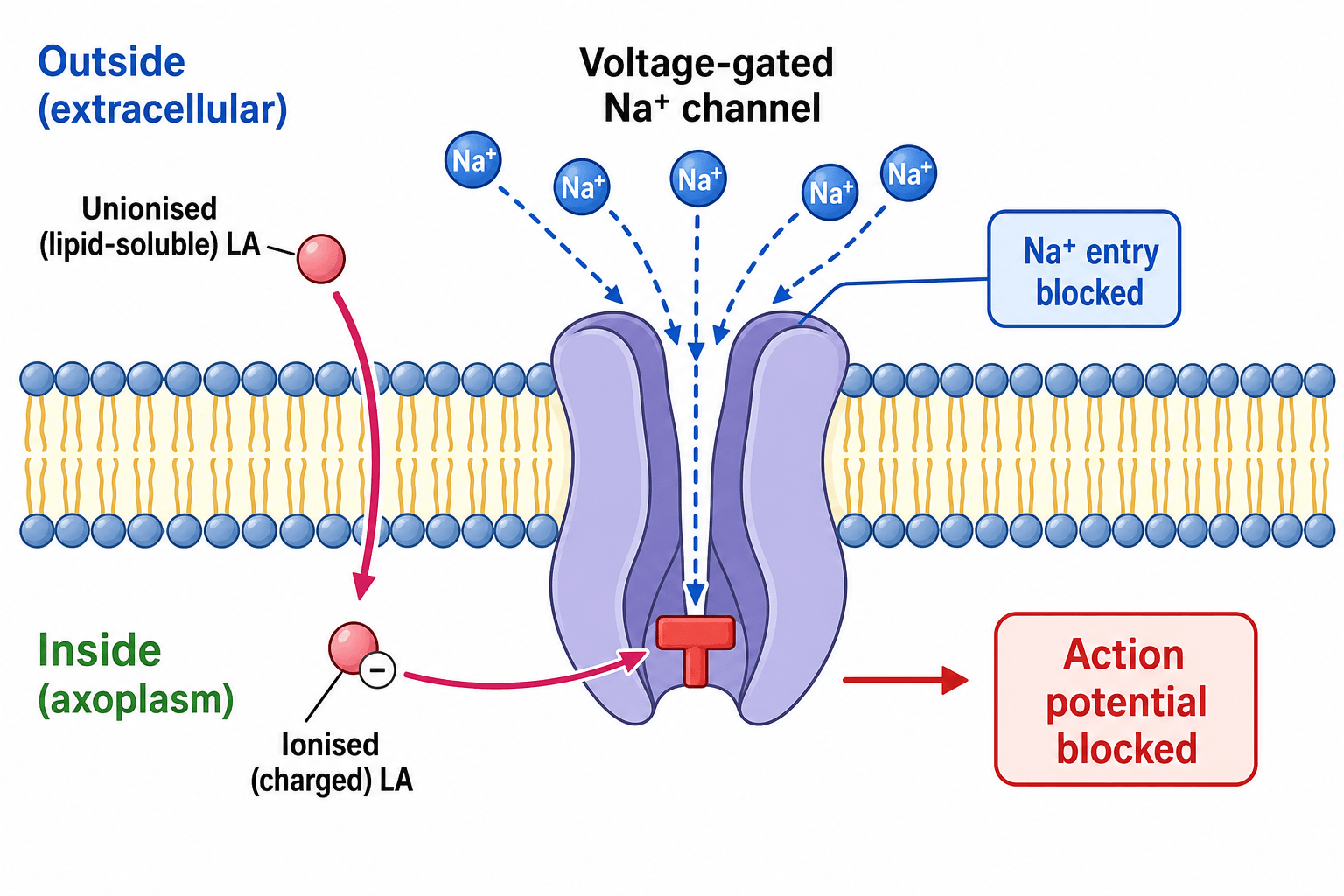
Local anaesthetics block voltage-gated sodium channels from the inside of the nerve. Without sodium influx the action potential cannot rise, so the nerve cannot conduct. Small unmyelinated pain fibres are blocked before large motor fibres, which is why patients keep some movement while pain is gone.
The single most testable safety point. Plain lignocaine 3 mg/kg, with adrenaline 7 mg/kg, plain bupivacaine 2 mg/kg. Convert the percentage to milligrams first (1 percent equals 10 mg/mL). Calculating the maximum dose before injecting prevents toxicity.
Bupivacaine is the most cardiotoxic common agent - it binds cardiac sodium channels avidly and dissociates slowly, so cardiac arrest may appear early and be hard to resuscitate. Ropivacaine and levobupivacaine were designed to be safer alternatives.
Local anaesthetic systemic toxicity starts with peri-oral tingling, a metallic taste, tinnitus, and confusion, then progresses to seizures and cardiovascular collapse. Stop injecting, call for help, manage the airway, and give intravenous lipid emulsion 20 percent.
Overview
Local anaesthetics are drugs that temporarily and reversibly block nerve conduction in a defined area, removing sensation (and at higher doses, movement) without putting the patient to sleep. In orthopaedics they are everywhere: infiltrating a wound, performing a digital block, doing a haematoma block for a wrist fracture, providing a peripheral nerve block for postoperative pain, and as part of spinal anaesthesia for lower-limb surgery.
For the exam, three threads run through this topic. The first is how they work - blocking sodium channels and the chemistry that decides onset, potency, and duration. The second is how to use them safely - the two drug classes, the use of adrenaline, and above all the maximum safe dose. The third is what goes wrong - recognising and treating local anaesthetic systemic toxicity before it becomes a fatal cardiac arrest. Get those three right and you can answer almost any question on this subject.
Principles: How Local Anaesthetics Work
A nerve fires by letting sodium ions rush in through voltage-gated channels, which produces the action potential. Local anaesthetics enter the nerve and plug these sodium channels from the inside, so the action potential cannot rise and the message stops. The block is reversible: as the drug washes away, the channels reopen and the nerve recovers.
To reach the inside of the nerve, the drug must first cross the fatty nerve membrane. Each molecule exists in two forms - an unionised (lipid-soluble) form that crosses the membrane, and an ionised (charged) form that actually blocks the channel once inside. The balance between the two depends on the drug's pKa and the surrounding pH, which explains several exam favourites.
- What it controls
- Speed of onset
- Why it matters clinically
- A lower pKa leaves more unionised drug to cross the membrane, so onset is faster (lignocaine acts faster than bupivacaine)
- What it controls
- Potency
- Why it matters clinically
- More lipid-soluble drugs cross the membrane more easily and are more potent (bupivacaine is potent)
- What it controls
- Duration of action
- Why it matters clinically
- More tightly protein-bound drugs stay at the channel longer, giving a longer block (bupivacaine is long-acting)
- What it controls
- Whether the block works at all
- Why it matters clinically
- Acidic infected tissue keeps the drug ionised and unable to cross the membrane, so blocks fail near abscesses
Nerve fibres are not all blocked at once. Small, thin pain and autonomic fibres are blocked first, then touch and temperature, and the large motor fibres last. This differential block is why a patient may be pain-free yet still able to move a little, and it is a neat point to mention in a viva.
The Two Classes and the Common Agents
Every local anaesthetic is either an amide or an ester, decided by the chemical link in the middle of the molecule. The distinction matters for metabolism and for allergy.
- Examples: lignocaine (lidocaine), bupivacaine, levobupivacaine, ropivacaine, prilocaine.
- Metabolism: in the liver - so caution in significant liver disease.
- Allergy: genuinely rare; most reported "allergies" are actually a reaction to adrenaline or a vasovagal faint.
- Memory trick: amide names contain two letter i's (l-i-gnoca-i-ne, bup-i-vaca-i-ne).
These are the agents you use almost every day in orthopaedics.
- Class
- Amide
- Onset / Duration
- Fast onset, short to medium duration
- Key points
- The workhorse for infiltration and blocks; plain 3 mg/kg, with adrenaline 7 mg/kg
- Class
- Amide
- Onset / Duration
- Slow onset, long duration
- Key points
- Long-lasting but the most cardiotoxic; plain about 2 mg/kg; avoid intravenous regional anaesthesia
- Class
- Amide
- Onset / Duration
- Slow onset, long duration
- Key points
- Designed as less cardiotoxic alternatives to racemic bupivacaine
- Class
- Amide
- Onset / Duration
- Fast onset, short duration
- Key points
- Low cardiotoxicity (favoured for intravenous regional anaesthesia); high doses can cause methaemoglobinaemia
- Class
- Ester
- Onset / Duration
- Variable
- Key points
- Older agents; higher allergy risk via PABA; now used less
Separate from LAST, prilocaine (and topical benzocaine) can cause methaemoglobinaemia, which is worth knowing in its own right. The prilocaine metabolite o-toluidine (and benzocaine directly) oxidises haemoglobin iron from the ferrous (Fe2+) to the ferric (Fe3+) state, producing methaemoglobin, which cannot carry oxygen and shifts the dissociation curve to the left. Classic exam triggers are a large prilocaine dose, a topical benzocaine spray, and EMLA cream in a neonate.
Recognise it by: central cyanosis that does NOT improve with oxygen, "chocolate-brown" arterial blood, and a pulse oximeter that sticks at around 85 percent regardless of the true saturation (a "saturation gap" between the SpO2 and the calculated SaO2). Confirm with co-oximetry.
Treat with intravenous methylene blue (about 1 to 2 mg/kg), which reduces methaemoglobin back to haemoglobin, and stop the offending agent — but methylene blue is ineffective and potentially harmful in G6PD deficiency (ascorbic acid is the alternative there).
Safe Dosing and the Role of Adrenaline
The maximum safe dose is the highest-yield practical point in this topic. Doses are by body weight, and you must convert the concentration to milligrams first.
Plain lignocaine about 3 mg/kg; lignocaine with adrenaline about 7 mg/kg; plain bupivacaine about 2 mg/kg. These are guides, not absolutes - reduce them in the frail, the elderly, and those with cardiac or liver disease.
A 1 percent solution is 10 mg/mL, 2 percent is 20 mg/mL, 0.5 percent is 5 mg/mL. Always turn the percentage into milligrams per millilitre, then work out how many millilitres your patient can safely receive.
Adrenaline causes vasoconstriction, which slows absorption into the blood, prolongs the block, reduces bleeding in the field, and raises the maximum safe dose of the local anaesthetic.
Traditional teaching avoided adrenaline in end-arteries (fingers, toes, nose, penis) for fear of ischaemia. Modern evidence shows low-dose adrenaline is usually safe in healthy digits, but exams still expect you to know and respect the classic caution.
A worked example examiners love: for a 70 kg adult, plain lignocaine at 3 mg/kg gives a maximum of 210 mg. As 1 percent lignocaine is 10 mg/mL, that is 21 mL of 1 percent solution. Showing this calculation out loud demonstrates safe practice.
Adrenaline is not the only way to modify a block, and examiners may push for the rest:
- Sodium bicarbonate (alkalinisation): adding a small amount of bicarbonate raises the solution's pH, increasing the unionised fraction so more drug crosses the membrane — this speeds onset, reduces the sting of injection, and partly counters the block failure of acidic, infected tissue. Add cautiously, because too much precipitates the drug (especially bupivacaine).
- Perineural adjuncts that prolong the block: alpha-2 agonists (clonidine, dexmedetomidine) and dexamethasone are commonly added to peripheral nerve blocks to extend their duration; opioids are used in neuraxial blocks.
- Tachyphylaxis: repeated top-up doses (for example through an epidural catheter) can give a progressively shorter or weaker effect over time, partly from local tissue acidosis — anticipate it rather than simply escalating the dose.
Local Anaesthetic Systemic Toxicity (LAST)
LAST occurs when the blood level of local anaesthetic rises high enough to poison the brain and heart. It usually follows accidental intravascular injection or simply giving too large a dose. It is the emergency every user of these drugs must be able to recognise and treat.
- Early signs
- Peri-oral tingling, metallic taste, tinnitus, light-headedness, agitation
- Late / severe signs
- Seizures, then loss of consciousness and coma
- Early signs
- Hypertension and tachycardia (early excitation)
- Late / severe signs
- Bradycardia, arrhythmias, hypotension, cardiac arrest
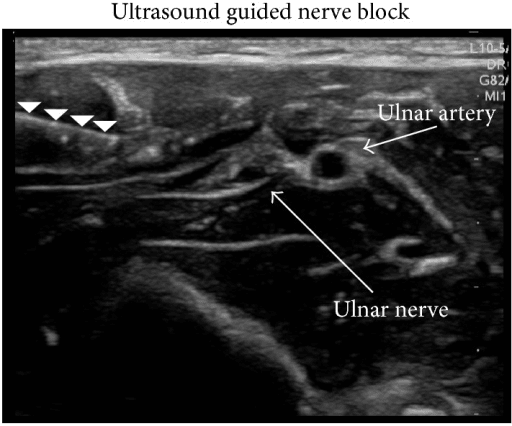
Classic teaching is that central nervous system signs come first, but cardiovascular collapse can be the first sign, especially with bupivacaine. Prevention is better than cure: use the lowest effective dose, aspirate before injecting, inject slowly in small increments, and use ultrasound guidance to see the needle and avoid vessels.
Stop injecting and call for help. Manage the airway with 100 percent oxygen and control seizures (a benzodiazepine). Start intravenous lipid emulsion 20 percent (a bolus followed by an infusion) - the "lipid sink" pulls the drug away from the heart and brain. Begin CPR if there is cardiac arrest; resuscitation may need to be prolonged. Avoid or reduce adrenaline doses and avoid certain antiarrhythmics during a LAST arrest - follow your local LAST protocol.
Clinical Relevance
Local anaesthetics touch nearly every part of orthopaedic practice. In the emergency department you use them for haematoma blocks to reduce a Colles' fracture, for digital blocks, and for wound infiltration. In theatre they appear in peripheral nerve blocks, periarticular infiltration after joint replacement, and spinal anaesthesia. On the ward they underpin multimodal, opioid-sparing pain relief. The exam tests this breadth in several ways: a basic-science viva on mechanism and the amide-versus-ester distinction, a safety question on calculating the maximum dose, and a CIM or clinical scenario on recognising and treating LAST. Knowing the mechanism, the safe dose, and the emergency lets you answer confidently and, more importantly, practise safely.
Guidelines, Registries and Global Practice
- Major guidelines (for example the American Society of Regional Anesthesia and Pain Medicine, and the Association of Anaesthetists in the UK) agree on the core safety message: calculate the maximum dose, aspirate and inject incrementally, use ultrasound guidance where possible, and keep intravenous lipid emulsion 20 percent immediately available wherever local anaesthetics are used.
- Where guidance differs is mostly in the small print of LAST treatment - the exact lipid emulsion bolus and infusion regimen and the maximum cumulative dose vary slightly between national protocols, so candidates are expected to follow their local protocol rather than memorise a single set of numbers.
- Maximum-dose figures quoted in textbooks vary modestly between countries and formularies; the safe approach is to know the commonly cited adult values (lignocaine 3 mg/kg, with adrenaline 7 mg/kg, bupivacaine 2 mg/kg) and to reduce them in vulnerable patients.
- Global practice variation reflects drug availability and cost more than disagreement on principle - long-acting and liposomal preparations are used selectively, and registry and trial evidence has tempered early enthusiasm for liposomal bupivacaine where it offers little over standard agents within a multimodal pathway.
Memory aids
iiiAmides vs Esters
Hook:Count the letter i - two i's means amide (liver), one i means ester (plasma esterases).
TASTESigns of LAST
Hook:A bad TASTE warns of LAST - Tingling/Taste, Auditory, Seizures, Tachy/brady, Emulsion.
PODWhat Drives the Drug
Hook:A POD of properties - pKa (onset), Oil solubility (potency), protein binding (Duration).
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You are about to infiltrate local anaesthetic before a minor hand procedure. The examiner asks how local anaesthetics work, the two drug classes, and how you choose a safe dose.”
“Minutes after you perform a regional block with bupivacaine, the patient complains of a metallic taste and tinnitus, becomes agitated, then has a seizure and loses cardiac output. What is happening and what do you do?”
Mechanism and Properties
- Block voltage-gated sodium channels from inside the nerve - reversible
- Pain fibres blocked before motor fibres (differential block)
- pKa sets onset, lipid solubility sets potency, protein binding sets duration
- Acidic infected tissue makes blocks fail
Classes
- Amides (lignocaine, bupivacaine, ropivacaine): liver metabolism, allergy rare, two i's in the name
- Esters (procaine, tetracaine, cocaine): plasma esterases to PABA, allergy more common, one i
- Bupivacaine is the most cardiotoxic; ropivacaine and levobupivacaine are safer alternatives
- Prilocaine favoured for intravenous regional anaesthesia (risk: methaemoglobinaemia at high dose)
Safe Dosing
- Plain lignocaine about 3 mg/kg; with adrenaline about 7 mg/kg
- Plain bupivacaine about 2 mg/kg
- 1 percent equals 10 mg/mL - convert before calculating
- Adrenaline: vasoconstriction slows absorption, prolongs block, reduces bleeding, raises max dose
LAST - Red Flags
- Early: peri-oral tingling, metallic taste, tinnitus, confusion
- Late: seizures, arrhythmias, cardiovascular collapse
- Treat: stop injecting, airway and oxygen, control seizures, intravenous lipid emulsion 20 percent
- Resuscitation may be prolonged; follow the local LAST protocol
Evidence and Key Concepts
Every citation below has been checked against its source record in PubMed. The two LAST reviews converge on the same message — atypical presentation (one-fifth purely cardiovascular), prevention by ultrasound/aspiration/minimal dose, and rescue with early IV lipid emulsion 20% — while the Hyland RCT tempers enthusiasm for costly liposomal bupivacaine, which gave no clinical edge within a modern multimodal pathway.
Local anesthetic systemic toxicity: current perspectives
- LAST is a life-threatening event with diverse effects on the central nervous and cardiovascular systems
- Presentation is often atypical, and about one-fifth of reported cases present with isolated cardiovascular disturbance
- Risk is reduced by ultrasound guidance for regional techniques and by restricting the drug dose
- Key treatment advances are early lipid emulsion therapy, prompt seizure control, and careful choice of cardiovascular support drugs
Local anesthetic systemic toxicity: a narrative review for emergency clinicians
- LAST is uncommon but potentially fatal and can follow any route of local anaesthetic use
- Extremes of age, organ dysfunction, and higher or repeated doses increase the risk
- Early recognition plus supportive care and intravenous lipid emulsion 20 percent are the mainstays of treatment
- Ultrasound guidance, aspiration before injection, and using the minimal effective dose reduce risk
Liposomal vs Standard Bupivacaine After Knee Replacement (RCT)
- Randomised controlled trial of 59 patients comparing liposomal bupivacaine with conventional bupivacaine periarticular injection in total knee arthroplasty
- All patients also received regional anaesthesia and a standard multimodal analgesia protocol
- No significant difference in the primary outcome (physical therapy sessions to discharge) or in clinical secondary outcomes
- Liposomal bupivacaine carried significantly higher medication charges